A recent randomised clinical trial published in Developmental Medicine & Child Neurology assessed whether injections of botulinumtoxin-A in calf muscles benefit children with cerebral palsy.
“We hypothesised that injections with botulinumtoxin-A in the calf muscles would make walking easier, caused by improved ankle joint functioning following spasticity reduction,” the authors wrote.
In the trial, one botulinumtoxin-A treatment was not superior to placebo in making walking easier (measured as a reduction in energy cost or improved walking capacity); however, there was some evidence of a delayed improvement in energy cost. Moreover, there was some evidence of a decrease in calf pain intensity. No serious adverse events related to botulinumtoxin-A treatment were recorded.
Researchers from Germany have made a surprising discovery about the aggressive, lethal glioblastomas: in the vicinity of glioblastomas, they found islands of highly potent immune cells in the neighbouring bone marrow of the skull, which play a central role in defending against cancer. The new data may open up prospects for innovative therapies. On the other hand, they cast a shadow over conventional strategies.
“What we have found is surprising and fundamentally new,” says Björn Scheffler, German Cancer Consortium (DKTK) researcher at the Essen site. Until now, the body’s own defences have always been thought of as a holistic system that sends its troops to different parts of the body as required. “However,” says Scheffler, “our data show that highly potent immune cells gather in regional bone marrow niches close to the tumour and organise the defence from there. At least this is the case with glioblastomas.”
Immune system on site
Based on new findings from animal experiments, the Essen team took tissue samples from the bone marrow near the tumor in the skull from untreated patients with glioblastoma. “However, the methods for this first had to be established,” reports first author Celia Dobersalske, emphasizing the fact that the new research results were obtained from human tissue samples.
The researchers hit the bull’s eye in their search: Bone marrow niches in close proximity to the glioblastoma appear to be the reservoir from which the anti-tumour defence is recruited. Apart from active lymphoid stem cells that develop into immune cells, the researchers also found mature cytotoxic T lymphocytes (CD8 cells) in the bone marrow close to the tumour. “These are highly effective immune cells that play a central role in the defence against cancer,” adds Celia Dobersalske. They can recognize and destroy malignant cells.
The CD8 cells in the bone marrow near the tumour had an increased number of receptors on their surface, which control the proliferation of mature T lymphocytes. In line with this, descendants of the same cell clones – one clone originates from one and the same cell – were detected both in the bone marrow and in the tumour tissue. This is clear evidence that the immune cells gathered on site are fighting the glioblastoma. “And they are successful – at least for a while,” says Björn Scheffler. “We were able to show that the course of the disease correlates with the activity of the local CD8 cells.”
Valuable immune cells destroyed?
This finding not only turns conventional ideas about how the immune system works on their head. The treatment concepts for glioblastoma must also be reconsidered in light of the new data. “Until now, we hadn’t even considered the skullcap in our considerations. How could we, since there was no evidence that highly potent immune cells could be hiding there,” says senior author Scheffler.
“When we opened the skull, we may have destroyed important immune cells in the process,” confirms Ulrich Sure, Director of the Department of Neurosurgery and member of the Essen research team. “In view of the new findings, we find ourselves in a dilemma: we have to gain access to the tumour in order to remove it and also to be able to confirm the diagnosis. There is currently no other way than through the skull. But we are thinking about how we can minimise damage to the local bone marrow in the future.”
On the other hand, the discovery of the local immune system opens up opportunities for innovative therapies. In particular, so-called checkpoint inhibitors are coming back into play. These are immunotherapeutic agents that aim to boost the body’s own cancer defenses. However, checkpoint inhibitors tested to date have shown little effect on glioblastomas.
“Various explanations have been suggested as an explanation, but perhaps we also need to rethink things in this respect,” says Björn Scheffler. “We now know that highly potent immune cells are indeed present on site. We were able to prove that they are fit to fight tumours, but they are not capable of destroying the tumour on their own. This is where we can start. One challenge will be to deliver drugs in sufficient concentration to the regional bone marrow niches at the right time. If we succeed, we may have a chance of controlling the growth of glioblastomas and improving our patients’ chances of survival.”
