A groundbreaking cancer drug could enhance how patients respond to chemotherapy even in treatment-resistant tumours.
The drug works by disarming a key defence mechanism that tumours use to protect themselves from treatment. In preclinical models, it has already shown promise in making chemotherapy-resistant cancers more responsive to therapy.
Chemotherapy is one of the most widely used cancer treatments, but it doesn’t always work as effectively as hoped. One major reason is that macrophages act as a barrier around tumours. These immune cells surround the blood vessels inside tumours and act like gatekeepers, blocking helpful immune cells from entering and doing their job in supporting the responses to chemotherapy.
The King’s College London scientists, who have launched a spinout company Aethox Therapeutics, found that these macrophages make a protein called heme oxygenase-1 (HO-1), which helps shield the tumour from the immune system and block the effects of chemotherapy. The new drug, KCL-HO-1i, targets this protein.
Professor James Arnold, Head of Tumour Immunology Group, King’s College London, said: “We discovered that these macrophages in cancer play a key role in blocking chemotherapy. By targeting the enzyme they produce using KCL-HO-1i, we were able to help beneficial immune cells and chemotherapy drugs become significantly more effective. In laboratory models, even chemotherapy-resistant tumours became responsive to treatment, which is a really exciting step forward.”
Unlike many cancer treatments that require hospital visits, KCL-HO1i is designed to be taken at home as a tablet between chemotherapy sessions. This makes it easier for patients to incorporate into their treatment plans without adding extra hospital burdens.
In early tests using mouse models of breast cancer, supported by funding by Cancer Research UK and Medical Research Council (MRC), the drug made tumours more responsive to a range of commonly used chemotherapies. These promising results suggest it could be used across a wide variety of cancer types and chemotherapy treatments.
The researchers hope that with funding, clinical trials on breast and other cancers could begin within two years.
Professor James Spicer, Professor of Experimental Cancer Medicine, King’s College London, said: “Chemotherapy remains a key part of treatment for many patients with cancer, but too often it is not as effective or long-lasting as we might like. This research has identified a key reason for these limitations, and discovered a drug that we are keen to test in the clinic alongside established chemotherapy drugs”.
This breakthrough is the result of a multidisciplinary collaboration between researchers including Professors James Arnold, James Spicer, and Miraz Rahman and their research teams at King’s College London.
If human trials are successful, KCL-HO-1i could become a valuable companion drug to existing cancer therapies – helping more patients to benefit from the treatments that are already available and reduce the need for more aggressive cancer therapies in the future.
Professor Miraz Rahman, Professor of Medicinal Chemistry, King’s College London
Study reveals that 1 in 10 will initiate opioid prescriptions long term.
Photo by Anna Shvets on Pexels
New research indicates that many patients who undergo surgery with the intent to cure early-stage cancer continue or start opioid prescriptions in the year following surgery. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
Pain management is essential during cancer care, but prescription opioid practices associated with cancer treatment may lead to unsafe long-term opioid use and adverse outcomes such as opioid use disorder and opioid overdose. To assess the situation, investigators examined rates of new persistent opioid use in the year following surgery for stage 0 to 3 cancers among 9213 U.S. Veterans who were opioid-naïve (not on prescribed opioids the year prior to their cancer diagnosis).
The team found that potentially dangerous co-prescription of opioid and benzodiazepine (a central nervous system depressant that treats anxiety, insomnia, and seizures and should not be combined with opioids) medications occurred in 366 (4.0%) Veterans during follow-up. Persistent opioid use occurred in 981 (10.6%). A higher intensity of exposure to opioid prescriptions during treatment was associated with these outcomes. People with a prior history of chronic pain, greater comorbidities, lower socioeconomic status, and who received adjuvant chemotherapy were at especially high risk of opioid use in the year after surgery.
“Minimising opioid exposure associated with cancer treatment while providing effective pain control will decrease long-term health risks among cancer survivors,” said lead author Marilyn M. Schapira, MD, MPH, of the University of Pennsylvania. “This is important as many patients are living longer after a cancer diagnosis and treatment.”
Gut Microbiome. Credit Darryl Leja National Human Genome Research Institute National Institutes Of Health
About a dozen studies in the past five years have made claims linking nearly every type of human cancer with the presence of microbiomes, “communities” of bacteria, viruses and fungi that live in or on peoples’ bodies. Now, scientists at Johns Hopkins Medicine say a study that sequenced human cancers found far less microbial DNA sequences than earlier studies reported in the same cancer tissue samples.
“It’s the nature of science to validate, confirm and reproduce findings,” says Steven Salzberg, PhD, Professor of Biomedical Engineering, Computer Science, and Biostatistics at The Johns Hopkins University. “Over time, we see a more complete picture of new research, and in this case, we did not find any associations between microbiomes and many types of cancer.”
