Leading vaccinologist Professor Shabir Madhi received the Lifetime Award from South Africa’s prestigious ‘Science Oscars’ held by the National Science and Technology Foundation. He received the honour for his leadership in research on vaccines against life-threatening diseases in Africa and globally, and he has been at the cutting edge of research in this area since 1997.
As well as being the Dean of the Faculty of Health Sciences and Professor of Vaccinology at Wits, Prof Madhi is also the director of the South African Medical Research Council (SAMRC) Vaccine and Infectious Diseases Analytics Research Unit (Wits-VIDA); and is co-director of African Leadership in Vaccinology Expertise, Wits. During the COVID pandemic he became one of the most-cited expert by the media as the public looked to the healthcare sector for advice and guidance during this crisis.
A number of awards also went to those in the field of healthcare or who contributed to healthcare, an area especially marked by SA’s response to the COVID pandemic.
CEO of SA Health Products Regulatory Authority (SAHPRA), Dr Boitumelo Semete-Makokotlela, received the Management Award for successfully leading the authorisation of a number of COVID diagnostic tests, vaccines and therapies during the COVID.
The Network for Genomics Surveillance (NGS-SA) in SA received the Data for Research award for NGS-SA, which generated of genomic surveillance data of SARS-CoV-2 aimed at informing SA’s public health response to this virus. It was represnted by its co-founders, Dr Jinal Bhiman, Scientific Lead for Global Immunology and Immune Sequencing for Epidemic Response South Africa (GIISER-SA); and Professor Tulio de Oliveira, SU.
Other recipients in the field of healthcare included Dr Wynand Goosen, who received an Emerging Researcher aware for leadership of research in SA on the surveillance of zoonotic TB in domestic cattle and wild animals as potential infection sources in susceptible people in rural areas.
Decades of research has provided no clear evidence that serotonin levels or serotonin activity are responsible for depression, according to a major review of existing literature.
Published in Molecular Psychiatry, this new umbrella review is an overview of existing meta-analyses and systematic reviews. It suggests that depression is not likely to be caused by a chemical imbalance. It also calls into question what antidepressants do: most antidepressants are selective serotonin reuptake inhibitors (SSRIs), whose mechanism of action was supposedly to correct abnormally low serotonin levels. But there is no other accepted pharmacological mechanism by which antidepressants affect the symptoms of depression.
Lead author Professor Joanna Moncrieff, at University College London said: “It is always difficult to prove a negative, but I think we can safely say that after a vast amount of research conducted over several decades, there is no convincing evidence that depression is caused by serotonin abnormalities, particularly by lower levels or reduced activity of serotonin.
“The popularity of the ‘chemical imbalance’ theory of depression has coincided with a huge increase in the use of antidepressants. Prescriptions for antidepressants have risen dramatically since the 1990s, with one in six adults in England and 2% of teenagers now being prescribed an antidepressant in a given year.
“Many people take antidepressants because they have been led to believe their depression has a biochemical cause, but this new research suggests this belief is not grounded in evidence.”
The umbrella review aimed to capture all relevant studies, encompassing tens of thousands of participants, that have been published in the most important fields of research on serotonin and depression.
Research that compared levels of serotonin and its breakdown products in the blood or brain fluids found no difference between participants diagnosed with depression and healthy controls.
Research on serotonin receptors and the serotonin transporter, the protein targeted by most antidepressants, found weak and inconsistent evidence suggestive of higher levels of serotonin activity in people with depression. However, the researchers say the findings are likely explained by the use of antidepressants among people diagnosed with depression, since such effects were not reliably ruled out.
Some studies artificially lowered serotonin levels were by depriving participant’s diets of the necessary amino acid. These studies have been cited as demonstrating that a serotonin deficiency is linked to depression. A meta-analysis conducted in 2007 and a sample of recent studies found that lowering serotonin in this way did not produce depression in hundreds of healthy volunteers, however. There was very weak evidence in a small subgroup of people with a family history of depression, but this only involved 75 participants, and more recent evidence was inconclusive.
