New research shows grass allergen levels are more consistently associated with hay fever symptoms than grass pollen counts.
The research, published in The Journal of Allergy and Clinical Immunology and led by King’s College London and Imperial College London, shows for the first time that measuring airborne allergen levels will help people with hay fever better control their symptoms.
In the UK, 1 in 4 adults suffer from hay fever from late-March to September. Symptoms include a runny or blocked nose, sneezing and coughing and itchy, red or watery eyes.
Hay fever can make lung conditions such as asthma worse, causing wheezing and breathing difficulties which can lead to hospitalisation.
Many people with hay fever monitor peak pollen times to manage their symptoms. In the UK (as well as South Africa), pollen grains are manually measured to find the daily pollen count.
But the study authors say measuring allergen levels instead will be more accurate as each pollen grain can release a different amount of allergen each day, and it is the allergens in the air that are primarily responsible for causing hay fever symptoms.
Currently, there is no regular monitoring of allergen levels in the UK or elsewhere.
Authors collected daily symptom and medication scores from adult participants in an allergy clinical trial as well as daily counts of asthma hospital admissions in London.
They measured grass pollen counts and but also sampled air for the grass pollen Phl p 5 grass allergen protein in the same location at King’s College London over the same time period.
First author Dr. Elaine Fuertes, from Imperial College London, said: “Grass pollen is the most common hay fever trigger. In this study, we measured grass allergen (Phl p 5) levels and found this was more consistently associated with allergic respiratory symptoms than grass pollen counts.”
Senior author Professor Stephen Till, from King’s College London, said: “High pollen season can be serious for people who suffer with hay fever, and can trigger severe asthma attacks in those who are allergic to grass pollen. This study shows there is a superior way of measuring pollen allergens in the air than the traditional pollen count. Monitoring grass allergen instead of grass pollen counts gives results that are more consistently linked to patients’ symptoms and could allow people with serious allergies to be better prepared during the pollen season.”
Research is ongoing to see whether regular measurement of allergen levels can become the standard in the UK, and whether there are other environmental factors, such as meteorological factors including temperature, wind, humidity, and air pollutants, that influence how much allergen each pollen grain releases.
“The path to ending AIDS is clear,” states a recent UNAIDS report. “HIV responses succeed when they are anchored in strong political leadership, have adequate resources, follow the evidence, use inclusive and rights-based approaches, and pursue equity. Countries that are putting people first in their policies and programmes are already leading the world on the journey to ending AIDS by 2030,” it reads.
Ending AIDS and the HIV epidemic mean different things to different people.
This very ambitious language is found in Sustainable Development Goal 3.3: “By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases”. The global target is to reduce the newly HIV infected population (per 1 000 uninfected population) to 0.05 by 2025 and to 0.025 by 2030.
Another version is “ending AIDS as a public health threat by 2030” which has been characterised as being “consistent with the three zeros vision: zero deaths, zero new infections and zero discrimination, operationalized as a 90% reduction of annual new HIV infections and AIDS-related deaths in 2030 compared to 2010”.
A third approach calls for countries to reach the 95-95-95 targets – 95% of people living with HIV are diagnosed, 95% of those that have been diagnosed are on antiretroviral treatment and 95% of those on treatment are virally suppressed – by 2025.
A fourth, more realistic approach, is to reduce the number of new HIV infections below the number of deaths from HIV – labelled ‘epidemic control’ – to an endemic status beyond 2030.
Regardless of the definition of ‘ending AIDS’, what should South Africa do in determining its path towards reducing the burden of HIV?
First, let’s start with what we think the HIV epidemic will look like in 2030. Whilst we do not have a crystal ball, we do have a well-recognised mathematical model – the Thembisa model, which is also used as the basis for UNAIDS’s HIV estimates for South Africa. The latest Thembisa model outputs, published last year, include projections up to 2030.
The model projects that in 2030 there will be around 128 535 new HIV infections with the bulk of these, over 54% (70 412) being young women between the ages of 15 and 24 years. Using the definition of a 90% decrease in new infections between 2010 and 2030, South Africa is projected to reach 65.7%.
The model projects that in 2030 around 8.1 million people will be living with HIV with 6.4 million being on antiretroviral treatment. The total number of AIDS deaths projected by the model in 2030 is 40 486 compared to 149 257 deaths in 2010. (This is a 72.9% reduction – not quite the 90% expected by one of the definitions noted above).
How well is the country doing in reaching the 95-95-95 targets?
According to the Thembisa model, the percentage of people ever tested for HIV stood at 83.7% in 2022 (projected to reach 86.1% in 2030). The percentage of people living with HIV who had been diagnosed was at 94.5% in 2022 and projected to reach 96.4% in 2030. The percentage of diagnosed people on treatment in 2022 stood at 77.4% and is projected to reach 81.1% in 2030.
