In people with chronic obstructive pulmonary disease (COPD), dysfunctional airway mucus is common. Mucus plugging (mucus that accumulates in the lungs and reduces airflow) and chronic bronchitis are both related to dysfunctional airway mucus. Sometimes mucus plugging and chronic bronchitis co-occur, but it is quite common to have one or the other but not both conditions. Given the limited availability of disease-modifying treatments for COPD, understanding the underlying biology of mucus pathology is critical to identifying new therapeutic targets.
In a new study published in the American Journal of Respiratory and Critical Care Medicine, researchers at Boston University Chobanian & Avedisian School of Medicine have found that mucus plugs in the lungs alter the pattern of gene activity in a way that is similar to chronic bronchitis, suggesting that there may be similar underlying causes to both conditions. It is believed these researchers are the first group to study gene activity differences associated with mucus plugging.
“Mucus plugs are quite common in people with COPD and they are associated with diminished quality of life and increased mortality. By identifying how the presence of mucus plugs impacts the biology of the lung we hope to be able to better treat them, or prevent them from forming in the first place,” says corresponding author Marc Lenburg, PhD, professor of medicine at the school.
The researchers studied participants in the Detection of Early Lung Cancer Among Military Personnel (DECAMP) 2 study who were mostly older US military veterans at high risk for lung cancer due to a history of heavy smoking, many of whom had COPD. Computed tomography was performed on them to determine who had mucus plugs and for those that had them, how extensive they were. From that group, a pulmonologist collected cells from their airways and sequenced the RNA from those cells to determine the level of gene activity. The researchers then compared the gene activity from each individual with the extent of mucus plugging to find genes that had increased (or decreased) activity in individuals with more extensive mucus plugging. Once they had this mucus plugging ‘gene signature’, they compared it with gene signatures from other diseases.
According to the researchers, having a better understanding of how mucus plugging impacts the lung and its relationship to chronic bronchitis may give new clues about how mucus dysfunction develops, which could be helpful for developing new therapies to better treat mucus dysfunction. “By uncovering the molecular pathways that drive mucus plugging and chronic bronchitis, we aim to identify biological targets for earlier diagnosis and intervention. Ultimately, we hope these insights will translate into therapies that restore airway health, reduce respiratory symptoms, and improve the quality of life for people living with these chronic lung diseases,” says coauthor Ehab Billatos, MD, an assistant professor of medicine at the school.
One- and three-month regimens both had few adverse reactions and high rates of completion
Tuberculosis bacteria. Credit: CDC
A study comparing one- and three-month antibiotic treatments to prevent active tuberculosis (TB) finds that a high percentage of patients successfully completed both regimens and suffered few adverse side effects. A team led by Richard Chaisson, of the Johns Hopkins School of Medicine, reports these findings February 10th in the open access journal PLOS Medicine.
Following TB exposure, the World Health Organization has traditionally recommended six to nine months of antibiotic treatment to prevent an active infection from developing, but many individuals fail to complete the long course of medication. Studies have shown that shorter regimens lasting one and three months are effective at preventing TB, but the one-month treatment had only been tested in people living with HIV, and the safety of the two regimens had not been compared in a head-to-head trial.
Researchers performed a clinical trial in 500 people residing in Brazil, who were not living with HIV and had been exposed to TB. They randomly assigned participants to take two antibiotics, isoniazid and rifapentine, daily for one month, or weekly for three months. Both the one- and three-month regimens had similarly high rates of completion, at 89.6% and 84.1%, respectively. Adverse reactions were typically mild or moderate, and occurred at comparable rates in both groups. Both regimens were deemed successful and neither proved superior to the other.
Expanding the number of people who receive preventive therapy is essential for reducing TB infections globally, but these efforts have been hampered by several factors, including the length of the treatments. The new findings provide evidence that a one-month course of antibiotics is safe for patients, regardless of HIV status, and will help clinicians, public health programs, and patients to make informed choices about which regimens to use. Experts hope the success of shorter treatments, combined with the availability of newer generic formulations of the medications, which can be taken at home, will facilitate broader use of preventive therapy for TB.
The authors add, “Prevention of tuberculosis in people at the greatest risk is essential for global control of the disease, and shorter preventive treatment regimens will be instrumental in catalyzing uptake in high-burden countries.”
“Tuberculosis preventive treatment regimens have now been shortened from 6-9 months of daily medication to 1 month of daily treatment or 12 once-weekly doses, a transformational advance. Our study shows that both of the ultra-short regimens are well-tolerated and have high rates of completion.”
“The high rates of treatment completion and excellent safety profile of the short-course regimens will help Brazil and other high-burden countries achieve TB control by facilitating widespread uptake of TB preventive treatment,” states coauthor Betina Durovni.
“Preventing TB with short courses of well-tolerated medicines ensures that millions more people around the world can be protected from the devastating consequences of TB disease,” says coauthor Marcelo Cordeiro-Santos.
Discovery could lead to mRNA therapeutic to reduce the risk of cardiac damage
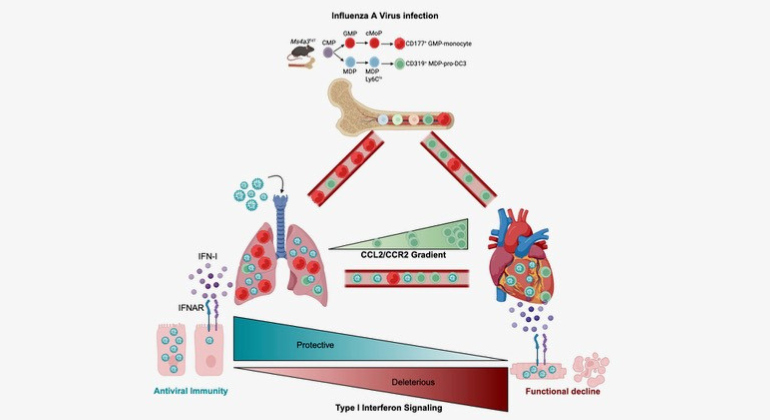
Graphical Abstract summarising the key findings of the paper. The authors found that severe influenza damages the heart by exploiting a specific immune cells and engaging a type-I interferon response. The authors also show that therapeutic silencing of the response mitigates heart damage.