Very large studies involving tens of thousands of patients looked at gene variation, including the gene for the serotonin transporter, and found no difference between people with depression and healthy controls. These studies also examined stressful life events, and found these to strongly increase people’s risk of becoming depressed. A famous early study found a relationship between stressful events, the type of serotonin transporter gene a person had and the chance of depression. But larger, more comprehensive studies suggest this was a false finding.
These findings together led the authors to conclude that there is “no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations.”
The researchers say their findings are important as studies show that as many as 85–90% of the public believes that depression is caused by low serotonin or a chemical imbalance. A growing number of scientists and professional bodies are recognising the chemical imbalance framing as an over-simplification. Evidence also suggests that believing that low mood is caused by a chemical imbalance leads to pessimism about recovery, and the possibility of managing moods without medical help. This is important because most people will at some point in their lives meet criteria for anxiety or depression.
A large meta-analysis provided evidence that people who used antidepressants actually had lower levels of serotonin in their blood. The researchers concluded that some evidence was consistent with the possibility that long-term antidepressant use reduces serotonin concentrations. The researchers say this may imply that the increase in serotonin that some antidepressants produce in the short term could lead to compensatory changes in the brain that produce the opposite effect in the long term.
Though antidepressants’ efficacies was not examined, the authors encourage looking into treatments such psychotherapy, alongside other practices such as exercise or mindfulness, or addressing underlying contributors such as poverty, stress and loneliness.
Professor Moncrieff said: “Our view is that patients should not be told that depression is caused by low serotonin or by a chemical imbalance, and they should not be led to believe that antidepressants work by targeting these unproven abnormalities. We do not understand what antidepressants are doing to the brain exactly, and giving people this sort of misinformation prevents them from making an informed decision about whether to take antidepressants or not.”
Co-author Dr Mark Horowitz said: “I had been taught that depression was caused by low serotonin in my psychiatry training and had even taught this to students in my own lectures. Being involved in this research was eye-opening and feels like everything I thought I knew has been flipped upside down.
“One interesting aspect in the studies we examined was how strong an effect adverse life events played in depression, suggesting low mood is a response to people’s lives and cannot be boiled down to a simple chemical equation.”
Professor Moncrieff added: “Thousands of people suffer from side effects of antidepressants, including the severe withdrawal effects that can occur when people try to stop them, yet prescription rates continue to rise. We believe this situation has been driven partly by the false belief that depression is due to a chemical imbalance. It is high time to inform the public that this belief is not grounded in science.”
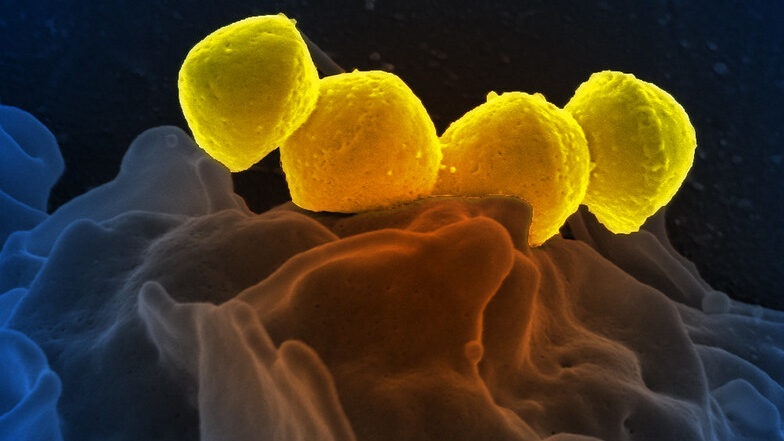
Streptococcus pyogenese bound to a human neutrophil. Credit: National Institute of Allergy and Infectious Diseases, National Institutes of Health
Bordering on science fiction, medicinal microrobots could help physicians better treat and prevent diseases. But a serious problem is the synthetic materials they are made of trigger immune responses. Now, for the first time, researchers report in ACS Central Science that they achieved precise control neutrophils as a natural, biocompatible microrobot by using lasers. By getting the ‘neutrobots’ to perform multiple tasks, the researchers demonstrated they could one day deliver drugs to precise locations in the body.
