Researchers have found why common cuff-based blood pressure readings are inaccurate and how they might be improved, which could improve health outcomes for patients.
Photo by CDC on Unsplash
High blood pressure, or hypertension, is the top risk factor for premature death, associated with heart disease, strokes and heart attacks. However, inaccuracies in the most common form of blood pressure measurement mean that as many as 30% of cases of high blood pressure could be missed.
The researchers, from the University of Cambridge, built an experimental model that explained the physics behind these inaccuracies and provided a better understanding of the mechanics of cuff-based blood pressure readings.
The researchers say that some straightforward changes, which don’t necessarily involve replacing standard cuff-based measurement, could lead to more accurate blood pressure readings and better results for patients. Their results are reported in the journal PNAS Nexus.
Anyone who has ever had their blood pressure taken will be familiar with the cuff-based method. This type of measurement, also known as the auscultatory method, relies on inflating a cuff around the upper arm to the point where it cuts off blood flow to the lower arm, and then a clinician listens for tapping sounds in the arm through a stethoscope while the cuff is slowly deflated.
Blood pressure is inferred from readings taken from a pressure gauge attached to the deflating cuff. Blood pressure is given as two separate numbers: a maximum (systolic) and a minimum (diastolic) pressure. A blood pressure reading of 120/80 is considered ‘ideal’.
“The auscultatory method is the gold standard, but it overestimates diastolic pressure, while systolic pressure is underestimated,” said co-author Kate Bassil from Cambridge’s Department of Engineering. “We have a good understanding of why diastolic pressure is overestimated, but why systolic pressure is underestimated has been a bit of a mystery.”
“Pretty much every clinician knows blood pressure readings are sometimes wrong, but no one could explain why they are being underestimated — there’s a real gap in understanding,” said co-author Professor Anurag Agarwal, also from Cambridge’s Department of Engineering.
Previous non-clinical studies into measurement inaccuracy used rubber tubes that did not fully replicate how arteries collapse under cuff pressure, which masked the underestimation effect.
The researchers built a simplified physical model to isolate and study the effects of downstream blood pressure — the blood pressure in the part of the arm below the cuff. When the cuff is inflated and blood flow to the lower arm is cut off, it creates a very low downstream pressure. By reproducing this condition in their experimental rig, they determined this pressure difference causes the artery to stay closed for longer while the cuff deflates, delaying the reopening and leading to an underestimation of blood pressure.
This physical mechanism — the delayed reopening due to low downstream pressure — is the likely cause of underestimation, a previously unidentified factor. “We are currently not adjusting for this error when diagnosing or prescribing treatments, which has been estimated to lead to as many as 30% of cases of systolic hypertension being missed,” said Bassil.
Instead of the rubber tubes used in earlier physical models of arteries, the Cambridge researchers used tubes that lay flat when deflated and fully close when the cuff pressure is inflated, the key condition for reproducing the low downstream pressure observed in the body.
The researchers say that there are a range of potential solutions to this underestimation, which include raising the arm in advance of measurement, potentially producing a predictable downstream pressure and therefore predictable underestimation. This change doesn’t require new devices, just a modified protocol.
“You might not even need new devices, just changing how the measurement is done could make it more accurate,” said Agarwal.
However, if new devices for monitoring blood pressure are developed, they might ask for additional inputs which correlate with downstream pressure, to adjust what the ‘ideal’ readings might be for each individual. These may include age, BMI, or tissue characteristics.
The researchers hope to secure funding for clinical trials to test their findings in patients, and are looking for industrial or research partners to help refine their calibration models and validate the effect in diverse populations. Collaboration with clinicians will also be essential to implement changes to clinical practice.
The research was supported by the Engineering and Physical Sciences Research Council (EPSRC), part of UK Research and Innovation (UKRI). Anurag Agarwal is a Fellow of Emmanuel College, Cambridge.
People who regularly consume caffeine are usually in a better mood after a cup of coffee or another caffeinated drink – an effect that is much more pronounced in the morning than later in the day. This finding comes from a new study by researchers at the University of Warwick and Bielefeld University, published in the journal Scientific Reports. Participants reported feeling significantly happier and more enthusiastic on those mornings compared with other days at the same hour when they had not yet had coffee.
Links to negative moods such as sadness and feeling upset were also observed, though these effects were less pronounced: after drinking coffee, participants felt slightly less sad or upset than on comparable days without coffee. Unlike the boost in positive emotions, this effect was not dependent on the time of day.
In total, 236 young adults in Germany were studied over a period of up to four weeks. Participants completed short questionnaires on their smartphones seven times a day, indicating their current mood and whether they had consumed a caffeinated drink in the preceding 90 minutes. Accordingly, the study focused on caffeine consumption in everyday life, not just in artificial laboratory settings.