Researchers at Mount Sinai in the US have identified a cellular mechanism linking infections from influenza A viruses (IAVs) to cardiovascular disease, providing critical insights on how influenza can damage the heart and increase the risk of a heart attack or other major cardiovascular event.
Through its work with mouse models and human data, the team also provided evidence that a cutting-edge modified mRNA treatment that dampens an interferon signalling pathway in the heart can significantly mitigate cardiac damage following viral infection while preserving the protective antiviral response of the immune system. The study was published in the February 9 issue of Immunity.
“We have known for years that the frequency of heart attacks increases during flu season, yet outside of clinical intuition, scant evidence exists of the underlying mechanisms of that phenomenon,” says senior author Filip Swirski, PhD, Director of the Cardiovascular Research Institute at the Icahn School of Medicine at Mount Sinai.
“Studies like ours are now shedding valuable light on immune system pathways, like the antiviral cytokine type 1 interferon (IFN-1), that factor into damage to the heart following severe influenza infection. These findings offer great promise for the development of new therapies, which are desperately needed since there are currently no viable clinical options to prevent cardiac damage.”
Influenza A viruses are responsible for an estimated 1 billion infections globally each year, ranging from seasonal flu outbreaks locally to pandemics globally. While most infections are mild and self-resolving, in some cases they can become severe or even fatal, particularly when the virus travels to the heart and triggers the death of cardiomyocytes, specialized muscle cells that are responsible for the rhythmic contraction and relaxation of the heart.
The Mount Sinai team studied autopsies of 35 hospitalised patients who died of influenza and found that more than 85% had at least one significant cardiovascular comorbidity, such as hypertension, and that the majority had multiple comorbidities, including atherosclerosis and cardiac fibrosis, underscoring cardiovascular disease as a major driver of influenza mortality.
The research team also uncovered the mechanism by which cardiac damage occurs. They learned, for example, that a novel subset of white blood cells, known as pro-dendritic cell 3, becomes infected in the lung and, after traveling to the heart, produces large amounts of type 1 interferon. This, instead of fulfilling its mission of clearing the virus from the heart, triggers the death of cardiomyocytes, impairing cardiac output.
“We found that the pro-dendritic cell 3 acts as the ‘Trojan horse’ of the immune system during influenza infection, becoming infected in the lung, trafficking the virus to the heart, and disseminating it to cardiomyocytes. This process causes production of the damaging type 1 interferon that comes with considerable collateral damage to the heart,” explains Jeffrey Downey, PhD, a member of Dr Swirski’s laboratory who served as lead author of the study. “The hopeful news for patients is that by injecting a novel mod-RNA therapeutic that modulates the IFN-1 signaling pathway, we reduced levels of cardiac damage, as evidenced by lower troponin, and improved cardiac function, as measured by higher left ventricular ejection fraction.”
As part of its ongoing research, Dr Swirski’s team is collaborating with Lior Zangi, PhD, Associate Professor of Medicine (Cardiology), and Genetics and Genomic Sciences, at the Icahn school of Medicine at Mount Sinai, to investigate the use of a safe and effective systemic delivery method of the mod-RNA therapeutic to the heart’s muscle cells, instead of the direct injection method used in its proof-of-concept study. Additional work is focused on the pro-dendritic cell 3 itself: why is it so susceptible to influenza and how could its protective capacity be fully harnessed to potentially minimize heart damage exacerbated by cardiovascular disease?
“Pathogens are constantly emerging and evolving, which means our strategies to combat them must evolve as well,” says Dr Swirski. “Better understanding of influenza pathogenesis and immune pathways that are activated throughout the body will help fuel the next stage of advanced care.”
A new test shows promising results for detecting latent tuberculosis infection in resource-limited settings. This is according to a study from Karolinska Institutet, published in the journal Clinical Infectious Diseases.
“This test can help more people with latent tuberculosis to be detected and receive preventive treatment, especially in rural areas in countries with limited resources,” says last author Lina Davies Forsman, a researcher at the Department of Medicine, Solna, Karolinska Institutet.
Tuberculosis remains one of the world’s deadliest infectious diseases. To reduce the number of new cases, infected individuals with latent infection must be detected and offered preventive treatment to avoid active tuberculosis, which can spread the disease to others.
Currently, latent tuberculosis is often diagnosed using a laboratory test called QuantiFERON-TB Gold Plus. This test involves several steps and can take one to two days before the results are available, as well as requiring advanced laboratory infrastructure and trained personnel. This makes it difficult to carry out tests in areas with a high prevalence of tuberculosis where access to laboratories and trained personnel is limited.
Results within 15 minutes
In the new study, researchers from Karolinska Institutet, together with colleagues in Vietnam, have therefore compared this test with another test, TB-Feron. This is a point-of-care test that provides results within 15 minutes and does not require an advanced laboratory or trained personnel.
The study included 345 adult participants in Hanoi, Vietnam, divided into three groups: people with confirmed tuberculosis, people in the same household as people with infectious tuberculosis, and people with no known exposure to tuberculosis. All were tested with both TB-Feron and the established laboratory test QuantiFERON-TB Gold Plus.
The results show that TB-Feron has high sensitivity – 88 percent of individuals with expected positive results were correctly identified. The corresponding figure for QuantiFERON-TB Gold Plus was 92 percent.
However, the specificity, i.e. TB-Feron’s ability to rule out tuberculosis infection in healthy individuals, was moderate at 70 percent. The corresponding figure for QuantiFERON-TB Gold Plus was 96 percent.
Among household contacts, the concordance between TB-Feron and the established test was good, with 92 percent concordance for positive samples.
“It is promising that TB-Feron works so well in an environment with a high disease burden. The test is patient-friendly and easy to use, with rapid same-day results, making it useful in primary care,” says Han Thi Nguyen, pulmonologist and doctoral student at the same department and first author of the study.