The percentage of all people living with HIV who were virally suppressed was at 65.4% in 2022 and projected to reach 71.3% in 2030. (These percentages are slightly higher if a viral load cut-off of 1000 copies/mL rather than 400 is used). This means only one of the 95s (percent diagnosed) is expected to be reached. (If the third 95 is defined as percentage of people on HIV treatment who are virally suppressed, rather than percentage of all people living with HIV who are virally suppressed, it will also be met.)
A more optimistic picture has been reported by the Human Sciences Research Council (HSRC) through their recently completed national survey. This survey found that 90% of 15-year-olds and older living with HIV knew their status (this included self-reported status), with 91% of them on treatment, and 94% of those on treatment being virally suppressed (at the 1000 copies/mL threshold).
Based on the Thembisa projections, South Africa is not expected to reach epidemic control by 2030. So, what needs to be done to achieve significantly fewer new infections and deaths?
What to do
In his address to the 2023 South African AIDS conference, the Minister of Health outlined what the Department of Health considered as necessary. He noted that the country has achieved 94:77:92 against the UNAIDS targets – far lower than the HSRC survey found. This means that, according to the Department’s data, there are over two million people who are living with HIV but not on treatment and a further 1.6 million people who are on treatment but are not virally suppressed. This is far higher than the 1.9 million that the HSRC survey suggests are not on treatment and not virally suppressed.
Regardless of which data is correct, it is urgent that these patients are found, initiated on treatment and supported to reach viral suppression.
While the Minister did not quantify the number of people living with HIV who are not being reached, he did outline the following interventions that he proposed should be prioritised:
Immediate implementation of the revised and consolidated ART Clinical Guidelines, which includes an integrated approach on prevention of vertical transmission, a focus on TB/HIV given high levels of coinfection, and differentiated service delivery.
A focus on the 100 identified health facilities which are lagging in reaching the 2nd and 3rd 95s (treatment coverage and viral suppression).
The need to close the testing and treatment gaps for men and children through HIV self-testing and index testing (an approach whereby the exposed contacts of an HIV-positive person are notified and offered an HIV test).
A focus on re-engaging those who have stopped taking treatment and scaling up of community treatment, 3-month dispensing of treatment medication as well as the use of community health workers in tracking and tracing people living with HIV.
A greater effort on combination prevention, using all currently available prevention methods as well as Cab-LA, which is an antiretroviral HIV prevention injection that provides two months of protection per shot.
These are well known interventions and if health workers and communities are committed to their urgent and full implementation, it is possible to achieve further reductions in new HIV infections, as well as further reductions in death. However, as most deaths in people living with HIV are due to TB, a greater focus should be placed on testing people living with HIV for TB – given the estimated 59% co-infection rates; and ensuring that they are successfully treated and initiating those that test negative for TB, on TB preventive therapy.
How do the Minister’s prescriptions align with the recently completed HIV investment case?
As recently reported in Spotlight, the only HIV intervention found to be cost saving for the health system in South Africa was condoms. However, the recent HSRC survey found that reported condom use at last sexual encounter declined in all age categories. The 2017 survey found that 68% of males aged 15-24 years reported condom use, compared to 50.6% in the latest report. Similarly, 53.4% of males aged 25-49 years reported condom use in 2017 compared to 44% in 2023.
Whilst the Minister noted in his speech at the South African AIDS conference the availability of Cab-LA for HIV prevention, the investment case found that at the current price, this was not a good investment and unaffordable! The investment case outputs suggest that it was most cost effective to increase HIV self-testing, focusing on improving linkage to treatment, as well as increasing the rate of testing infants for HIV at 10 weeks after birth. It is therefore important to prioritise HIV interventions, as noted in the investment case, given that the National Treasury has reduced the HIV conditional grant by R1 billion and that the National Strategic Plan for 2023-2028 is not fully funded!
In UNAIDS’s path to ending AIDS, the organisation suggests what countries can do to intervene. These include: political commitment to ending AIDS, respecting human rights, engaging affected communities, removing criminalising policies and laws, addressing gender inequities, stigma and discrimination, as well as a focused approach to prevention. Some of the barriers to ending AIDS are listed as: inadequate prevention programmes, large treatment gaps, and lack of sufficient funding.
In summary, to respond to the call to end AIDS by 2030:
Firstly, it is critical to agree on its definition.
Secondly, it is important to have accurate data, including at sub-national level given that national averages hide variability by province and district. District level data by sex, age and by key populations will allow a more targeted approach to reaching those that the health system typically does not reach.