Perceived effect regardless of consumption habits
The researchers also investigated whether coffee has different effects on different individuals. Justin Hachenberger from the Bielefeld University in Germany says, ‘We were somewhat surprised to find no differences between individuals with varying levels of caffeine consumption or differing degrees of depressive symptoms, anxiety, or sleep problems. The links between caffeine intake and positive or negative emotions were fairly consistent across all groups.’
The researchers expected that people with higher levels of anxiety would experience negative mood changes, such as increased nervousness, after consuming caffeine. However, Hachenberger emphasises that people who react to caffeine in a bad way may avoid it and that the study did not include people who completely abstain from caffeine.
Role of caffeine withdrawal symptoms remains unclear
The researchers explain the mood-boosting effect of caffeine on morning mood with its ability to block adenosine receptors, which promotes wakefulness and makes people feel more energetic. ‘Caffeine works by blocking adenosine receptors, which can increase dopamine activity in key brain regions – an effect that studies have linked to improved mood and greater alertness’, says Professor Anu Realo from the University of Warwick.
Yet, it remains unclear whether these effects are related to a reduction in withdrawal symptoms after a night’s sleep. ‘Even people with moderate caffeine consumption can experience mild withdrawal symptoms that disappear with the first cup of coffee or tea in the morning’, says Anu Realo.
Caffeine consumption: a universal habit
‘Around 80 per cent of adults worldwide consume caffeinated beverages, and the use of such stimulating substances dates far back in human history’, says Professor Sakari Lemola from Bielefeld University, the study’s senior author. ‘Even wild animals consume caffeine; bees and bumblebees prefer nectar from plants that contain caffeine.’
Still, the study authors caution that caffeine can lead to dependence. Excessive intake is linked to various health risks, and consuming it later in the day can lead to sleep problems.
Paracetamol (acetaminophen) is one of the most common painkillers and is found in hundreds of different medications. While safe at recommended doses, paracetamol overdose is the leading cause of acute liver injury in the U.S. Now, researchers propose that a new molecule has the potential to treat acetaminophen-induced liver injury (AILI) and other inflammatory conditions. They conducted a small-scale mouse trial and found that the new compound decreased AILI-caused liver inflammation and prevented liver damage.
Jannatun Nayem Namme, a graduate student at Virginia Commonwealth University, will present her team’s results at the fall meeting of the American Chemical Society (ACS). ACS Fall 2025 is being held Aug. 17-21; it features about 9000 presentations on a range of science topics.
Most acetaminophen overdoses are accidental, often due to people unintentionally consuming multiple products containing the painkiller or misinterpreting dosage. After taking a recommended amount of paracetamol, a person’s liver converts a small percentage of it into a toxic molecule called N-acetyl-p-benzoquinone imine (NAPQI). Normally, the liver can quickly metabolise NAPQI into a non-toxic form. But if a person takes too much acetaminophen, NAPQI builds up and causes irreversible cell damage, leading to liver injury or death. Currently, N-acetylcysteine is the only drug available to treat AILI, and it must be administered within eight hours of overdose.
To develop novel treatments for inflammatory conditions, such as AILI, and neurodegenerative conditions, Namme and her colleagues previously focused on small molecules that reduce the activity of inflammation-causing proteins, known as inflammasomes. Inflammasomes are also involved in pyroptosis, a type of cellular death associated with AILI. While developing inflammasome inhibitors, the researchers noticed that some of the compounds they created could target a specific inflammatory protein called gasdermin D (GSDMD). GSDMD is involved in pyroptosis.
Namme and the team synthesised several different GSDMD-inhibiting compounds and tested them for their ability to bind to GSDMD. They discovered that one small molecule, which they labelled YM81, selectively binds to and inhibits GSDMD from initiating pyroptosis.
Next, the researchers treated five mice with AILI using YM81 and compared them to 10 mice given a placebo. They monitored the extent of liver damage in the animals 17 hours after the acetaminophen overdose. Compared to the placebo group, mice treated with YM81 had significantly lower levels of alanine transaminase and aspartate transaminase, two liver injury biomarkers. These results indicate that the YM81 treatment helped decrease liver inflammation by inhibiting GSDMD.
Shijun Zhang, the study’s principal investigator, says that YM81 is in the early stages of drug development. “In the future, we will focus on optimising YM81 to increase its potency, safety and stability, in addition to exploring its therapeutic potential in additional animal models,” he says.
Namme adds that GSDMD inhibitors like YM81 have the potential to treat other inflammatory conditions. “GSDMD is a common protein involved in multiple inflammatory and neurodegenerative diseases, such as arthritis, sepsis and gout,” she says. “Targeting GSDMD could offer a therapeutic strategy to reduce the inflammation and damage from multiple diseases and causes.”