Salzberg says details of the new study, published Sept. 3 in Science Translational Medicine, surveyed the whole genome sequences generated from 5734 tissue samples collected from 25 cancer types and stored in a large National Cancer Institute-funded database, The Cancer Genome Atlas (TCGA). About half of the samples are from normal tissues and blood, the other half from solid tumours and blood-based cancers.
The TCGA’s whole genome sequencing data contains millions of chopped up pieces of DNA molecules, known as reads, from each tissue sample. The original goal of the TCGA studies was to identify mutations in the DNA sequence of genes that might be associated with various cancer types. Sometimes, though, the original tumors might have microbes in them, and the reads could be used to identify those microbes.
Because reads often contain contaminants from bits of DNA left behind in sequencing machinery or picked up from the air or surfaces, samples can acquire DNA from those sources, as well as from the original tumour tissues. Salzberg says extraordinary efforts were made to identify such contaminants, preventing their study from displaying false results.
To rule out contaminants, Salzberg and his team relied on extensive experience with genomic sequencing and careful analysis of control samples to identify reads belonging to sequences known or highly likely to have contaminated samples.
For the current study, a continuation of one that the Johns Hopkins team published in 2023, Salzberg and first author Yuchen “Peter” Ge, a graduate student in biomedical engineering at Johns Hopkins, removed human DNA sequences from the TCGA data sets by mapping each read against two human reference genomes – one from the Telomere-to-Telomere (T2T) project and another from the Genome Reference Consortium.
After removing human DNA, the research team was left with, on average, 2.4 million reads per sample, or about 0.35% of the total 6.5 billion tumour sample reads. Of these, the research team found 323 million human DNA reads that weren’t eliminated in the first pass and 986 million reads they classified as contaminants.
They next compared the remaining sequencing reads against a database containing 50 651 genomes representing 30,355 species of bacteria, viruses, fungi and archaea (single-celled organisms that aren’t bacteria or viruses).
After removing human DNA sequences and contaminants, the average proportion of microbial DNA reads in solid tumour samples was 0.57% and 0.73% in blood cancers.
The Johns Hopkins researchers then compared their new results to a study published five years ago in the journal Nature [since retracted, because of concerns about contaminants in the microbial data], and found the previous study identified 56 times as many microbial reads as the new study for half of the total microbial reads. And 5% of the time, the previous study found 9,000 times the number of microbial reads as the current Johns Hopkins study. Salzberg says the microbial reads in the retracted study were highly likely to be contaminants.
“This disparity in the number of microbial reads didn’t occur in just a few samples,” says Salzberg. “Over the whole study, the previous researchers found far more microbial reads than we did.”
In another comparison of a study published in Cell in 2022 and the current Johns Hopkins work, the 2022 study reported fungal DNA amounts that were hundreds of times more than what was found in the current Johns Hopkins study, largely due to contaminants.
Among the DNA samples in the current Johns Hopkins study, in which they did find microbiome DNA, the researchers found microbes that have long been linked with human cancer, such as HPV (linked with cervical and some head and neck cancers), Helicobacter pylori (linked to stomach cancer), and Fusobacterium nucleatum and Bacteroides fragilis (linked with GI cancers).
The current Johns Hopkins study and the previous ones published in Cell and Nature reported microbiomes of Saccharomyces cerevisiae, commonly known as baker’s yeast. “It’s one of the most common contaminants in sequencing labs,” says Salzberg. They also found a virus that infects plant fungi, Rosellinia necatrix partitivirus 8, which has no known link to human disease.
Salzberg said the need to carefully document claims about the links between cancer and microbiomes is “especially important” as efforts ramp up to diagnose cancers early using microbiome information.
The Johns Hopkins researchers have made their sequencing analysis data available online to other scientists in the supplementary materials in Science Translational Medicine and online.
In the latest chapter of a long-running legal battle over the Gauteng Department of Health’s obligation to provide people in the province with radiation oncology services, the department has suffered another loss in the courts. Spotlight assesses the legal situation and asks what it means for people still waiting for the life-saving treatment.
With another court loss suffered this August, the Gauteng Department of Health has once again been ordered to urgently provide treatment for cancer patients who have been left in the lurch.
This ruling, handed down on August 5 by Judge Evette Dippenaar, follows urgent legal action brought by the Cancer Alliance. It was in response to the Gauteng health department’s appeal against a ruling handed down on March 27 by acting Judge Stephen van Nieuwenhuizen. That order compelled the department to clear its years-long backlogs in getting cancer treatment to patients.
In its March ruling, the South Gauteng High Court in Johannesburg found the department’s failure to deliver this critical treatment to be unconstitutional and unlawful. The decision follows the department’s failure to spend a R784 million allocation granted by the provincial Treasury in 2023 to reduce the treatment backlog by outsourcing services to the private sector over a three-year period. Due to severe delays, the department was forced to return the first R250 million tranche.