While South Africa largely funds much of its HIV response – despite the reduction noted above, the possibility of reduced external funding – through PEPFAR (a US government’s effort to address HIV globally) and The Global Fund (an international financing and partnership organisation to fight AIDS, TB and Malaria) in the future, requires the country to move to a more efficient HIV response, with more precise targeting and with greater levels of accountability. For this more granular and real time data will be required.
*Dr Pillay is extraordinary professor at the Department of Global Health, Stellenbosch University and director for HIV and TB delivery at the Bill and Melinda Gates Foundation.
Note: Spotlight receives funding from the Gates Foundation, but is editorially independent and a member of the South African Press Council. The views expressed in this opinion piece are not necessarily shared by Spotlight.
In social media posts on the community network Reddit, users reported reduced cravings for alcohol when taking drugs intended to treat Type 2 diabetes and obesity. Across a number of threads – with titles such as “Did scientists accidentally invent an anti-addiction drug?” and “I don’t know if this is a side effect but … Mounjaro makes me drink less!!!!!” – users reported a changing relationship with beer, wine, and liquor.
An analysis of those posts, together with a remote study of individuals with obesity who reported using semaglutide and tirzepatide, found that the drugs decreased cravings and reduced alcohol consumption, according to a study by Virginia Tech researchers published inScientific Reports.
“These findings add to a growing literature that these medications may curb dangerous drinking habits,” said Warren Bickel, Virginia Tech Carilion Behavioral Health Research Professor at the Fralin Biomedical Research Institute at VTC and corresponding author.
Combing Reddit for users’ experiences
Scientists with the Fralin Biomedical Research Institute’s Addiction Recovery Research Center combined two different studies to build on existing research, including studies that showed the drugs were effective in reducing alcohol consumption in animal models.
The first was an analysis of more than 68 000 Reddit posts from 2009-23 that included terms linked to GLP-1 approved medications.
Semaglutide is a GLP-1 agonist, a class of drugs that reduce blood sugar and energy intake by mimicking the actions of hormones released after eating.
Among the keywords included in the search were Mounjaro, Wegovy, Ozempic, and Trulicity.
After cleaning the resulting data – such as eliminating comments with fewer than 100 characters – the set was narrowed to 33 609 posts from 14 595 unique users.
The study was unique in using Reddit to analyse the reported experience of thousands of users.
On examining alcohol-related discussions, researchers found that 962 individuals made 1580 alcohol-related posts.
Of those, 71.7% addressed reduced cravings, reduced usage, and other negative effects due to drinking.
In a second study, 153 participants who self-reported having obesity were recruited from various social media platforms.
Roughly a third of these participants represented the control group, a third were taking either a semaglutide injection or tablet, and a third were using tirzepatide.
Participants on semaglutide or tirzepatide reported drinking significantly fewer drinks, on average, than those in the control group who were not on any medication for diabetes or weight loss.
In addition, researchers found that both the average number of drinks and the odds of binge drinking were found to be significantly lower.
Results also found that the stimulative and sedative effects of alcohol intoxication are reduced when taking these medications.
“Participants reported drinking less, experienced fewer effects of alcohol when they did drink it, and decreased odds of binge drinking,” said Alexandra DiFeliceantonio, assistant professor at Fralin Biomedical Research Institute and one of the study’s co-authors.
Researchers believe theirs is the first published report following tirezepatide, sold under the brand name Mounjaro, which was approved in 2022 and is used for treatment of Type 2 diabetes and weight loss.
Why this matters
Case studies and reports in the popular press hint at the drugs’ unexpected side effect of reducing addictive behaviors, including the desire to consume alcohol.
The US Food and Drug Administration has approved only three medications to treat alcohol use disorder: disulfiram, naltrexone, and acamprosate.
They have shown only modest success, have poor compliance, and are underprescribed.
The authors suggest further randomized controlled trials to explore the therapeutic potential of GLP-1 agonists and GIP/GLP-1 combination drugs to treat alcohol use disorder, which affects 5.9% of individuals in the United States ages 12 and older.
In addition, the participants identified as mostly white and female, and further studies in more diverse populations are needed to examine sex and race differences.
“Although evidence supporting the use of these medications for alcohol use disorder is growing, the field still needs to learn considerably more about them, particularly in identifying the underlying mechanisms. We plan to contribute to that effort,” Bickel said.
The drugs are a promising development in the study of alcohol use disorder. Data from the National Survey on Drug Use and Health indicate 15.7 million people in the United States meet the criteria for the chronic, relapsing brain disorder that is a significant contributor to global mortality yet remains one of the most undertreated conditions, Bickel said.