Microrobots being developed for medical applications would need to be administered in injections or oral capsules to get them inside the body. But these microscopic objects are often found to trigger immune reactions in small animals, resulting in the the microrobots being ejected from the body before they can carry out their tasks. By using the body’s own cells, such as neutrophils, drugs could be delivered less invasively without provoking an immune response.
Neutrophils already naturally pick up nanoparticles and dead red blood cells and can migrate through blood vessels into adjacent tissues, so they are good candidates for becoming microrobots. Previously, researchers have guided neutrophils with lasers in lab dishes, moving them around as ‘neutrobots’. However, this had not been tried in living animals. So, researchers set out to demonstrate the feasibility of light-driven neutrobots in animals using live zebrafish.
The researchers manipulated and moved neutrophils in zebrafish tails, using focused laser beams as optical tweezers. The ‘neutrobots’ could be moved up to a velocity of 1.3 µm/s, three times faster than a neutrophil’s natural speed. The optical tweezers were able to precisely and actively control the functions that neutrophils conduct as part of the immune system. For example, moving through a blood vessel wall into the surrounding tissue; carrying a plastic nanoparticle, showing potential for delivering medicine; and pushed towards red blood cell debris, a neutrophil engulfed the pieces. Surprisingly, at the same time, a different neutrophil, which wasn’t controlled by a laser, tried to naturally remove the cellular debris. Because they successfully controlled neutrobots in vivo, the researchers say this study advances the possibilities for targeted drug delivery and precise treatment of diseases.
From left to right: Junior doctor Aniket Bharadwaj with trainers Dr Ruby Woodard and Dr Jonny Martin, diagnosing a hologram patient. Credit: University of Cambridge
A new effort from Cambridge University brings medical training in ‘mixed reality’ one step closer with modules that allow student doctors to interact with a ‘holographic’ patient.
Traditional simulation has numerous costs including maintaining simulation centres, their equipment and the faculty and staff hours to operate the labs and hire and train patient actors. This new technology could provide more flexible, cost-effective training that can be accessed all over the world.
HoloScenarios is a new training application based on life-like holographic patient scenarios, is being developed by Cambridge University Hospitals NHS Foundation Trust (CUH), in partnership with the University of Cambridge and US tech company GigXR. The first module focuses on common respiratory conditions and emergencies.
“Mixed reality is increasingly recognised as a useful method of simulator training,” said project leader Dr Arun Gupta, consultant anaesthetist at CUH and director of postgraduate education at CUH.
“As institutions scale procurement, the demand for platforms that offer utility and ease of mixed reality learning management is rapidly expanding,” he said.
Learners wearing mixed-reality headsets can interact with each other and a multi-layered, medically accurate ‘holographic’ patient. This creates a unique environment to learn and practice vital, real-time decision making and treatment choices.
Medical instructors with their own headsets can make changes on the fly, by changing patient responses or introducing complications – whether in person in a teaching group or over the internet.
Learners can also watch, contribute to and assess the holographic patient scenarios from Android, iOS smartphone or tablet. This means true-to-life, safe-to-fail immersive learning can be accessed, delivered and shared across the world, with the technology now available for license to learning institutions everywhere.
Professor Riikka Hofmann at Cambridge’s Faculty of Education is leading an analysis of the technology as a teaching method.
“Our research is aimed at uncovering how such simulations can best support learning and accelerate the adoption of effective mixed reality training while informing ongoing development,” said Prof Hofmann.
“We hope that it will help guide institutions in implementing mixed reality into their curricula, in the same way institutions evaluate conventional resources, such as textbooks, manikins, models or computer software, and, ultimately, improve patient outcomes.”
Junior doctor Aniket Bharadwaj is one of the first to try out the new technology. “Throughout medical school we would have situations where actors would come in an act as patients. With the pandemic a lot of that changed to tablet based interactions because of the risk to people of the virus,” he said.