A study led by Georgetown University neuroscientists reveals that the part of the brain that receives and processes visual information in sighted people develops a unique connectivity pattern in people born blind. They say this pattern in the primary visual cortex is unique to each person, akin to a fingerprint.
The findings, published in PNAS, have profound implications for understanding brain development and could help launch personalised rehabilitation and sight restoration strategies.
For decades, scientists have known that the visual cortex in people born blind responds to a myriad of stimuli, including touch, smell, sound localization, memory recall and response to language. However, the lack of a common thread linking the tasks that activate primary areas in the visual cortex has perplexed researchers. The new study, led by Lenia Amaral, PhD, a postdoctoral researcher; and Ella Striem-Amit, PhD, the Edwin H. Richard and Elisabeth Richard von Matsch Assistant Professor of Neuroscience at Georgetown University’s School of Medicine, offers a compelling explanation: differences in how each individual’s brain organizes itself.
“We don’t see this level of variation in the visual cortex connectivity among individuals who can see – the connectivity of the visual cortex is usually fairly consistent,” said Striem-Amit, who leads the Sensory and Motor Plasticity Lab at Georgetown. “The connectivity pattern in people born blind is more different across people, like an individual fingerprint, and is stable over time – so much so that the individual person can be identified from the connectivity pattern.”
The study included a small sample of people born blind who underwent repeated functional MRI scans over two years. The researchers used a neuroimaging technique to analyze neural connectivity across the brain.
“The visual cortex in people born blind showed remarkable stability in its connectivity patterns over time,” Amaral explained. “Our study found that these patterns did not change significantly based on the task at hand , whether participants were localising sounds, identifying shapes, or simply resting. Instead, the connectivity patterns were unique to each individual and remained stable over the two-year study period.”
Striem-Amit said these findings tell us how the brain develops. “Our findings suggest that experiences after birth shape the diverse ways our brains can develop, especially if growing up without sight. Brain plasticity in these cases frees the brain to develop, possibly even for different possible uses for the visual cortex among different people born blind,” Striem-Amit said.
The researchers posit that understanding each person’s individual connectivity may be important to better tailor solutions for rehabilitation and sight restoration to individuals with blindness, each based on their own individual brain connectivity pattern.
Why do new comorbidities arise because of ischaemic stroke? A study from Germany recently published in the journal Cell has discovered why this can happen – and ways in which it might be countered. The findings from the study show that the immune system is involved in damage to other organs, including the heart.
Besides the early mortality and morbidity resulting from the ischaemic brain injury itself, long-term morbidity after stroke is also due to the high prevalence of secondary comorbidities and complications, such as cognitive impairment and dementia, post-stroke depression, cardiac events, persistent vascular inflammation, and stroke-induced metabolic disturbances.
Liesz is the principal investigator of this new study. The researchers worked on the hypothesis that the high rate of comorbidities that develop after a stroke could have a common immunological cause. And they actually managed to find it: the origin of the dysfunctions in other parts of the body lies in the immunological memory of the blood-forming cells in bone marrow.
Using single-cell sequencing techniques, Liesz and his team demonstrated the presence of permanent proinflammatory changes in the transcriptome of certain immune cells (monocytes/macrophages) in several organs. In other words, certain gene segments are transcribed differently there after the stroke, which unbalances the proteome. These epigenetic modifications occur most frequently in the heart, where they can cause scarring and impair pumping function. “We managed to identify the protein IL-1b as the main culprit for the epigenetic modifications that affect immunological memory after a stroke,” says Liesz.
Promising therapeutic approaches on the horizon
The researchers demonstrated in a mouse model the connection between modified blood formation in bone marrow through overexpressed IL-1b and cardiac dysfunctions. Moreover, they showed that blocking IL-1b and inhibiting migration of the proinflammatory cells to the heart both successfully prevented cardiac problems after a stroke.
“These findings are hugely significant, as they open up the promise of effective therapeutic approaches for the prevention of secondary cardiac conditions after a stroke,” reckons Liesz.
The authors of the study believe that the epigenetic mechanisms they described for the reprogramming of the immune system in the brain-heart axis will create a new framework for explaining the development of various IL-1b-mediated comorbidities.