Colourised electron micrograph image of a macrophage. Credit: NIH
Scientists have created a new treatment for traumatic brain injury (TBI). The new approach leverages macrophages, which can increase or decrease inflammation in response to infection and injury. The team attached “backpacks” containing anti-inflammatory molecules directly to the macrophages. These molecules kept the cells in an anti-inflammatory state when they arrived at the injury site in the brain, enabling them to reduce local inflammation and mitigate the damage caused. The research is reported in PNAS Nexus.
“Every year, millions of people suffer from a TBI, but there is currently no treatment beyond managing symptoms. We have applied our cellular backpack technology – which we previously used to improve macrophages’ inflammatory response to cancerous tumours – to deliver localised anti-inflammatory treatment in the brain, which helps mitigate the cascade of runaway inflammation that causes tissue damage and death in a human-relevant model,” said senior author Samir Mitragotri, PhD, in whose lab the research was performed.
Stopping a runaway inflammation train
There is currently no treatment for the damage caused to brain tissue during a traumatic brain injury (TBI), beyond managing a patient’s symptoms. One of the main drivers of TBI-caused damage is a runaway inflammatory cascade in the brain.
As cells die from the impact, they release a cocktail of pro-inflammatory cytokine molecules that attract immune cells to clean up the damage. But the same cytokine molecules can also disrupt the blood-brain barrier, which causes blood to leak into the brain. Blood accumulation in the brain causes swelling, impaired oxygen delivery, and increased inflammation, and creates a vicious cycle of bleeding and damage that drives even more cell death.
The Mitragotri lab saw an opportunity in this problem.
“It’s generally believed anti-inflammatory therapies can be effective for treating TBI, but so far, none of them have proven effective clinically. Our previous work with macrophages has shown us that we can use our backpack technology to effectively steer their behaviour when they arrive at the injury site. Since these cells are already active players in the body’s natural immune response to a TBI, we had a hunch we could augment that pre-existing biology to reduce the initial damage,” said co-first author Rick Liao, Ph.D., a Postdoctoral Fellow at the Wyss Institute and SEAS.
“Body, heal thyself”…with backpacks
Macrophages are very malleable cells and can “switch” between pro-inflammatory and anti-inflammatory states. While the team’s previous work in cancer had been focused on keeping macrophages in a pro-inflammatory state when they arrive at the inflammation-reducing microenvironment of a tumour, this new project would be trying to do the opposite: keep the macrophages “calm” in the inflammation-riddled setting of a brain injury.
To do so, they used a disc-shaped “backpack” they had previously designed to treat multiple sclerosis that contained layers of two anti-inflammatory molecules: dexamethasone, a steroid, and interleukin-4, a cytokine that encourages macrophages to adopt an anti-inflammatory state. They then incubated these microparticles with both human and pig macrophages in vitro and saw that the backpacks stably stuck to the cells without causing any negative effect. They also observed that application of their backpacks decreased the expression of pro-inflammatory biomarkers and increased the expression of anti-inflammatory biomarkers, retaining the pig macrophages in a healing state.
But to prove that this shift would work in the body, they had to test the backpack-bearing macrophages in vivo. They chose pigs as their model organism because their brains’ structures and responses to injury more closely mimic those of humans than mice.
“Probably our biggest challenge in this project was scaling up production to match what we needed to run the experiments. Our previous studies were done in rodents, which required about two million macrophages and four million backpacks administered per subject. For the porcine study, we needed 100 million macrophages and 200 million backpacks per subject – on the scale of what would be administered in humans – and lots of helping hands,” said co-first author Neha Kapate, PhD, a Postdoctoral Fellow at the Wyss Institute and SEAS.
Once they had generated enough backpack-wearing porcine macrophages, they infused them into the pigs’ bloodstreams four hours after a TBI. Seven days later, they analysed the animals’ brains. Pigs that had received the macrophage treatment showed a high concentration of the cells in the area immediately surrounding the injury site, their lesions were 56% smaller, and there was significantly less haemorrhaging than in untreated animals.
Local immune cells also displayed a lower amount of a pro-inflammatory activation marker called CD80, indicating that the macrophages had accomplished their damage control by reducing inflammation in the brain. Corroborating that data, the levels of two soluble biomarkers for inflammation in the blood and cerebrospinal fluid were lower in treated animals than in untreated animals. The macrophage treatment also did not cause any negative effects.
The team plans to conduct future studies that focus on elucidating exactly how their anti-inflammatory macrophage therapy affects the blood-brain barrier’s integrity to prevent bleeding, which could also hold promise for treating other conditions like hemorrhagic strokes.