Van Nieuwenhuizen strongly criticised the department, stating: “The provincial health respondents have done nothing meaningful since the money was allocated in March 2023 to actually provide radiation oncology treatment to the cancer patients. Meanwhile, the health and general well-being of the patients has significantly deteriorated. There is clear, ongoing, and irreparable harm being suffered by those still waiting for treatment.”
He also condemned the department for its lack of accountability and poor management of public resources, finding that it had failed to uphold ethical standards, act transparently, or respond to patients’ needs fairly and effectively.
The court instructed the department to:
Take immediate action, including diversion to private facilities, to provide radiation oncology services to all patients on the backlog list,
Update the backlog list within 45 days,
Submit a detailed progress report on efforts to deliver treatment, and
Present a long-term plan for ongoing cancer treatment services within three months.
But Gauteng health MEC Nomantu Nkomo-Ralehoko and the health department challenged the judgment in May, just as their 45 days to act ran out. They chose instead to take the entire matter on appeal to the Supreme Court of Appeal (SCA).
In response, the Cancer Alliance, represented by SECTION27 (*see disclosure), went back to court for an interim order to make the March 27 ruling immediately enforceable, and not suspended until a ruling is made by the SCA. It is in response to this application that Judge Dippenaar ruled on August 5 that the March ruling is indeed immediately enforceable.
Two courts have now sent a clear message to the Gauteng health department, says attorney Khanyisa Mapipa, who heads health rights at SECTION27. She adds: “The Gauteng Department of Health’s action should be in the interest of the person who is seeking treatment. It should not be to deny, deny, deny and then to fight in the courts and not take any accountability.”
The waiting list
The estimated number of people on a waiting list for cancer treatment in 2022 was around 3 000 people. New data on this has not been made publicly available.
There are some signs of progress, although details are hard to pin down. In a statement released on August 24, which reiterates a July 20 statement, the Gauteng health department said it had introduced a strategic partnership with private service providers. “As the beginning of August 2025, 563 patients were receiving radiation oncology care through private partnerships, while 1 076 patients had completed treatment by end of July 2025,” it stated.
Both statements also noted that work was underway to complete new radiotherapy centres at Chris Hani Baragwanath and Dr George Mukhari Academic Hospitals.
But Mapipa says they still don’t have full details that comply with the court order. “What we’re asking for essentially is what the department should be doing anyway and that is for them to go through their patient files to establish who is still on the backlog list; who has passed away, who has received treatment, when patients were last assessed and what treatment they qualify for; and if it was a public facility or were they diverted to a private facility,” she says.
“As the judge pointed out in March, the department has to do this as a constitutional obligation, whether they fight this to the Constitutional Court or not, their obligation is to provide treatment for people who meet the criteria. Those on the backlog list meets the criteria,” she says.
Part of the March order also compelled the department to file progress reports with the court within three months on the measures taken to provide treatment and its long-term plans to resolve the ongoing cancer treatment crisis in Gauteng. Spotlight’s understanding is that these progress reports have not been submitted.
This is an important measure, Mapipa says, given the department’s poor track record. “The court rulings in both judgments found that because they have failed to be transparent throughout this process, the department is compelled to provide these reports to the courts,” she adds.
It is as yet unclear how the Gauteng health department plans to proceed. The department, in its three-paragraph statement following the August judgment, stated that it would review “the contents and implications” to determine and communicate its next steps. Their deadline to appeal the August 5 ruling was 26 August 2025. The department did not respond to questions from Spotlight.
Calls for accountability
Jack Bloom, Democratic Alliance shadow health MEC in Gauteng, says that without a proper audit and update of the backlog list of patients needing care, the “cancer treatment scandal has probably cost more lives than the 144 mental patients who died in the Life Esidimeni tragedy when they were sent to illegal NGOs”.
Bloom is calling for heads to roll, with Nkomo-Ralehoko and head of department Arnold Lesiba Malotana in his crosshairs.
“The DA condemns the department’s legal stalling tactics that harms patients who urgently require lifesaving treatment…Premier [Panyaza] Lesufi should not allow this cancer disaster to continue,” he says.
Salomé Meyer, spokesperson for Cancer Alliance, says that the legal proceedings are a distraction of the realities on the hospital floor. Charlotte Maxeke Johannesburg Academic Hospital for instance, she says, remains in “crisis”. She maintains there is a scarcity of sufficient and operational radiation oncology machinery, as well as extreme shortages in radiation oncology staff to operate the machines.
Meyer says the situation at Charlotte Maxeke Hospital dates back to 2017 when CEO Gladys Bagoshi was made aware of mounting challenges from a shortage of equipment and staffing.
“In 2021, Bagoshi turned down an equipment allocation, which Charlotte Maxeke Hospital desperately needed, so this allocation went to George Mukhari Hospital and Chris Hani Baragwanath Hospital instead. But the cobalt bunkers required to house the machines at these hospitals had not been built and are only expected to be completed in 2026 – so the machines remain in storage. In 2022, an order was finally placed for additional linacs [used for high energy beam radiation treatments] for the existing cobalt bunkers at Charlotte Maxeke Hospital, but that tender is still not finalised,” says Meyer.