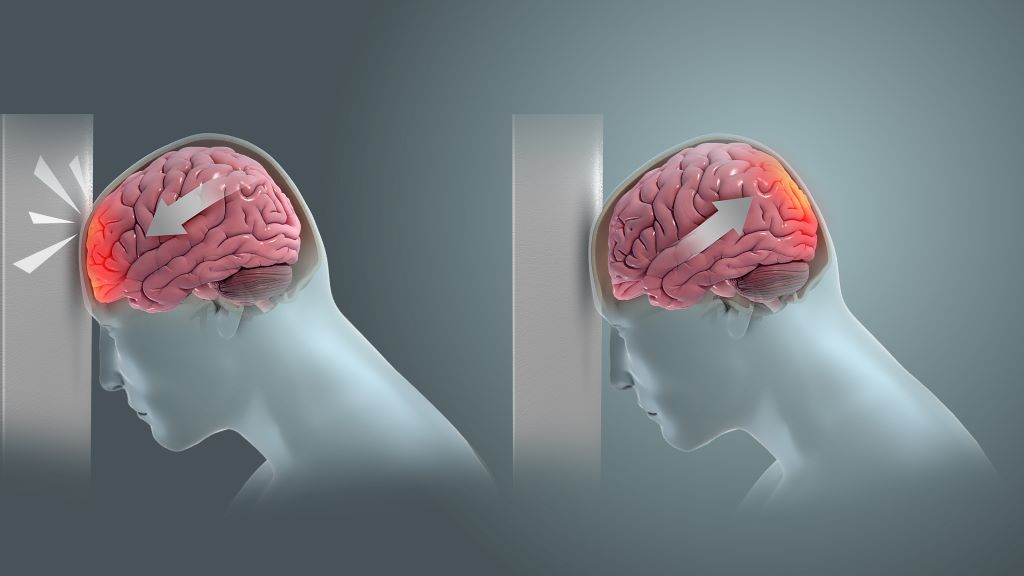
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Researchers at Johns Hopkins explored a potential alternative and less-invasive approach to evaluate intracranial pressure (ICP) in patients with serious neurological conditions. This research, using artificial intelligence (AI) to analyse routinely captured ICU data, was published in Computers in Biology and Medicine.
ICP is a physiological variable that can increase abnormally if one has severe traumatic brain injury, stroke or obstruction to the flow of cerebrospinal fluid. Symptoms of elevated ICP may include headaches, blurred vision, vomiting, changes in behaviour and decreased level of consciousness. It can be life-threatening, hence the need for ICP monitoring in selected patients who are at increased risk. But the current standard for ICP monitoring is highly invasive: it requires the placement of an external ventricular drain (EVD) or an intraparenchymal brain monitor (IPM) in the functional tissue in the brain consisting of neurons and glial cells by drilling through the skull.
“ICP is universally accepted as a critical vital sign – there is an imperative need to measure and treat ICP in patients with serious neurological disorders, yet the current standard for ICP measurement is invasive, risky, and resource-intensive. Here we explored a novel approach leveraging Artificial Intelligence which we believed could represent a viable noninvasive alternative ICP assessment method,” says senior author Robert Stevens, MD, MBA, associate professor of anaesthesiology and critical care medicine.
EVD procedures carry a number of risks including catheter misplacement, infection, and haemorrhaging at 15.3 %, 5.8 %, and 12.1 %, respectively, according to recent research. EVD and IPM procedures also require surgical expertise and specialised equipment that is not consistently available in many settings thus underscoring the need for an alternative method in examining and monitoring ICP in patients.
The Johns Hopkins team, a group that included faculty and students from the School of Medicine and Whiting School of Engineering, hypothesised that severe forms of brain injury, and elevations in ICP in particular, are associated with pathological changes in systemic cardiocirculatory function due, for example, to dysregulation of the central autonomic nervous system. This hypothesis suggests that extracranial physiological waveforms can be studied to better understand brain activity and ICP severity.
In this study, the Johns Hopkins team set out to explore the relationship between the ICP waveform and the three physiological waveforms that are routinely captured in the ICU: invasive arterial blood pressure (ABP), photoplethysmography (PPG) and electrocardiography (ECG). ABP, PPG and ECG data were used to train deep learning algorithms, resulting in a level of accuracy in determining ICP that rivals or exceeds other methodologies.
