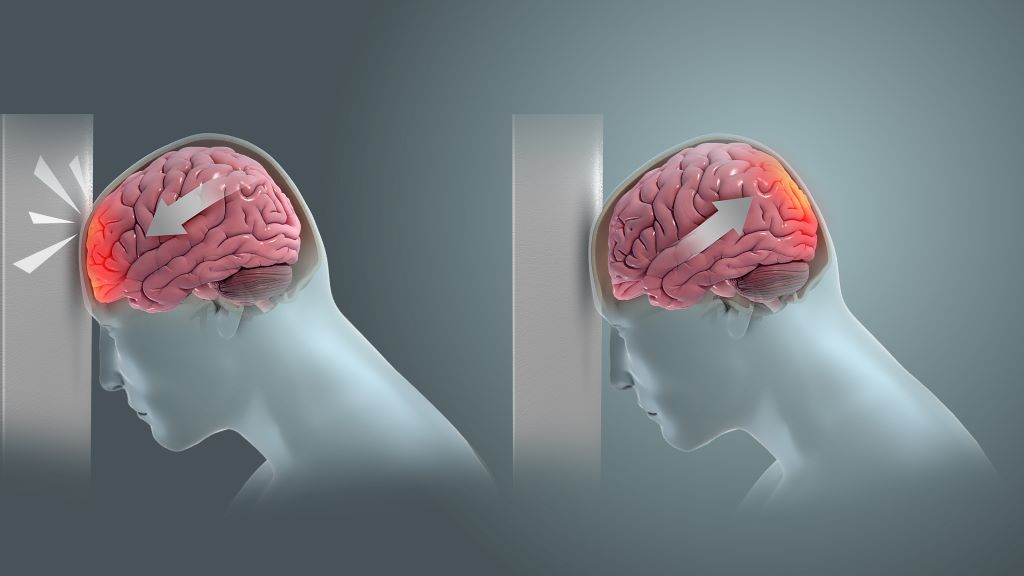
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Recent research has indicated that acoustic stimulation of the brain may ease persistent symptoms in individuals who experienced mild traumatic brain injury in the past.
The study, which appears in Annals of Clinical and Translational Neurology, included 106 military service members, veterans, or their spouses with persistent symptoms after mild traumatic brain injury sustained three months to 10 years ago. Participants were randomised 1:1 to receive either 10 sessions of engineered tones linked to brainwaves (intervention), or random engineered tones not linked to brainwaves (sham control). All participants rested comfortably in the dark in a ‘zero-gravity’ chair, eyes closed and listening to the computer-generated tones via earbud-style headphones. The primary outcome was change in symptom scores, with secondary outcomes of heart rate variability and self-reported measures of sleep, mood, and anxiety.
Among all study participants, symptom scores clinically and statistically improved compared with baseline, with benefits largely sustained at three months and six months; however, there were no significant differences between the intervention and control groups. Similar patterns were observed for secondary outcomes.
The results indicate that although acoustic stimulation is associated with marked improvement in postconcussive symptoms, listening to acoustic stimulation based on brain electrical activity, as it was delivered in this study, may not improve symptoms, brain function, or heart rate variability more than randomly generated, computer engineered acoustic stimulation.
“Postconcussive symptoms have proven very difficult to treat, and the degree of improvement seen in this study is virtually unheard of, though further research is needed to identify what elements are key to its success,” said corresponding author Michael J. Roy, MD, MPH, of Uniformed Services University and the Walter Reed National Military Medical Center, in Bethesda.
Lung cancer metastasis. Credit: National Cancer Institute
The largest review of papers for brain metastases of lung cancer has found abnormalities in their genetic mutations and for which licensed drugs could be clinically trialled to find out if they could treat the disease. The research led by the University of Bristol and published in Neuro-Oncology Advances also uncovered differences in those mutations between smokers and non-smokers.
Brain metastases most commonly occur from lung and breast cancer, and in the majority of cases are fatal. The genetic mutations in primary lung cancers have been widely studied, but less is known about the changes in the cancer once it has metastasised to the brain.
The research team wanted to find out the genetic changes in brain metastasis from non-small cell lung cancer (NSCLC) and whether there are drugs already available that could potentially be offered to these patients.
The researchers carried out a review from 72 papers of genetic mutations in brain metastasis of NSCLC from 2346 patients’ data on demographics, smoking status, genomic data, matched primary NSCLC, and PD-L1 – a protein found on cancer cells.
The study found the most commonly mutated genes were EGFR, TP53, KRAS, CDKN2A, and STK11.
Common missense mutations – mutations that lead to a single amino acid change in the protein coded by the gene – included EGFR L858R and KRAS G12C
In certain cases the genetic mutations were different in the brain metastasis from the primary lung cancer.
There were also differences in the genetic mutations in smokers versus patients who had never smoked. Brain metastases of smokers versus non-smokers had different missense mutations in TP53 and EGFR, except for L858R and T790M in EGFR, which were seen in both subgroups.
The research team found from the top ten commonly mutated genes which had primary NSCLC data, 37% of the specific mutations assessed were different between primary NSCLC and brain metastases.
The researchers suggest Medicines and Healthcare products Regulatory Agency-approved drugs already licensed could potentially be tested to treat the disease in clinical trials.
