UCSF researchers discover that oestrogen can turn on pain signals associated with conditions like irritable bowel syndrome.
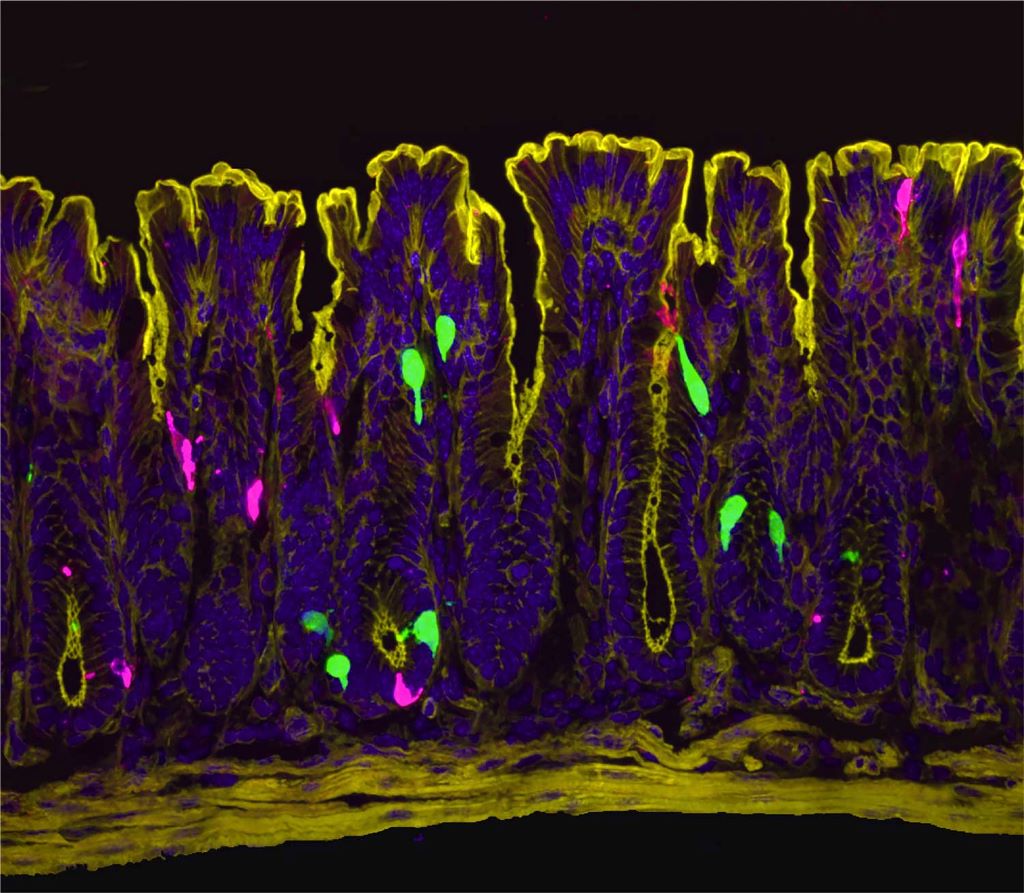
A zoomed in image of the lining of the colon. Cells that produce the hormone PYY (peptide YY) are in green. Cells that produce the neurotransmitter serotonin are in magenta. PYY triggers the release of serotonin, which activates pain-sensing nerve fibers. Image by Archana Venkataraman/UCSF
Women are dramatically more likely than men to suffer from irritable bowel syndrome (IBS), a chronic condition causing abdominal pain, bloating, and digestive discomfort. Now, scientists at UC San Francisco have discovered why.
Oestrogen, the researchers report in Science, activates previously unknown pathways in the colon that can trigger pain and make the female gut more sensitive to certain foods and their breakdown products. When male mice were given oestrogen to mimic the levels found in females, their gut pain sensitivity increased to match that of females.
The findings not only explain the female predominance in gut pain disorders but also point to potential new ways to treat the conditions.
“Instead of just saying young women suffer from IBS, we wanted rigorous science explaining why,” said Holly Ingraham, PhD, professor UCSF and co-senior author of the study. “We’ve answered that question, and in the process identified new potential drug targets.”
The research also suggests why low-FODMAP diets – which eliminate certain fermentable foods, such as onions, garlic, honey, wheat, and beans – help some IBS patients, and why women’s gut symptoms often fluctuate with their menstrual cycles.
“We knew the gut has a sophisticated pain-sensing system, but this study reveals how hormones can dial that sensitivity up by tapping into this system through an interesting and potent cellular connection,” said co-senior author David Julius, PhD. Julius won the 2021 Nobel Prize for Physiology or Medicine for his work on pain sensation.
Search for oestrogen
Previous research had hinted that oestrogen was to blame for higher rates of IBS in females, but not why. To understand how oestrogen might be involved, Ingraham’s and Julius’s teams first needed to see exactly where the hormone was working in the gut.
“At the time I started this project, we didn’t know where and how oestrogen signalling is set up in the female intestine,” said Archana Venkataraman, PhD, a postdoc in Ingraham’s lab and co-first author of the research. “So, our initial step was to visualise the oestrogen receptor along the length of the female gut.”
The team expected to see oestrogen receptors in enterochromaffin (EC) cells, which were already known to send pain signals from the gut to the spinal cord. Instead, they got a surprise: oestrogen receptors were clustered in the lower part of the colon and in a different cell type known as L-cells.
The scientists pieced together a complex chain reaction that occurs when oestrogen binds to the L-cells. First, oestrogen causes L-cells to release a hormone called PYY (peptide YY). PYY then acts on neighbouring EC cells, triggering them to release the neurotransmitter serotonin, which activates pain-sensing nerve fibres. In female mice, removing the ovaries or blocking oestrogen, serotonin, or PYY dramatically reduced the high gut pain observed in females.