The researchers also investigated the reliability of TB-Feron by comparing results from two different groups with laboratory staff. No systematic differences were observed, indicating good reproducibility.
Chronic fatigue syndrome – medically unexplained fatigue lasting six months or more, preventing people from carrying out their normal activities, and often worsening after any exertion – is hard to treat. But new research could offer a lifeline. Chronic fatigue patients appear to be much more prone to disordered breathing than healthy controls, suggesting that chronic fatigue could cause respiratory issues which make patients’ symptoms worse. These findings might lead to new treatments reducing chronic fatigue symptoms by improving patients’ breathing.
Chronic fatigue syndrome leaves patients exhausted and struggling with brain fog – and it typically gets worse after mental or physical exercise, a phenomenon called post-exertional malaise. Now scientists investigating shortness of breath in chronic fatigue patients have discovered that they are highly likely to experience dysfunctional breathing, which could be caused by dysautonomia, abnormal control of innervation to blood vessels and muscles. Targeting treatments towards these breathing problems could potentially offer patients some relief from their symptoms.
“Nearly half of our chronic fatigue subjects had some disorder of breathing – a totally unappreciated issue, probably involved in making symptoms worse,” said Dr Benjamin Natelson of Icahn School of Medicine, senior author of the article in Frontiers in Medicine. “Identifying these abnormalities will lead researchers to new strategies to treat them, with the ultimate goal of reducing symptoms.”
Breathe easy
The scientists recruited 57 patients diagnosed with chronic fatigue syndrome and 25 control participants whose ages and activity levels matched the chronic fatigue cohort. Both groups took part in cardiopulmonary exercise tests over two days. The scientists measured their heart rate and blood pressure, how effectively they were taking in oxygen, the oxygen saturation of their blood, and how hard they had to breathe to get enough oxygen. They also tracked how fast participants breathed and the patterns of their breathing, to identify hyperventilation and dysfunctional breathing.
Dysfunctional breathing is usually associated with asthma patients, but it can arise from many different causes. Characteristics include deep sighing in the course of ordinary breathing, overly rapid breathing, forcing your exhale from your abdomen, breathing from your chest without using your diaphragm so your lungs are never properly full, and a loss of synchrony between your chest and abdomen, so the different muscles which help you breathe aren’t working together.
“While we know the symptoms generated by hyperventilation, we remain unsure what symptoms may be worse with dysfunctional breathing,” said Dr Donna Mancini of the Icahn School of Medicine, first author of the article. “But we are sure patients can have dysfunctional breathing without being aware of it. Dysfunctional breathing can occur in a resting state.”
The scientists found that participants with chronic fatigue were taking in approximately the same amount of oxygen when they breathed compared to the control participants — their peak VO2 maxes were comparable. However, 71% of the participants with chronic fatigue experienced breathing problems — either hyperventilation, dysfunctional breathing, or both.
Almost half of the participants with chronic fatigue were observed breathing erratically during the test, compared to only four of the control participants. A third of the chronic fatigue patients hyperventilated, compared to just one control participant. Nine chronic fatigue patients displayed dysfunctional breathing as well as hyperventilation. None of the control participants had this combination of breathing issues. Both dysfunctional breathing and hyperventilation can cause symptoms similar to chronic fatigue, like dizziness, difficulty focusing, shortness of breath and exhaustion. Combining the two can also cause people to experience heart palpitations, chest pain, fatigue, and (unsurprisingly) anxiety. These breathing problems, the scientists suggest, could be exacerbating chronic fatigue symptoms or even directly contributing to post-exertional malaise.
“Possibly dysautonomia could trigger more rapid and irregular breathing,” said Mancini. “It is well known that chronic fatigue syndrome patients often have dysautonomia in the form of orthostatic intolerance, which means you feel worse when upright and not moving. This raises the heart rate and leads to hyperventilation.”
Pulmonary physiotherapy?
This could mean that tackling dysfunctional breathing would relieve some patients’ symptoms. The scientists intend to follow up on this research to learn more about how dysfunctional breathing and hyperventilation interact. Although more research will be needed before treatments can be rolled out, they already have ideas for possible therapies that could improve breathing function.
“Breathing exercises via yoga could potentially help, or gentle physical conditioning where breath control is important, as with swimming,” suggested Natelson. “Or biofeedback, with assessment of breathing while encouraging gentle continuous breath use. If a patient is hyperventilating, this can be seen by a device that measures exhaled CO2. If this value is low, then the patient can try to reduce the depth of breathing to raise it to more normal values.”
Case Western Reserve University researchers say discovery of new inflammatory molecules could transform treatment
For decades, scientists have thought they understood the biochemical machinery that causes asthma: inflammation in the lungs that constricts airways and makes it hard to breathe. Leukotrienes – molecules that get released from white blood cells due to airway irritation or allergen inhalation – were labelled the culprits. Medications have been developed to block the molecular cascade they initiate that leads to difficulty breathing.
“We’ve found molecules that are alike in structure but generated through a completely different chemical pathway in the body,” said lead researcher Robert Salomon, the Charles Frederic Mabery Professor of Research in Chemistry. “We think the molecules we’re calling ‘pseudo leukotrienes,’ may be the dominant players in the inflammatory cascade that causes disease.”
The research opens new avenues for treating asthma as well as other inflammatory diseases, possibly including neurological diseases like Parkinson’s and Alzheimer’s diseases. The research, funded by the U.S. National Institutes of Health, is available online as a pre-proof ahead of publication in the Journal of Allergy and Clinical Immunology.
The ‘flames’ of oxidation
The presumed culprits in inflammatory diseases – the leukotrienes – are formed under the control of enzymes that transform lipids. By contrast, the pseudo leukotrienes Salomon and his team discovered, are formed by adding oxygen to lipids by molecules called “free radicals.”
“The free radical process is almost like an explosion or a fire,” said Salomon, who is also professor of ophthalmology in the Case Western Reserve School of Medicine. “It’s just like when oxygen reacts with fuel and you get flames. It can easily get out of control.”