The genetic landscape of the different subtypes of NSCLC is well known. TP53 and LRP1B mutations are common to all NSCLC subtypes, but certain subtypes also have specific alterations.
Lung adenocarcinoma is the most common type of lung cancer and has higher frequencies of KRAS, EGFR, KEAP1, STK11, MET, and BRAF somatic mutations – changes that have accumulated in the cancer genome.
Some studies suggested that the genomic landscape of NSCLC in smokers vs non-smokers differ independent of subtype.
One study found EGFR mutations, ROS1 and ALK fusions to be more prevalent in non-smokers, whereas KRAS, TP53, BRAF, JAK2, JAK3 and mismatch repair gene mutations were more commonly mutated in smokers.
Kathreena Kurian, Professor of Neuropathology and Honorary Consultant at North Bristol NHS Trust, Head of the Brain Tumour Research Centre at the University of Bristol and co-author of the paper, said: “Our research recommends that all patients should have their brain metastasis examined for mutations in addition to their primary lung cancer because they may be different.
“This evidence could form the backbone for new clinical trials for patients with brain metastasis in non-small cell lung cancer using drugs that are already available.”
The team suggest the next steps for the research would be to consider whole genome sequencing on brain metastasis to look for other types of mutations, such as, common insertions/deletions for which drugs are already available.
Cross-sectional diagram of the NexGen 7T scanner, showing the new Impulse head-only gradient coil (green) and receiver-transmit coil (white) resting on a movable bed (brown) and connected to an electronic interface (blue) containing nearly a thousand wires (blue) that extend out of the magnet. Credit: Bernhard Gruber, MGH Harvard
An intense international effort to improve the resolution of magnetic resonance imaging (MRI) for studying the human brain has culminated in an ultra-high resolution 7 Tesla scanner that records up to 10 times more detail than current 7T scanners and over 50 times more detail than current 3T scanners, the mainstay of most hospitals.
This next generation or NexGen 7T functional MRI (fMRI) scanner can resolve features 0.4mm across, compared to the 2–3mm typical of today’s standard 3T fMRIs. It is described in a paper published in Nature Methods.
“The NexGen 7T scanner is a new tool that allows us to look at the brain circuitry underlying different diseases of the brain with higher spatial resolution in fMRI, diffusion and structural imaging, and therefore to perform human neuroscience research at higher granularity,” said David Feinberg, the director of the project to build the scanner. “The ultra-high resolution scanner will allow research on underlying changes in brain circuitry in a multitude of brain disorders, including degenerative diseases, schizophrenia and developmental disorders, including autism spectrum disorder.”
The improved resolution will help neuroscientists probe the neuronal circuits in different regions of the brain’s neocortex and allow researchers to track signals propagating from one area of the cortex, and perhaps discover underlying causes of developmental disorders. This could lead to better ways of diagnosing brain disorders, perhaps by identifying new biomarkers that would allow diagnosis of mental disorders earlier or, more specifically, in order to choose the best therapy.
“Normally, MRI is not fast enough at all to see the direction of the information being passed from one area of the brain to another,” Feinberg said. “The scanner’s higher spatial resolution can identify activity at different depths in the brain’s cortex to indirectly reveal brain circuitry by differentiating activity in different cell layers of the cortex.”
This is possible because neuroscientists have found in vision brain areas that the superficial and deepest cortex layers incorporate ‘top-down’ circuits, that is, they receive information from higher cortical brain areas, whereas the middle cortex involves ‘bottom-up’ circuitry, receiving sensory input. Pinpointing the fMRI activity to a specific depth in the cortex lets neuroscientists track the flow of information throughout the brain and cortex.
With the higher spatial resolution, neuroscientists will be able to home in on the activity of something on the order of 850 individual neurons within a single voxel – a 3D pixel – instead of the 600 000 recorded with standard hospital MRIs, said Silvia Bunge, a UC Berkeley professor of psychology who is one of the first to use the NexGen 7T to conduct research on a human brain.
“We were able to look at the layer profile of the prefrontal cortex, and it’s beautiful,” said Bunge, who studies abstract reasoning. “It’s so exciting to have this state-of-the-art, world-class machine.”
For William Jagust, a UC Berkeley professor of public health who studies the brain changes associated with Alzheimer’s disease, the improved resolution could finally help connect the dots between observed changes due to Alzheimer’s that occur in the brain – abnormal clumps of protein called beta amyloid and tau – and changes in memory.
“We know that part of the memory system in the brain degenerates as we get older, but we know little about the actual changes to the memory system – we can only go so far because of the resolution of our current MRI systems,” said Jagust. “With this new scanner, we think we’re going to be able to take apart a lot more carefully exactly where things have gone wrong. This could help with diagnosis or predicting outcomes in normal people.”
Jack Gallant, a UC Berkeley professor of psychology, hopes the scanner will help neuroscientists discover how functional changes in the brain lead to developmental and mental disorders such as dyslexia, autism and schizophrenia, or that result from neurological disorders, such as dementia and stroke.