“Having a hologram patient you can see, hear and interact with is really exciting and will really make a difference to student learning.”
The first module features a hologram patient with asthma, followed by anaphylaxis, pulmonary embolism and pneumonia. Further modules in cardiology and neurology are in development.
Delivered by the Gig Immersive Learning Platform, HoloScenarios aims to centralise and streamline access and management of mixed reality learning, and encapsulate the medical experience of world-leading doctors at CUH and across the University of Cambridge.
While carbon monoxide is associated with asphyxiation cases, in small doses it also has beneficial qualities, helping reduce inflammation and stimulate tissue regeneration.
But now, a team of researchers have devised a novel way to deliver carbon monoxide to the body without its hazardous effects. Inspired by techniques used in molecular gastronomy, they were able to incorporate carbon monoxide into stable foams that can be delivered to the digestive tract.
In a mouse study, the researchers showed that these foams reduced inflammation of the colon and helped to reverse acute liver failure caused by acetaminophen overdose. The researchers said that their new technique, described today in a Science Translational Medicine paper, could also be used to deliver other therapeutic gases.
“The ability to deliver a gas opens up whole new opportunities of how we think of therapeutics. We generally don’t think of a gas as a therapeutic that you would take orally (or that could be administered rectally), so this offers an exciting new way to think about how we can help patients,” said Giovanni Traverso, a professor at MIT and a gastroenterologist at Brigham and Women’s Hospital.
Inspired by fine cuisine
Since the late 1990s, Leo Otterbein, a professor of surgery at Harvard Medical School and Beth Israel Deaconess Medical Center, has been studying the therapeutic effects of low CO doses. The gas has been shown to impart beneficial effects in preventing rejection of transplanted organs, reducing tumour growth, and modulating inflammation and acute tissue injury.
When inhaled at high concentrations, CO binds to haemoglobin in the blood and prevents the body from obtaining enough oxygen, which can be fatal in same cases. However, at lower doses, it has beneficial effects such as reducing inflammation and promoting tissue regeneration, Prof Otterbein said.
“We’ve known for years that carbon monoxide can impart beneficial effects in all sorts of disease pathologies, when given as an inhaled gas,” he saud. “However, it’s been a challenge to use it in the clinic, for a number of reasons related to safe and reproducible administration, and health care workers’ concerns, which has led to people wanting to find other ways to administer it.”
Prof Traverso’s lab specialises in developing novel methods for delivering drugs to the gastrointestinal tract. They came up with the idea of incorporating the gas into a foam, much the way that chefs use carbon dioxide to create foams infused with fruits, vegetables, or other flavours.
Culinary foams are usually created by adding a thickening or gelling agent to a liquid or a solid that has been pureed, and then either whipping it to incorporate air or using a specialised siphon that injects gases such as carbon dioxide or compressed air.
The MIT team created a modified siphon that could be attached to any kind of gas canister, allowing them to incorporate CO into their foam. To create the foams, they used food additives such as alginate, methyl cellulose, and maltodextrin. Xantham gum was also added to stabilise the foams. By varying the amount of xantham gum, the researchers could control the release rate of CO gas from the foam.
After showing that they could control the timing of the gas release in the body, the researchers decided to test the foams for a few different applications. First, they studied two types of topical applications, analogous to applying a cream to soothe itchy or inflamed areas. In a study of mice, they found that delivering the foam rectally reduced inflammation caused by colitis or radiation-induced proctitis (inflammation of the rectum that can be caused by radiation treatment for cervical or prostate cancer).
Current treatments for colitis and other inflammatory conditions such as Crohn’s disease usually involve drugs that suppress the immune system, which can make patients more susceptible to infections. Treating those conditions with a foam that can be applied directly to inflamed tissue offers a potential alternative, or complementary approach, to those immunosuppressive treatments, the researchers said. While the foams were given rectally in this study, it could also be possible to deliver them orally, the researchers say.
Controlling the dose
The researchers then investigated possible systemic applications to deliver CO to remote organs, such as the liver, because of its ability to diffuse from the GI tract elsewhere in the body. For this study, they used a mouse model of acetaminophen overdose, which causes severe liver damage. They found that gas delivered to the lower GI tract was able to reach the liver and greatly reduce the amount of inflammation and tissue damage seen there.