She adds: “This is a failure of planning, governance, and accountability and we have to ask who is being held accountable when the same CEO has remained in place all these years.”
Neither Bagoshi nor the health department responded to questions on these assertions.
Disclosure: SECTION27 was involved in the court proceedings described in this article. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. The Spotlight editors gave special attention to maintaining this editorial firewall in the production of this story.
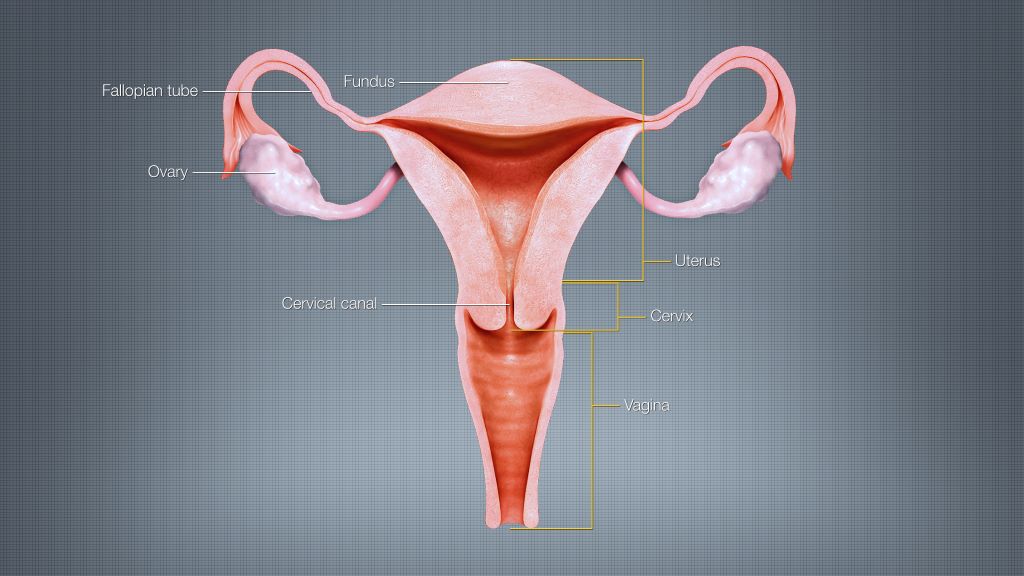
In a recent paper published in Nature, researchers at the University of Chicago discovered how to block nicotinamide N-methyl transferase (NNMT), an enzyme that is involved in the progression of high-grade serous ovarian cancer. The team showed that NNMT promotes cancer growth by helping the tumour evade the immune system, and they also developed a potent NNMT inhibitor that could help overcome therapy resistance, providing a new and effective strategy for treating ovarian cancer.
A common yet deadly form of ovarian cancer
High-grade serous ovarian cancer is the most common and deadly form of ovarian cancer. It is often diagnosed at advanced stages and is notoriously challenging to treat. Although surgery and chemotherapy initially provide substantial benefits, the cancer frequently recurs, leading to low survival rates. Immunotherapy, a breakthrough treatment for many cancers, has failed in ovarian cancer, largely because activity of surrounding cells has been programmed by the tumour to suppress the immune response. These cells, known as cancer-associated fibroblasts (CAFs), differ from normal fibroblasts, which play a vital role in supporting tissue integrity and facilitating wound healing. Instead, CAFs surround the tumor, offer protection, and release signals that weaken immune responses and promote metastasis.
“Most therapies focus on the cancer cells, but we are interested in the fibroblasts in the surrounding stroma. These cells don’t mutate like cancer cells, which makes them more stable and, we think, more targetable,” said Ernst Lengyel, MD, PhD, Professor and Chair of Obstetrics and Gynecology at UChicago and lead author of the paper. “We have pinpointed the mechanism behind CAF activation and found a drug that can halt it in its tracks.”
NNMT: A master regulator
In a landmark 2019 Nature study, Lengyel’s team showed that NNMT, a metabolic enzyme, is highly expressed in CAFs and converts normal fibroblasts into tumour-promoting fibroblasts by changing epigenetic and metabolic programming. The new Nature study demonstrates how NNMT promotes immune evasion and how to stop it. The UChicago team discovered that NNMT-expressing CAFs secrete complementary proteins, which convert monocytes (a type of white blood cells) into myeloid-derived suppressor cells (MDSCs).
“The enzyme NNMT induces widespread epigenetic changes in fibroblasts that promote tumour growth. Inhibiting NNMT has the potential to reverse these changes and reduce the tumour-supportive role of fibroblasts,” says Janna Heide, MD, a postdoctoral researcher in the Lengyel Lab and first author of the study.