“Mental disorders have an enormous impact on individuals, families and society. Together they represent about 10% of the US GDP. Mental disorders are fundamentally disorders of brain function, but functional measures are not used currently to diagnose most brain disorders or to look to see if a treatment’s working. Instead, these disorders are diagnosed behaviourally. This is a weak approach, because there are a lot of different mental brain states that can lead to exactly the same behaviour,” Gallant said. “What we need is more powerful MRI machines like this so that we can map, at high resolution, how information is represented in the brain. To me this is the big potential clinical benefit of ultra-high resolution MRI.”
Funding initiatives lead to ‘quantum leap’
The breakthrough came about through $22 million of funding from various government and private sector sources.
Incorporating newly developed hardware technology from those groups, Siemens collaborated with Feinberg’s team to rebuild a conventional 7 Tesla MRI scanner delivered to UC Berkeley in 2000 to improve the spatial resolution in pictures captured during brain scans.
“There’s been a large increase throughout the world of sites that use 7T MRI scanners, but they were mostly for development and were difficult to use,” said Nicolas Boulant, a physicist visiting from the NeuroSpin project at the University of Paris in Saclay, where he leads the team that operates the world’s only 11.7 Tesla MRI scanner, the strongest magnetic field employed to date. “David’s team really put together many ingredients to make a quantum leap at 7 Tesla, to go beyond what was achievable before and gain performance.”
Boulant hopes to adapt some of the new ingredients in the NexGen 7T – in particular, redesigned gradient coils – to eventually achieve even better resolution with the 11.7 Tesla MRI scanner. The gradient coils generate a rising magnetic field across the brain so that each part of the brain sees a different field strength, which helps to precisely map brain activity.
“The higher the magnetic field, the more difficult it is to really grab the potential promised by these higher-field MRI scanners to see finer details in the human brain,” he said. “You need all this peripheral equipment, which needs to be on steroids to meet those promises. The NexGen 7T is really a game-changer when you want to do neuro MRI.”
To reach higher spatial resolution, the NexGen 7T scanner had to be designed with a greatly improved gradient coil and with larger receiver array coils – which pick up the brain signals – using from 64 to 128 channels to achieve a higher signal-to-noise ratio (SNR) in the cortex and faster data acquisition. All these improvements were combined with a higher signal from the ultra-high field 7T magnet to achieve cumulative gains in the scanner performance.
The extremely powerful gradient coil is the first to be made with three layers of wire windings. Designed by Peter Dietz at Siemens in Erlangen, Germany, the “Impulse” gradient has 10 times the performance of gradient systems in current 7T scanners. Mathias Davids, then a physics graduate student at Heidelberg University in Mannheim, Germany, and a member of Feinberg’s team, collaborated with Dietz in performing physiologic modelling to allow a faster gradient slew rate – a measure of how quickly the magnetic field changes across the brain – while remaining under the neuronal stimulation thresholds of the human body.
“It’s designed so that the gradient pulses can be turned on and off much quicker – in microseconds – to record the signals much quicker, and also so the much higher amplitude gradients can be utilised without stimulating the peripheral nerves in the body or stimulating the heart, which are physiologic limitations,” Feinberg said.
A second key development in the scanner, Feinberg said, is the 128-channel receiver system that replaces the standard 32 channels. The large receiver coil arrays built by Shajan Gunamony of MR CoilTech in Glasgow, UK, gave a higher signal-to-noise ratio in the cerebral cortex and also provided higher parallel imaging acceleration for faster data acquisition to encode large image matrices for ultra high resolution fMRI and structural MRI.
To take advantage of the new hardware technology, Suhyung Park, Rüdiger Stirnberg, Renzo Huber, Xiaozhi Cao and Feinberg designed new pulse sequences of precisely timed gradient pulses to rapidly achieve ultra high resolution. The smaller voxels, measured in units of cubic millimetres and less than 0.1 microlitre, provide a 3D image resolution that is 10 times higher than that of previous 7T fMRIs and 125 times higher than the typical hospital 3T MRI scanners used for medical diagnosis.
Voxel-perfect resolution
The most common MRI scanners employ superconducting magnets that produce a steady magnetic field of 3 Tesla – 90 000 times stronger than Earth’s magnetic field and 3000 times stronger than a fridge magnet.
“A 3T fMRI scanner can resolve spatial details with a resolution of about 2 to 3mm. The cortical circuits that underpin thought and behaviour are about 0.5mm across, so standard research scanners cannot resolve these important structures,” Gallant said.
In contrast, fMRI focuses on blood flow in arteries and veins and can vividly distinguish oxygenated haemoglobin funnelling into working areas of the brain from deoxygenated haemoglobin in less active areas. This allows neuroscientists to determine which areas of the brain are engaged during a specific task.
But again, the 3mm resolution of a 3T fMRI can distinguish only large veins, not the small ones that could indicate activity within microcircuits.
The NexGen 7T will allow neuroscientists to pinpoint activity within the thin cortical layers in the grey matter, as well as within the narrow column circuits that are organised perpendicular to the layers. These columns are of special interest to Gallant, who studies how the world we see is represented in the visual cortex. He has actually been able to reconstruct what a person is seeing based solely on recordings from the brain’s visual cortex.
“The machine that David has built, in theory, should get down to 500 microns, or something like that, which is way better than anything else – we’re very near the scale you would want if you’re getting signals from a single column, for example,” Gallant said. “It’s fantastic. The whole thing about MRI is how big is the little volumetric unit, the voxel […] that’s the only thing that matters.”
