
Severe Infections May Raise Dementia Risk, Study Finds
Finnish registry study finds that infections like cystitis and bacterial disease are linked to higher dementia risk independently of other coexisting conditions
Severe infections increase the risk of dementia independently of other coexisting illnesses, according to a new study published March 24th in the open-access journal PLOS Medicine by Pyry Sipilä of the University of Helsinki, Finland, and colleagues.
Severe infections have been linked to an increased risk of dementia. However, it has been unclear whether this association is explained by other coexisting, non-infectious diseases that predispose people to both infections and dementia.
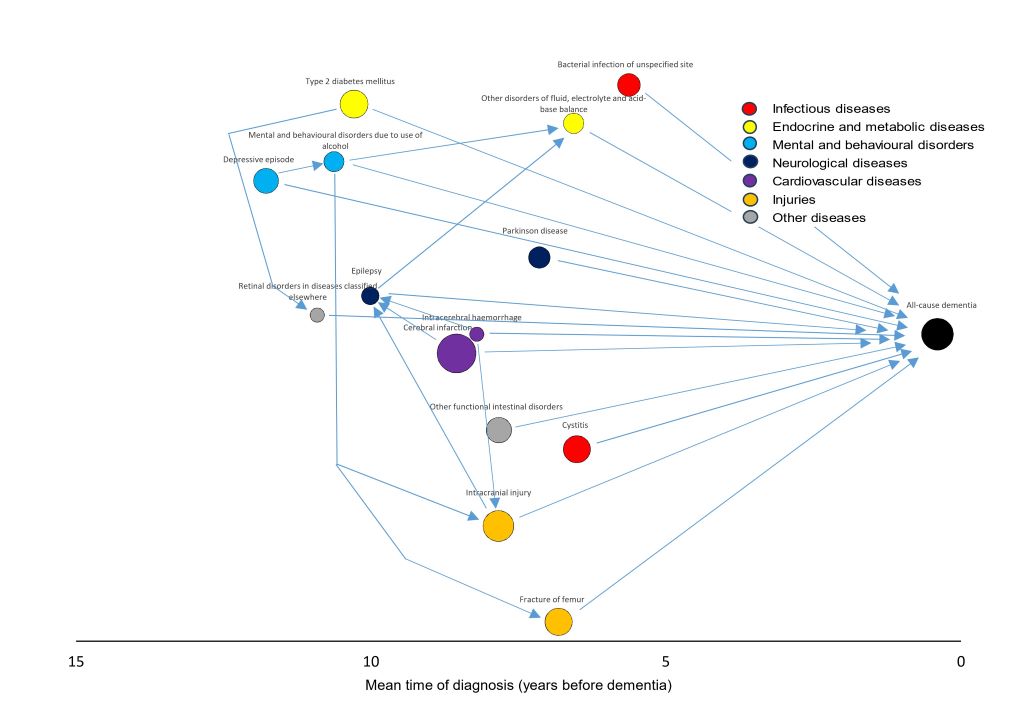
In the new study, researchers used nationwide Finnish health registry data covering more than 62 000 individuals aged 65 or older who were diagnosed with late-onset dementia between 2017 and 2020, along with more than 312 000 matched dementia-free controls. Taking a broad approach, they examined all hospital-treated diseases recorded during the previous twenty years, identifying 29 diseases that were robustly associated with increased dementia risk. Nearly half (47%) of dementia cases had at least one of the 29 identified diseases before their diagnosis.
Of those diseases, two were infections: cystitis (a urinary tract infection) and bacterial infection of an unspecified site. Among the non-infectious diseases, the strongest associations with dementia were seen for mental disorders due to brain damage or physical disease, Parkinson’s disease, and alcohol-related mental and behavioural disorders.
When the researchers then adjusted for all 27 non-infectious dementia-related diseases identified, the association between both infections and dementia remained largely intact. Less than one-seventh of the excess dementia risk among individuals with hospital-treated cystitis or bacterial infections was attributable to pre-existing conditions. The link between infections and dementia was even stronger for early-onset dementia (diagnosed before age 65), where five types of infection – including pneumonia and dental caries – were associated with elevated risk.
The study was limited by the lack of baseline cognitive assessments and clinical examination data before dementia diagnoses, as well as a lack of data on infection treatments.
“Overall, our findings support the possibility that severe infections increase dementia risk; however, intervention studies are required to establish whether preventing or effectively treating infections yields benefits for dementia prevention,” the authors say.
The authors add, “We found 27 diverse severe, hospital-treated diseases that were robustly associated with an increased risk of dementia. Two of these diseases were infections, namely urinary tract infections and unspecified bacterial infections.”
“In our study, dementia-related infections occurred on average 5 to 6 years before dementia diagnosis. Given that the development of dementia often takes years or even decades, these findings suggest that severe infections might accelerate underlying cognitive decline. However, as these findings were observational, we cannot exclude the possibility that some unmeasured confounding factors might also have affected our findings. Thus, we cannot prove cause and effect.”
“Ideally, intervention trials should examine whether better infection prevention helps reduce dementia occurrence or delay the onset of this disease.”
Provided by PLOS