A new article published in the Canadian Medical Association Journal warns of the mental health dangers stemming from the increasing potency of cannabis. In Ontario, there has been a more than 14-fold increase in risk for visiting the emergency department for cannabis-related schizophrenic disorders. After a cannabis-induced psychotic episode, cessation of cannabis use is necessary to reduce the risk of relapse, and in severe cases, antipsychotics may be needed.
“Cannabis from the 2000s is not the same as in 2025,” said coauthor Dr Nicholas Fabiano, MD, resident and researcher with the Department of Psychiatry, University of Ottawa, Ottawa, Ontario. “THC content has increased by 5 times. This is likely a significant driver in the increasing link between cannabis use and schizophrenia.”
Cannabis potency is increasing — The concentration of tetrahydrocannabinol (THC) has increased fivefold in the last 20 years in Canada from about 4% to 20% in most legal dried cannabis.
High-potency and regular cannabis use is linked to increased risk of psychosis — The risk of psychosis is increased in people using high-potency THC (more than 10% THC), people using it frequently, and those who are younger and male. A history of mental disorders (depression, anxiety, etc) also appears to increase the risk.
Cannabis-induced psychosis and cannabis use disorder increase the risk of schizophrenia — A recent study of 9.8 million people in Ontario found a 14.3-fold higher risk of developing a schizophrenia-spectrum disorder in people visiting the emergency department for cannabis use and a 241.6-fold higher risk from visits for cannabis-induced psychosis.
Treatment requires stopping cannabis and taking medication — Continued use of cannabis after a first episode of cannabis-induced psychosis is linked to greater risk of returning symptoms. Antipsychotic medication can help people with severe and prolonged symptoms.
Behavioural options may help with cannabis cessation — Motivational interviewing or cognitive behavioural therapy by a physician or psychologist can help build skills to resist cravings and follow treatment recommendations.
South Africa is facing a major health transition. While the average life expectancy has nearly doubled over the past century, the quality of those additional years, commonly referred to as one’s ‘healthspan,’ remains under threat from non-communicable diseases (NCDs). This threat calls for a renewed national focus on prevention and early intervention to address the rapidly growing challenge.
The Healthspan Imperative
According to health data presented at the 2025 Momentum Healthcare Insights Summit, NCDs such as heart disease, cancer, diabetes and neurodegenerative disorders now account for 51% of all deaths in South Africa. In contrast, communicable diseases make up around 40% and non-natural causes (like accidents and violence) account for a mere 9%. This shift reflects a global trend, although some challenges remain; infectious diseases become more manageable, while chronic conditions associated with lifestyle and ageing take centre stage.
Damian McHugh, Chief Marketing Officer at Momentum Health
“Medical advances have added years to our lives, but not necessarily life to our years. More and more, there is growing evidence to support the fact that prevention offers the greatest potential to reduce the burden as well as cost of chronic disease and improve quality of life,” says Damian McHugh, Chief Marketing Officer at Momentum Health.
Prevention Outperforms Treatment
The summit highlighted compelling evidence that prevention is more effective than treatment for advanced disease. For example, research from the American Cancer Society shows that tobacco control measures, such as smoking bans and taxes, have prevented 3.8 million lung cancer deaths in the United States since 1970. The most effective way to save lives from late-stage lung cancer has not been through treatment, but through reducing or eliminating smoking altogether.
The same principle applies to other chronic diseases. Managing risk factors such as high blood pressure, obesity, high blood glucose, and abnormal cholesterol can actively prevent or delay the onset of disease. These factors are strongly influenced by behaviours such as a lack of physical activity, poor nutrition, unmanaged stress levels, and even excessive alcohol use or smoking.
Investing in regular health check-ups and preventative care can mitigate the risk of serious health problems, ultimately reducing the incidence of costly, advanced illnesses. Simple lifestyle changes, such as prioritising rest and recovery, making time to connect with loved ones, maintaining balanced nutrition, practicing mindfulness, and engaging in regular exercise not only promotes physical and mental health, but can also translate into significant long-term savings in healthcare costs.
“Making quality healthcare more accessible, while enabling and rewarding healthy, preventative habits can lead to complete physical and mental health and wellbeing. Investing in access and wellbeing is a powerful pathway to realising more wealth and more health for more South Africans,” says McHugh.
Measuring and Managing Healthspan within the South African Context
Momentum Health’s data reveals that many South Africans are living longer, but the average age of medical scheme beneficiaries has increased by nearly three years over the past decade, and the proportion of pensioners in medical schemes is rising. Without proactive measures, our nation’s ailing healthcare system will face increasing claims and costs as the population ages and chronic diseases become more prevalent.