In these experiments, the researchers did not find any adverse effects after the carbon monoxide administration. A healthy individual has CO levels of ~1% in the bloodstream, and studies of human volunteers have shown that levels as high as 14% can be tolerated without adverse effects.
“We think that with the foam used in this study, we’re not even coming close to the levels that we would be concerned about,” Otterbein says. “What we have learned from the inhaled gas trials has paved a path to say it’s safe, as long as you know and can control how much you’re giving, much like any medication. That’s another nice aspect of this approach — we can control the exact dose.”
In this study, the researchers also created carbon-monoxide containing gels, as well as gas-filled solids, using techniques similar to those used to make Pop Rocks, the hard candies that contain pressurised carbon dioxide bubbles. They plan to test those in further studies, in addition to developing the foams for possible tests in human patients.
A new research paper has signalled a crisis in medical research: “over 60% of trials are so methodologically flawed we cannot believe their results”. Researchers estimate that 88% of trial spending is wasted.
Dodgy research design and bad statistical methodology mean that most randomised trials are a waste of time, money and effort, and of no or dubious scientific value, say Stefania Pirosca, Frances Shiely, Mike Clarke and Shaun Treweek, in a new paper published in the journal Trials in early June.
Their paper examined 1659 randomised trials, involving 400,000 participants, that took place between May 2020 and April 2021 in 84 countries as well as 193 multinational trials.
The majority of trials (62%) showed a high risk of bias. More than half of trial participants were in these high risk of bias trials. Trials where the risk of bias was unclear accounted for 30% of those reviewed, while trials with a low risk of bias – those that can be trusted – accounted for just 8% of the total.
Bad trials – ones where we have little confidence in the results – are not just common, they represent the majority of trials in all countries and across most clinical areas. For instance, all trials looking at drugs and alcohol exhibited a high risk of bias. The most reliable field was anaesthesia, with 60% of trials exhibiting a low risk of bias.
The research team drew trial data from 96 reviews from 49 of the 53 clinical Cochrane Review Groups. Cochrane is an international organisation that helps to gather and propagate the results of medical research to better guide medical decision-making. This is done by experts compiling and evaluating research trials and results in “standardised, high-quality systematic reviews”.
Bad science was common everywhere. “No patient or member of the public should be in a bad trial and ethical committees, like funders, have a duty to stop this happening,” the paper’s authors write.
South Africa was bad, but Spain and Germany may be worse
In the seven trials reviewed that took place in South Africa, four had a high risk of bias, two had an unclear bias risk, and one trial was “good science”. This share of bad science is roughly similar to those found in the clinical trials done in the UK and USA. The most reliable health research science was done in multinational trials – with these, 23% of trials were a low risk of bias. (The authors didn’t identify the trials.)
The least reliable science, in countries that conducted 20 or more RCTs, was done in Spain and Germany, with 86% and 83% of the trials exhibiting a high risk of bias.
While results from just one year were interrogated, the paper’s authors found that their results map to similar studies, and that bad science can be expected to be the norm, over time.
This amounts to a massive waste of money and effort.
Statisticians and research method experts have been sounding the alarm on biased research for years, since Doug Altman’s 1994 paper in the British Medical Journal, “The scandal of poor medical research”.
Doctors want to know if they can rely on a particular treatment to produce a desired outcome, and need research that confers a degree of confidence. One way to do that – the most popular – is randomised control trials.
Randomised trials are great – but you need statisticians
Randomised control trials, also known as randomised trials, or RCTs, are for many (though not all), the gold standard for achieving scientific knowledge about a medical intervention – whether a drug or another type of therapy. The way that RCTs are conducted is crucial, as it is adherence to the method that gives people relying on the research confidence that the results produce scientific knowledge. See this explainer video for more: How do we know vaccines work?