Overall study findings suggest a completely new, noninvasive alternative to monitor ICP in patients.
Stevens says, “with validation, physiology-based AI solutions, such as the one used here, could significantly expand the proportion of patients and health care settings in which ICP monitoring and management can be delivered.”
There are many drugs that anaesthesiologists can use to induce unconsciousness in patients. Exactly how these drugs cause the brain to lose consciousness has been a longstanding question, but MIT neuroscientists have now answered that question for the commonly used drug propofol.
Using a novel technique for analysing neuron activity, the researchers discovered that the drug propofol induces unconsciousness by disrupting the brain’s normal balance between stability and excitability. The drug causes brain activity to become increasingly unstable, until the brain loses consciousness.
“The brain has to operate on this knife’s edge between excitability and chaos. It’s got to be excitable enough for its neurons to influence one another, but if it gets too excitable, it spins off into chaos. Propofol seems to disrupt the mechanisms that keep the brain in that narrow operating range,” says Earl K. Miller, the Picower Professor of Neuroscience and a member of MIT’s Picower Institute for Learning and Memory.
The new findings, published in Neuron, could help researchers develop better tools for monitoring patients as they undergo general anaesthesia.
Miller and Ila Fiete, a professor of brain and cognitive sciences, the director of the K. Lisa Yang Integrative Computational Neuroscience Center (ICoN), and a member of MIT’s McGovern Institute for Brain Research, are the senior authors of the new study. MIT graduate student Adam Eisen and MIT postdoc Leo Kozachkov are the lead authors of the paper.
Losing consciousness
Propofol is a drug that binds to GABA receptors in the brain, inhibiting neurons that have those receptors. Other anaesthesia drugs act on different types of receptors, and the mechanism for how all of these drugs produce unconsciousness is not fully understood.
Miller, Fiete, and their students hypothesised that propofol, and possibly other anaesthesia drugs, interfere with a brain state known as “dynamic stability.” In this state, neurons have enough excitability to respond to new input, but the brain is able to quickly regain control and prevent them from becoming overly excited.
Previous studies of how anaesthesia drugs affect this balance have found conflicting results: Some suggested that during anaesthesia, the brain shifts toward becoming too stable and unresponsive, which leads to loss of consciousness. Others found that the brain becomes too excitable, leading to a chaotic state that results in unconsciousness.
Part of the reason for these conflicting results is that it has been difficult to accurately measure dynamic stability in the brain. Measuring dynamic stability as consciousness is lost would help researchers determine if unconsciousness results from too much stability or too little stability.
In this study, the researchers analysed electrical recordings made in the brains of animals that received propofol over an hour-long period, during which they gradually lost consciousness. The recordings were made in four areas of the brain that are involved in vision, sound processing, spatial awareness, and executive function.
These recordings covered only a tiny fraction of the brain’s overall activity, so to overcome that, the researchers used a technique called delay embedding. This technique allows researchers to characterize dynamical systems from limited measurements by augmenting each measurement with measurements that were recorded previously.
Using this method, the researchers were able to quantify how the brain responds to sensory inputs, such as sounds, or to spontaneous perturbations of neural activity.
In the normal, awake state, neural activity spikes after any input, then returns to its baseline activity level. However, once propofol dosing began, the brain started taking longer to return to its baseline after these inputs, remaining in an overly excited state. This effect became more and more pronounced until the animals lost consciousness.
This suggests that propofol’s inhibition of neuron activity leads to escalating instability, which causes the brain to lose consciousness, the researchers say.
Better anesthesia control
To see if they could replicate this effect in a computational model, the researchers created a simple neural network. When they increased the inhibition of certain nodes in the network, as propofol does in the brain, network activity became destabilized, similar to the unstable activity the researchers saw in the brains of animals that received propofol.
“We looked at a simple circuit model of interconnected neurons, and when we turned up inhibition in that, we saw a destabilization. So, one of the things we’re suggesting is that an increase in inhibition can generate instability, and that is subsequently tied to loss of consciousness,” Eisen says.