Momentum Health believes that the solution lies in taking measures to improve access to both quality medical care and reliable health information and empowering individuals to take responsibility for their own health.
South Africa’s rising NCD burden is not inevitable. With early detection, healthy lifestyle choices, and consistent engagement with preventative healthcare, individuals can not only extend their lifespan but also improve the years lived in good health.
“Prevention isn’t just a personal choice; it’s a public health imperative. By investing in wellness now, we can reduce the future burden on our healthcare system and help more South Africans enjoy longer, healthier lives,” concludes McHugh.
He speaks in measured tones – calm, reflective, deliberate. But when Dr Dumisani Bomela describes the future he envisions, the words carry power. For the CEO of the Hospital Association of South Africa (HASA), healthcare is not just a profession. It is a promise rooted in dignity, equity and access to every South African.
Q: Dr Bomela, what drew you to medicine and what keeps you committed to healthcare in South Africa? A: I have always seen healthcare as an act of service. As a doctor, you learn to see beyond symptoms, to understand the person behind the diagnosis. As a leader at HASA, I take that same approach. Our work is about people. About making sure that every South African can get quality care when they need it.
Q: HASA represents South Africa’s private hospital sector. Why is this sector important to the country’s overall health system? A: Private hospitals are a cornerstone of healthcare in South Africa. We treat millions of patients each year. More than that, HASA members invest heavily in medical training, advanced technology and infrastructure. We are strategic partners in the national system, that makes our sector a vital national asset.
Q: How does HASA contribute to economic development beyond just healthcare? A: Healthcare is a growth engine. HASA members are major employers, from doctors and nurses to technicians and support staff. We support local communities and stimulate investment. When healthcare systems are strong, economies thrive – and so do people.
Q: What is HASA’s stance on universal health coverage? A: We believe every person has the right to choose their provider and to receive high-quality care. That is why we support reforms that strengthen the system and build equity. HASA members are ready to work side by side with the government to make that vision a reality. Our hospital groups bring deep experience, including in some cases from geographies where universal healthcare systems operate, and strong infrastructure to the table.
Q: What kind of leadership do you believe is needed in South African healthcare today? A: We need leaders who listen. Who understand not just policy, but people. Leadership in healthcare must be grounded in compassion and collaboration. At HASA, we strive to lead by example, building trust, fostering partnerships, and always remembering that every system ultimately affects human lives.
Q: How do HASA hospitals stay at the forefront of medical technology and innovation? A: By investing intentionally. Our members understand that modern medicine is not static, it is constantly evolving. We equip our hospitals with advanced diagnostic and treatment tools. But technology alone is not enough. We also invest in people – training nurses, specialists and support teams to lead with excellence.
Q: In a country facing complex health challenges, how do you stay hopeful? A: Hope grows where there is action. Across our hospitals, I see incredible work being done every day – surgeons saving lives, nurses comforting families, teams innovating to improve care. We are proving, together, that with collaboration and commitment, South Africa’s health system can be strong, inclusive and world-class.
Q: What gives you the greatest sense of pride in your work with HASA? A: Honestly, it is seeing the impact private hospitals have. When families walk out of our hospitals healed. When professionals grow into health leaders. When communities feel their well-being is supported. These outcomes remind us why the work matters. My pride does not come from titles; it comes from knowing we are making a real, human difference every single day.
Many diseases affect men and women differently. Asthma tends to strike men earlier in life, yet more women develop asthma as they get older. Parkinson’s is more common in men, but Alzheimer’s is more common in women.
The differences are even more stark when it comes to autoimmune disease. Women are around two and a half times more likely than men to develop multiple sclerosis and nine times more likely to develop lupus.
Why would some diseases strike one sex more than another? And why do some tissues, such as the lungs and brain, seem especially vulnerable to these sex-based differences?
To answer these questions, scientists at La Jolla Institute for Immunology (LJI) are leading new research into how our immune cells defend specific parts of the body.
“In just the last two years, LJI scientists have uncovered a whole new body of information about how the immune systems of men and women are very different,” says Saphire. “We’re looking at what is genetically encoded in our XX or XY chromosomes, and how hormones like oestrogen and testosterone affect what is genetically programmed into our immune cells.”
In the paper, the researchers define biological sex (in an immunology context) as the presence of XX chromosomes in females and XY chromosomes in males. “Every cell in your body is either XX or XY,” says Saphire. “That X chromosome has many, many immune-related genes. Women have two copies of each. That gives them, in a sense, twice the palette of colours to paint from in formulating an immune response. It can also give them a stronger immune response for those genes that are doubly active – active in both copies simultaneously.