For the moment, NexGen 7T brain scanners must be custom-built from regular 7T scanners but should be a lot cheaper than the $22 million required to build the first one.
Feinberg said that UC Berkeley’s NexGen 7T scanner technology will be disseminated by Siemens and MR CoilTech Ltd.
“My view is that we may never be able to understand the human brain on the cellular synaptic circuitry level, where there are more connections than there are stars in the universe,” Feinberg said. ” But we are now able to see signal patterns of brain circuits and begin to tease apart feedback and feed forward circuitry in different depths of the cerebral cortex. And in that sense, we will soon be able to understand the human brain organisation better, which will give us a new view into disease processes and ultimately allow us to test new therapies. We are seeking a better understanding and view of brain function that we can reliably test and reproducibly use noninvasively.”
A recent study has revealed a new culprit in the formation of brain haemorrhages that does not involve injury to the blood vessels, as previously believed. In the first-of-its kind study, researchers led by the University of California, Irvine discovered that interactions between aged red blood cells and brain capillaries can lead to cerebral microbleeds, offering deeper insights into how they occur and identifying potential new therapeutic targets for treatment and prevention.
The findings, published in the Journal of Neuroinflammation, describe how the team was able to watch the process by which red blood cells stall in the brain capillaries and then observe how the haemorrhage happens.
Cerebral microbleeds are associated with a variety of conditions that occur at higher rates in older adults, including hypertension, Alzheimer’s disease and ischaemic stroke.
“We have previously explored this issue in cell culture systems, but our current study is significant in expanding our understanding of the mechanism by which cerebral microbleeds develop,” said co-corresponding author Dr Mark Fisher, professor of neurology in UCI’s School of Medicine.
“Our findings may have profound clinical implications, as we identified a link between red blood cell damage and cerebral haemorrhages that occurs at the capillary level.”
The team exposed red blood cells to a chemical called tert-butyl hydroperoxide that caused oxidative stress; the cells were then marked with a fluorescent label and injected into mice.
Using two different methods, the researchers observed the red blood cells getting stuck in the brain capillaries and then being cleared out in a process called endothelial erythrophagocytosis.
As they moved out of the capillaries, microglia inflammatory cells engulfed the red blood cells, which led to the formation of a brain haemorrhage.
“It has always been assumed that in order for cerebral haemorrhage to occur, blood vessels need to be injured or disrupted. We found that increased red blood cell interactions with the brain capillaries represent an alternative source of development,” said co-corresponding author Xiangmin Xu, UCI professor of anatomy & neurobiology and director of the campus’s Center for Neural Circuit Mapping.
“We need to examine in detail the regulation of brain capillary clearance and also analyse how that process may be related to insufficient blood supply and ischaemic stroke, which is the most common form of stroke, to help advance the development of targeted treatments.”
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
Contrary to the commonly-held view, the brain does not have the ability to rewire itself to compensate for conditions such as stroke, loss of sight or an amputation, say scientists in the journal eLife.
Professors Tamar Makin of Cambridge University and John Krakauer of Johns Hopkins University argue that the notion that the brain, in response to injury or deficit, can reorganise itself and repurpose particular regions for new functions, is fundamentally flawed – despite being commonly cited in scientific textbooks. Instead, they argue that what is occurring is merely the brain being trained to utilise already existing, but latent, abilities.
One of the most common examples given is where a person loses their sight – or is born blind – and the visual cortex, previously specialised in processing vision, is rewired to process sounds, allowing the individual to use a form of ‘echolocation’ to navigate a cluttered room. Another common example is of people who have had a stroke and are initially unable to move their limbs repurposing other areas of the brain to allow them to regain control.
Krakauer, Director of the Center for the Study of Motor Learning and Brain Repair at Johns Hopkins University, said: “The idea that our brain has an amazing ability to rewire and reorganise itself is an appealing one. It gives us hope and fascination, especially when we hear extraordinary stories of blind individuals developing almost superhuman echolocation abilities, for example, or stroke survivors miraculously regaining motor abilities they thought they’d lost.
“This idea goes beyond simple adaptation, or plasticity – it implies a wholesale repurposing of brain regions. But while these stories may well be true, the explanation of what is happening is, in fact, wrong.”
In their article, Makin and Krakauer look at a ten seminal studies that purport to show the brain’s ability to reorganise. They argue, however, that while the studies do indeed show the brain’s ability to adapt to change, it is not creating new functions in previously unrelated areas – instead it’s utilising latent capacities that have been present since birth.
For example, a 1980s study by Professor Michael Merzenich at University of California, San Francisco looked at what happens when a hand loses a finger. The hand has a particular representation in the brain, with each finger appearing to map onto a specific brain region. Remove the forefinger, and the area of the brain previously allocated to this finger is reallocated to processing signals from neighbouring fingers, argued Merzenich – in other words, the brain has rewired itself in response to changes in sensory input.
Not so, says Makin, whose own research provides an alternative explanation.
In a study published in 2022, Makin used a nerve blocker to temporarily mimic the effect of amputation of the forefinger in her subjects. She showed that even before amputation, signals from neighbouring fingers mapped onto the brain region ‘responsible’ for the forefinger — in other words, while this brain region may have been primarily responsible for process signals from the forefinger, it was not exclusively so. All that happens following amputation is that existing signals from the other fingers are ‘dialled up’ in this brain region.