But, if there is a high risk that the results were biased by errors in how they were conducted and how results were achieved, they should not be relied on. Pirosca and colleagues did not examine the type (or domain) of bias in the studies, arguing that having a high risk in one type of bias is sufficient to undermine the trial’s results.
In short, for Pirosca and colleagues, health research in randomised trials is bad when there is an identifiable risk of bias in the way that the results were obtained.
The large number of high risk of bias trials appears to be due to “a lack of input from methodologists and statisticians at the trial planning stage combined with insufficient knowledge of research methods among the trial teams”. You would not, they say by analogy, think it appropriate that a statistician conduct surgery, just because they are doing work in a surgical domain.
Bad science during COVID
Recent medical scandals in the headlines have highlighted the risks of bad science in medicine. The Covid pandemic has brought a boom in medical research, and popular attention to the results of medical research. This environment has produced some remarkable science, but it has also created scientific fiascos, like the one that surrounded ivermectin.
As GroundUp has previously reported, a review of studies investigating ivermectin as a possible therapy for Covid initially suggested that the deworming drug led to better outcomes in those that used it. On the face of it, the small studies that supported this conclusion seemed to provide promise for a low-cost, life-saving Covid intervention. But once the methodology and statistics were looked at closely, many of these papers were deemed unscientific – for instance, patients were excluded from analysis for no good reason. And once these trials were excluded from the review, the drug’s promise as a Covid treatment vanished.
Medical research watchdog Retraction Watch currently lists 12 papers purporting to investigate ivermectin that were subsequently withdrawn or for which concerns have been expressed. According to their records, 235 Covid papers have been withdrawn to date.
But the crisis is not insurmountable. Pirosca and colleagues say that relatively simple fixes would dramatically reduce the amount of untrustworthy health research – by ensuring that methodological principles that underlie RCTs are not compromised.
More expenditure on statistical expertise will save money
A 2015 review examined 142 trials that exhibited a high risk of bias. The authors found that in half of the high risk trials, the methodological adjustments required to reduce the risk of bias would have been low or zero cost. Easy adjustments at the design stage would have made important improvements to 42% of trials that exhibited high risk of bias.
Pirosca and colleagues propose that no medical RCT should be funded or given ethical approval if it cannot prove that the team conducting the trial has a member that has methodological and statistical expertise. Every RCT should, in its design, use risk of bias tools to make sure that results are not compromised.
The expertise that could restore the worth to medical research is in short supply.
More methodologists and statisticians are needed, and money should be invested in training people with this expertise, and investing in applied methodology research and supporting infrastructure. The authors call for 10% of a funder’s budget.
This might seem like a lot of money, but, argue Pirosca and co, it would be a fraction of the cost of the wasted research in the year under review – estimated to be billions of rands.
The task is urgent: “Randomised trials have the potential to improve health and wellbeing, change lives for the better and support economies through healthier populations … Society will only see the potential benefits of randomised trials if these studies are good, and, at the moment, most are not.”
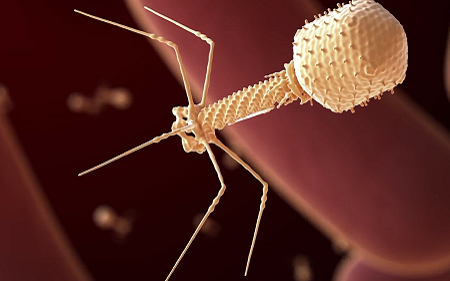
Using bacteriophages, viruses which prey on bacteria, is an emerging alternative to antibiotic use but with limited evidence. Now, with a new paper published in Clinical Infectious Diseases, collaborators report 20 new case studies on the use of the experimental treatment in Mycobacterium infections, with successes in more than half of the patients.
This is the largest ever set of published case studies for bacteriophage (or ‘phage’) therapy, giving unprecedented detail on their use to treat dire infections while laying the groundwork for a future clinical trial.
“Some of those are spectacular outcomes, and others are complicated,” said Professor Graham Hatfull at the University of Pittsburgh. “But when we do 20 cases, it becomes much more compelling that the phages are contributing to favourable outcomes – and in patients who have no other alternatives.”