Sex hormones are important for much more than reproductive function. Immune cells can also sense hormones such as oestrogen and testosterone and use them to determine which genes to turn on or off and which ones to turn on more brightly or dim. This means similar immune cells can do different things, depending on whether that cell is from a male or a female.
Further, female cells vary in which of their two copies of X is “turned on.” As a result, women have organs with a collage, or mosaic, of immune cells that work differently in different tissues. This innate “variety” of immune cells appears to be an effective way to ward off infectious disease (women are better than men at fighting off pathogens such as SARS-CoV-2).
But scientists have also found that having more genes from X chromosomes may predispose women to autoimmune disease. This increased X chromosome “dosage” is closely linked to a higher risk for autoimmune diseases such as Sjögren’s syndrome and scleroderma.
New research into sex-based immune system differences is also critical for developing new cancer immunotherapies, Sharma explains.
“We’re increasingly understanding how sex-based differences affect disease outcomes. When it comes to medicine, one size doesn’t fit everybody,” says Sharma, who directs LJI’s Center for Sex-Based Differences in the Immune System. “This is leading to new research, particularly in the cancer field, toward precision medicine. We’re asking how a person’s individual immune system is contributing to controlling that cancer through immunotherapy.”
Saphire and Sharma also highlight environmental factors, such as nutrition and chemical exposures, that may add to the complex interplay of chromosomes and sex hormones. Men and women also appear to have some signature differences in their skin and gut microbiomes.
The researchers hope these foundational discoveries can lead to medical advances for all, and they’re working with collaborators across the country to move this research forward. “It takes a team to translate these findings,” says Sharma.
In response to US funding cuts for South African health services and research projects, National Treasury has provided the National Department of Health with hundreds of millions of rands in emergency funds. Spotlight and GroundUp look at how precisely the government intends to spend this money.
Health Minister Dr Aaron Motsoaledi recently announced that National Treasury had released roughly R753 million to help plug the gap left by US funding cuts to South Africa’s health system. Another R268 million is also being released in the following two years for researchers that lost their US grants.
But this may only constitute the first round of emergency funds from government, according to sources we spoke to. The health department is planning on submitting a bid for an additional allocation later on, which will be considered by Treasury. But this will likely only be approved if the first tranche of funding is properly used.
So how is the money supposed to be used? To find out, we spoke with officials from the National Treasury, the National Department of Health and the South African Medical Research Council (SAMRC).
Money for provinces is for saving jobs at government clinics
The current tranche of money comes from Treasury’s contingency reserve, which exists partially to deal with unforeseen funding shortfalls. It was released in terms of Section 16 of the Public Finance Management Act.
Of the R753 million that’s been announced for this year, Motsoaledi stated that R590 million would be going to provincial health departments via the District Health Programme Grant – a conditional grant for funding the country’s public health efforts, particularly HIV, TB, and other communicable diseases. Such conditional grants typically give the health department more say over how provincial departments spend money than is the case with most other health funding in provinces.
To explain how government officials arrived at this figure, it’s worth recapping what services the US previously supported within provinces.
Prior to Donald Trump becoming US president on 20 January, the US Agency for International Development (USAID) had financed health programmes in specific districts with high rates of HIV. These districts were scattered across all South Africa’s provinces, save for the Northern Cape.
The funds were typically channelled by USAID to non-governmental organisations (NGOs), which used the money to assist the districts in two ways.
The first is that NGOs would hire and deploy health workers at government clinics. The second is that the NGOs would run independent mobile clinics and drop-in centres, which assisted so-called key populations, such as men who have sex with men, sex workers, transgender people, and people who inject drugs.
In response, the health department began negotiations with Treasury to get emergency funding to restore some of these services. As part of its application, the health department submitted proposals for each province, which specified how much money was needed and how it would be used. (Though this only took place after significant delay and confusion).
Since Treasury couldn’t afford to plug the entire gap left by the US funding cuts, the provincial-level proposals only requested money for some of the services that had been terminated. For instance, funding was not requested for the key populations health centres. Instead, the priority was to secure the jobs that had been lost at government health facilities.
As such, the total amount that was requested from Treasury for each province was largely calculated by taking the total number of health workers that NGOs had hired at clinics and working out how much it would cost to rehire them for 12 months.
Rather than paying the NGOs a grant to deploy these workers as was done by USAID, the health department proposed hiring them directly. This meant that they calculated their wages according to standard government pay scales, which is less than what these workers would have earned from the NGOs.
The total came to just under R1.2 billion for all the provinces combined.
Treasury awarded roughly half of this on the basis that the money would be used to finance these wages for six months, rather than 12. This amounts to the R590 million for provinces that was announced by Motsoaledi.