Makin, from the Medical Research Council (MRC) Cognition and Brain Sciences Unit at the University of Cambridge, said: “The brain’s ability to adapt to injury isn’t about commandeering new brain regions for entirely different purposes. These regions don’t start processing entirely new types of information. Information about the other fingers was available in the examined brain area even before the amputation, it’s just that in the original studies, the researchers didn’t pay much notice to it because it was weaker than for the finger about to be amputated.”
Another compelling counterexample to the reorganisation argument is seen in a study of congenitally deaf cats, whose auditory cortex appears to be repurposed to process vision. But when they are fitted with a cochlear implant, this brain region immediately begins processing sound once again, suggesting that the brain had not, in fact, rewired.
Examining other studies, Makin and Krakauer found no compelling evidence that the visual cortex of individuals that were born blind or the uninjured cortex of stroke survivors ever developed a novel functional ability that did not otherwise exist.
Makin and Krakauer do not dismiss stories such as blind people navigating using hearing, or individuals who have experienced a stroke regain their motor functions. They argue instead that rather than completely repurposing regions for new tasks, the brain is enhancing or modifying its pre-existing architecture — and it is doing this through repetition and learning.
Understanding the true nature and limits of brain plasticity is crucial, both for setting realistic expectations for patients and for guiding clinical practitioners in their rehabilitative approaches, they argue.
Makin added: “This learning process is a testament to the brain’s remarkable – but constrained – capacity for plasticity. There are no shortcuts or fast tracks in this journey. The idea of quickly unlocking hidden brain potentials or tapping into vast unused reserves is more wishful thinking than reality. It’s a slow, incremental journey, demanding persistent effort and practice. Recognising this helps us appreciate the hard work behind every story of recovery and adapt our strategies accordingly.
“So many times, the brain’s ability to rewire has been described as ‘miraculous’ – but we’re scientists, we don’t believe in magic. These amazing behaviours that we see are rooted in hard work, repetition and training, not the magical reassignment of the brain’s resources.”
For some people, drinking red wine even in small amounts causes a headache, which typically occurs within 30 minutes to three hours after drinking as little as a small glass of wine. Researchers have examined why this happens – even to people who don’t get headaches when drinking small amounts of other alcoholic beverages. In their work, published in the journal Scientific Reports, the researchers posit that a flavanol found naturally in red wines can interfere with the proper metabolism of alcohol and can lead to a headache.
The headache culprit: Quercetin, a flavanol
This flavanol is called quercetin and it is naturally present in all kinds of fruits and vegetables, including grapes. It’s considered a healthy antioxidant and is even available in supplement form. But when metabolized with alcohol, it can be problematic.
“When it gets in your bloodstream, your body converts it to a different form called quercetin glucuronide,” said wine chemist and corresponding author Andrew Waterhouse, professor emeritus with the UC Davis Department of Viticulture and Enology. “In that form, it blocks the metabolism of alcohol.”
Acetaldehyde toxin buildup leads to flushing, headache, nausea
As a result, people can end up accumulating the toxin acetaldehyde, explains lead author Apramita Devi, postdoctoral researcher with the UC Davis Department of Viticulture and Enology.
“Acetaldehyde is a well-known toxin, irritant and inflammatory substance,” said Devi. “Researchers know that high levels of acetaldehyde can cause facial flushing, headache and nausea.”
The medication disulfiram prescribed to alcoholics to prevent them from drinking causes these same symptoms. Waterhouse said that’s because the drug also causes the toxin to build up in the body when normally an enzyme in the body would break it down. About 40% of the East Asian population also has an enzyme that doesn’t work very well, allowing acetaldehyde to build up in their system.
“We postulate that when susceptible people consume wine with even modest amounts of quercetin, they develop headaches, particularly if they have a preexisting migraine or another primary headache condition,” said co-author Morris Levin, professor of neurology and director of the Headache Center at the University of California, San Francisco. “We think we are finally on the right track toward explaining this millennia-old mystery. The next step is to test it scientifically on people who develop these headaches, so stay tuned.”
Sunlight increases headache-causing flavanol in grapes
Waterhouse said levels of this flavanol can vary dramatically in red wine.
“Quercetin is produced by the grapes in response to sunlight,” Waterhouse said. “If you grow grapes with the clusters exposed, such as they do in the Napa Valley for their cabernets, you get much higher levels of quercetin. In some cases, it can be four to five times higher.”
Levels of quercetin can also differ depending on how the wine is made, including skin contact during fermentation, fining processes and aging.
Clinical trial on wine headaches
Scientists will next compare red wines that contain a lot of quercetin with those that have very little to test their theory about red wine headaches on people. This small human clinical trial, funded by the Wine Spectator Scholarship Foundation, will be led by UCSF.
Researchers said there are still many unknowns about the causes of red wine headaches. It’s unclear why some people seem more susceptible to them than others. Researchers don’t know if the enzymes of people who suffer from red wine headaches are more easily inhibited by quercetin or if this population is just more easily affected by the buildup of the toxin acetaldehyde.
“If our hypothesis pans out, then we will have the tools to start addressing these important questions,” Waterhouse said.
