
The Cold Virus ‘Hides’ and Multiplies in the Tonsils and Adenoids, Even in People Without Symptoms
2026-04-15
A study conducted at the University of São Paulo shows that the pathogen can persist in these tissues for long periods, be transmitted unexpectedly, and trigger new outbreaks of the disease.
By Karina Toledo | Agência FAPESP – A study conducted at the University of São Paulo (USP) in Brazil reveals that tissues such as the tonsils and adenoids can serve as hiding places for the rhinovirus, which causes the common cold and is responsible for most respiratory infections worldwide.
Using samples from 293 children who underwent surgery to remove these tissues, the study showed that the pathogen can infect immune cells known as lymphocytes and remain there for long periods without causing symptoms. This allows the virus to potentially be transmitted to others without warning.
“The virus has a ‘date’ with the child population. Every year, about two or three weeks after school starts in temperate regions, there’s a rhinovirus outbreak. And children pass it on to their parents and grandparents. We’ve always wondered: What does the start of school have to do with it? Well, children gather in closed spaces, and some of them with the virus in their throats can spark an outbreak at school, even if they’re asymptomatic,” comments rhinovirologist Eurico de Arruda Neto, a professor at the Ribeirão Preto School of Medicine (FMRP-USP) and coordinator of the research, supported by FAPESP (projects 13/06380‐0, 13/16349‐2 and 17/25654‐4).
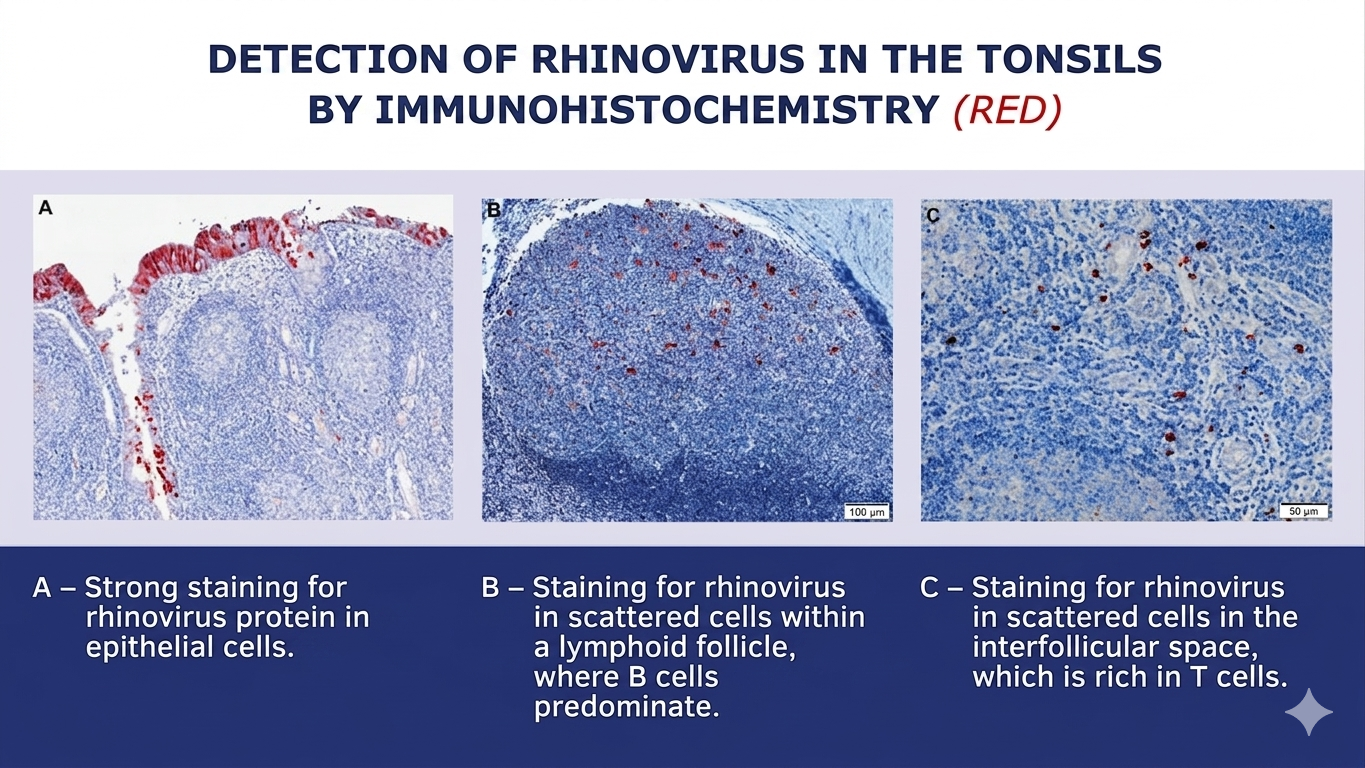
As the researcher explains, it was already known that the rhinovirus infects the epithelium (the outermost layer of the mucosa) of the nose and throat, hijacks the cellular machinery to multiply, and causes the host cell to rupture once this process is complete, releasing progeny capable of generating new infections. For this reason, scientists consider it a lytic virus, one that causes cell lysis, or rupture. This rapid and destructive cycle quickly draws the attention of the immune system, which, in most cases, eliminates the virus from the body within about five to seven days.