Better results with combined NNMT inhibitor and immunotherapy
To translate these findings into treatment, the team collaborated with scientists at the National Center for Advancing Translational Sciences (NCATS) and the National Cancer Institute (NCI) Experimental Therapeutics (NExT) program, which supports early-stage drug development with high translational potential. After screening over 150 000 compounds, they identified a highly targeted NNMT inhibitor. In preclinical animal models of ovarian cancer, the NNMT inhibitor decreased tumour burden and restored immune activity. Most importantly, when the inhibitor was combined with immune checkpoint inhibitors, it halted tumour growth.
Historically, drug development has focused almost entirely on cancer cells. This study demonstrates that non-cancerous cells in the tumour microenvironment can also play a crucial role in disease progression and treatment resistance. Targeting CAFs through NNMT inhibition offers a new therapeutic approach to overcome these barriers.
“Immunotherapy hasn’t worked in ovarian cancer, but the combination therapy of an NNMT inhibitor with immunotherapy worked remarkably well in our preclinical models,” Lengyel said. “It was exciting to show that tumor growth can be controlled without even touching the cancer cells, just by reprogramming the supporting cells around them.”
Lengyel said this research was only possible through the partnership with the National Center for Advancing Translational Sciences and the collaborative spirit at the UChicago, particularly with Ralph Weichselbaum, MD, Chair of the Department of Radiation Oncology, an expert in immune regulation, and his team, including postdoctoral researcher András Piffkó, MD. This work is part of Lengyel’s broader efforts to transform ovarian cancer treatment, supported by an NCI Outstanding Investigator Award (R35), which funds long-term, high-impact research with the potential to change clinical practices.
“Without NIH funding, we simply couldn’t have accomplished this,” Lengyel said. “It allowed us to take risks, innovate, and ultimately develop something that might help patients.”
Eating animal-sourced protein foods is not linked to a higher risk of death and may even offer protective benefits against cancer-related mortality, new research finds.
The study, published in Applied Physiology, Nutrition, and Metabolism, analysed data from nearly 16 000 adults aged 19 and older using the National Health and Nutrition Examination Survey (NHAMES III).
Researchers examined how much animal and plant protein people typically consume and whether those patterns were associated with their risk of dying from heart disease, cancer or any cause.
They found no increased risk of death associated with higher intake of animal protein. In fact, the data showed a modest but significant reduction in cancer-related mortality among those who ate more animal protein.
“There’s a lot of confusion around protein – how much to eat, what kind and what it means for long-term health. This study adds clarity, which is important for anyone trying to make informed, evidence-based decisions about what they eat,” explains Stuart Phillips, Professor and Chair of the Department of Kinesiology at McMaster University, who supervised the research.
To ensure reliable results, the team employed advanced statistical methods, including the National Cancer Institute (NCI) method and multivariate Markov Chain Monte Carlo (MCMC) modelling, to estimate long-term dietary intake and minimize measurement error.
“It was imperative that our analysis used the most rigorous, gold standard methods to assess usual intake and mortality risk. These methods allowed us to account for fluctuations in daily protein intake and provide a more accurate picture of long-term eating habits,” says Phillips.
The researchers found no associations between total protein, animal protein or plant protein and risk of death from any cause, cardiovascular disease, or cancer. When both plant and animal protein were included in the analysis, the results remained consistent, suggesting that plant protein has a minimal impact on cancer mortality, while animal protein may offer a small protective effect.
Observational studies like this one cannot prove cause and effect; however, they are valuable for identifying patterns and associations in large populations. Combined with decades of clinical trial evidence, the findings support the inclusion of animal proteins as part of a healthy dietary pattern.
“When both observational data like this and clinical research are considered, it’s clear both animal and plant protein foods promote health and longevity,” says lead researcher Yanni Papanikolaou, MPH, president, Nutritional Strategies.
This research was funded by the National Cattlemen’s Beef Association (NCBA), a contractor to the Beef Checkoff. NCBA was not involved in the study design, data collection and analysis or publication of the findings.