People who suffer from asthma may lack enzymes and antioxidant molecules that normally keep a damper on free radicals by scavenging for and destroying them.
The leukotrienes and their mimics initiate inflammation by fitting into a receptor, like a key in an ignition, starting a molecular cascade that constricts the airways of asthmatics. Effective asthma drugs like Singulair block the ignition so the key won’t fit.
“The real importance of this discovery is the possibility of treating these diseases with drugs that prevent the free radical process or moderate it rather than drugs that block the receptor,” Salomon said.
Inflammation: a curse or a benefit?
Not all inflammation is harmful. The body needs inflammation to direct white blood cells to the site of a wound to heal, and it is also involved in memory and development.
Asthma drugs are being repurposed off-label to treat neurological diseases. But these treatments could also block the beneficial effects of the leukotrienes.
“If the molecules that are causing the problem are not the leukotrienes but these other molecules,” Salomon said, “a better treatment would be to just stop the formation of these other molecules rather than gumming up the ignition.”
The study
Salomon and his colleagues used their decades of experience studying the oxidation of lipids – and some chemical intuition – to guess that pseudo leukotrienes existed. They made the molecules in the laboratory to develop methods to detect them.
They obtained urine samples from patients designated with mild or severe asthma and compared them to urine from people who don’t suffer from the disease.
Not only were pseudo leukotrienes found in the asthma patients’ urine, but also the amounts correlated directly to the severity of the disease. Severe asthma sufferers or even those suffering mild asthma had four to five times more than the controls. The researchers suggest this could be a new biomarker to test for the severity of disease and monitor the effectiveness of therapies.
The researchers next plan to investigate whether these pseudo leukotrienes are involved in other respiratory diseases, like respiratory syncytial virus (commonly known as RSV) and bronchiolitis in babies, and chronic obstructive pulmonary disease.
Researchers from University of Maryland Schools of Public Health and Engineering in College Park and the School of Medicine in Baltimore wanted to find out how the flu spreads, so they put college students already sick with the flu into a hotel room with healthy middle-aged adult volunteers. The result? No one caught the flu.
“At this time of year, it seems like everyone is catching the flu virus. And yet our study showed no transmission – what does this say about how flu spreads and how to stop outbreaks?” said Dr Donald Milton, professor at SPH’s Department of Global, Environmental and Occupational Health and a global infectious disease aerobiology expert who was among the first to identify how to stop the spread of COVID-19.
The study, out in PLOS Pathogens, is the first clinical trial in a controlled environment to investigate exactly how the flu spreads through the air between naturally infected people (rather than people deliberately infected in a lab) and uninfected people. Milton and his colleague Dr Jianyu Lai have some ideas about why none of the healthy volunteers contracted the flu.
“Our data suggests key things that increase the likelihood of flu transmission – coughing is a major one,” said Lai, post-doctoral research scientist, who led data analysis and report writing for the team.
The students with the flu had a lot of virus in their noses, says Lai, but they did not cough much at all, so only small amounts of virus got expelled into the air.
“The other important factor is ventilation and air movement. The air in our study room was continually mixed rapidly by a heater and dehumidifier and so the small amounts of virus in the air were diluted,” Lai said.
Lai adds that middle-aged adults are usually less susceptible to influenza than younger adults, another likely factor in the lack of any flu cases.
Most researchers think airborne transmission is a major factor in the spread of this common disease. But Milton notes that updating international infection-control guidelines requires evidence from randomised clinical trials such as this one. The team’s ongoing research aims to show the extent of flu transmission by airborne inhalation and exactly how that airborne transmission happens.
The lack of transmission in this study offers important clues to how we can protect ourselves from the flu this year.
“Being up close, face-to-face with other people indoors where the air isn’t moving much seems to be the most risky thing – and it’s something we all tend to do a lot. Our results suggest that portable air purifiers that stir up the air as well as clean it could be a big help. But if you are really close and someone is coughing, the best way to stay safe is to wear a mask, especially the N95,” said Milton.
The team used a quarantined floor of a Baltimore-area hotel to measure airborne transmission between five people with confirmed influenza virus with symptoms and a group of 11 healthy volunteers across two cohorts in 2023 and 2024. A similar quarantine set-up was used in an earlier study and exhaled breath testing was used in several pioneering studies by Milton and colleagues on influenza transmission.
During the most recent flu study, participants lived for two weeks on an isolated floor of the hotel, and did daily activities simulating different ways that people gather and interact – including conversational ice-breakers, physical activities like yoga, stretching or dancing. Infected people handled objects such as a pen, tablet computer and a microphone, before passing the objects among the whole group.
Researchers measured a wide range of parameters throughout the experiment, including participant symptom monitoring, daily nasal swabs and saliva samples and blood collection to test for antibodies. The study measured the viral exposure in volunteers’ breathing area as well as the ambient air of the activity room. Participant exhaled breath was also measured daily in the Gesundheit II machine, invented by Milton and colleagues at Harvard T.H. Chan School of Public Health.
Finding ways to control flu outbreaks is a public health priority, says Milton. Flu is responsible for a considerable burden of disease in the United States and globally – up to 1 billion people across the planet catch seasonal influenza every year and this season has seen at least 7.5 million flu cases so far in the United States alone, including 81 000 hospitalisations and over 3000 deaths.
President Cyril Ramaphosa addresses the nation in 2021 on developments in the country’s response to the COVID-19 pandemic. (Photo: GCIS)
By Janet Giddy
South Africa had several “family chats” in which President Cyril Ramaphosa addressed the nation during the height of the COVID-19 pandemic. He should do the same for tuberculosis, argues Dr Janet Giddy of the advocacy group TB Proof.
Recently, I was flying home and got chatting to the stylishly dressed woman in the window seat next to me. We asked each other the sort of questions that traveller’s often do. Suzie (name changed) was going to Cape Town to facilitate an artist’s workshop. I told her that I worked for an NGO that did tuberculosis (TB) research and advocacy. Suzie nodded pensively, then said: “My dad had TB”. I was just thinking how to respond, when she added: “he died from it”.