For decades, scientists believed PYY primarily suppressed appetite – drug companies even tried developing it as a weight-loss medication. But those clinical trials failed due to a troubling side effect that was never fully explained; participants experienced severe gut distress. The new findings mesh with this observation and suggest a completely new role for PYY.
“PYY had never been directly described as a pain signal in the past,” said co-first author Eric Figueroa, PhD, a postdoc in Julius’ lab. “Establishing this new role for PYY in gut pain reframes our thinking about this hormone and its local effects in the colon.”
This video shows what happens to the enterochromaffin (EC) cells in the colon when they are treated with PYY. Upon PYY treatment, calcium activity increases in the EC cell, causing it to fluoresce more brightly as it releases serotonin that is detected by nearby pain-sensing nerve fibres. Video by Eric Figueroa/UCSF
A link between IBS and diet
Increased PYY wasn’t the only way that L-cells responded to oestrogen. Levels of another molecule, called Olfr78, also went up in response to the hormone. Olfr78 detects short-chain fatty acids – metabolites produced when gut bacteria digest certain foods. With more Olfr78 receptors, L-cells become hypersensitive to these fatty acids and are more easily triggered to become active, releasing more PYY.
“It means that oestrogen is really leading to this double hit,” said Venkataraman. “First it’s increasing the baseline sensitivity of the gut by increasing PYY, and then it’s also making L-cells more sensitive to these metabolites that are floating around in the colon.”
The observation may explain why low-FODMAP diets help some IBS patients. FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are carbohydrates that gut bacteria ferment into those same fatty acids sensed by Olfr78. By eating fewer FODMAPs, patients may be preventing the activation of Olfr78, and, in turn, keeping L-cells from churning out more of the pain signalling PYY.
While men have this same cellular pathway, their lower oestrogen levels keep it relatively quiet. However, the pathway could engage in men taking androgen-blocking medications, which block the effects of testosterone and can elevate oestrogen in some cases, potentially leading to digestive side-effects.
The new work suggests potential ways to treat IBS in women and men alike.
“Even for patients who see success with a low-FODMAP diet, it’s nearly impossible to stick to long term,” Ingraham said. “But the pathways we’ve identified here might be leveraged as new drug targets.”
The researchers are now studying how such drugs might work, as well as asking questions about what other hormones, such as progesterone, might play a role in gut sensitivity and how pregnancy, lactation, and normal menstrual cycles affect intestinal function.
A drug mimicking the hormone progesterone has anti-cancer activity when used together with conventional anti-oestrogen treatment for women with breast cancer, a new Cambridge-led trial has found.
In the two-week window that we looked at, adding a progestin made the anti-oestrogen treatment more effective at slowing tumour growth. What was particularly pleasing to see was that even the lower dose had the desired effectRebecca Burrell
A low dose of megestrol acetate (a synthetic version of progesterone) has already been proven as a treatment to help patients manage hot flushes associated with anti-oestrogen breast cancer therapies, and so could help them continue taking their treatment. The PIONEER trial has now shown that the addition of low dose megestrol to such treatment may also have a direct anti-cancer effect.
Around three-quarters of all breast cancers are ER-positive. This means the tumours are abundant in a molecule known as an oestrogen receptor, ‘feeding’ on the oestrogen circulating in the body. These women are usually offered anti-oestrogens, medication that reduces level of oestrogen and hence deprives the cancer of oestrogen and inhibits its growth. However, reducing oestrogen levels can bring on menopause-like symptoms, including hot flushes, joint and muscle pain, and potential bone loss.
In the PIONEER trial, post-menopausal women with ER-positive cancers were treated with an anti-oestrogen with or without the progesterone mimic, megestrol. After two weeks of treatment, those that received the combination saw a greater decrease in tumour growth rates compared to those treated with an anti-oestrogen only.
Although further work is required in larger patient cohorts and over a longer period of time to confirm the findings, researchers at the University of Cambridge say the trial suggests that megestrol could help improve the lives of thousands of women for whom anti-oestrogen medication causes uncomfortable side-effects and can lead to some women stopping taking the medication.
PIONEER was led by Dr Richard Baird from the Department of Oncology at the University of Cambridge and Honorary Consultant Medical Oncologist at Cambridge University Hospitals NHS Foundation Trust (CUH). He said: “On the whole, anti-oestrogens are very good treatments compared to some chemotherapies. They’re gentler and are well tolerated, so patients often take them for many years. But some patients experience side effects that affect their quality of life. If you’re taking something long term, even seemingly relatively minor side effects can have a big impact.”
Some ER-positive breast cancer patients also have high levels of another molecule, known as progesterone receptor (PR). This group of patients also respond better to the anti-oestrogen hormone therapy.
To explain why, Professor Jason Carroll and colleagues at the Cancer Research UK Cambridge Institute used cell cultures and mouse models to show that the hormone progesterone stops ER-positive cancer cells from dividing by indirectly blocking ER. This results in slower growth of the tumour. When mice treated with anti-oestrogen hormone therapy were also given progesterone, the tumours grew even more slowly.
Professor Carroll, who co-leads the Precision Breast Cancer Institute and is a Fellow of Clare College, Cambridge, said: “These were very promising lab-based results, but we needed to show that this was also the case in patients. There’s been concern that taking hormone replacement therapy – which primarily consists of oestrogen and synthetic versions of progesterone (called progestins) – might encourage tumour growth. Although we no longer think this is the case, there’s still been residual concern around the use of progesterone and progestins in breast cancer.”
To see whether targeting the progesterone receptor in combination with an anti-oestrogen could slow tumour growth in patients, Dr Baird and Professor Carroll designed the PIONEER trial, which tested adding megestrol, a progestin, to the standard anti-oestrogen treatment letrozole.