The major finding of the study was that the rhinovirus can reach the deeper layers of tonsil and adenoid tissues in addition to the epithelium. There, it can infect B lymphocytes, which produce antibodies, and CD4 T lymphocytes, which conduct the local immune response. These cells have a long lifespan and store the “memory” of the immune system. Rather than killing them, the rhinovirus remains inside these cells for extended periods, in a state of persistence similar to that seen with herpes viruses, HPV, and cytomegalovirus.
“The samples we analyzed are from children who underwent surgery due to snoring, sleep apnea, or recurrent infections related to tonsillar and adenoid hypertrophy. At the time of surgery, they were necessarily asymptomatic. Nevertheless, we detected the rhinovirus in a large number of participants,” says Arruda.
In addition to the tonsils and adenoids, the children’s nasal secretions were analyzed as well. According to data published in the Journal of Medical Virology, the virus was present in at least one of the three sites (tonsil, adenoid, or secretion) in 46% of the volunteers. Viral proteins and other signs that the rhinovirus was replicating – and therefore capable of infecting another person – were also observed in these tissues.
The research was conducted in collaboration with Ronaldo Martins, a virologist from the Ribeirão Preto School of Pharmaceutical Sciences (FCFRP-USP), as well as professors Wilma Anselmo-Lima, Edwin Tamashiro, and Fabiana Valera from the FMRP-USP.
(image: press release)
Virus garden
In previous studies, Arruda’s team detected adenovirus (another cause of the common cold), influenza A (flu), and SARS-CoV-2 (COVID-19) in samples of tonsils and adenoids from children who had undergone surgery. The latter two are known to cause longer-lasting infections in some patients. In the case of the rhinovirus, however, this came as a surprise.
“I get the impression that no matter what common virus we look for, we’ll find it. And not just in the tonsils and adenoids, but in other lymphoid tissues throughout the body, such as lymph nodes. We already have some preliminary evidence that lymphoid tissues are a sort of ‘garden’ for viruses. And our hypothesis is that this is a good thing. It acts as a booster for immune memory, meaning antibodies continue to be produced even long after initial exposure,” says Arruda.
However, in the case of people with asthma, this can be problematic. One hypothesis raised by the authors of the article is that infectious viruses in tonsil CD4 T lymphocytes may release inflammatory substances that act on the lungs and cause asthma attacks. It is already known that colds and the flu are among the most common causes of asthma attacks, especially in young children.
Additionally, a previous study by the group detected respiratory viruses in normal adenoids (without hypertrophy), which are located next to the Eustachian tube. This may explain why some children suffer from recurrent otitis media.
“This virus can pass from the adenoids to the middle ear and cause inflammation there. The child won’t sneeze or cough, but the ear will become inflamed, closing the narrow Eustachian tube and leading to a buildup of fluid in which the local bacterial flora begins to proliferate,” the researcher explains.
Clinical implications
Based on these findings, Arruda believes that pediatricians should be mindful of the possibility of diagnostic confusion regarding the causes of childhood illnesses.
“For example, a child with hypertrophic tonsils arrives at the emergency room with a respiratory infection and bronchiolitis symptoms caused by respiratory syncytial virus, but the throat swab test detects rhinovirus from a previous infection. In other words, tests performed on secretions may not always reflect what’s actually happening in the lungs,” says the researcher. “We have evidence that this viral persistence can also occur in people with normal-sized tonsils and adenoids.”
Another hypothesis to be investigated, Arruda says, is whether viruses that persist in lymphoid tissues can cause problems for immunosuppressed patients. “Patients who undergo bone marrow transplants, for example, frequently develop lung infections and bronchiolitis. Doctors, nurses, and medical students are usually blamed for bringing the virus into the high-risk ward. But could it be that the virus was already present in the patient’s tonsils or adenoids and has now been reactivated due to low immunity? It doesn’t have to be transmission from outside to inside. That’s what we’ve started to investigate in mice,” he explains.
The article “Rhinovirus infects B and CD4 T lymphocytes in hypertrophic tonsils in children” can be read at pmc.ncbi.nlm.nih.gov/articles/PMC12831225/.
Republished from Agência FAPESP under a Creative Commons licence.
Read the original article.








{kind=link}