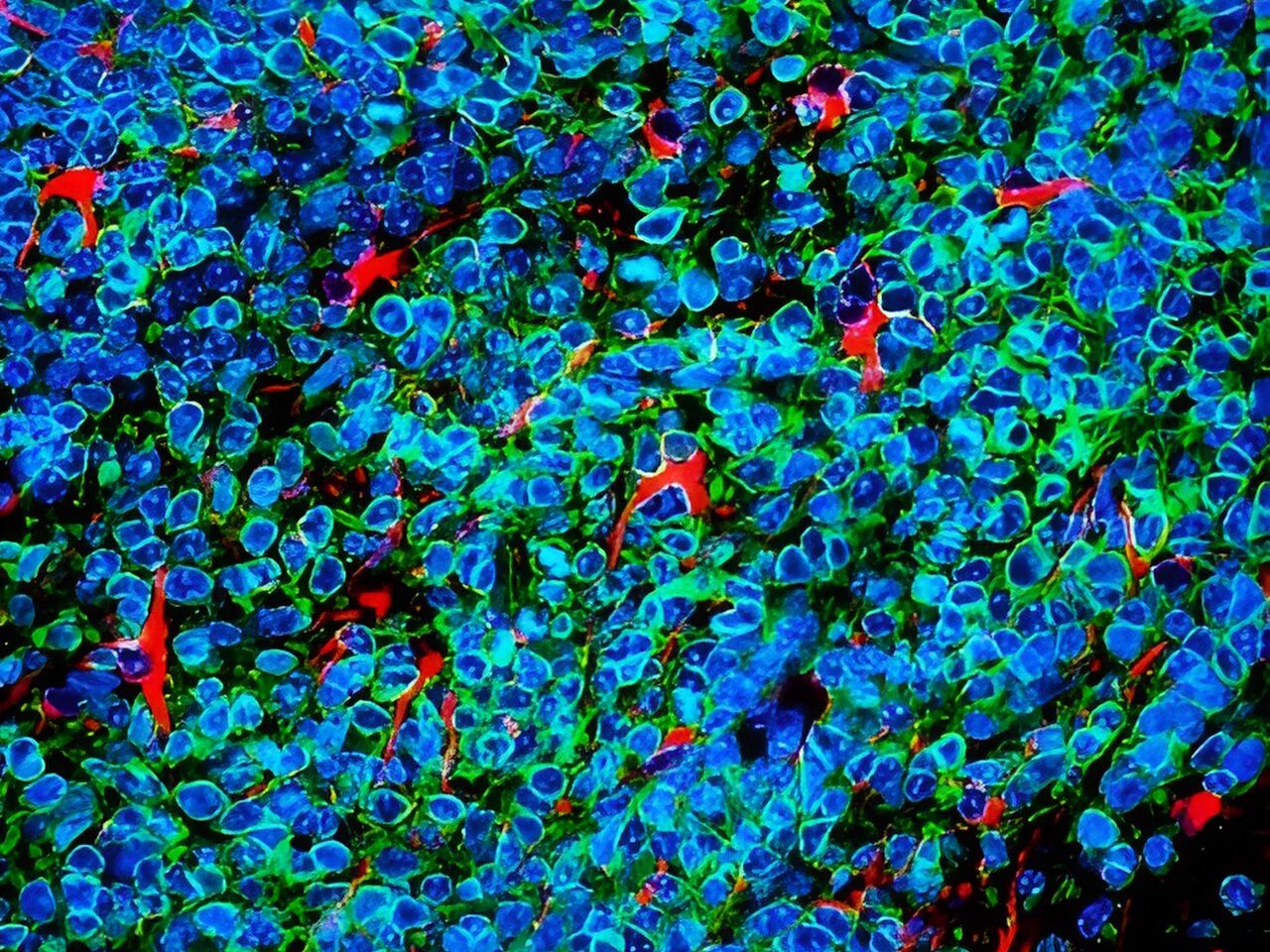
Small cell lung cancer cells (green and blue) that metastasised to the brain in a laboratory mouse recruit brain cells called astrocytes (red) for their protection. Credit: Fangfei Qu
Lung cancer cells that metastasise to the brain survive by convincing brain cells called astrocytes that they are baby neurons in need of protection, according to a study by researchers at Stanford Medicinepublished in Nature Cell Biology.
The cancer cells carry out their subterfuge by secreting a chemical signal prevalent in the developing human brain, the researchers found. This signal draws astrocytes to the tumour, encouraging them to secrete other factors that promote the cancer cells’ survival. Blocking that signal may be one way to slow or stop the growth of brain metastases of small cell lung cancer, which account for about 10% to 15% of all lung cancers, the researchers believe.
In the adult brain, astrocytes play a critical role in maintaining nerve function and connectivity. They are also important during brain development, when they facilitate connections between developing neurons.
The researchers studied laboratory mice, human tissue samples and human mini-brains, or organoids, grown in a lab dish to dissect the unique relationship between the cancer cells and their ‘big sister’ astrocytes, which hover nearby and shower them with protective factors.
“Small cell lung cancers are known for their ability to metastasise to the brain and thrive in an environment that is not normally conducive to tumour growth,” said professor of paediatrics and of genetics Julien Sage, PhD. “Our study suggests that these cancer cells reprogram the brain microenvironment by recruiting astrocytes for their protection.”