As Fiete explains, “This paradoxical effect, in which boosting inhibition destabilises the network rather than silencing or stabilising it, occurs because of disinhibition. When propofol boosts the inhibitory drive, this drive inhibits other inhibitory neurons, and the result is an overall increase in brain activity.”
The researchers suspect that other anesthetic drugs, which act on different types of neurons and receptors, may converge on the same effect through different mechanisms – a possibility that they are now exploring.
If this turns out to be true, it could be helpful to the researchers’ ongoing efforts to develop ways to more precisely control the level of anaesthesia that a patient is experiencing. These systems, which Miller is working on with Emery Brown, the Edward Hood Taplin Professor of Medical Engineering at MIT, work by measuring the brain’s dynamics and then adjusting drug dosages accordingly, in real-time.
“If you find common mechanisms at work across different anaesthetics, you can make them all safer by tweaking a few knobs, instead of having to develop safety protocols for all the different anaesthetics one at a time,” Miller says. “You don’t want a different system for every anesthetic they’re going to use in the operating room. You want one that’ll do it all.”
The researchers also plan to apply their technique for measuring dynamic stability to other brain states, including neuropsychiatric disorders.
“This method is pretty powerful, and I think it’s going to be very exciting to apply it to different brain states, different types of anaesthetics, and also other neuropsychiatric conditions like depression and schizophrenia,” Fiete says.
The cerebellum has traditionally been viewed only as a motor control centre; however, recent studies have revealed its involvement in non-motor functions such as cognition, emotion, memory, autonomic function, satiety and meal termination.
In a recent mouse-model study, published in Nature Neuroscience, researchers at University Hospitals (UH), Harrington Discovery Institute at UH, and Case Western Reserve University have now found that the cerebellum also controls thirst, a major function necessary for survival. Specifically, the research team found that a hormone, asprosin, crosses from the periphery into the brain to activate Purkinje neurons in the cerebellum. This leads to an enhanced drive to seek and drink water.
“Asprosin, a hormone our lab discovered in 2016, is known to stimulate food intake and maintain body weight by activating key ‘hunger’ neurons in a part of the brain called the hypothalamus, and works by binding a protein on the neuron surface called a ‘receptor,’” explained Associate Professor Atul Chopra, MD, PhD, senior author on the study.
A receptor is necessary for a hormone to work, and in the case of asprosin’s ability to control appetite and body weight, that receptor is Ptprd. Besides the hypothalamus, the team found that it is also highly expressed in the cerebellum, although the functional significance of this was unknown.
“At the outset, we wondered whether asprosin action in the cerebellum was to coordinate food intake with the hypothalamus, which turned out to be incorrect. The breakthrough came when Ila Mishra, a postdoctoral fellow in the lab, and now the head of her own lab at the University of Kentucky, discovered that mice generated to lack cerebellar responsiveness to asprosin exhibited reduced water intake. Our intended endpoint was measurement of food intake, not water intake, making this a serendipitous observation.”
These mice also showed reduced Purkinje neuron activity accompanied by hypodipsia (reduced feelings of thirst). Their food intake, motor coordination, and learning remained unaffected. By contrast, mice generated to preclude hypothalamic responsiveness to asprosin show reduced food intake without impacting thirst.
“Our results identified not only a new function of cerebellar Purkinje neurons in the modulation of thirst, but also its independent regulation from their well-established role in motor coordination and learning,” added Dr Chopra. “It is fascinating that after a century or more of neuroscience, we are still discovering major new functions of parts of the brain long thought to be understood. The broader implication of this discovery lies in its potential to inform the management of thirst disorders like polydipsia (excessive thirst), hypodipsia and adipsia, for which no current treatments exist.”
Since I was young, I have been intrigued by altered states of consciousness, such as out-of-body experiences, paranormal phenomena and religious visions. I studied psychology and neuroscience to gain a better understanding of how these experiences come about. And in my scientific career, I have focused on the question of why some people are more prone to having these experiences than others.
Naturally, when I came across psychedelic science a couple of years ago, this field also sparked my academic interest. Here was an opportunity to study people who had a psychedelic experience and who claimed to have had a glimpse of ultimate reality. I started to research psychedelic experiences at Leiden University and founded the PRSM lab – a group of scientists from different academic backgrounds who study psychedelic, religious, spiritual and mystical experiences.