“Macrophages’ susceptibility to their local environment has historically prevented scientists from taking full advantage of their immune-modulating capabilities. This impressive study describes a truly novel and potentially powerful macrophage-based therapy for treating the inflammation that is the root cause of so many human afflictions in an effective and non-invasive way that works with biology rather than against it,” said Wyss Founding Director Donald Ingber, MD, PhD.
Diffuse gliomas are malignant brain tumours that cannot be optimally examined by means of conventional MRI imaging. So-called amino acid PET (positron emission tomography) scans are better able to image the activity and spread of gliomas. An international team of researchers from the RANO Working Group have drawn up the first ever international criteria for the standardised imaging of gliomas using amino acid PET. It has published its results in the journal The Lancet Oncology.
PET uses a radioactive tracer to measure metabolic processes in the body. Amino acid PET is used in the diagnosis of diffuse gliomas, with tracers that work on a protein basis (amino acids) and accumulate in brain tumours.
The Response Assessment in Neuro-Oncology (RANO) Working Group is an international, multidisciplinary consortium founded to develop standardised new response criteria for clinical studies relating to brain tumours.
Under the joint leadership of nuclear physician Nathalie Albert from LMU and oncologist Professor Matthias Preusser from the Medical University of Vienna, the RANO group has developed new criteria for assessing the success of therapies for diffuse gliomas.
Nathalie Albert explains: “PET imaging with radioactively labelled amino acids has proven extremely valuable in neuro-oncology and permits reliable representation of the activity and extension of gliomas. Although amino acid PET has been used for years, it had not been evaluated in a structured manner before now. In contrast to MRI-based diagnostics, there have been no criteria for interpreting these PET images.” According to the researchers, the new criteria allow PET to be used in clinical studies and everyday clinical practice and create a foundation for future research and the comparison of treatments for improved therapies.
New criteria for PET examinations of brain tumours
Diffuse gliomas are malignant brain tumorus that cannot be optimally examined by means of conventional MRI imaging. So-called amino acid PET scans are better able to image the activity and spread of gliomas.
These malignant brain tumours develop out of glial cells and are generally aggressive and difficult to treat.
The RANO group has developed criteria that permit evaluation of the success of treatment using PET. Called PET RANO 1.0, these PET-based criteria open up new possibilities for the standardised assessment of diffuse gliomas.
What if in the years prior to the COVID pandemic, scientists had developed a universal coronavirus vaccine, one that targets parts common to coronaviruses, offering some protection against all strains? Would it have been of help during the pandemic?
A new study suggests if such a vaccine were available at the start of the pandemic, it could have saved millions of lives, prevented suffering, and saved billions of dollars in direct medical and other costs until the strain-specific (ie, SARS-CoV-2) vaccine went through the entire development, testing, and emergency use authorisation process that lasted 10 months.
In this study, published in The Lancet’s eClinicalMedicine, researchers show that having a universal vaccine at the start of the pandemic would have had substantial health and economic benefits under almost all scenarios tested.
In order to determine the value of investing in developing and stockpiling a universal coronavirus vaccine, the team developed a computational model that simulated the entire US population, the introduction and spread of a novel coronavirus like SARS-CoV-2 in 2020 and the resulting health (eg, infections, hospitalisations) and economic (eg, direct medical costs, productivity losses) outcomes.
The experiments simulated what would happen if a universal coronavirus vaccine was available at the start of the COVID pandemic.
Vaccinating with a universal coronavirus vaccine as a standalone intervention (e.g., no face mask use or social distancing) was cost-saving even when its efficacy was as low as 10% and only 10% of the U.S. population received the vaccine.
For example, when a universal coronavirus vaccine has 10% efficacy, vaccinating a quarter of the U.S. population within two months of the start of the pandemic averts an average of 14.6 million infections and saves over $27 billion in direct medical costs.
Such low vaccine coverage at the start of the pandemic could occur if a vaccine were only made available to certain high-risk subpopulations (eg, 65 years and older, the immunocompromised, frontline workers), similar to the approach when mRNA vaccines became available in December 2020.
“COVID-19 was the third major and serious coronavirus epidemic or pandemic following SARS in 2002 and MERS in 2012, thus, we should anticipate a fourth coronavirus outbreak within the next decade or so,” says Peter J. Hotez, MD, PhD, dean of Baylor’s National School of Tropical Medicine and co-director of the Texas Children’s Hospital Center for Vaccine Development.
“A universal vaccine is cost-effective and cost-saving and a priority for advancement.”
A universal coronavirus vaccine was also shown to be highly cost-effective even if a more specific and more efficacious vaccine came to market.
For example, the study shows if it takes four months or longer for a strain-specific vaccine to reach the market, using a universal vaccine was still cost cost-saving.
