Daily doses of peppermint oil have been proved to lower blood pressures for patients with mildly high readings, new research has found.
A team of University of Lancashire academics discovered a daily intake of 100 microlitres of peppermint oil, taken twice a day over 20 days, lowered the systolic blood pressure by an average of 8.5mmHg.
The findings have been published in PLOS One Journal and prove there could be a simple, inexpensive, and well‑tolerated way to help treat people with slightly raised blood pressure.
Lead author Dr Jonnie Sinclair, Reader in Sport and Health Sciences, said: “High blood pressure is one of the biggest causes of heart disease and death worldwide, and it costs a huge amount of money to treat. Although medicines are commonly used to treat it, it’s not always clear how well they work in the long-term, and they can cause unwanted side effects.”
Peppermint oil is low in calories and price so it’s proved to be a very simple and cost-effective solution to potentially treat millions of people around the world.
– Lead author Dr Jonnie Sinclair, Reader in Sport and Health Sciences
Peppermint contains substances like menthol and flavonoids and in the study, 40 18 to 65-years-olds were randomly split into two groups. One group in the pre‑hypertension and stage 1 hypertension phases took a small daily dose of oil and saw the improvement while the other took a peppermint‑flavoured placebo that did not contain the active oil and saw no real change.
Researchers measured the change in systolic blood pressure, but they also looked at body measurements, blood results, diastolic blood pressure (the bottom number in a blood pressure reading), heart rate, mental wellbeing and sleep quality.
Dr Sinclair added: “Our findings were very positive and they have significant clinical implications, especially given arterial hypertension is the most common preventable risk factor for cardiometabolic disease and the greatest single risk factor for global mortality.
“Peppermint oil is low in calories and price so it’s proved to be a very simple and cost-effective solution to potentially treat millions of people around the world.”
Tuberculosis (TB) is not a medical mystery, writes AI Diagnostics CEO, Braden van Breda. It’s a detection failure. And with technology like AI at our disposal, he believes the MedTech industry has the power to step up and fix it.
Tuberculosis bacteria. Credit: CDC
TB remains the deadliest infectious disease in the world, but it’s not killing people indiscriminately, it’s killing people in poor, developing countries.
Data from the World Health Organization makes this very clear. In 2024, most TB cases were concentrated in developing regions, especially South-East Asia, the Western Pacific, and Africa. In South Africa, an estimated 54 000 people died of TB in 2024. That’s a soccer stadium full of people wiped out by TB in a single year. Meanwhile, the Americas accounted for just 3.3% of global cases and Europe 1.9%.
The danger is that we get complacent about these numbers because we’re so used to hearing them. It’s not normal that people’s loved ones are dying from TB by the tens of thousands in some parts of the world, while in others, the incidence is low enough to be almost negligible.
Detection is the crisis
We already know what causes TB. We know how it spreads, how to diagnose it, and how to treat it. South Africa is losing this fight because the tools we currently have don’t catch cases early enough.
Since TB is easiest to treat (and least likely to spread) when it’s found early, the result compounds. Too many people are only diagnosed once they become seriously ill. By then, they’ve already infected others, and the cost and effort of accessing care often becomes a barrier in itself.
The science is there; the failure now lies in access to quality screening. The question we need to ask ourselves is whether we’re serious about bringing healthcare to people instead of forcing people to chase healthcare.
Start designing TB screening around the communities that need it most
Too much of our TB diagnostic infrastructure remains concentrated in too few facilities, and that depends on expensive equipment, medical specialists, and referral pathways.
For many people, especially in rural areas and poorer communities, getting to a hospital means losing a day’s wages, while having to pay for transport they can’t afford. The result is that people wait or don’t go at all. In 2024, only about 184 000 of the estimated 249 000 South Africans who fell ill with TB were diagnosed and started on treatment. That leaves around 65 000 people who were missed altogether.
This is why community-level screening matters so much. We can’t build specialist diagnostic centres next to every rural clinic. Even if we could, we don’t have enough specialists to run them. The answer is to put simpler, portable, and locally workable screening tools into the hands of frontline healthcare workers, especially nurses in primary care settings.
South Africa can’t wait around to be rescued
If the bottleneck is access, then innovation has to begin where access fails. That means building around the healthcare system we have, not the one we wish we had. How do we equip the nurse at the overcrowded community clinic? If we’re serious about combating TB, that’s the question we have to answer.
It’s also why South Africa can’t keep assuming that imported solutions from European or American healthcare systems will automatically fit our realities. We need tools designed for our burden of disease, clinic environments, and constraints. The countries carrying the heaviest burden should also be shaping the next generation of practical, scalable solutions.
The local MedTech sector needs to decide whether it’s serious about that responsibility. It’s one thing to produce impressive technology for conferences and investor decks, but can it be used in a crowded community clinic by a healthcare worker at the end of an 18-hour shift? If the answer is no, it’s not solving the real problem.
When a curable disease is killing tens of thousands of people, we can’t afford to sit around and wait to solve the problem. Thanks to advances in technology, the tools to close the screening gap are no longer beyond our reach. Failing to use them is inexcusable.