If all goes smoothly and this money is used effectively to hire these staff over the next six months, then a new tranche of Section 16 funding could be released in order to continue hiring them. Funds might also be released to fund the key populations health sites.
A concern, however, is that the money may just be used by provinces to augment their ordinary budgets. If the funds aren’t actually used to respond to the US cuts, then it is much less likely that more emergency funding will be released.
At this stage, it is too early to tell how provinces will use the money, particularly given that it appears that at least some of them haven’t gotten it yet.
Spotlight and GroundUp sent questions to several provincial health departments. Only the Western Cape responded. The province’s MEC for Health and Wellness, Mireille Wenger, said that the funds have not yet been received by her department, but that once they were, they would be directed to several key priority areas, including digitisation of health records, and the strengthening of the primary healthcare system.
It’s thus not clear whether the province will be using any of the funds to employ health staff axed by US-funded NGOs. In response to a question about this, Wenger stated that “further clarity is still required from the National Department of Health and National Treasury regarding the precise provincial allocations and conditions tied to the additional funding”.
What about research?
Of the R753 million that’s been released for this year, R132 million has been allocated to mitigate the funding cuts for research by US federal institutions, primarily the National Institutes for Health (NIH). Unlike USAID, the NIH is not an aid body. It provides grants to researchers who are testing new treatments and medical interventions that ultimately benefit everyone. These grants can be awarded to researchers in the US or abroad as part of a highly competitive application process.
Researchers in South Africa are awarded a few billion rands worth of grants from the NIH each year, largely due to their expertise in HIV and TB. But over the last few months, much of this funding has been terminated or left in limbo. (See a detailed explanation of the situation here).
The R132 million issued by Treasury is supposed to assist some of these researchers. It will be followed by another R268 million over the following two years. The Gates Foundation and Wellcome Trust are chipping in an additional R100 million each – though in their case, the funds are being provided upfront.
All of this money – R600 million in total – is being channelled to the SAMRC, which will release it to researchers via a competitive grant allocation system.
According to SAMRC spokesperson Tendani Tsedu, they have already received the R132 million from Treasury, though they are still “finalizing the processes with the Gates Foundation and Wellcome Trust for receipt of [their donations]”.
The SAMRC is also in negotiation with a French research body about securing more funds, though these talks are ongoing.
In the meantime, the SAMRC has sent out a request for grant applications from researchers who have lost their US money. The memo states: “Applicants may apply for funding support for up to 12 months to continue, wind down or complete critical research activities and sustain the projects until U.S. funding is resumed or alternative funds are sourced.”
“The plan,” Tsedu said, “is to award these grants as soon as possible this year.”
Professor Linda-Gail Bekker, CEO of the Desmond Tutu Health Foundation, told us that the hope is that the grants could fill some of the gaps. “This is a bridge and it is certainly going to save some people’s jobs, and some research,” she said, but “it isn’t going to completely fill the gap”.
Indeed, the SAMRC has made clear that its grants aren’t intended to replace the US funding awards entirely. This is unsurprising given that the money that’s being made available is a tiny fraction of the total grant funding awarded by the NIH.
It’s unlikely that research projects will continue to operate as before, and will instead be pared down, said Bekker.
“It’s going to be about getting the absolute minimum done so you either save the outcome, or get an outcome rather than no outcome,” she said.
In other cases, the funds may simply “allow you to more ethically close [the research project] down,” Bekker added.
For some, this funding may also have come too late. Many researchers have already had to lay off staff. Additionally, patients who had been on experimental treatments may have already been transitioned back into routine care. It’s unclear how such projects could be resumed months later.
In response, Tsedu stated: “For projects that have already closed as a result of the funding cuts, the principal investigator will need to motivate whether the study can be appropriately resurrected if new funds are secured.”
The SAMRC has established a steering committee which will adjudicate bids. They will be considering a range of criteria, Tsedu said, including how beneficial the research might be for the South African health system, and how heavily the project was impacted by the US funding cuts. They will also consider how an SAMRC grant could “be leveraged for future sustainability of the project, personnel or unit”, added Tsedu.
An endless back and forth
The job of the SAMRC steering committee will likely be made a lot more complicated by the erratic policy changes within the NIH. On 25 March, the body sent a memo to staff – leaked to Nature and Bhekisisa – instructing them to hold all funding awards to researchers in South Africa. After this, numerous researchers in the country said they couldn’t renew their grants.
However, last month, Science reported that a new memo had been sent to NIH staff which said that while South African researchers still couldn’t get new grants, active awards could be resumed.
