
New Antenna Upgrade Boosts MRI Image Quality

Magnetic resonance imaging (MRI) is one of medicine’s most powerful diagnostic tools. But certain tissues deep inside the body – including brain regions and delicate structures of the eye and orbit that are of particular relevance for ophthalmology – are difficult to image clearly. The problem is not the scanner itself, but the hardware that sends and receives radio signals.
Now, researchers at the Max Delbrück Center have developed an advanced materials-based MRI antenna that overcomes these limitations – delivering enhanced images more quickly and that can be used in existing MRI machines. The research, led by Nandita Saha, a doctoral student in the Experimental Ultrahigh Field Magnetic Resonance lab of Professor Thoralf Niendorf, was published in Advanced Materials.
Niendorf and his team worked closely with researchers at Rostock University Medical Center, combining expertise in MRI physics with clinical ophthalmology and translational imaging. The Rostock team is also supporting clinical validation of the technology.
“By using concepts from metamaterials, we were able to guide radiofrequency fields more efficiently and demonstrate how advanced physics can directly improve medical imaging,” says Niendorf, senior author of the paper. “This work shows a pathway toward faster, clearer MRI scans that could benefit patients in many clinical areas.”
Rethinking MRI hardware with metamaterials
MRI works by sending radiofrequency (RF) signals into the body and detecting how tissues respond inside a strong magnetic field. The stronger the signal response, the better the image. Conventional MRI antennas – also called RF coils – often struggle to collect enough signal from deep or anatomically complex regions. This leads to images that lack detail and prolongs scan times.
The research team addressed this bottleneck by integrating metamaterials directly into the MRI antenna. Metamaterials are engineered structures that interact with electromagnetic waves in ways not found in natural materials. The engineered RF antenna increases signal strength from targeted tissues, improves spatial resolution and image sharpness and enables faster data acquisition. Crucially, the antenna fits into existing MRI systems, avoiding the need for new infrastructure. The team validated the technology by imaging the eye and orbit region in a group of volunteers at 7.0 Tesla.
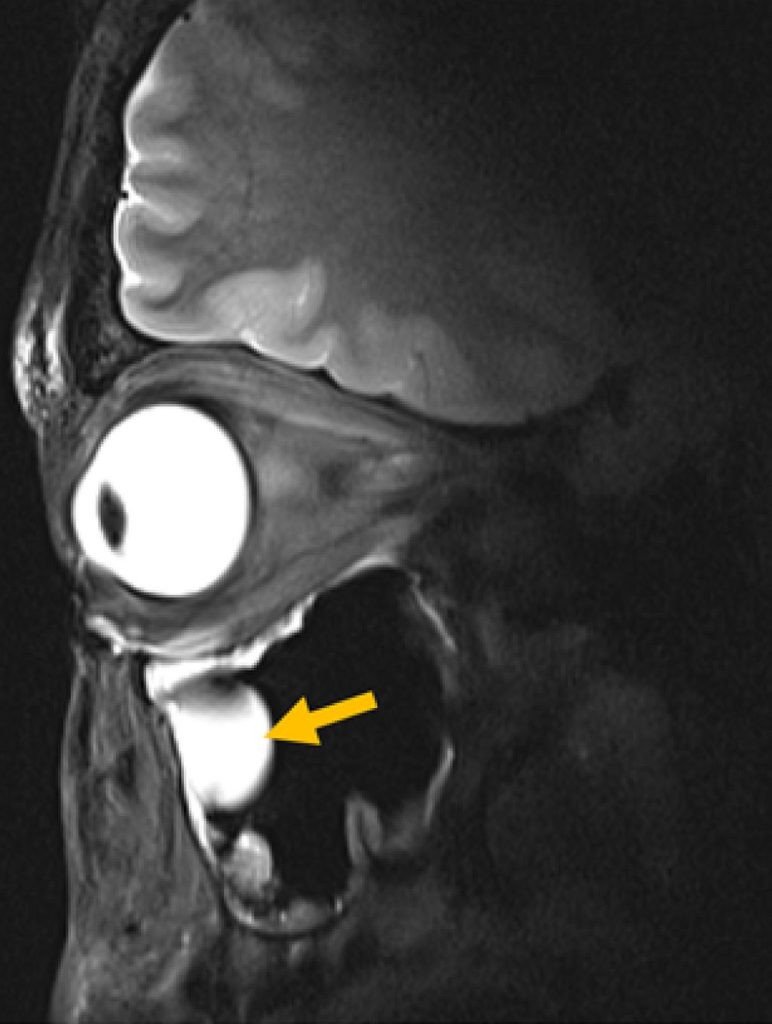
© AG Niendorf, Max Delbrück Center
“Our research demonstrates clear relevance for ophthalmological applications as it can facilitate anatomically detailed, high-spatial resolution MRI of the eye,” says Professor Oliver Stachs, a co-author of the paper at University Medicine Rostock. “It offers the potential to open a window into the eye and into (patho)physiological processes that in the past have been largely inaccessible.”
“Our goal was to rethink MRI hardware from the modern physics of antenna design,” adds Saha. This technology can also be tuned to protect sensitive areas of the body during MRI, for example, to reduce unwanted heating around medical implants, she adds. It could also be used to focus RF energy more effectively for MRI guided therapies for various cancer treatments, such as gentle heating of tumors (hyperthermia) or thermal ablation of tissue.
Better diagnostics
For patients, MRI scans can be uncomfortable and time-consuming – even more so when images need to be repeated because important details are hard to see. Faster scans mean patients spend less time inside scanners. Clearer images mean doctors can make diagnoses with greater confidence. And because the new antenna is lightweight and compact, it can also be designed to better fit specific parts of the body, improving comfort even further.
The technology could also be adapted to support MRI systems running at magnetic field strengths lower or higher than 7.0T, to image target anatomy other than the eye, orbit or the brain or to track metabolism or drug movement inside the body, says Niendorf. Special MRI scans that use other atoms, such as sodium or fluorine, could also benefit from this technology by producing clearer signals and better images, he adds.
“Innovations in imaging hardware have the potential to transform diagnostics, and this study is an important step toward next-generation MRI technology,” says Dr Ebba Beller, a co-author of the paper at Rostock University Medical Center.
The researchers are already planning larger studies at multiple hospitals and adapting the design for other organs, such as the heart and kidneys. The collaboration will continue to be strengthened by long-standing reciprocal visiting scientist appointments of Stachs and Niendorf.