Professor Sage is the senior author of the study, while postdoctoral scholar Fangfei Qu, PhD, is the lead author.
Invasion of the brain
Small cell lung cancer excels at metastasising to the brain – about 15% to 20% of people already have clusters of cancer cells in their brains when their lung tumours are first diagnosed. As the cancer progresses, about 40% to 50% of patients will develop brain metastases. The problem is so prevalent, and the clinical outcome so dire, that clinicians recommend cranial radiation even before brain metastases have been found.
How and why small cell lung cancer has such an affinity for the brain has been something of a mystery. Brain metastases are rarely biopsied or removed because doing so has not been shown to affect a patient’s survival, and brain surgery is so invasive. Using laboratory mice is also of little help since small cell lung cancers in those animals rarely develop metastases in the brain, perhaps due to subtle biological differences between species.
Small cell lung cancers have another distinguishing feature – they are neuroendocrine cancers, meaning they arise from cells with similarities to both neurons and hormone-producing cells. Neuroendocrine cells link the nervous system with the endocrine system throughout the body, including in the lung.
Sage and his colleagues wondered whether neuronal-associated proteins on the surface of small cell lung cancer cells give them a leg up when the cells first begin to infiltrate the brain.
“We know the brain is full of neurons,” Sage said. “Maybe that’s why these cancer cells with some neuronal traits are happy in the brain and are accepted into that environment.”
Qu and Sage developed a way to inject mouse small cell lung cancer cells grown in the laboratory into the brains of mice to spark the development of brain tumours. They saw that astrocytes, a subtype of glial cell, flocked to the infant tumours and began to churn out proteins critical during brain development, including factors that stimulate nerve growth.
A plethora of astrocytes
A similar call happens in human brains, they noted: Brain tissue samples from people who had died of metastatic small cell lung cancer, shared by professor of pathology and paper co-author Christina Kong, MD, had many more protective astrocytes in the interior of the tumours than did metastases of melanoma, breast cancer and another type of lung cancer called adenocarcinoma.
Qu worked with assistant professor of paediatrics and co-author Anca Pasca, MD, to fuse aggregates of small cell lung cancer, lung adenocarcinoma or breast cancer cells with what are called cortical organoids – in vitro-grown clumps of brain cells including neurons and astrocytes that begin to mimic the organisation and connectivity of a human cortex. Within 10 days, many more protective astrocytes had infiltrated the small cell lung cancer pseudo-tumours than the adenocarcinoma or breast cancer.
“This showed us that the astrocytes actively move toward the small cell lung cancer cells, rather than simply being engulfed by the growing tumour,” Sage said. “What’s more exciting, though, is that these organoids, or mini-brains, realistically model the developing human brain. So, we’re no longer relying on a mouse model. It’s a perfect system to study brain metastases.”
Further research showed that the small cell lung cancer cells summon protective astrocytes by secreting a protein called Reelin that mediates the migration of neuronal and glial cells during brain development. Triggering Reelin expression in mouse breast cancer cells injected into the brain significantly increased the number of astrocytes in the resulting tumours in the mice, and the tumours were larger than in control animals injected with cells with low Reelin expression.
The apparent reliance of the cancer cells on chemical signals and responses specific to the developing brain may give clues for the development of future therapies, Sage believes.
“Some of these signals may not be as relevant or as highly expressed in the adult brain,” Sage said. “As a result, perhaps they could still be targeted to slow or prevent brain metastases without harming a normal brain. This might be an important window of opportunity for therapy.”
At 18 Spanish hospitals, when a patient with brain metastasis undergoes surgery, they can donate a tiny part of their brain to the first repository of brain metastasis living samples in the world, based at the Spanish National Cancer Research Centre (CNIO). A world-first collection, it was created to accelerate the search for therapies against brain metastasis, a disease that affects up to 30% of patients with systemic cancer.
The creators of this repository, called RENACER (Spanish acronym for the National Brain Metastasis Network), are two CNIO researchers, Manuel Valiente, head of the Brain Metastasis Group, and Eva Ortega-Paíno, director of the Biobank. They explained the advantages of the collection in the journal Trends in Cancer. In just three years RENACER has compiled samples from more than 150 patients.
The truly unique feature of RENACER, which makes it a valuable tool for the international scientific community, is that it contains living samples, conserved in cultures that enable the cells to continue behaving in a similar way as they were in the body.
A living biobank that enables organotypic cultures
“We have built a ‘living’ biobank” write Valiente and Ortega-Paíno. And this characteristic can be “transformative, not only for research but also for clinical trial design, especially when focused on unmet clinical needs, such as brain metastasis”.
The fact that the cells are living allows them, for example, to study their response to specific drugs. RENACER paves the way to create avatars for each patient in order to identify the best therapeutic options in an individualised way.
“Research contracts have been already signed to exploit patient-derived organotypic cultures (PDOCs) as avatars, thus providing the possibility to generate biomarkers of sensitivity or resistance to specific drugs” the authors explain.
The hospitals involved with RENACER work as a network to pass on research findings to patients as quickly as possible. In fact, thanks to this network, there are already two clinical trials underway, which will determine the capacity of two biomarkers to discriminate cases in which radiotherapy – a technique with side effects – will be effective.