A total of 198 patients were recruited at ten UK hospitals, including Addenbrooke’s Hospital in Cambridge, and randomised into one of three groups: one group received only letrozole; one group received letrozole alongside 40mg of megestrol daily; and the third group received letrozole plus a much higher daily dose of megestrol, 160mg. In this ‘window of opportunity’ trial, treatment was given for two weeks prior to surgery to remove the tumour. The percentage of actively growing tumour cells was assessed at the start of the trial and then again before surgery.
In findings published today in Nature Cancer, the team showed that adding megestrol boosted the ability of letrozole to block tumour growth, with comparable effects at both the 40mg and 160mg doses.
Joint first author Dr Rebecca Burrell from the Cancer Research UK Cambridge Institute and CUH said: “In the two-week window that we looked at, adding a progestin made the anti-oestrogen treatment more effective at slowing tumour growth. What was particularly pleasing to see was that even the lower dose had the desired effect.
“Although the higher dose of progesterone is licenced as an anti-cancer treatment, over the long term it can have side effects including weight gain and high blood pressure. But just a quarter of the dose was as effective, and this would come with fewer side effects. We know from previous trials that a low dose of progesterone is effective at treating hot flushes for patients on anti-oestrogen therapy. This could reduce the likelihood of patients stopping their medication, and so help improve breast cancer outcomes. Megestrol – the drug we used – is off-patent, making it a cost-effective option.”
Because women in the trial were only given megestrol for a short period of time, follow-up studies will be needed to confirm whether the drug would have the same beneficial effects with reduced side-effects over a longer period of time.
The research was funded by Anticancer Fund, with additional support from Cancer Research UK, Addenbrooke’s Charitable Trust and the National Institute for Health and Care Research Cambridge Biomedical Research Centre.
Personalised and precise cancer treatments underpin the focus of care at the future Cambridge Cancer Research Hospital. The specialist facility planned for the Cambridge Biomedical Campus will bring together world-leading researchers from the University of Cambridge and its Cancer Research UK Cambridge Centre and clinical excellence from Addenbrooke’s Hospital under one roof in a brand-new NHS hospital.
More than half of teenage girls experienced heavy bleeding and 40% had an iron deficiency, in a study carried out among girls in upper-secondary schools. The research, led from Lund University in Sweden, also shows that young teenage girls who experience heavy menstrual bleeding – and are therefore at greater risk of iron deficiency – can be identified using a simple questionnaire.
The 2023 study, published in PLOS One, was carried out in two Swedish upper-secondary schools; a total of 394 girls aged 15 and over took part. They responded to questions about menstruation and eating habits and provided blood samples for analysis of blood count (Hb) and iron stores (ferritin). Lund University has previously reported how the research team saw a particularly high risk of iron deficiency and anaemia among those eating a vegetarian or pescetarian diet. Now, researchers have gone further and investigated how the extent of menstruation affects iron deficiency and anaemia.
“We see a lot of young girls who are tired and distracted. Linking that to menstruation or diet is not obvious,” says Moa Wolff, researcher and associate professor at Lund University, specialist physician in general medicine at Region Skåne and the researcher in charge.
Girls with heavy menstruation were three times more likely to have an iron deficiency, with an even higher risk for those who restricted the quantity of meat in their diet.
“Many of them only compare with their own previous experiences without knowing what counts as heavy menstrual bleeding. We also note that many are not aware of the over-the-counter medicines available that reduce the volume of blood,” says Lisa Söderman, gynaecologist and postdoc researcher at Karolinska Institutet who collated the results for the article in question.
SAMANTA questionnaire could be a new tool for school health services
Part of the study evaluated a Spanish questionnaire which asks six questions. This is the first time it has been used in Sweden and the first time it has been tested on teenage girls anywhere, even though it is a validated screening instrument for adult women.
“Based on the answers to the questionnaire, it was possible to clearly identify which secondary school students were at risk of having low iron levels. It is easy to use and could be a valuable tool for school health services and youth clinics or other care healthcare settings where we meet these girls,” says Moa Wolff.
Previous research shows that iron deficiency in young people may affect their energy levels, schoolwork and general wellbeing. Iron stores – Ferritin – form an important component in the formation of red blood cells and is needed for oxygen transport. Therefore, iron deficiency with low ferritin levels can eventually lead to a drop in haemoglobin, which can result in anaemia.
“In the next few years, some of these girls will get pregnant. When that happens, we would like them to have good stores of iron to enable as complication-free a pregnancy as possible, with a successful labour,” says Lisa Söderman.
Over the last 20 years, substance use-related deaths have more than doubled for women of reproductive age. Overdose deaths are now a leading cause of maternal mortality in the US, and in some states, the leading cause.
Still, substantial gaps remain in understanding how different treatment approaches influence the short- and long-term health of mothers and infants, as well as their broader economic impacts over time.
New research published this month in the journal JAMA Pediatrics found that while established medications for opioid use disorder in mothers – buprenorphine and methadone – are both superior and cost saving compared to alternative treatment pathways (naltrexone, medication-assisted withdrawal or no treatment), buprenorphine produced the greatest health gains and cost savings for mothers and infants.
Using a mathematical simulation model, the study projected the health and cost outcomes for pregnant individuals with opioid use disorder and their infants over their lifetime. The economic model captured how treatment decisions during pregnancy can have lasting health and economic consequences, such as risks of preterm birth, that extend from infancy through adulthood and drive substantial downstream health effects and costs. Outpatient buprenorphine emerged as the optimal treatment in most scenarios tested (58%-100%) and in nearly every lifetime scenario that incorporated both mother and infant trajectories (99%). In other words, across thousands of simulations, buprenorphine consistently produced the best health outcomes and lower costs compared to alternative strategies.