In a scenario where a strain-specific vaccine has 90% efficacy but is unavailable for two months after the start of the pandemic, the results from the model show that vaccinating only 10% of the population with a universal vaccine that has 10% efficacy at the start of the pandemic can save over $2 billion in societal costs (eg, direct medical costs and productivity losses from absenteeism). Given the time required to develop a strain-specific vaccine during a pandemic to match circulating strains of the virus, this highlights the importance of having a universal vaccine readily available as a stopgap.
“Our study shows the importance of giving as many people as possible in a population at least some degree of immune protection as soon as possible,” explains Bruce Y. Lee, MD, MBA, executive director of PHICOR and professor at CUNY SPH.
“Having a universal vaccine developed, stockpiled, and ready to go in the event of a pandemic could be a game-changer even if a more specific vaccine could be developed three to four months later.”
Generally, results from the model found that a universal vaccine would end up saving money if the cost to get a person vaccinated (eg, cost of the vaccine itself, distribution, administration, storage, research, and development) is as high as $10 390 from a societal perspective.
A new Vanderbilt University study published in the journal Diabetes demonstrates that a glucagon-like peptide-1 receptor (GLP-1R) agonist, a member of a class of medication used to treat Type 2 diabetes and obesity, can lead to a rapid improvement in insulin sensitivity.
Insulin sensitivity is how responsive cells are to insulin; reduced insulin sensitivity or insulin resistance is a feature of Type 2 diabetes, so improving it can reduce the risk of developing the disease or improve its treatment.
GLP-1R agonists are medications that influence metabolism, such as decreasing blood sugar levels by promoting insulin secretion. Dipeptidyl peptidase 4 (DPP-4) inhibitors block the degradation of the body’s own endogenous GLP-1, as well as other peptide hormones such as glucose-dependent insulinotropic peptide (GIP).
“We know that GLP-1R agonists promote weight loss, but we were surprised to find that the GLP-1R agonist liraglutide also has rapid effects on insulin sensitivity, independent from weight loss,” said Mona Mashayekhi MD, PhD, assistant professor of Medicine in the Division of Diabetes, Endocrinology and Metabolism.
“This effect requires activation of the GLP-1 receptor, but increasing the body’s own endogenous GLP-1 through the use of the DPP4 inhibitor sitagliptin does not achieve similar effects.”
“Our research suggests that liraglutide, and presumably other GLP-1R agonists, are having important metabolic effects in a way that’s different from increasing endogenous GLP-1 levels, even though they’re using the same receptor. Future research will focus on potential mechanisms of how GLP-1R agonists are improving insulin sensitivity independent of weight loss.”
Eighty-eight individuals with obesity and pre-diabetes were randomized for 14 weeks to receive the GLP-1R agonist liraglutide, the dipeptidyl peptidase 4 (DPP-4) inhibitor sitagliptin, or weight loss without drug using a low-calorie diet.
To further investigate the GLP-1R-dependent effects of the treatments, the GLP-1R antagonist exendin and a placebo were given in a two-by-two crossover study during mixed meal tests.
Crossover studies allow the response of a subject to treatment A to be compared with the same subject’s response to treatment B.
Liraglutide was shown to rapidly improve insulin sensitivity as well as decrease blood glucose within two weeks of beginning treatment and before any weight loss.
“GLP-1R agonists are an exciting class of medications, given their strong glucose-lowering effects combined with tremendous weight-loss benefits, and they have transformed how we manage diabetes and obesity in the clinic,” Mashayekhi said.
“Since the number of medications in this class is rapidly expanding, a deeper understanding of the mechanisms of benefit is crucial so we can design the right drugs for the desired effects in the right patients.”
The investigators’ prior research demonstrated that liraglutide, but not sitagliptin or diet, improves measures of heart disease and inflammation.
This matches the clinical findings of reduced cardiovascular disease with GLP-1R agonist treatment.
Future studies will continue to explore both receptor- and weight loss-dependent effects of GLP-1R agonists in humans.
A breakthrough study sets the foundation of a ground-breaking treatment regimen for treating ventricular arrhythmia. The study, published in Nature Communications, demonstrates the design and feasibility of a new hydrogel-based pacing modality.
The urgent need for an effective therapeutic regimen for ventricular arrhythmia inspired a team led by Dr. Mehdi Razavi at The Texas Heart Institute (THI), to collaborate The University of Texas at Austin (UT Austin) Cockrell School of Engineering led by Dr. Elizabeth Cosgriff-Hernandez, to co-develop an innovative strategy that addresses the pathophysiology of re-entrant arrhythmia.
Ventricular arrhythmia, which occurs in the lower chambers of the heart or ventricles, is the leading cause of sudden cardiac death in the United States.
When heart rhythm abnormality occurs in a self-sustained manner, it is called re-entrant arrhythmia, which is usually fatal.