The patients in the study had an infection from one or more strains of Mycobacterium, a group of bacteria that can cause deadly, treatment-resistant infections in those with compromised immune systems or cystic fibrosis. In 2019, Prof Hatfull led a team showing the first successful use of phages to treat one of these infections.
“For clinicians, these are really a nightmare: They’re not as common as some other types of infections, but they’re amongst some of the most difficult to treat with antibiotics,” said Prof Hatfull. “And especially when you take these antibiotics over extended periods of time, they’re toxic or not very well-tolerated.”
Since 2019, Prof Hatfull and his lab have fielded requests from more than 200 clinicians looking for treatments for their patients, working with them to find phages that could be effective against the particular strain of bacteria infecting each patient.
This newest paper, with collaborators from 20 institutions, dramatically expands the body of published evidence on the effectiveness of the therapy.
“These are incredibly brave physicians, jumping off the ledge to do an experimental therapy to try to help patients who have no other options,” said Prof Hatfull. “And each of these collaborations represents a marker that can move the field forward.”
Going on patient health and presence of Mycobacterium in samples, the team found that the therapy was successful in 11 out of 20 cases. No patients showed any adverse reactions to the treatment.
In another five patients the results of the therapy were inconclusive, and four patients showed no improvement. According to Prof Hatfull, even these apparent failures are key to making the therapy available to more patients. “In some ways, those are the most interesting cases,” he said. “Understanding why they didn’t work is going to be important.”
Several unexpected patterns emerged from the case studies. In 11 cases, researchers were unable to find more than one kind of phage that could kill the patient’s infection, even though standard practice would be to inject a cocktail of different viruses so the bacteria would be less likely to evolve resistance.
“If you’d asked me whether that was a good idea three years ago, I would have had a fit,” Prof Hatfull said. “But we just didn’t observe resistance, and we didn’t see a failure of treatment from resistance even when using only a single phage.”
Additionally, the team saw that some patients’ immune systems attacked the viruses, but only in a few cases did that render the virus ineffective. And in some instances, the treatment was still successful despite such an immune reaction. The study paints an encouraging picture for the therapy, said Prof Hatfull, opening up the possibility for new phage regimens that clinicians could use to maximise the treatment’s chance of success.
Along with the study’s significance to patients facing Mycobacterium infections, it also represents a substantial advance for the wider field of phage therapy. One concern is that researchers may be only publishing case studies of successful phage therapy.
“A series of consecutive case studies, where we’re not cherry-picking, is a much more transparent way of looking to see what works and what doesn’t,” said Prof Hatfull. “This adds considerable weight to the sense that the therapy is safe.”
This is still a very early stage in the development of phage therapy, and phages have not even begun to be tailored for treatment, Prof Hatfull said.
Researchers have helped isolate the Lloviu virus (LLOV), a close relative of Ebola virus, for the first time, showing that it could cross over into humans, highlighting the need for future research to ensure pandemic preparedness. The study is reported in Nature Communications.
LLOV is part of the filovirus family, which also includes the Ebola virus. While Ebola (and other filoviruses including the lethal Marburg virus) have only occurred naturally in Africa, Lloviu has been discovered in Europe. The filovirus LLOV, was genetically identified in 2002 in Schreiber’s bats in Spain and was subsequently detected in bats in Hungary.
As a zoonotic virus, LLOV is of public health interest to public health around the world due to our close relationship with animals in agriculture, as companions and in the natural environment. Increasing encroachment on the natural environment is creating more opportunities for zoonotic viruses to cross over into humans.
Dr Simon Scott, from the Viral Pseudotye Unit (VPU) at Medway School of Pharmacy were part of a team led by Dr Gábor Kemenesi from Pécs University/National Laboratory of Virology in Hungary. The VPU were involved in conducting all the antibody detection experiments using bat sera as part of the study, even before the virus itself was isolated. This isolation occurred in the Hungarian lab from the very last bat which tested LLOV positive.