The study, led by Ashley Leech, PhD, assistant professor of Health Policy at Vanderbilt University Medical Center, and Stephen Patrick, MD, MPH, O. Wayne Rollins Distinguished Professor of Health Policy and chair of the Department of Health Policy and Management at Emory University, is among the first to compare the short- and long-term health benefits and costs of opioid use disorder treatment for mothers and infants, examining outcomes during pregnancy, postpartum and beyond the infant’s first year of life using simulation modeling.
Existing studies have not examined outcomes beyond the infant’s first year of life. The study used a hypothetical treatment group modeled on known demographic and other social factors to estimate differences in outcomes and cost savings over time for each treatment and population group. The paper found that, although neonatal opioid withdrawal syndrome (NOWS) has received much of the clinical attention as a marker of poor infant health after opioid exposure during pregnancy, preterm birth and low birth weight carry greater morbidity and mortality and played a more significant role in shaping long-term infant outcomes. Notably, buprenorphine, despite its direct association with NOWS, was protective against these critical outcomes.
“Nationwide, we have seen a significant growth of pregnant women with opioid use disorder, but there have not been comprehensive models that evaluate trade-offs of different medications and strategies,” said Patrick. “This study evaluated the trade-offs we face as clinicians – How will medications affect moms and babies? With the evidence we have available, what can we expect years from now? Bottom line, we found that buprenorphine treatment in pregnancy was cost saving and improved outcomes for mothers with opioid use disorder and their babies.”
The researchers emphasised, however, that patient-centred care and patient choice remain essential to sustaining treatment. “While we found that buprenorphine yielded the greatest health gains and was cost saving across all model variations, methadone could still be a viable option for mothers, and at the individual level, it might work better for some,” said Leech, the lead author of the study. “Buprenorphine shows clear benefits for long-term infant outcomes, but it can be more difficult for patients to start and stay on this treatment because, as a partial agonist, it may not feel as strong to those dependent on drugs like heroin or fentanyl. Methadone, by contrast, is often easier for patients to initiate and sustain.
“This is an opportunity to make sure buprenorphine works as well as possible – by ensuring pregnant individuals receive effective doses across trimesters (since they often need higher and increasing amounts for effectiveness compared to nonpregnant patients) and by removing unnecessary Medicaid restrictions.”
The study estimated substantial cost savings to public insurance programmes like Medicaid, finding that treating pregnant individuals this year could save roughly $4 billion in infant-related lifetime costs alone.
“Medicaid is the largest payer for pregnant individuals and those with substance use disorders. Our research shows that treatment is not only effective but also has the potential to generate significant savings for Medicaid, benefiting both mothers and their children’s long-term health,” Leech said.
After birth, moms and babies are required to visit healthcare facilities for essential services like immunisations, postnatal care and HIV testing. Photo by William Fortunato on Pexels
By Elri Voigt
In South Africa, many mothers and their babies have to visit the clinic more than 10 times in the first six months of the postnatal period. Early findings from an ongoing implementation science project suggests we can get this down to five. The hope is that the new approach will also help reduce HIV transmission from mothers to their babies.
Over the last two decades, South Africa has taken huge strides in reducing HIV transmission from mothers to their babies (often called vertical transmission).
Maternal deaths from non-pregnancy-related infections have decreased, because more women are taking HIV treatment, and HIV rates among babies at birth have also gone down. This has all been possible largely because of integrating HIV services with our antenatal services, Dr Jeanette Wessels, of the University of Pretoria’s Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, told delegates at the recent Southern African HIV Clinicians Society (SAHCS) Conference.
However, a closer look at the data shows us that while vertical transmission at or before birth has come down dramatically, HIV transmission in the months after birth remains alarmingly common. This happens particularly when the mother contracts HIV in this period and the virus is then transmitted to her baby before she is diagnosed, or before the virus can be brought under control with antiretrovirals. As Wessels puts it, “our next frontier to tackle is the breastfeeding period”.
During the antenatal period (before birth), pregnant women are offered HIV tests and prevention pills or HIV treatment when they visit clinics for their pregnancy check-ups. However, during the postnatal period (after birth), HIV services are not integrated in the same way. This fragmentation of care after birth is a key driver of vertical transmissions, suggests specialist paediatrician Dr Nthabiseng Serudu-Nageng. The thinking is that the fragmentation and high number of clinic visits makes it less likely that new HIV infections in mothers will be picked up before the virus can be transmitted to their babies and that it makes it less likely that new mothers will take the HIV prevention pills or HIV treatment they might need.
Spotlight previously reported that, according to the latest estimates from Thembisa – the leading mathematical model of HIV and TB in South Africa – of the roughly 7 200 babies who contracted HIV in the country from mid-2023 to mid-2024, only about 2 500 got HIV before or at birth. This means that about 4 700 babies got HIV in the months after birth, and while some of these mothers were on antiretroviral therapy, according to the Thembisa estimates, the majority of mothers had not been diagnosed with HIV yet. Meaning a contributing factor to some of these infections is likely that many of these mothers got HIV after the birth of their babies and were unaware of it.
Wessels told delegates that around 75% of mother-to-child transmission of HIV is happening during breastfeeding, and just over one third (35%) of those are due to new HIV infections in the mother. She added that about 80% of those new infections in babies after birth happen in the first six months.
It is important to realise that in terms of absolute numbers, HIV transmission during the breastfeeding period has gone down, but proportionally more babies are getting HIV after birth, explained Professor Ute Feucht, the Director for the University of Pretoria’s Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies. Feucht is also the Community Paediatrician in the Tshwane District Clinical Specialist Team at the Gauteng Department of Health.