“Re-entry occurs mainly from delayed conduction in scarred heart tissues, usually after coronary artery occlusion during a heart attack, which can be corrected by enabling pacing in these regions,” said Dr. Razavi, a practicing cardiologist and cardiac electrophysiologist.
“These hydrogels then can access the scarred tissue, thereby enabling direct pacing of the otherwise inaccessible regions of the heart.”
Given hydrogels’ biostability, biocompatibility, tunable properties, and the ease of incorporating electrical conductivity, the scientists are exploring them as potential electrodes that can be easily delivered inside coronary veins.
A clinical advantage of the unique system is that ischemia can be avoided by delivering the hydrogel using the veins.
The researchers successfully deployed the innovative hydrogel technology through minimally invasive catheter delivery in a pig model.
“The hydrogels have significant conductive properties that enable simultaneous pacing from multiple sites along the length of the hydrogel and create a conduction highway similar to those in Purkinje fibers,” according to Dr. Cosgriff-Hernandez.
Today, arrhythmia is treatable with medicines and procedures that control the irregular rhythms.
The current anti-arrhythmic drugs on the market are not always effective; although the drugs slow the conduction velocity, they facilitate re-entry arrhythmia.
Moreover, these drugs can be toxic and can lead to the destruction of tissues near the diseased regions of the heart.
Even with the widely used interventional ablation therapies, arrhythmia recurs in a significant proportion of patients. None of these procedures address the mechanism of re-entry.
Cardiac defibrillators implanted to compensate for the shortfalls in the current therapy options are painful when delivering electric shocks to restore heart rhythm and can severely deteriorate the patient’s quality of life.
If left untreated, arrhythmia can damage the heart, brain, or other organs, leading to stroke or cardiac arrest, during which the heart suddenly and unexpectedly stops beating.
“When injected into target vessels, the conductive hydrogel conforms to the patient’s vessel morphology. Adding a traditional pacemaker to this gel allows for pacing that resembles the native conduction in the heart — effectively mimicking the native electrical rhythm of the heart — and extinguishes the cause for arrhythmia, providing painless defibrillation,” added Dr. Cosgriff-Hernandez.
The work demonstrates for the first time the ability to confer direct electrical stimulation of the native and scarred mid-myocardium through injectable hydrogel electrodes as a pacing modality.
With minimally invasive catheter delivery and standard pacemaker technologies, this study indicates the feasibility of a novel pacing modality that resembles native conduction, potentially eliminating lethal re-entrant arrhythmia and providing painless defibrillation, which can be successfully adopted in a clinical workflow.
The scientific advance is significant considering pain management is highly relevant to overall wellness for patients with heart, lung, and blood diseases.
Such innovation in painless defibrillation and preventing arrhythmia could revolutionize cardiac rhythm management.
Including patients as partners for making decisions about their medical treatments is an important aspect of patient-centred care. A new study from England examined choices that patients with breast cancer make when considering where to have surgery for their condition and assessed how policies that offer such choices might affect inequalities in the health care system. The findings are published in CANCER.
For the study, investigators analysed data from the National Health Service (NHS), the publicly funded health care system in the United Kingdom that offers patients with cancer the opportunity to select any hospital providing cancer treatment, and identified all women diagnosed with breast cancer from 2016 to 2018 who had breast-conserving surgery or a mastectomy.
Records showed that 22 622 of 69,153 patients undergoing breast-conserving surgery (32.7%) and 7179 of 23 536 patients undergoing mastectomy (30.5%) bypassed their nearest hospital to receive surgery farther away from home. Women who were younger, without additional medical conditions, of white ethnic background, or lived in rural areas were more likely to travel to more distant hospitals.
Patients were more likely to be treated at hospitals classified as specialist breast reconstruction centres even if they personally were not undergoing breast reconstruction after surgery. Patients who had a mastectomy and immediate breast reconstruction were more likely to travel to hospitals that had surgeons with a strong media reputation for breast cancer surgery, and patients were less likely to travel to hospitals with shorter surgical waiting times. Patients did not seem to make choices based on hospitals’ research activity, quality rating, breast re-operation rates (to remove additional cancer cells that were missed), or status as a multidisciplinary cancer centre (where patients can receive all their care at one location).
The investigators noted that this separation – elderly patients, those with comorbidities, and those from ethnic minority backgrounds receiving care at their local hospital, while others travel to other hospitals and specialist centres – could further drive inequalities in access to quality care.