I have conversations about TB almost every day, and have previously written about high-altitude chats with fellow travellers. I get into these conversations not because TB work is my “day job” – which it is – but because I am a TB activist, and a survivor of childhood TB.
There are many remarkable things about TB that keep me engaged, enraged and activated. For example, that 29 934 people were diagnosed with TB in 2024 in the Cape Town metro, which was more than the combined number diagnosed with TB in the whole of the United States (10 347), the United Kingdom (5 480), France (4 217), and Canada (1 258). The population of these four countries combined is over 500 million, while Cape Town has a population of just under five million people. If you do the math, the risk of getting TB clearly depends massively on where you live. If these figures do not shock you, they should.
Why are so many people in South Africa unaware and seemingly unconcerned about the extraordinarily high numbers of people infected with TB in our country? Could we take TB more seriously as a country? My answer is yes.
If COVID-19, why not TB?
As expected, South Africa worked up a huge head of steam at every level of society about COVID-19. I think back on President Cyril Ramaphosa’s regular avuncular “family chats” to the nation. In the first COVID-19 “family chat”, our president told us:
“This is a decisive measure to save lives of South Africans from infection and save the lives of hundreds of thousands of our people. While this measure will have a considerable impact on people’s livelihoods, and on the life of our society and on our economy, the human cost of delaying this action would be far, far greater.”
Why has Ramaphosa not ever spoken in this intimate “family style” way to the nation about how important or urgent it is to tackle TB? A disease which continues to cause significantly more suffering and death than COVID-19 did.
In 2018, our president spoke to the international world about TB, when he addressed the President of the General Assembly of the United Nations (UN) and Director-General of the World Health Organization at the first ever UN High-Level Meeting on Tuberculosis. With great gravitas and in oratorial style, Ramaphosa said: “This … is a historic opportunity that we must embrace if we are to effectively respond to a disease that has killed more people than smallpox, malaria, the plague, influenza, HIV and AIDS, and Ebola combined. This meeting is taking place in the year of the centenary of the birth of South Africa’s founding President, Nelson Mandela. President Mandela was a survivor of tuberculosis, which he contracted while in prison, and was firmly committed to the campaign against the disease.”
Ramaphosa went on to highlight the social determinants of TB, including poverty, unemployment, poor nutrition, overcrowding and social stigma that fuel the spread of diseases. He also noted: “In South Africa, TB is the biggest cause of mortality in the general population, especially among men.”
This was an excellent message, but since 2018, our president has not had much to say about TB in public or to South Africans. It would be powerful and impactful if he were to talk about TB as a national emergency that requires a coordinated “family response” as a nation.
In considering the seriousness of TB as compared to COVID-19, let’s look at mortality.
By November 2022, the official number of deaths recorded as being due to COVID-19 in South Africa was around 102 000, approximately 34 000 per year when averaged out. Official numbers are however widely considered to be an underestimate. The Medical Research Council estimated in the region of 300 000 excess deaths relating to COVID-19 from 2020 to 2022, with around 85 000 in 2020, 200 000 in 2021, and around 15 000 a few months into 2022. Not all of these excess deaths would have been directly due to COVID-19, but it is likely that over 80% was (say 240 000 over the three years).
By comparison, TB has in recent years been claiming between 50 000 and 70 000 lives per year, based on estimates from the World Health Organization (WHO) and the Thembisa mathematical model. Thus, while there were many more COVID-19 deaths in 2021 than there were TB deaths, TB deaths almost certainly surpassed COVID-19 deaths in 2022 and subsequent years. The more one zooms out, the more the steady torrent of TB deaths over the last five, 10, 20 years, dwarfs the spike in COVID-19 deaths around 2021.
‘We are all at risk’
Back to my recent high-altitude chat in the plane: somehow, it was a uniquely South African sort of conversation. What is the chance that, while cruising at 10 000 meters over the Atlantic on a flight between the United States and France, that you’d sit next to someone whose parent recently died of TB? An extremely small chance. So, I would contend that all South Africans do need to know about TB, which is a disease that affects families profoundly.
It’s time for South Africa to have family chats about TB. There are many reasons to have these chats, starting with the fact that we are all at risk of getting it, given that we live in a country with a high TB prevalence – it was estimated that 389 people per 100 000 in South Africa fell ill with TB in 2024. We could compare this with the 2024 figures for the United Kingdom, at 9.7 per 100 000, which is higher than the United States’ rate of 3.2 per 100 000. For those who are interested, you can look up the latest numbers for different countries on the WHO’s excellent TB data portal.
The bottom line is that the higher the TB prevalence in the country you live in, the more chance that you or a family member could get TB. This is because it is caused by a bacteria which is transmitted through the air via talking, singing and coughing, so anyone can breathe it in – as was the situation (and therefore, panic) with Covid. The mode of transmission is the main similarity between TB and COVID-19 – there are lots of differences.
While some people are more at risk of getting TB, anyone can get TB, from any background. As a recent example: in 2024 Anna (name changed), a professional woman who lived in a green leafy suburb, was referred to me by her GP. Anna was shocked and outraged that she had been diagnosed with TB: “Janet, I feel as if I have been infected with a third world plague”. Anna wanted to believe that she had been infected with TB on a visit to India 18 months previously, but together we traced back her potential exposure and worked out she most likely was infected six months earlier, by a family member in a care home. Because Anna and her GP did not think about TB, it took more than a month of her coughing, losing weight and having no energy and taking several courses of antibiotics, before the diagnosis was finally made. By this time, she was very unwell, and her family members and many clients were at risk of getting TB.
Anna’s experience highlights how stigmatised TB still is as a disease. Stigma is a challenge to people from all backgrounds, and there are different reasons for it. Talking about TB more openly is one way to reduce stigma.
As with many other diseases, the earlier TB is diagnosed, the better the chance of full recovery, with no residual lung damage. There is effective medication to treat TB, and although treatment typically takes 6 months, it is not lifelong unlike chronic diseases like diabetes, hypertension and HIV. Young children with uncomplicated lung TB take medication for 4 months only.