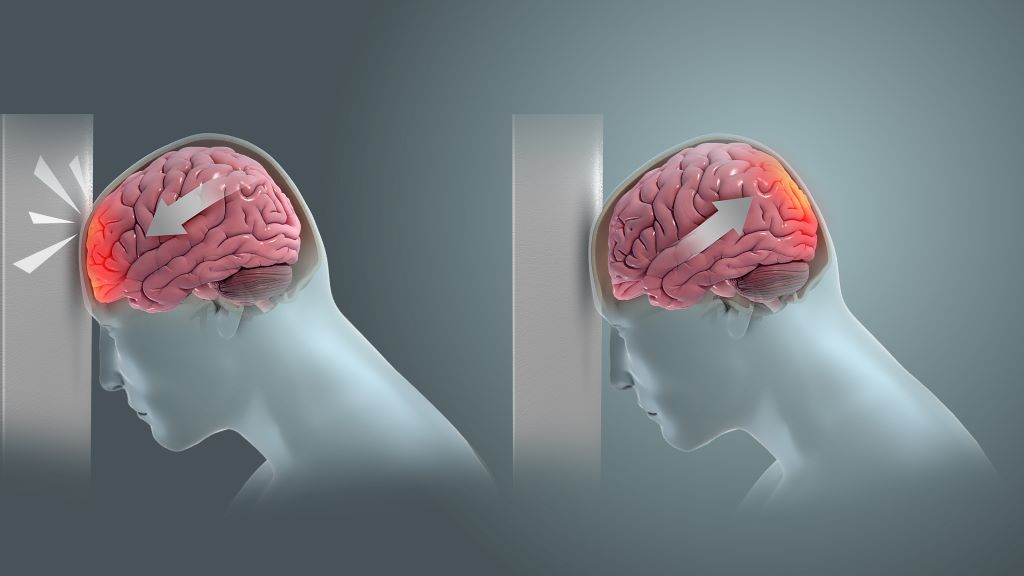
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
New research led by investigators at Mass General Brigham suggests a link between a history of traumatic brain injury (TBI) and risk of developing a malignant brain tumour. By evaluating data from 2000–2024 of more than 75 000 people with a history of mild, moderate or severe TBI, the team found the risk of developing a malignant brain tumour was significantly higher compared to people without a history of TBI. The results were published in JAMA Network Open.
“I see these results as alarming,” said co-senior author and corresponding author Saef Izzy, MD, FNCS, FAAN, a neurologist and head of the Immunology of CNS Injury Program at Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system. “Our work over the past five years has shown that TBI is a chronic condition with lasting effects. Now, evidence of a potential increased risk of malignant brain tumours adds urgency to shift the focus from short-term recovery to lifelong vigilance.
“Alongside our earlier findings linking TBI and cardiovascular disease, this underscores the importance of long-term monitoring for anyone with a history of TBI.”
The team divided the severity of TBI between mild, moderate and severe, with participants suffering from incidents ranging from car accidents to falls. In the two categories of moderate and severe, 0.6% of people (87 out of 14 944) developed brain tumours within 3-to-5 years after the TBI, which was a higher percentage than controls. Mild cases of TBI, such as those caused by concussions, were not associated with an increased risk of tumour. The aim of the study was not to establish a cause-and-effect link between moderate-to-severe TBI and malignant tumours, but rather to explore whether an association exists. Determining causality and understanding the underlying mechanisms will require a dedicated translational study in the future.
A previous study showed veterans of the Iraq and Afghanistan wars who suffered TBI experienced an increased risk of brain tumours, but previous studies on civilian populations showed conflicting results. The collaborative team of researchers used an international disease classifying system known as ICD codes to exclude anyone in the study with a history of brain tumour, benign tumours, and risk factors such as radiation exposure.
Previous neurotrauma studies from Mass General Brigham have looked at patients with a history of TBI and found an association with the emergence of anxiety, depression, and other psychiatric, neurological, and cardiovascular diseases, but the current study focuses on malignant tumour development.
Future imaging studies could draw a connection between the location of the TBI and where tumours developed in the brains of participants. The team would like to further study patients with repeated injuries, such as falls.
“While there is an increased risk of tumour from TBI, the overall risk remains low. Still, brain tumour is a devastating disease and often gets detected in later stages,” said lead author Sandro Marini, MD, a neurologist at Mass General Brigham. “Now, we’ve opened the door to monitor TBI patients more closely.”