Clinic visits can be halved
To improve care in the postnatal period, researchers in Gauteng have launched an ambitious implementation science project called Sihamba Kunye. Their key idea is that clinic visits for mother and baby can be much better integrated and optimised. This could make it more likely that mother and baby will attend all required clinic visits and get all the healthcare services they need. The project is funded by the Gates Foundation.
During the postnatal period, said Wessels, a mother may have to come to the clinic up to 11 or 12 times in the first six months. This can be to get her baby to the necessary visits for immunisations, as well as family planning, to pick up HIV treatment or prevention pills or postnatal care for herself. Wessels was presenting early observations from the study at the SAHCS conference.
Commenting on this, Feucht, who is the study’s principal investigator, told Spotlight: “That is twice a month, and yes, with a newborn baby!”
To make matters worse, throughout these many visits, mothers and babies are often seen separately, which isn’t optimal since, as Serudu-Nageng pointed out, “whatever affects the mother directly impacts her baby, so integrating their care is essential”. She is the study’s consultant paediatrician.
“One of the biggest challenges mothers face is having to come to the clinic many times in the first six months. This has a huge impact: it affects food security, especially for unemployed mothers, its transport costs, its time away from work or home, and long waiting hours at the facility. Each visit comes with an emotional and financial cost,” said Serudu-Nageng.
“Through the Sihamba Kunye project, we are addressing this [challenge] by aligning and coordinating the mother and baby’s visits so they can be seen together, on the same day and ideally at the same service point,” she said. “This reduces the number of visits, saves time and cost for the mother, eases the workload for the facility because it means less feet through the clinic all while maintaining quality care for both mother and baby.”
By coordinating these different visits, the total number of times a mother and baby might need to go the facility is reduced to only five visits.
How it works
The researchers conducted time-and-motion studies – where industrial engineering students from the University of Pretoria followed patients around with stopwatches to time how long it took them to move through the clinic from arrival to exit. They also conducted interviews with mothers and infant pairs, had consultations with facility managers, and conducted workshops with healthcare workers, as well as created curated resources and tools to assist with the transition to offering integrated care.
Integration of services was classified into two levels, depending how much the services could be streamlined, said Serudu-Nageng. Level two integration means that a mom and her baby are seen on the same day, but at different parts of the facility and likely by different nurses. Level three integration means they are seen together, on the same day, by the same nurse.
“We worked closely with facility managers, sub-district programme managers and clinicians to redesign processes and adapt the model to fit each facility’s realities,” she said.
The time-and-motion studies helped identify bottlenecks and improve the flow and efficacy at the clinics, Serudu-Nageng said. One big time waster was that if a mom comes in with her baby and the healthcare staff only draw baby’s file but later see mom also needs care, she’ll have to go back to get her own file. To resolve this, the project recommends drawing both mom and baby’s files when they visit the facility, regardless of the reason for the visit.
One major component of integrating care, Serudu-Nageng said, was task-shifting. This is to ensure that professional nurses have the time to spend doing clinical consultations with mom and baby together, since their consultation time has essentially doubled. This means designating tasks like checking vital signs, weighing, giving immunisations and vitamin A and deworming to support staff, leaving professional nurses to do tasks only they are qualified to do.
“[T]he professional nurses can be used for other things like clinical decision making and we can rather delegate work that doesn’t require clinical decision making to lower cadres of nurses of staff,” she said. “Together, these efforts have helped facilities streamline workflow, strengthen teamwork and deliver this integrated postnatal care package for both mothers and babies.”
Another thing the researchers did was to compile two important tools that pulled together information from all the relevant national guidelines for primary healthcare – like the HIV, TB, ideal clinic and immunisation guidelines – and putting them together in one place called the the First 1000-day Roadmap. This is used alongside an Integration Wheel that helps nurses coordinate the different visits moms might need to come to the clinic for.
Wessels in her presentation explained that the roadmap has different sections categorised according to the type of visit mom and baby are at the clinic for. She gave the example of the 10-week visit, where babies normally receive some of their key childhood immunisations. One section of the roadmap will include “all the care needed for the mom, her general postnatal care, nutrition, VTP [Vertical Transmission Prevention] and screening like TB screening, STIs, mental health, her contraception and extra care”. The other section will cover all the things the baby will need.
The roadmap is used alongside the Integration Wheel, which is designed like a pregnancy wheel. The front of the wheel can spin to the visit the mom and baby are at the clinic for. “It outlines [among other things] what you do for an HIV positive mom, for an HIV negative mom, what contraception do you get every mom,” Wessels said. At the back, the wheel has information on the different visits mom and baby would still need to come to the clinic for and helps nurses align those visits.
The front of the Integration wheel can be spun to the specific visit mom and baby are at the clinic for and help align their next visits to reduce the number of times they have to come to the facility. Source: Screenshot from Professor Ute Feucht’s presentation on the Sihamba Kunye Project at the 2025 SA AIDS conference.The back of the Integration wheel shows nurses everything they need to do for both mom and baby, depending on their HIV status, baby’s age and mom’s family planning needs and postnatal care. Source: Screenshot from Professor Ute Feucht’s presentation on the Sihamba Kunye Project at the 2025 SA AIDS conference.
With these resources, according to Wessels, nurses at the participating facilities are able to align mom and baby’s visits from their six-day postnatal visit and can reduce those visits to only five in the first six months.
What’s next?
The response to the project has been very positive and created a bit of a “snowball effect”, Feucht said. “The district has actually been asking us, when can we go to the rest [of the clinics in Tshwane]?”
The first phase, she added, was to figure out what is possible in terms of integrating care and how can it be done. “[T]he next step is then taking that toolkit out to the other provinces as well.”