The team discovered that Lloviu has the potential to both infect human cells and replicate, raising concerns about potential widespread transmission in Europe and urges immediate pathogenicity and antiviral studies. The VPU work also revealed no antibody cross-reactivity between LLOV and Ebola, suggesting that existing Ebola vaccines might not protect against Lloviu.
Dr Scott said that their research “is a smoking gun. It’s vital that we know both more about the distribution of this virus and that research is done in this area to assess the risks and to ensure we are prepared for potential epidemics and pandemics.”
The research revealed a considerable knowledge gap regarding the pathogenicity, animal hosts, and transmissibility of these newly discovered viruses. Dr Scott created a consortium of European bat virologists, harnessing expertise in the field, from ecology to virology, which is aiming to carry out essential further research across Europe into the risks of the Lloviu virus to humans.
In research published in Physics of Fluids, researchers used computer modelling investigate mask fit and found that face shape, especially natural facial asymmetry, influences the most ideal fit. The findings suggested that double masking with improperly fitted masks may not greatly improve mask efficiency and produces a false sense of security.
Using more layers results in a less porous face covering, leading to more flow forced out the sides, top, and bottom of masks with a less secure fit. Double layers increase filtering efficiency only with good mask fit, however they could also lead to difficulties in breathing.
The researchers modelled a moderate cough jet from a mouth of an adult male wearing a cloth mask over the nose and mouth with elastic bands wrapped around the ears. They calculated the maximum volume flow rates through the front of mask and peripheral gaps at different material porosity levels.
To create a more realistic 3D face shape and size, the researchers used head scan data for 100 adult male and 100 adult female heads.
Their model showed how the slight asymmetry typical in all facial structures can affect proper mask fitting. For example, a mask can have a tighter fit on the left side of the face than on the right side.
“Facial asymmetry is almost imperceivable to the eye but is made obvious by the cough flow through the mask,” explained co-author Tomas Solano, from Florida State University. “For this particular case, the only unfiltered leakage observed is through the top. However, for different face shapes, leakage through the bottom and sides of the mask is also possible.”
Producing individually customised ‘designer masks’ is not practical at large scales. Still, better masks can be designed for different populations by revealing general differences between male and female or child versus elderly facial structures and the associated air flow through masks.
Carbon monoxide (CO) is an odourless and colourless gas is produced from incomplete burning, and is a silent killer, binding to haemoglobin with few treatments available other than administering oxygen. Now, research published in Chemical Communications suggests a path to a possible antidote.
In the US, more than 400 deaths and 20 000 emergency room visits are attributable to carbon monoxide (CO) poisoning every year. While CO detectors and making sure fireplace and heaters work correctly can help prevent exposure, there are limited treatment options for those suffering from CO poisoning.
To address this, Tim Johnstone, an assistant professor of chemistry and biochemistry at UC Santa Cruz, has been working to develop an easy-to-administer antidote.
“If you are exposed to carbon monoxide, the primary treatment right now is fresh air,” said A/Prof Johnstone. “It is a question of time. In fresh air, you need four to six hours for the level of CO in your blood to be cut in half. With 100 percent oxygen or hyperbaric oxygen, the half-life shortens further. Even then, the high blood levels of CO can persist long enough to lead to long-term deficits and neurological problems.”
A/Prof Johnstone has been studying the chemistry of carbon monoxide. In a biological context, CO binds to metal centres such as the iron in haemoglobin, preventing this protein from carrying out its oxygen carrying function.
To mitigate this, A/Prof Johnstone has designed small molecules that possess many of the features of the active site of haemoglobin but can bind CO much more tightly than the protein. In his most recent study, his group described the ability of one such molecule to bind CO, sequester CO that is already bonded to haemoglobin, and rescue red blood cells exposed to CO: all promising signs for a future antidote.
These are early results, said A/Prof Johnstone, but the hope is to create a point-of-care treatment that can be administered quickly. The most common carbon monoxide poisoning symptoms are headache, dizziness, weakness, upset stomach, vomiting, chest pain, and confusion. Because it mimics the flu, people may experience symptoms without realizing the danger and delay seeking treatment.