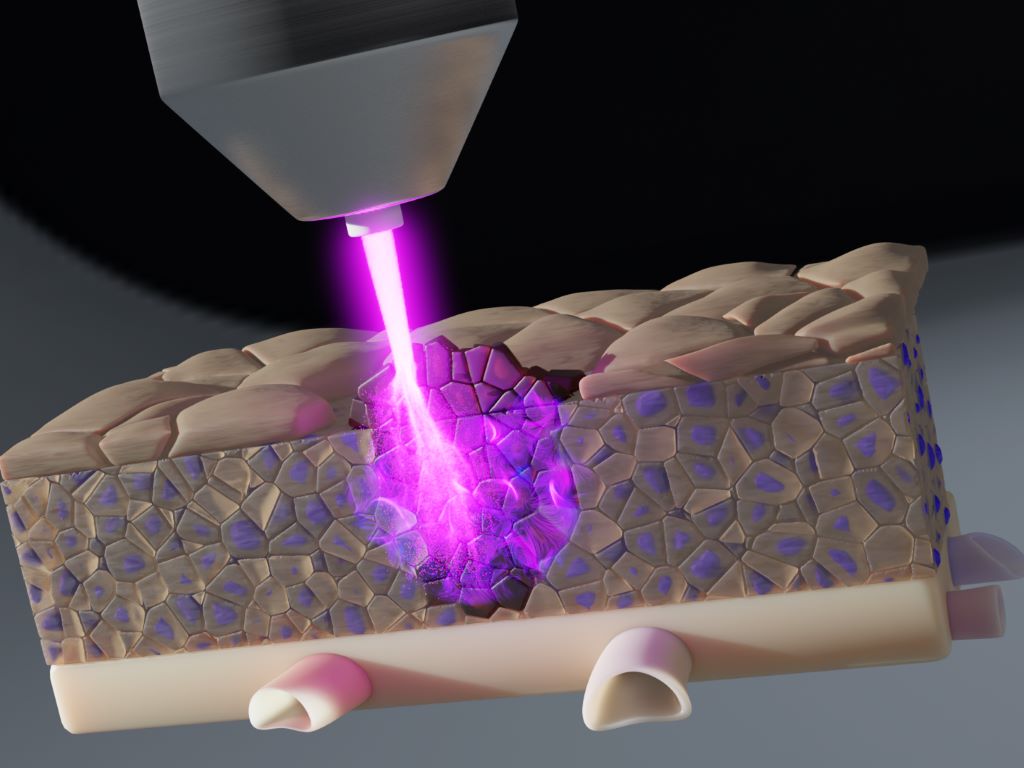
Researchers at the Leibniz Institute for Plasma Science and Technology (INP) have collaborated with partners at Greifswald University Hospital and University Medical Centre Rostock to demonstrate that cold plasma can effectively combat tumour cells even in deeper tissue layers. What is particularly noteworthy is that, by developing new tissue models, they were able to precisely investigate the effect of individual plasma components on tumour cells for the first time.
Plasma is an ionised gas that produces a large number of chemically reactive molecules known as reactive oxygen and nitrogen species. These short-lived molecules can have a strong influence on biological processes such as the growth or death of tumour cells.
New tissue models provide important insights
“The effect of plasma in tissue is very complex and little understood. We have therefore developed a 3D model made of hydrogels that mimics real tumour tissue. In this model, we were able to observe exactly how deep the molecules from the plasma penetrate – and which of these molecules are important for the effect on tumour cells,” explains Lea Miebach, first author of the study. Particularly short-lived molecules such as peroxynitrite penetrated several millimetres deep into the tissue. Hydrogen peroxide, which had previously been considered the main active ingredient in laboratory research, showed little effect: even when it was specifically removed, the effect of the plasma remained strong.
Use during surgery also conceivable
Another model investigated how well plasma could work in the follow-up treatment of tumour surgery. Residual tumour cells at the edge of an artificial surgical wound were specifically treated with plasma. The result: here too, a strong effect was observed, especially in cells that had already spread into the surrounding tissue. These findings could help to better prevent relapses after surgery.
Important step for plasma medicine
“Our results could significantly improve the medical application of plasma,” says Prof Dr Sander Bekeschus, head of the Plasma Medicine research programme at INP. “The better we understand which molecules are active in the tissue, the more precisely plasma devices can be used for specific types of cancer.”
The work was carried out using the medically approved plasma jet “kINPen”. In the long term, the method could help make therapies more effective and gentler.
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
Increased activity in a specific biological pathway may explain why many patients with a deadly form of skin cancer do not respond to the latest cancer treatments, a new study shows.
Publishing in the journal Cancer Research, the study featured data generated from experiments with human tissues and cells from patients with advanced melanoma that were implanted into mice. Results uncovered therapeutic targets that could limit melanoma growth in patients whose cancer failed to respond to initial treatment with immune checkpoint inhibitors.
Led by researchers at NYU Langone Health and its Perlmutter Cancer Center, the study focused on a subgroup of melanoma patients with mutations in the neurofibromin 1 (NF1) gene. NF1 mutations are just one type among several mutations, including those in the BRAF, NRAS, and PARP genes, that are linked to many cases of cancer, particularly melanoma. As many as 27% of melanoma patients are estimated to have NF1 mutations.
While immunotherapy, which stimulates the immune system to attack cancer cells as it would an invading virus, has proved to be a successful treatment, it does not work well for more than half of NF1-mutant melanoma patients.
“There is a pressing need for new drug therapies for melanoma patients with neurofibromin 1 mutations that do not respond to the latest immunotherapy, and for which there are no subsequent effective treatment options,” said study lead investigator Milad Ibrahim, PhD. Ibrahim is a postdoctoral fellow in the Dr Iman Osman Laboratory in the Ronald O. Perelman Department of Dermatology at the NYU Grossman School of Medicine.
To investigate why these patients were treatment resistant, investigators examined tumour cells from 30 melanoma patients who did not respond to immunotherapy. NF1 mutations were found in 40% of these melanoma samples. The samples came from NYU Langone’s extensive repository from more than 6000 melanoma patients.