The research team hopes to have several publications showcasing their findings ready to present at key health conferences next year. But they also hope to see the model being more widely used in the future.
“It’s got potential to transform the postnatal period and make it as good as the antenatal period,” Serudu-Nageng said. “[I]ntegrating care and putting the patient at the centre will really, really, be great for outcomes, but for mom and baby as well.”
“Based on my experience, this approach is highly feasible within the broader public healthcare system because it builds on existing structures and staff,” she added. “It is practical and scalable, and we are hopeful that it will serve as a proof of concept for future scale-up across South Africa’s public health system.”
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council and subject to the Press Code.
Nearly one million babies are stillborn in Africa every year. Behind every stillbirth is a mother, a family and a story left untold. Most of these are preventable, many unrecorded, and too often invisible. Each number hides a moment of heartbreak, and every uncounted loss represents a missed opportunity to learn and to act.
As a public health researcher specialising in maternal and newborn health, I have spent the past two decades working on strengthening health systems and quality of care across Africa. My research has focused on understanding how health systems can prevent stillbirths and provide respectful, people-centred care for women and newborns. Most recently, I was part of the team that led a new report called Improving Stillbirth Data Recording, Collection and Reporting in Africa. It is the first continent-wide assessment of how African countries record and use stillbirth data.
The burden of stillbirths in Africa is staggering. Africa accounts for half of all stillbirths globally, with nearly eight times higher rates than in Europe. Even stillbirths that happen in health facilities may never make it into official statistics despite every maternity registry documenting this birth outcome.
Part of the challenge is that there are multiple data systems for capturing births and deaths, including stillbirths, like routine health information systems, civil registration and other surveillance systems. But these systems often don’t speak to each other either within countries or between countries. This data gap hides both the true burden and the preventable causes.
Despite advances in several countries to prevent stillbirths, large gaps remain, especially on data systems. Only a handful of African countries routinely report stillbirth data to the UN, and many rely on outdated or incomplete records. Without reliable, comparable data, countries cannot fully understand where and why stillbirths occur or which interventions save lives.
Strengthening stillbirth data is not just about numbers; it is about visibility, accountability and change. When countries count every stillbirth and use the data for health system improvement, they can strengthen care at birth for mothers and newborns and give every child a fair start in life.
Findings
The report was based on a regional survey of ministries of health. This was followed by document reviews and expert consultations to assess national systems, policies and practices for stillbirth reporting and review.
The report reveals that 60% of African countries have national and sub-national committees responsible for collecting and using stillbirth data, which produce national reports to respective health ministries. But data use remains limited. Capacity gaps, fragmented systems and insufficient funding prevents many countries from translating information into action.
To guide investment and accountability, the report categorises countries into three readiness levels:
Mature systems needing strengthening, such as Kenya, Rwanda and Uganda. These countries have consistent data flows but need more analysis and use.
Partial systems requiring support, where reporting mechanisms exist but are not systematically implemented, like Ghana, Malawi and Tanzania.
Foundational systems still being built, including fragile or conflict-affected countries like South Sudan and Somalia. Here, policies and structures for data collection and use remain absent.
The findings show both progress and persistent gaps. Two-thirds of African countries now include stillbirths in their national health strategies, and more than half have set reduction targets. Nearly all countries report that they routinely record stillbirths through their health sectors using standard forms and definitions, yet these definitions vary widely. Most systems depend on data reported from health facilities. But the lack of integration between health, civil registration and other data systems means that countless losses never enter national statistics.
For example, if a woman delivers at home alone in Mozambique and the baby is stillborn, the loss is only known to the family and community. Without a facility register entry or civil registration notification, the death never reaches district or national statistics. Even when a stillbirth occurs in a health centre, the health worker may log it in a facility register but not report it to the civil registration system. This means the loss of the baby remains invisible in official data.
What this means
Stillbirths are a sensitive measure of how health systems are performing. They reflect whether women can access timely, quality care during pregnancy and at birth. But unlike maternal deaths, which are often a benchmark for health system strength, stillbirths remain largely absent from accountability frameworks.
Their causes, like untreated infections, complications during labour, or delays in accessing emergency caesarean sections, are often preventable. The same interventions that prevent a stillbirth also reduce maternal deaths. These improve newborn survival, and lay the foundation for better health and development outcomes in early childhood.
Accurate data on stillbirths can guide clinical care and direct scarce resources to where they are needed most. When data systems are strong, leaders can identify where and why stillbirths occur, track progress and make informed decisions to prevent future tragedies.
The analysis also highlights promising signs of momentum. Over two-thirds of countries now reference stillbirths in national health plans, an important marker of growing political attention. Several countries are moving from isolated data collection to more coordinated, system-wide approaches. This progress shows that change is possible when stillbirths are integrated into national health information systems and supported by investment in workforce capacity, supervision and data quality.
What’s needed
Africa has the knowledge, evidence and experience to make change happen.
The report calls for harmonised definitions, national targets and stronger connections and data use between the different data sources within and across African countries. Above all, it calls for collective leadership and investment to turn information into impact, so that every stillbirth is counted, every death review leads to learning and no parent grieves alone.
The author acknowledges and appreciates the partners involved in developing the report and the support from the Global Surgery Division at UCT.
Planned birth at term reduces the incidence of pre-eclampsia in women at high risk of the condition, without increasing emergency Caesarean or neonatal unit admission, according to new trial results.
The PREVENT-PE trial, led by researchers from King’s College London and King’s College Hospital NHS Foundation Trust, is the first to find that a strategy of screening for pre-eclampsia risk at 36 weeks of pregnancy, and then offering planned early term delivery according to the mother’s risk, can reduce the incidence of subsequent pre-eclampsia by 30%, compared with usual care.