“As marginalized groups already face barriers to high-quality care, it is important for policy makers to consider measures that mitigate against the risks of increasing inequalities in access and outcomes, by for example providing free transport, accommodation, or even protection against loss of income,” said co-author Lu Han, PhD, of the London School of Hygiene & Tropical Medicine. “Moreover, patients prefer to access information on the quality of breast cancer care of the hospitals in their region at the start of the management pathway when a diagnosis is sought. Such information should be easy to understand and presented in a format that can support the trade-offs that patients have to make.”
An international research team has found a number of substances with a dual effect against tuberculosis (TB): They make the bacteria causing the disease less pathogenic for human immune cells whilst boosting the activity of conventional antibiotics. They published their findings in the journal Cell Chemical Biology.
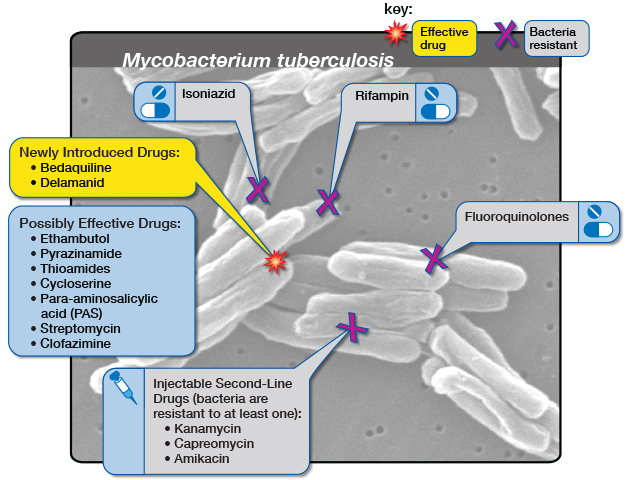
Infectious disease specialist Dr Jan Rybniker and colleagues have identified new, antibiotic molecules that target Mycobacterium tuberculosis and make it less pathogenic for humans.
Diagram by the United States-based National Institute of Allergy and Infectious Diseases showing the medicine options for drug-resistant tuberculosis. (Via Flickr, CC BY 2.0 Deed)
In addition, some of the discovered substances may allow for a renewed treatment of tuberculosis with available medications – including strains of the bacterium that have already developed drug resistance.
Although treatable with antibiotics, it still ranks among the infectious diseases that claim the most lives worldwide: According to the World Health Organization (WHO), only COVID was deadlier than TB in 2022. The disease also caused almost twice as many deaths as HIV/AIDS. More than 10 million people continue to contract TB every year, mainly due to insufficient access to medical treatment in many countries.
Limited targets
Multidrug-resistant tuberculosis is emerging especially in eastern Europe and Asia. That is of particular concern to researchers because like all bacteria that infect humans, Mycobacterium tuberculosis possesses only a limited number of targets for conventional antibiotics.
That makes it increasingly difficult to discover new antibiotic substances in research laboratories.
Working together with colleagues from the Institute Pasteur in Lille, France, and the German Center for Infection Research (DZIF), the researchers at University Hospital Cologne have now identified an alternative treatment strategy for the bacterium.
The team utilized host-cell-based high-throughput methods to test the ability of molecules to stem the multiplication of bacteria in human immune cells: From a total of 10,000 molecules, this procedure allowed them to isolate a handful whose properties they scrutinized more closely in the course of the study.
Two-pronged attack
Ultimately, the researchers identified virulence blockers that utilise target structures that are fundamentally distinct from those targeted by classical antibiotics.
“These molecules probably lead to significantly less selective pressure on the bacterium, and thus to less resistance,” said Jan Rybniker, who heads the Translational Research Unit for Infectious Diseases at the Center for Molecular Medicine Cologne (CMMC) and initiated the study.
In deciphering the exact mechanism of action, the researchers also discovered that some of the newly identified chemical substances are dual-active molecules.
Thus, they not only attack the pathogen’s virulence factors, but also enhance the activity of monooxygenases — enzymes required for the activation of the conventional antibiotic ethionamide.
Ethionamide is a drug that has been used for many decades to treat TB. It is a so-called prodrug, a substance that needs to be enzymatically activated in the bacterium to kill it. Therefore, the discovered molecules act as prodrug boosters, providing another alternative approach to the development of conventional antibiotics.
In cooperation with the research team led by Professor Alain Baulard at Lille, the precise molecular mechanism of this booster effect was deciphered.
Thus, in combination with these new active substances, drugs that are already in use against tuberculosis might continue to be employed effectively in the future.
The discovery offers several attractive starting points for the development of novel and urgently needed agents against tuberculosis.
“Moreover, our work is an interesting example of the diversity of pharmacologically active substances. The activity spectrum of these molecules can be modified by the smallest chemical modifications,” Rybniker added.
However, according to the scientists it is still a long way to the application of the findings in humans, requiring numerous adjustments of the substances in the laboratory.