Recent TB guidelines recommend that all close contacts of people diagnosed with TB (usually family or household members) should be tested for TB (even if they don’t have symptoms), and if they test negative, they can be offered TB preventive treatment (TPT), which will protect them against getting active TB disease. There is also more “user friendly” TPT now available, which consists of taking medication once a week for 3 months – a total of 12 doses only. Counselling people with TB needs to be family focused, given these new developments.
So, my challenge to readers is to have regular intentional conversations about TB with family and friends, with colleagues, in airplanes, and while waiting in queues.
Keely, a young women who read a previous Spotlight article I wrote, said she was amazed to discover that her colleague was very anxious because her mother was being treated for TB. If Keely had not decided to talk about TB at work, she would not have been able to offer her colleague support.
Try having a conversation about TB in the next week and see what comes of it.
*Giddy is a consultant at the TB advocacy group TB Proof.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
First study to use worn face masks as a passive tool to monitor indoor air
Photo by Daniel Eledut on Unsplash
According to a new Northwestern University study, the ambient air on aeroplanes and in hospitals mostly contains harmless microbes typically associated with human skin.
In the first study of its kind, scientists used an unexpected sampling tool – used face masks and an aircraft air filter – to uncover the invisible world of microbes floating in our shared air. Their results revealed that the same types of harmless, human-associated bacteria dominate both aeroplane and hospital air.
Across all samples, the team detected 407 distinct microbial species, including common skin bacteria and environmental microbes. While a few potentially pathogenic microbes did appear, they were in extremely low abundance and without signs of active infection.
Not only does the study help illuminate what microbes exist in shared air, but it also demonstrates that face masks and air filters can be repurposed as non-invasive, cost-effective tools to monitor confined, high-traffic environments.
“We realized that we could use face masks as a cheap, easy air-sampling device for personal exposures and general exposures,” said Northwestern’s Erica M. Hartmann, who led the study. “We extracted DNA from those masks and examined the types of bacteria found there. Somewhat unsurprisingly, the bacteria were the types that we would typically associate with indoor air. Indoor air looks like indoor air, which also looks like human skin.”
An expert on indoor microbiomes, Hartmann is an associate professor of civil and environmental engineering at Northwestern’s McCormick School of Engineering.
A second life for used face masks
Hartmann and her team conceived the project in January 2022, amid the COVID-19 pandemic. At the time, travellers became increasingly concerned with how well aircraft cabins filtered and circulated air. Hartmann received a grant to collect aircraft cabin filters to look for evidence of pathogens.
Although Hartmann did procure an aircraft’s high-efficiency particulate air (HEPA) filter, which had been used for more than 8000 flight hours, she quickly realised the project might be impractical.
“At the time, there was a serious concern about Covid transmission on planes,” Hartmann said. “HEPA filters on planes filter the air with incredibly high efficiency, so we thought it would be a great way to capture everything in the air. But these filters are not like the filters in our cars or homes. They cost thousands of dollars and, in order to remove them, workers have to pull the airplane out of service for maintenance. This obviously costs an incredible amount of money, and that was eye opening.”
Searching for another method that passively traps microbes, Hartmann and her team pivoted to a much cheaper and much less disruptive tool: face masks. For the study, volunteers wore face masks on both domestic and international flights. After landing, they put the masks into sterile bags and sent them to Hartmann’s lab. For comparison, Hartmann also collected face masks that volunteers took on flights but never wore.
To understand how indoor environments differ, Hartmann and her team wanted to examine another high-traffic, enclosed environment with heavily filtered air. The team selected hospitals as the second testbed. After wearing a face mask during a shift, hospital workers submitted their masks to Hartmann’s lab.
“As a comparison group, we thought about another population of people who were likely wearing masks anyway,” Hartmann said. “We landed on health care providers.”
The sky is clear
After receiving masks from travellers and health care workers, Hartmann’s team collected DNA from the outsides of masks. They found the air in hospitals and in aircraft contains a diverse but mostly harmless mix of microbes, with only minimal traces of potentially pathogenic species.
In both environments, common human-associated bacteria – especially those found on skin and in indoor air – dominated the samples. Although the abundance of each microbe present was slightly different, the microbial communities from hospitals and aeroplanes were highly similar. The overlap suggests that people themselves – rather than the specific environment – are the main source of airborne microbes in both settings. And those microbes floating around indoor air come from people’s skin, not from illness.
Hartmann’s team also identified a handful of antibiotic resistance genes, linked to major classes of antibiotics. While these genes do not indicate the presence of dangerous microbes in the air, they highlight how widespread antibiotic resistance has become.
Although indoor air might not be as harmful as some people may have feared, Hartmann emphasises that airborne spread is just one way infections can travel. For many common illnesses, other routes – such as direct contact with an infected individual or interacting with high-touch surfaces – are far more important.
“For this study, we solely looked at what’s in the air,” Hartmann said. “Hand hygiene remains an effective way to prevent diseases transmission from surfaces. We were interested in what people are exposed to via air, even if they are washing their hands.”
The study, published in the journal Microbiome, was supported by the Walder Foundation.
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
By Elri Voigt
From studies of new medicines and a mask used to diagnose TB, there was no shortage of interesting findings presented at the recent Union World Conference on Lung Health, held in Copenhagen, Denmark. Spotlight rounds up six studies that stood out.
1. People do better if we dispense all TB prevention pills at once
One of the most important questions in TB is how to best prevent people from getting ill if they’ve been exposed to the bug. While effective treatments to prevent TB disease in people who have been exposed exist, uptake has generally been poor.
Now, researchers have found that, dispensing all the pills in a three-month course of TB preventive Therapy (TPT) at once, instead of asking people to collect pills at the clinic every few weeks, led to many more people completing the treatment course.