The trial, funded by the Fetal Medicine Foundation (FMF), also found that the intervention did not increase the rates of birth by emergency Caesarean or neonatal care needs, and there was no evidence of other harms to mother or baby.
Pre-eclampsia is high blood pressure that develops during pregnancy, most commonly at term gestational age. Pre-eclampsia affects 2-8% of pregnancies worldwide and can be life-threatening – there are around 46,000 maternal deaths due to pre-eclampsia each year and around 500,000 foetal or newborn deaths.1
Pre-eclampsia usually develops after 20 weeks of pregnancy, or soon after the baby is born. While aspirin can be taken to significantly reduce the risk of developing pre-eclampsia before 37 weeks of pregnancy, there are no treatments available to reduce risk at term (37-42 weeks).
Building on findings from an earlier data analysis, the PREVENT-PE trial recruited over 8,000 women from King’s College Hospital and Medway NHS Foundation Trusts. Women were randomly allocated into one of two groups: the intervention group (risk assessment for pre-eclampsia, followed by planned early term delivery according to risk) and the control group (usual care at term).
Pre-eclampsia risk was assessed using a model developed by the FMF, which combines maternal demographics and history, with blood pressure, and specific markers in the blood.
Those at high risk of developing pre-eclampsia at term were offered planned birth at 37, 38, 39 or 40 weeks of pregnancy. Women considered to be at low risk received usual care, according to their hospital protocols and UK standards of care.
A 30% reduction in term pre-eclampsia, from 5.6% to 3.9%, is very important. It represents an even greater reduction in the number of pre-eclampsia cases than we can achieve for preterm pre-eclampsia with aspirin.Professor Kypros Nicolaides, founder and chairman of the Fetal Medicine Foundation, and senior author of the paper
This trial took place in busy NHS maternity units serving a highly diverse population, and often socially deprived communities where the burden of pre-eclampsia is greatest. The high level of participation and adherence shows that a personalised, risk-based approach is acceptable, practical, and aligns with what women want from their care. Achieving a 30% reduction in term pre-eclampsia, without increasing emergency Caesarean birth or neonatal admissions, represents a meaningful and reassuring improvement for women, babies, and maternity services.Dr Argyro Syngelaki, Reader in Maternal-Fetal Medicine at King’s College London and co-lead author of the paper
We will soon report on the health economic implications of the trial, as well as the experiences of women and staff who participated, to provide policy-makers with the information that they need to implement the trial intervention within the NHS.Professor Laura A. Magee, Professor of Women’s Health at King’s College London and co-author of the paper
In a discovery that could shift labour and delivery practices around the world, researchers at Michigan State University have found that the effectiveness of oxytocin, used to induce or speed up labour, depends on the time of day it’s administered, especially for patients with gestational diabetes.
The study, published in Molecular Metabolism, combined laboratory research in mice and human cells with a retrospective review of more than 2300 pregnancies. The results were striking. Women whose labours were induced in the early morning to around noon experienced significantly shorter labour durations than those induced around midnight. For patients with gestational diabetes, the timing difference amounted to as much as seven hours.
“Our findings suggest timing isn’t just about scheduling – it can affect how well a patient’s uterus responds to labour-inducing medication,” said Hanne Hoffmann, associate professor of animal science at MSU and lead author of the study.
The science behind the clock
At the centre of the discovery is BMAL1, a key circadian rhythm gene that helps control the body’s biological 24-hour clock. In mice, the researchers showed that BMAL1 helps regulate the oxytocin receptor in the uterus, which is the same receptor that synthetic oxytocin targets to trigger contractions. When the gene was turned off or suppressed, either genetically or through a mouse model of gestational diabetes, oxytocin was significantly less effective at inducing contractions.
“We were able to show that BMAL1 directly controls the oxytocin receptor, which helps explain why time of day changes the drug’s effectiveness,” Hoffmann said. “This is the first study to make that molecular connection in the uterus.”
In human cell experiments, MSU scientists observed a circadian rhythm of contraction responses to oxytocin confirming what had previously only been speculated.
Real-world implications for labor and delivery
The team also analysed labour and delivery records from Sparrow Health System in Lansing, Michigan, focusing on more than 2300 patients who were at least 39 weeks pregnant. Labour duration was compared across different time windows of the day and between patients with and without gestational diabetes.
The shortest labours occurred when induction started between 8 a.m. and noon and the longest when induction began between midnight and 4 a.m. This effect was especially dramatic in patients with gestational diabetes, suggesting reduced oxytocin sensitivity during nighttime hours.
“This isn’t about convenience,” Hoffmann said. “It’s about optimising outcomes. If we can better align medical interventions with a patient’s internal clock, we may improve safety for both mother and baby, while potentially being able to reduce the amount of a drug a woman receives.”
Hoffmann and her team are now expanding their research to a larger cohort to refine the optimal timing of labour induction. “Our ongoing work suggests that factors such as whether a woman has previously given birth and her BMI may further influence oxytocin’s effectiveness,” Hoffmann explained.
“By integrating these considerations with the time of day of drug administration, we can make labour induction safer, faster and more personalised. These simple, evidence-based steps could significantly improve delivery outcomes, lower the rates of caesarean sections and NICU admissions, and strengthen maternal and neonate recovery.”
The next phase of research will include a prospective study in collaboration with labour and delivery units to develop clear, practical guidelines for obstetricians to optimise induction timing. Ultimately, aligning medical care with the body’s natural rhythms has the potential to enhance not only birth outcomes, but the long-term health and well-being of mothers, babies and families – a cornerstone of a healthy and thriving population.
Data analysed by Penn researchers clarifies risks associated with general anaesthesia, giving patients more control over their delivery experience.