Since then, some funds appear to be trickling back into the country, but certainly not all. For instance, Spotlight and GroundUp spoke to one researcher who had two active NIH awards before the cuts. He stated that one of these was resumed last month, while the other is still paused.
Bekker also told us that she had heard of one or two research grants being resumed in the last week, though she said the bulk of active awards to South Africa are still pending.
“Where people are the prime recipients [of an NIH grant] without a sub awardee, there seems to be a queue and backlog but some [of those awards] are coming through,” said Bekker. “But how long this is going to take and when it might come through, we’re waiting to hear.” She said a strategy might be to apply for the SAMRC bridging funding and “if by some miracle the [NIH funding is resumed]” then researchers could then presumably retract their SAMRC application.
In the meantime, health researchers will have to continue spending their time working out how to respond to the abrupt and increasingly confusing changes to funding guidelines that have dogged them since Trump assumed office.
“It’s such a dreadful waste of energy,” said Bekker. “If we were just getting on with the research, it would be so much better.”
Gait analysis and pain measures show that subtly adjusting the angle of the foot during walking may reduce knee pain caused by osteoarthritis, an approach which may also slow progression of the incurable condition.
Led by a team of researchers at NYU Langone Health, the University of Utah, and Stanford University, a new study explored whether changing the way patients position their feet when walking could lessen extra loading, helping to treat the disease.
For the investigation, the scientists tested this intervention in 68 men and women with mild to moderate knee osteoarthritis and then used advanced MRI scans to track how well it worked.
The results suggest that those trained to angle their feet slightly inward or outward from their natural alignment experienced slower cartilage degeneration in the inner part of their knee compared with those who were encouraged to walk more frequently without changing their foot position. The study is reported online in The Lancet Rheumatology.
“Although our results will have to be confirmed in future studies, they raise the possibility that the new, noninvasive treatment could help delay surgery,” said study co-lead author Valentina Mazzoli, PhD.
Dr. Mazzoli, an assistant professor in the Department of Radiology at NYU Grossman School of Medicine, notes that the earlier patients receive a knee replacement, the more likely they are to require additional procedures in the future.
The findings also revealed that those who adjusted their foot angle reduced their pain score by 2.5 points on a 10-point scale, an effect equivalent to that of over-the-counter pain medications. By contrast, those who did not change their gait reduced their pain scores by little more than a point.
“Altogether, our findings suggest that helping patients find their best foot angle to reduce stress on their knees may offer an easy and fairly inexpensive way to address early-stage osteoarthritis,” added Dr. Mazzoli.
About one in seven Americans have some form of osteoarthritis, commonly in the inner side of the knee, according to the U.S. Centers for Disease Control and Prevention. A leading cause of disability, the disease is often managed with pharmaceutical pain relievers, physical therapy, and in the most severe cases, knee-replacement surgery. Experts believe that excess loading can over time contribute to the condition.
Past research has offered little evidence that changes in gait can effectively reduce knee pain caused by osteoarthritis, says Dr. Mazzoli. Some previous trials trained all participants to adopt the same foot angle and found no relief, while others did not compare the intervention to a control group or only followed the participants for a month.
The new study is the first to show that tailoring each patient’s foot angle to their unique walking pattern can alleviate the disease’s symptoms in the long term and may slow cartilage breakdown, the authors say.
Dr Mazzoli adds that this technique may have a significant advantage over pharmaceutical painkillers. These drugs, she says, do not address the underlying disease and can cause liver and kidney damage, stomach ulcers, and other unwanted side effects when taken for long periods.
For the study, the research team recorded the participants walking on a treadmill at a specialized gait-assessment laboratory. A computer program simulated their walking patterns and calculated the maximum loading that occurred in the inner side of their knees. Next, the team generated computer models of four new foot positions—angled inward or outward by either 5 or 10 degrees—and estimated which option reduced loading the most.
The patients were then randomly divided into two groups. Half were trained in six sessions to walk with their ideal angle, while the other half were instructed to continue walking naturally. Pain scores and MRI scans were taken at the beginning of the study period and one year after the intervention.
Study findings showed those who adjusted their gait reduced the maximum loading in the knees by 4 percent, while those who kept their normal walking pattern increased their loading by more than 3 percent.
“These results highlight the importance of personalizing treatment instead of taking a one-size-fits-all approach to osteoarthritis,” said Dr. Mazzoli. “While this strategy may sound challenging, recent advances in detecting the motion of different body parts using artificial intelligence may make it easier and faster than ever before.”
While the authors relied on a specialized laboratory for the new study, AI software that estimates joint loading using smartphone videos is now available and can allow clinicians to perform a gait analysis in the clinic.
The researchers next plan to test whether these tools can indeed identify the most effective walking method for osteoarthritis patients, says Dr. Mazzoli. They also plan to expand their study to people with obesity.