From the operating theatre to the biobank in hours
The requirement for cells to be “alive” is not easy to achieve, since it involves a sophisticated logistics chain. The samples are taken from the operating theatre in a special container, in their culture medium, at a temperature of between 4 and 8 degrees centigrade.
They must reach the CNIO Biobank, in Madrid, in less than 24 hours. There, they are processed, organotypic cultures are created, and they are divided into proportional parts that are stored as samples for future investigations. They are also analysed using various techniques and sequenced, to extract as much information as possible from them. All the data are put into a database that is open to the international scientific community.
“It is pivotal to empower patients”
“This is happening just a few years after the project was launched,” said Valiente. “It’s a strategy that helps to improve knowledge as well as diagnosis and treatment options, but also brings all the people involved closer together: patients, core researchers, chemical re searchers, healthcare professionals, and the biobank.”
Patients, “[because they act] as donors during a difficult brain metastasis neurosurgery, play a crucial role and we strongly believe that it is pivotal to empower them,” the researchers explain. GEPAC (Spanish Group of Patients with Cancer) is also involved with RENACER.
Looking away from something frightening may be due to a specific cluster of neurons in a visual region of the brain, according to new research at the University of Tokyo. Researchers found that, in fruit fly brains, these neurons release a chemical called tachykinin which appears to control the fly’s movement to avoid facing a potential threat. Fruit fly brains can offer a useful analogy for larger mammals, so this study, published in Nature Communications, may help studies of human reactions to fearful situations and phobias.
“We discovered a neuronal mechanism by which fear regulates visual aversion in the brains of Drosophila (fruit flies). It appears that a single cluster of 20-30 neurons regulates vision when in a state of fear. Since fear affects vision across animal species, including humans, the mechanism we found may be active in humans as well,” explained Assistant Professor Masato Tsuji from the Department of Biological Sciences at the University of Tokyo.
The team used puffs of air to simulate a physical threat and found that the flies’ walking speed increased after being puffed at. The flies also would choose a puff-free route if offered, showing that they perceived the puffs as a threat (or at least preferred to avoid them). Next the researchers placed a small black object, roughly the size of a spider, 60 degrees to the right or left of the fly. On its own the object didn’t cause a change in behavior, but when placed following puffs of air, the flies avoided looking at the object and moved so that it was positioned behind them.
To understand the molecular mechanism underlying this aversion behavior, the team then used mutated flies in which they altered the activity of certain neurons. While the mutated flies kept their visual and motor functions, and would still avoid the air puffs, they did not respond in the same fearful manner to visually avoid the object.
“This suggested that the cluster of neurons which releases the chemical tachykinin was necessary for activating visual aversion,” said Tsuji. “When monitoring the flies’ neuronal activity, we were surprised to find that it occurred through an oscillatory pattern, ie, the activity went up and down similar to a wave. Neurons typically function by just increasing their activity levels, and reports of oscillating activity are particularly rare in fruit flies because up until recently the technology to detect this at such a small and fast scale didn’t exist.”
By giving the flies genetically encoded calcium indicators, the researchers could make the flies’ neurons shine brightly when activated. Thanks to the latest imaging techniques, they then saw the changing, wavelike pattern of light being emitted, which was previously averaged out and missed.
Next, the team wants to figure out how these neurons fit into the broader circuitry of the brain. Although the neurons exist in a known visual region of the brain, the researchers do not yet know from where the neurons are receiving inputs and to where they are transmitting them, to regulate visual escape from objects perceived as dangerous.
“Our next goal is to uncover how visual information is transmitted within the brain, so that we can ultimately draw a complete circuit diagram of how fear regulates vision,” said Tsuji. “One day, our discovery might perhaps provide a clue to help with the treatment of psychiatric disorders stemming from exaggerated fear, such as anxiety disorders and phobias.”
People often experience headaches and body pain after a lack of sleep, but the mechanisms behind this phenomenon are unclear. A new study published in Nature Communicationsreveals that a certain endocannabinoid neurotransmitter plays a major role.
The animal-based study, led by investigators at Massachusetts General Hospital (MGH), a founding member of Mass General Brigham (MGB), found that the heightened pain sensitivity than can result from chronic sleep disruption (CSD) – or CSD-induced hyperalgaesia – involved signalling from a part of a brain known as the thalamic reticular nucleus (TRN).
Analyses of metabolites showed that the level of N-arachidonoyl dopamine (NADA), a type of neurotransmitter called an endocannabinoid, decreased in the TRN as a result of sleep deprivation.
Activity of the cannabinoid receptor 1, which is involved in controlling pain perception, also decreased in the thalamic reticular nucleus after CSD.
Administering NADA to the TRN reduced CSD-induced hyperalgaesia in mice.
This beneficial effect of administered NADA could be countered by blocking the cannabinoid receptor 1, suggesting that both the receptor and NADA play a role in pain sensitivity due to sleep deprivation.
“We provide a mechanism as to how sleep disruption leads to exaggerated pain, suggesting that harnessing the endocannabinoid system might break the vicious cycle between pain and sleep loss,” says co-senior author Shiqian Shen, MD, the clinical director of MGH’s Tele Pain Program.