Molecular testing showed that the signalling pathway built around a protein called epidermal growth factor receptor (EGFR) was more active in NF1 mutant melanoma cells than in cells with other melanoma-gene mutations. Increased EGFR activity has long been linked to abnormal cell growth in tumours and shorter survival with various cancers. The researchers also found that NF1 mutant melanoma cells depended on increased EGFR activity for survival, regardless of the presence of other mutations.
Because EGFR-inhibiting drugs are already used to treat some head and neck cancers, as well as colorectal and lung cancers, researchers then tested two drugs in the class, cetuximab and afatinib, in both NF1 mutant cell cultures and cancer cell lines without NF1 mutations. After transplanting both tumour cell types into mice and treating them with these drugs, results showed that both EGFR inhibitors were effective against cells and transplanted tumours with NF1 mutations, and they had no effect on melanomas without NF1 mutations.
“Our study results reveal a unique vulnerability in melanoma patients with neurofibromin 1 mutations, that an overexpression of the epidermal growth factor receptor pathway is essential for their survival and growth,” said the study’s senior investigator, Professor Iman Osman, MD.
“While further tests are needed, our results support a novel approach of deploying EGFR inhibitors either alone or in combination with other immunotherapies for treatment of melanoma patients whose tumours harbour NF1 mutation,” said the study’s co-senior investigator, Associate Professor Markus Schober, PhD.
However, Schober says this requires further testing in a clinical trial, which the research team plans to develop. He adds that if trial findings prove successful, the team’s research could provide a lifeline for many of these melanoma patients.
Immune cells (red) accumulating within a tumour (blue) and multiplying (green). When blood flow is blocked either in the heart or legs, these immune cells change in a way that enables tumour growth. Credit: NYU Langone
Cutting off blood flow can prematurely age the bone marrow, weakening the immune system’s ability to fight cancer, according to a new study from NYU Langone Health.
Published online August 19 in JACC: CardioOncology, the study showed that peripheral ischaemia, restricted blood flow in the arteries in the legs, caused breast tumours in mice to grow at double the rate seen in mice without restricted flow. These findings build on a 2020 study from the same team that found ischemia during a heart attack to have the same effect.
Ischaemia occurs when fatty deposits, such as cholesterol, accumulate in artery walls, leading to inflammation and clotting that restrict the flow of oxygen-rich blood. When this happens in the legs, it causes peripheral artery disease, which can increase the risk of heart attack or stroke.
“Our study shows that impaired blood flow drives cancer growth regardless of where it happens in the body,” says corresponding author Kathryn J. Moore, PhD, tProfessor of Cardiology at NYU Grossman School of Medicine. “This link between peripheral artery disease and breast cancer growth underscores the critical importance of addressing metabolic and vascular risk factors as part of a comprehensive cancer treatment strategy.”
Importantly, the research team found that restricted blood flow triggers a shift toward immune cell populations that cannot efficiently fight infections and cancer, mirroring changes seen with aging.
Systemic Skewing
To examine the mechanisms behind the link between cardiovascular disease and cancer growth, the study authors developed a mouse model with breast tumours and induced temporary ischaemia in one hind limb. The team then compared cancer growth in mice with and without impaired blood flow.
Their findings build on the nature of the immune system, which evolved to attack invading bacteria and viruses, and under normal conditions detects and eliminates cancer cells. These protective functions rely on stem cell reserves in the bone marrow, which can be activated as needed to produce key white blood cell populations throughout life.
Normally, the immune system responds to injury or infection by ramping up inflammation to eliminate threats, then scaling back to avoid harm to healthy tissue. This balance is maintained by a mix of immune cells that either activate or suppress inflammation. The researchers found that reduced blood flow disrupts this equilibrium. It reprograms stem cells in the bone marrow to favour the production of “myeloid” immune cells (monocytes, macrophages, neutrophils) that dampen immune responses, while reducing output of lymphocytes like T cells that help to mount strong antitumour responses.
The local environment within tumours showed a similar shift, accumulating more immune-suppressive cells, including Ly6Chi monocytes, M2-like F4/80+ MHCIIlo macrophages, and regulatory T cells, that shield cancer from immune attack.
Further experiments showed that these immune changes were long-lasting. Ischaemia not only altered the expression of hundreds of genes, shifting immune cells into a more cancer-tolerant state, but also reorganised the structure of chromatin, the protein scaffolding that controls access to DNA. This made it harder for immune cells to activate genes involved in fighting cancer.
“Our results reveal a direct mechanism by which ischemia drives cancer growth, reprogramming stem cells in ways that resemble aging and promote immune tolerance,” says first author Alexandra Newman, PhD, a postdoctoral scholar in Dr Moore’s lab. “These findings open the door to new strategies in cancer prevention and treatment, like earlier cancer screening for patients with peripheral artery disease and using inflammation-modulating therapies, to counter these effects.”
Moving forward, the research team hopes to help design clinical studies that evaluate whether existing inflammation-targeted therapies can counter post-ischaemic changes driving tumour growth.