Initially, I was enthusiastic about the mind-transforming potential of psychedelics. These substances, when administered correctly, appear to be capable of enhancing people’s mental and physical wellbeing. They also increase feelings of connectedness to and concern for the environment.
Psychedelic therapy appeared to offer great potential for treating a wide variety of disorders, including depression, anxiety, addiction and post-traumatic stress disorder. This enthusiasm about the potentially transformative effects of psychedelics was reflected in positive media attention on this topic over the past few years. Michael Pollan, an American author and journalist, has brought psychedelics to an audience of millions with his book and Netflix documentary.
However, my initial optimism about psychedelics and their potential has changed into scepticism about the science behind much of the media hype. This is due to a closer scrutiny of the empirical evidence. Yes, at face value it seems as if psychedelic therapy can cure mental disease. But on closer inspection, the story is not that straightforward.
The main reason? The empirical evidence for the efficacy of and the working mechanisms underlying psychedelic therapy is far from clear.
Two issues
I wrote a critical review paper with my colleague Eiko Fried in which we listed the problems with the current clinical trials on psychedelic therapy. The main concern is called the “breaking blind problem”. In psychedelic studies, patients easily figure out if they have been randomly assigned to the psychedelic or the placebo group, simply because of the profound mind-altering effects of psychedelic substances.
This breaking-of-the-blind can actually result in placebo effect in patients in the psychedelic group: they finally get the treatment they’d been hoping for and they start feeling better. But it can also result in frustration and disappointment in patients assigned to the control group. They were hoping to get a miracle cure but now find out they will have to spend six hours on a placebo pill with their therapist.
As a consequence, any difference in therapeutic outcomes between the psychedelic and the placebo group is largely driven by these placebo and nocebo effects. (A nocebo effect is when a harmless treatment causes side-effects or worsening of symptoms because the person believes they may occur or expects them to occur.)
Knowing who received what also affects the therapists, who may be motivated to get more out of the therapy session if their patient got the “real deal”. And this problem is impossible to control for in so-called randomised controlled trials – still the gold standard in evaluating the effectiveness of drugs and treatments.
Also, non-clinical research on psychedelics faces problems. You may recall the graphic of a brain on psilocybin compared to one on a placebo (see below). Psilocybin increases the connections between different brain areas, which is represented in a colourful array of connecting lines.
This has become known as the “entropic brain hypothesis”. Psychedelics make your brain more flexible such that it returns to a child-like state of openness, novelty and surprise. This mechanism in turn has been hypothesised to underlie psychedelic therapy’s efficacy: by “liberating your brain” psychedelics can change entrenched and maladaptive patterns and behaviour. However, it turns out the picture is much more complicated than that.
Psychedelics constrict the blood vessels in your body and brain and this causes problems in the measurement of brain signals with MRI machines.
The graphic of the entropic brain may simply reflect the fact that the blood flow in the brain is dramatically altered under psilocybin. Also, it is far from clear what entropy exactly means – let alone how it can be measured in the brain.
A recent psilocybin study, which is yet to be peer-reviewed, found that only four out of 12 entropy measures could be replicated, casting further doubt on how applicable this mechanism of action is.
Although the story about psychedelics freeing your mind is compelling, it does not yet square well with the available empirical evidence.
These are just two examples that illustrate why it is important to be really cautious when you evaluate empirical studies in psychedelic science. Don’t trust findings at face value, but ask yourself the question: is the story too good or too simple to be true?
Personally, I have developed a healthy dose of scepticism when it comes to psychedelic science. I am still intrigued by psychedelics’ potential. They offer great tools for studying changes in consciousness. However, it is too early to conclude anything definite about their working mechanisms or their therapeutic potential. For this, we need more research. And I’m excited to contribute to that endeavour.
Having more positive experiences in life is associated with lower odds of developing brain disorders like Alzheimer’s disease, slower cognitive decline with age, and even a longer life. But how feelings and experiences are translated into physical changes that protect or harm the brain is still unclear.