The study, called ThiPhiSA, was conducted in four clinics and communities in KwaZulu-Natal. 268 households who qualified to receive TPT were enrolled in the trial. 301 participants from these households were randomised to one of two arms, explained Dr Adrienne Shapiro, Assistant Professor of Global Health and Infectious Diseases at the University of Washington.
In the first arm, 159 people were given a two-week supply of the standard of care 3HP (consisting of the drugs isoniazid and rifapentine, taken once a week for 3 months). They then had to go to clinic to receive their refills as per the clinic schedule. They received weekly sms reminders to take their pills and were visited by researchers at month one and two and at the end of the study.
In the second arm, 142 people were given all the pills for the full three-month course of 3HP at once. While no clinic visits were required, they were remotely registered at their clinics just in case they had to visit the clinic. This group also got weekly sms reminders to take their pills and were visited at month one and two and at the end of the study.
Whether people had taken their pills was assessed through self-reporting, as well as a calendar dosing diary, pill count and assessment of urine colour change if the visit was on a day when the participant had recently taken a dose of 3HP.
For those who had to go to the clinic at regular intervals to collect their pills, only 28% completed their treatment course. By contrast, 86% of those who had the full course dispensed at once completed their treatment.
Much of the difference was due to the fact that some people in the prior group simply did not go to the clinic every time to collect pills. There was also a drug stockout at one of the clinics – which somewhat skewed the results in favour of the latter group, but not enough so to change the fact that people were more likely to complete treatment if they got all the pills at once.
Dispensing a full course of TPT at once was safe, according to Shapiro, with no serious adverse events seen in the study.
“Multi-month delivery of TPT is safe, and person-friendly approaches improving the convenience of TPT should be adopted to decompress health facilities and improve TPT coverage to meet TB prevention goals,” she concluded.
2. A new medicine might help shorten TB treatment
Much TB research in recent years have focussed on reducing the duration of TB treatment – it typically takes six months. In addition, researchers have also been looking for medicines that have fewer side effects. Growing resistance to some existing TB drugs is also a concern.
One of the big talking points at this year’s conference was data on an experimental new drug called sorfequiline. It is thought that sorfequiline could be a replacement for bedaquiline, arguably the most important TB drug developed in recent decades. This is because sorfequiline appears to be more potent than bedaquiline and because of worries over TB strains that are resistant to bedaquiline.
The new data is from a phase 2 trial of sorfequiline used in combination with two other TB drugs – pretomanid and linezolid – to treat drug susceptible TB. The regimen is called SpaL for short. 309 participants with newly diagnosed TB were either given the standard of care first-line drugs isoniazid, rifampicin, pyrazinamide, and ethambutol (HRZE) for 26 weeks, the BPaL regimen consisting of the drugs bedaquiline, pretomanid and linezolid for 26 weeks (not all drugs in these first two arms are taken for the entire period), or one of three different doses – 25mg, 50mg or 100mg – of sorfequiline along with linezolid and pretomanid for 8 weeks.
Once those in the sorfequiline arms completed the initial 8-week course, they had to take the drugs isoniazid and rifampicin (HR) for another 7 weeks and were then tested for TB again. Meaning at this point they had gotten treatment for 15 weeks (or around 3 and a half months). If they tested negative and had no TB symptoms, they could stop treatment. But if they tested positive for TB and had symptoms then they’d have to continue taking isoniazid and rifampicin.
Among the participants who got sorfequiline, 64% in the 100mg arm were able to stop treatment after 15 weeks, compared to 46% in the 50mg arm, and 28% in the 25mg arm.
Study participants gave regular sputum samples that were tested for the presence of TB bacteria. The researchers then estimated the probability of a “stable sputum culture conversion at week 8”. In simple terms, this means the researchers wanted to find out what the probability is that all the TB bacteria had been killed by the different regimens after 8 weeks of treatment.
For the 25mg arm, there was 31% stable culture conversion, in the 50mg arm 48%, and in the 100mg arm 59%. For both HRZE and BPaL it was 45%. In other words, 100mg of sorfequiline plus pretomanid and linezolid showed better stable sputum culture conversion after eight weeks than HRZE, the regimen currently used to treat drug-susceptible TB in South Africa and most other countries.
“[W]e believe that SPaL is a promising four-month regimen,” said Dr Morounfolu Olugbosi, the medical lead for the study, which is being conducted by the non-profit TB Alliance.
The regimen was well tolerated at all dose levels, according to Olugbosi, with no difference in safety signals in the sorfequiline arm compared to the other treatment arms. “So that lack of observable difference is what we consider positive news,” he said.
While this trial looked at people with drug susceptible TB, the research team will be investigating how well it works for drug resistant TB in an upcoming phase 3 study, said Dr Maria Beumont, the Chief Medical Officer at TB Alliance, during a press conference.
Indeed, while these phase 2 results are promising, the real test for this drug will be in the larger phase 3 study to come.
3. Co-morbidities are really important when people have TB
A prospective cohort study in South Africa looked at the burden of co-morbidities and the impact it has on TB mortality. The researchers followed around 2 000 adults with pulmonary TB, diagnosed with Gene Xpert (a molecular TB test), and looked at mortality rates for 1 896 of those people after 15 months. Of those, 272 people (14.3%) had passed away during the study duration.
According to the study presenter, Dr Greta Wood, a Clinical Research Fellow in Infectious Diseases at the University of Liverpool, the prevalence of TB multimorbidity among the whole study group was 86%. Meaning most had TB as well as another illness or risk factor.
The researchers looked at five key co-morbidities identified by the World Health Organization (WHO) – HIV, smoking, undernutrition, diabetes and alcohol use. “These five key comorbidities alone explained over half of the mortality that we saw in this cohort,” Wood said.
The researchers found that the more co-morbidities a person had, the higher their risk of dying was when they got ill with TB. The risk of dying for someone with TB was 19% if they had three or more co-morbidities compared to 16% if they had two, and 11% if they had no co-morbidities.
The key conditions driving mortality in this group of people with TB is HIV and undernutrition. Undernutrition in particular was flagged in the study, as in this setting it was responsible for around one in five TB deaths in people under the age of 40, according to Wood.