Discovery could help pave the way for a prosthetic device to restore blink function lost to injury or disease
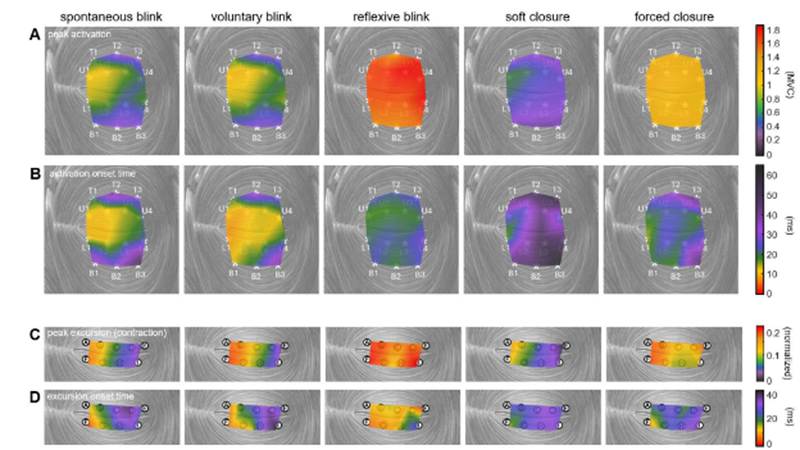
Muscle activation and movement patterns over time across the upper and lower eyelids, shown under different actions. Credit: Anatomical Engineering Group/UCLA
A blink of an eye is vital to protecting the eye by keeping it from drying out. This simple function seems natural and instantaneous, but is it?
Now, a team of UCLA biomechanical engineers and ophthalmologists has uncovered new details about the muscle that controls blinking, offering a pathway toward developing blink-assisting prostheses. Published in PNAS, the study found that the orbicularis oculi – the muscle that controls eyelid movement – contracts in complex patterns that vary by action and move the eyelid in more than just a simple up-and-down motion.
The researchers studied how this muscle behaves differently across various actions including spontaneous blinks, protective rapid closures and squeezed shut-eye motions.
“The eyelid’s motion is both more complex and more precisely controlled by the nervous system than previously understood,” said study corresponding author Tyler Clites, an assistant professor of mechanical and aerospace engineering at the UCLA Samueli School of Engineering. “Different parts of the muscle activate in carefully timed sequences depending on what the eye is doing. This level of muscle control has never been recorded in the human eyelid. Now that we have this information in rich detail, we can move forward in designing neuroprostheses that help restore natural eyelid function.”
In experiments with volunteers, the researchers looked at five different ways the eyes close:
Spontaneous blink: An automatic, unconscious blink that occurs regularly to keep the eye lubricated
Voluntary blink: An intentional blink, as when someone is asked to blink on command
Reflexive blink: A rapid, involuntary blink triggered to protect the eye from a collision
Soft closure: A gentle, slow eyelid descent, similar to the beginning of sleep
A forced closure: A deliberate squeezing of the eyelids tightly shut
To record activity in the orbicularis oculi with high precision, an ophthalmic surgeon inserted tiny wire electrodes into the eyelid. The researchers then used a motion-capture system to track eyelid movement in ultraslow motion. These tools allowed the team to measure subtle differences in eyelid movement, including speed, direction, and which part of the muscle initiated the action.
Video of spontaneous blink – dynamic muscle activation patterns and eyelid kinematics. Credit: Anatomical Engineering Group/UCLA
“People can lose the ability to blink due to a stroke, tumour, infection or injury. The condition is painful in the short term and can damage the eyes enough to cause vision loss,” said study co-author Dr Daniel Rootman, an associate professor of ophthalmology at the David Geffen School of Medicine at UCLA and director of the UCLA Orbital Disease Center. “We know that a small electric pulse can stimulate the orbicularis oculi muscle to move, but designing one that works well has been elusive. What we now have is a good roadmap to such a device, including where exactly to place electrodes, how to time them, and how strong the pulse should be. These guidelines could help pave the way for the development and clinical testing of such a device, with the ultimate goal of providing real relief for patients.”
With this fundamental knowledge of eyelid biomechanics in hand, the researchers can now work on refining a prototype neuroprosthesis to assist people with blinking.
“Understanding how the eyelid works is crucial to designing an accurate stimulation pattern for a prosthesis, as well as for diagnostic purposes,” said study first author Jinyoung Kim, a UCLA mechanical engineering doctoral student and member of Clites’ research group, the Anatomical Engineering Group at UCLA. “We are more than excited to bridge this gap and move forward to work with patients who have facial paralysis and help improve their lives.”