Now, a study from Columbia researchers suggests that the brain’s mitochondria may play a fundamental part. The new study shows that the molecular machinery used by mitochondria to transform energy is boosted in older adults who experienced less psychological stress during their lives compared with individuals who had more negative experiences.
“We’re showing that older individuals’ state of mind is linked to the biology of their brain mitochondria, which is the first time that subjective psychosocial experiences have been related to brain biology,” says Caroline Trumpff, assistant professor of medical psychology, who led the research with Martin Picard, associate professor of behavioural medicine at Columbia University Vagelos College of Physicians and Surgeons and in the Robert N. Butler Columbia Aging Center.
“We think that the mitochondria in the brain are like antennae, picking up molecular and hormonal signals and transmitting information to the cell nucleus, changing the life course of each cell,” says Picard. “And if mitochondria can change cell behaviour, they can change the biology of the brain, the mind, and the whole person.”
Study details
The new research used data collected by two extensive studies of nearly 450 older adults in the United States. Each study collected detailed psychosocial information from the participants for two decades during their lives. Study participants donated their brains after death for further analysis, which provided data on the state of the participants’ brain cells.
Trumpff created indices that converted patients’ reports of positive and negative psychosocial factors into a single score of overall psychosocial experience. She also scored each participant on seven domains that represent distinct genetic networks active in mitochondria.
“The use of multivariate mitotype indices is an important innovation because we could more easily interpret the biological state of the mitochondria with networks of related genes than an analysis of thousands of individual genes,” Picard says.
Study results
The results showed that one mitochondrial domain – which assessed the organelle’s energy transformation machinery – was associated with psychosocial scores.
“Greater well-being was linked to greater abundance of proteins in mitochondria needed to transform energy, whereas negative mood was linked to lower protein content,” Trumpff says. “This may be why chronic psychological stress and negative experiences are bad for the brain, because they damage or impair mitochondrial energy transformation in the dorsolateral prefrontal cortex, the part of the brain responsible for high-level cognitive tasks.”
The researchers also analysed mitochondria in specific cell types in the brain and found that the associations between mitochondria and psychosocial factors were driven not by the brain’s neurons, but its glia cells, which may be playing more than their traditionally assumed “supportive” roles.
“This piece of the study, made possible by our collaboration with the Columbia Center for Translational and Computational Neuroimmunology, is what I think makes it particularly significant,” Picard says. “To ask questions at this level of cellular resolution in the brain is unprecedented in the mitochondrial field.
“Neurons have been the focus of neuroscience, but we’re waking up to the fact that other cells in the brain may be driving disease.”
Do mitochondria change mood, or does mood change mitochondria?
Though the current study cannot determine if the participant’s psychosocial experiences altered their brain mitochondria or if innate or acquired mitochondrial states contributed to those experiences, other studies suggest that the relationship between mitochondria and mood works both ways.
In animal studies, the evidence is very strong, Picard says, that chronic stress affects mitochondrial energy transformation. And in people, a recent study conducted by Picard and collaborator Elissa Epel at UCSF found the first evidence that mood may affect mitochondria in humans: In that study, positive mood predicted greater mitochondrial energy production in the participants’ blood cells on subsequent days, but mitochondrial activity did not predict mood on subsequent days.
A growing body of work in animals and humans also indicates that mitochondria themselves can alter behaviour.
“It’s possible that these mechanisms reinforce one another,” Trumpff says. “Chronic stress could alter an individual’s mitochondrial biology in ways that subsequently affects their perception of social events, creating more stress. The emerging picture in the literature is that all these pathways are interactive.”
Next steps
Though the brain’s energy transformation machinery was greater in participants with higher psychosocial scores, the researchers do not yet know if that leads to greater energy transformation. Trumpff and Picard are currently doing those studies with hundreds of brains from the same cohorts of participants.
The team is also exploring a way to measure the brain’s mitochondrial health, which could be used in doctors’ offices in the future.
“Mitochondria are the source of health and life, but we don’t have ways to quantify health, only disease,” Picard says. “We need a science of health. We need tests that show how healthy and resilient someone is.
“This would be valuable clinically to monitor changes in health before the appearance of disease, and it could transform medical research by giving scientists something to target other than decades of accumulated protein deposits or other forms of long-term damage.”