“[I]n this cohort, we didn’t find an association between diabetes, smoking, alcohol and mortality, but that has been demonstrated in other settings,” she added.
This data should lead to urgent action, concluded Wood, saying that “to reduce the risk of death, we need to urgently start operationalising screening for these key five TB comorbidities and linking people into treatment”.
4. Point-of-care testing leads to people starting treatment faster
As shown in several studies at this year’s conference, the details of how TB services are delivered can make a significant difference to TB outcomes.
One such study, led by researchers from the University of Cape Town (UCT), explored whether it made a difference if someone had a TB test done at a mobile van, or had their sputum sample collected and sent off to a lab. In other words, the study was indirectly testing whether it makes a difference if someone gets a test result right after testing, versus having to wait a day or two to be contacted with a result.
The study, of over 7 000 people, was conducted in South Africa, Zambia, Zimbabwe, and Mozambique. Around half of those screened in the study were at high risk for TB and randomised to either receive point of care testing on a GeneXpert machine in a mobile van or centralised GeneXpert testing at a laboratory.
In the point of care arm, results were available for 1 641 people, and of those 55 (3.3%) had microbiologically confirmed TB. While 67 (4.1%) of the 1 632 tested in the centralised testing arm had microbiologically confirmed TB. Overall, across both arms, 93 of the people diagnosed with TB (76%) were successfully linked to care.
“When compared to those who had their Xpert performed at a central laboratory, those who had their Xpert done at point of care had a 43% lower probability of treatment initiation failure and initiated treatment twice as fast,” said Tahlia Perumal, a researcher at UCT, who presented the results. Participants in the point of care arm on average started treatment four days sooner than those whose TB tests were done in a centralised laboratory.
“[T]here is an argument to be made about the clinical significance of a four-day reduction. We are in the process of doing transmission modelling to be able to provide more granular details about the difference this may make in active case finding models in larger population sizes,” she said.
5. Promising signs for a portable TB test
In the above study, point-of-care testing was done in a relatively large machine in a mobile van. We may however be able to go much smaller.
Tessa Mochizuki, a Research Scientist at University of California in San Francisco, presented results from a multi-country study evaluating how accurate a portable, battery-operated testing device, called MiniDock MTB, was at diagnosing TB from sputum swabs and tongue swabs.
“The test is run on a small device about the size of my hand, and results are available in under 30 minutes, often even faster for positive results,” Mochizuki said.
1 380 people, aged 12 years and older with presumptive TB were enrolled across seven countries – South Africa, India, Nigeria, the Philippines, Uganda, Vietnam, and Zambia. Sputum samples from all participants were tested using two MIDGIT cultures (a test in which the bug will grow if present), smear microscopy (where the bug is looked for under a microscope), and GeneXpert Ultra (a molecular test).
Results from these tests were then compared with results from the MiniDock MTB machine.
For the tongue swab test, a healthcare worker runs a swab over the participants tongue for 30 seconds, then it is put into a buffer liquid, mounted on a testcard which is run through the portable machine. For the sputum swab, a swab is dipped into a test tube that contains sputum for about 15 seconds, put into a buffer liquid and mounted onto a testcard and run through the portable machine.
When comparing sputum swabs results to the Xpert Ultra results there was not a statistically significant difference, according to Mochizuki, as sputum swabs showed 87% sensitivity compared to GeneXpert Ultra’s 89%. Sensitivity is a measure of how likely the test is to detect a bug if the bug is present in the sample.
Tongue swabs performed a bit worse with 81% sensitivity. This was however much better than the 62% with microscopy. Microscopy is rarely used for TB diagnosis in South Africa, but this finding could be important in other countries where health systems haven’t switched as fully over to molecular testing as we’ve done here.
All sample types and tests achieved 98% specificity. Specificity is an indication of how likely a test is to give a negative result if the bug being tested for is not present in the sample.
These findings meet the WHO target product profile requirements – a minimum of 85% sensitivity and 98% specificity for sputum tests and a minimum of 75% sensitivity and 98% specificity for non-sputum tests.
“We submitted this data to the WHO guideline development group that convened last week, and we look forward to news on any official recommendations in the coming year,” Mochizuki said. “These results show that we can achieve high accuracy with a low-complexity platform, bringing molecular testing closer to people seeking care without sacrificing performance.”
6. A mask that can help diagnose TB
An even more interesting idea that some researchers have been working on is to use a diagnostic mask to diagnose TB.
At this year’s conference, Dr Rouxjeane Venter, a researcher based at the Clinical Mycobacteriology and Epidemiology (CLIME) research group at Stellenbosch University, presented a proof-of-concept study testing whether a mask, called the Avelo Mask, can be used to diagnose whether TB bacteria is present in the air a person breathes out.
58 adults, across four clinics in Cape Town, who had TB symptoms and tested positive for TB on a molecular test were given the mask to wear for 45 minutes. The filter in the mask is able to trap tiny particles from .3 micrometers and above – meaning it can trap viruses and bacteria. This filter is then pushed into a buffer tube using a sample stick – where it can be stored or tested directly. The mask as well as the stick and buffer tube are part of the Avelo mask kit developed by Avelo Diagnostics. For this study, the researchers used a qPCR test – a rapid test that looks for TB DNA – to detect TB bacteria.
When the mask filters were tested, 34 people were found to be negative for TB bacteria and 24 were positive. When compared to their Xpert Ultra sputum results, it was found that there were two false positives.
Overall, according to Venter, the mask had a sensitivity of 71% when compared to GeneXpert Ultra and 65% when compared to the Microbiological Reference Standard and a specificity of about 92%.
People with higher bacillary loads – meaning lots of bacteria – in their sputum were more likely to be positive, but there was still a large percentage of participants with low or very low bacillary loads that were picked up by the mask.
These numbers aren’t nearly as good as those for the MiniDock MTB, but it is positive that masks like these are showing promise. A long-standing problem in TB diagnosis is that not everyone can produce sputum samples. The more alternatives we have, be it tongue swabs or masks, the better.