Photo by Anna Shvets on Pexels
Regional anaesthesia has long been favoured for caesarean births due in part to concerns about the effects that general anaesthesia may have on newborns during labour and delivery. Powerful societal pressures also push the idea that mothers need to be awake during delivery to witness the first cry and capture the ‘perfect’ birth moment. But for some women who undergo a caesarean birth, the pain can become excruciating, even after they received a spinal or epidural block.
Now, new research from a team at the Perelman School of Medicine at the University of Pennsylvania, finds that general anaesthesia may be a reasonable alternative for many patients. The findings are published today in Anesthesiology, the peer-reviewed medical journal of the American Society of Anesthesiologists.
“No patient should have to experience pain during caesarean section; as an anaesthesiologist, I never want someone to feel forced to choose between their baby’s health and not having to experience the pain of surgery,” said Mark Neuman, MD, MSc, Professor of Anesthesiology and senior author of the study. “Since regional anaesthesia is so widely used, it’s common for patients to feel that a spinal or epidural block is the only safe option for caesarean section. But as our study shows, anaesthesia type during pregnancy does not need to be one-size-fits-all.”
Reducing pain during C-section delivery
The research analysed 30 years’ worth of data from multiple clinical trials, comparing outcomes between general anaesthesia versus spinal or epidural anaesthesia for C-sections. The Penn study found that, while babies born under spinal or epidural anaesthesia had slightly higher Apgar scores than those born under general anaesthesia, the differences were small and not likely to be clinically meaningful.
While the majority of patients experience good outcomes with spinal or epidural block for caesarean delivery, recent studies show that up to one in six patients who receive an epidural or spinal may feel pain during their C-section. These experiences can be traumatic and have lasting emotional impacts.
The findings come amid growing public discourse on caesarean experiences. Recent podcasts and published news stories have featured candid patient accounts of pain under spinal or epidural anaesthesia. “This study equips women with evidence-based context about the use of general anaesthesia during c-section.” said Sarah Langer, MD, a resident in anaesthesiology at the Perelman School of Medicine and lead author the study. “Childbirth is a physically and emotionally demanding process, but we do not want patients to feel like there aren’t options when it comes to their anaesthesia for c-section,”
Broadening evidence-based choices
The study found that babies born under general anaesthesia were slightly more likely to need breathing support immediately after birth, but there was no increase in NICU admissions. The research does not suggest that general anaesthesia should replace regional techniques, but it can be a reasonable option in certain cases.
“For patients who are open to regional anaesthesia, spinal or epidural block remain great first choice options,” Neuman emphasised. “But having conversations with patients about general anaesthesia doesn’t need to be taboo. Patients deserve to know they have options, and our study helps provide the evidence to support those discussions.”
The authors note that most of the trials included in the analysis were conducted outside North America, highlighting the need for more US-based research in this area. They also point to historical barriers in studying women during pregnancy, which have limited the availability of robust data.
An international panel of leading experts on women’s mental health is recommending that postpartum psychosis be recognised as a distinct category of mental illness and classified accordingly within standardised medical coding systems.
The recommendation, published in Biological Psychiatry, follows a comprehensive review of the scientific literature on the illness.
Postpartum psychosis is an acute and severe psychiatric illness that sets in within weeks after delivery. Most women with postpartum psychosis experience severe mood symptoms, including mania, mixed episodes, or depression with psychotic features. Impaired cognition, irritability, and agitation are also common.
The condition is considered a psychiatric emergency and, in most cases, requires hospitalisation of the mother. If left untreated, postpartum psychosis is associated with high risks of suicide and infanticide. However, if it is detected and treated in time, patients respond well to treatment and most women return to their previous functioning.
Despite being one of the most distinct clinical phenotypes in psychiatry, postpartum psychosis is not recognized in the Diagnostic and Statistical Manual (DSM-5) or the International Classification of Disease (ICD), which are used to code diseases and medical conditions for treatment and billing purposes.
The panel, in close collaboration with patient advocacy organisations and key interested partners, recommended classifying postpartum psychosis as a distinct category within the bipolar disorders chapter of the DSM and ICD.
“Postpartum psychosis is the most severe perinatal mental health problem, and yet one that is often misdiagnosed and mismanaged, with severe consequences for women, and their children and families. A proper nosological classification of this disorder is an essential step towards its correct identification and treatment”.Professor Paola Dazzan, Professor of Neurobiology of Psychosis, Vice Dean (International) at King’s IoPPN and a member of the research panel
Due to the risks to the patient and the infant, the rapid escalation of severity, and its severe and sudden course, it is imperative that postpartum psychosis is recognized, diagnosed, and treated as early as possible. To facilitate such care, the panel recommends DSM-5 and ICD-10 include the following criteria for a diagnosis of postpartum psychosis:
The onset of at least one of the following states within 12 weeks of childbirth, lasting at least one week and present most of the day, nearly every day, or any duration if hospitalisation is necessary:
Mania/mixed state
Delusions
Hallucinations
Disorganised speech or formal thought disorder
Disorganised, confusional, or catatonic behaviour
Depression with psychotic features
The episode is associated with an unequivocal change in functioning that is uncharacteristic of the postpartum period.
The disturbance in mood and the change in functioning are observable by others.
The episode is sufficiently severe enough to cause marked impairment in social functioning and in the care of the baby or to necessitate hospitalization to prevent harm to the patient, baby, or others.
“We have been working with the American Psychiatric Association and the DSM steering committee since 2020 to find a solution that will facilitate diagnostic accuracy and the provision of timely and evidence-based treatment to improve the quality of treatment and outcomes for women with postpartum psychosis and to prevent the tragic outcomes of suicide and infanticide. We are committed to continue this work,” concludes Dr Veerle Bergink, Director of the Women’s Mental Health Center at Mount Sinai and first author of the paper.