New research describes how a spreading wave of disruption and the flow of fluid in the brain triggers headaches, detailing the connection between the neurological symptoms associated with aura and the migraine that follows. The study, which appears in Science, also identifies new proteins that could be responsible for headaches and may serve as foundation for new migraine drugs.
“In this study, we describe the interaction between the central and peripheral nervous system brought about by increased concentrations of proteins released in the brain during an episode of spreading depolarization, a phenomenon responsible for the aura associated with migraines,” said lead author Maiken Nedergaard, MD, DMSc, co-director of the University of Rochester Center for Translational Neuromedicine. “These findings provide us with a host of new targets to suppress sensory nerve activation to prevent and treat migraines and strengthen existing therapies.”
It is estimated that one out of 10 people experience migraines and in about a quarter of these cases the headache is preceded by an aura, a sensory disturbance that can includes light flashes, blind spots, double vision, and tingling sensations or limb numbness. These symptoms typically appear five to 60 minutes prior to the headache.
The cause of the aura is a phenomenon called cortical spreading depression, a temporary depolarization of neurons and other cells caused by diffusion of glutamate and potassium that radiates like a wave across the brain, reducing oxygen levels and impairing blood flow. Most frequently, the depolarization event is located in the visual processing centre of the brain cortex, hence the visual symptoms that first herald a coming headache.
While migraines auras arise in the brain, the organ itself cannot sense pain. These signals must instead be transmitted from the central nervous system to the peripheral nervous system. The process of communication between the brain and peripheral sensory nerves in migraines has largely remained a mystery.
Fluid dynamics models shed light on migraine pain origins
Nedergaard and her colleagues at the University of Rochester and the University of Copenhagen are pioneers in understanding the flow of fluids in the brain. In 2012, her lab was the first to describe the glymphatic system, which uses cerebrospinal fluid (CSF) to wash away toxic proteins in the brain. In partnership with experts in fluid dynamics, the team has built detailed models of how the CSF moves in the brain and its role in transporting proteins, neurotransmitters, and other chemicals.
The most widely accepted theory is that nerve endings resting on the outer surface of the membranes that enclose the brain are responsible for the headaches that follow an aura. The new study, which was conducted in mice, describes a different route and identifies proteins, many of which are potential new drug targets, that may be responsible for activating the nerves and causing pain.
As the depolarization wave spreads, neurons release a host of inflammatory and other proteins into CSF. In a series of experiments in mice, the researchers showed how CSF transports these proteins to the trigeminal ganglion, a large bundle of nerves that rests at the base of the skull and supplies sensory information to the head and face.
It was assumed that the trigeminal ganglion, like the rest of the peripheral nervous system, rested outside the blood-brain-barrier, which tightly controls what molecules enter and leave the brain. However, the researchers identified a previously unknown gap in the barrier that allowed CSF to flow directly into the trigeminal ganglion, exposing sensory nerves to the cocktail of proteins released by the brain.
Migraine-associated proteins double during brain wave activity
Analysing the molecules, the researchers identified twelve proteins called ligands that bind with receptors on sensory nerves found in the trigeminal ganglion, potentially causing these cells to activate. The concentrations of several of these proteins found in CSF more than doubled following a cortical spreading depression. One of the proteins, calcitonin gene-related peptide (CGRP), is already the target of a new class of drugs to treat and prevent migraines called CGRP inhibitors. Other identified proteins are known to play a role in other pain conditions, such as neuropathic pain, and are likely important in migraine headaches as well.
“We have identified a new signaling pathway and several molecules that activate sensory nerves in the peripheral nervous system. Among the identified molecules are those already associated with migraines, but we didn’t know exactly how and where the migraine inducing action occurred,” said Martin Kaag Rasmussen, PhD, a postdoctoral fellow at the University of Copenhagen and first author of the study. “Defining the role of these newly identified ligand-receptor pairs may enable the discovery of new pharmacological targets, which could benefit the large portion of patients not responding to available therapies.”
The researchers also observed that the transport of proteins released in one side of the brain reaches mostly the nerves in the trigeminal ganglion on the same side, potentially explaining why pain occurs on one side of the head during most migraines.