Every day, thousands of people worldwide suffer a heart attack, often leading to lasting damage to the heart muscle. New research from the University of Oslo suggests that targeting inflammation in the body helps protect the heart and improve recovery after a heart attack.
“In a small country like Norway alone, we see around 11 000 heart attacks every year,” says postdoctoral fellow Camilla Huse at the Research Institute for Internal Medicine, at University of Oslo and Oslo University Hospital. “Forty heart attacks every day is a lot.”
Fortunately, modern treatments are so effective that most patients survive a heart attack.
Inflammation damages the heart
However, a heart attack triggers a strong inflammatory reaction in the body. While this inflammation is part of the body’s natural response, it also causes damage to the heart muscle during a heart attack.
Such injury can lead to poorer health, a reduced quality of life and fewer working years for those affected. It also increases the risk of developing new heart diseases later in life.
So, how can we protect the heart during a heart attack?
Can anti-inflammatory medication improve heart attack treatment?
For some time, the researchers at the University of Oslo and Oslo University Hospital have been studying a medicine that blocks the effect of a substance that stimulates inflammation, a substance called IL-6. Previously, they have shown that administering this medicine in addition to established treatment for heart attacks has promising results: the patients suffered less damage to their hearts.
“This could be a new way of treating patients,” senior researcher Tuva Børresdatter Dahl says, and continues:
“To move forward with treatment, we need to understand what happens in the body when we block inflammation. Which processes inside the cells are affected by the medicine being tested? Which are not? And how does this relate to damage to the heart and to the improved recovery of the patient?”
How to investigate the effect of the treatment
The researchers conducted a study in which they examined the immune cells of 200 patients with STEMI. STEMI is a type of heart attack where the risk of serious complications is high.
The patients were randomly divided into two groups. Half of them received the anti-inflammatory medication, blocking the IL-6 signal, while the other half received a placebo, i.e. a treatment without any active ingredient.
The researchers then monitored how the treatment affected the immune cells in the blood. They also measured how much of the heart muscle was damaged.
Monocytes at the front line of our immune system
The researchers found that the treatment affects a type of immune cell called monocytes, which play an important role in all forms of inflammation.
“The monocytes are right at the front line of our immune system. They are among the first immune cells to arrive to the heart when a heart attack occurs,” Huse says.
Shortly after a heart attack, a strong inflammatory mobilisation occurs in the body, and monocytes flow to the heart muscle.
“The monocytes help to repair and clean up after a heart attack. But they can often get a little too eager. Thus, they also contribute to worsening the damage to the heart muscle after the heart attack,” she explains.
Reduced inflammation linked to better heart attack recovery
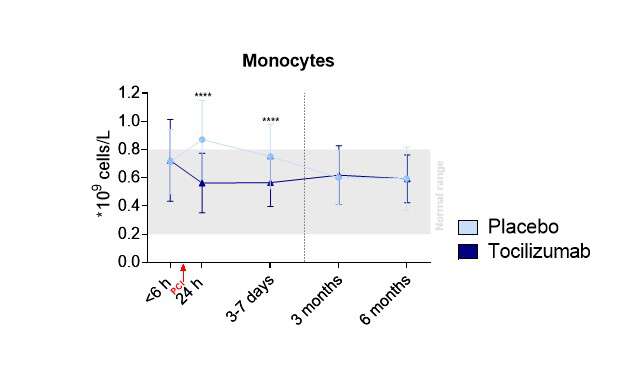
The study showed that the patients who received the anti-inflammatory medication had fewer monocytes in their blood shortly after the heart attack.
Normally, having high levels of these immune cells soon after a heart attack are linked to more heart damage and worse outcomes for the patients. Lower levels, on the other hand, are associated with less damage to the heart and better healing.
The researchers also found that the medicine made the cells in the heart muscle more resistant to damage, so that more heart cells survived the heart attack.
The study showed that patients who received the anti-inflammatory drug (dark blue) had fewer monocytes in their blood shortly after the heart attack. Illustration from the researchers.
Changing immune cell behaviour to protective
As a result of the treatment, the way the monocytes behave was also changed.
“The function of the monocytes changed, from being more harmful to becoming more protective. The “good” functions of the immune cells were strengthened,” Huse says.
“We believe that those functions are the reason why patients suffer less damage after the heart attack. The heart is helped towards recovery,” she adds.
The study also showed another important effect: mechanisms that normally draw inflammatory cells into the damaged area were prevented in the patients who received the medicine.
What could this mean for heart attack patients in the future?
The research provides new insight into how inflammation affects the heart during a heart attack, and how this treatment can protect the heart from damage following STEMI.
This creates an opportunity for anti-inflammatory drugs to become part of a standard treatment for heart attacks and give patients a better life afterwards.
“The study shows that monocytes play an important role in the development of heart attacks. We believe that affecting these cells, which the blocking of IL-6 does, is beneficial. It could be a new and important additional treatment for these patients,” Dahl points out.
Why mechanism-focused research matters
The researcher believes that more such in-depth studies are needed when new medicines are tested.
“They provide a better understanding of the mechanisms behind illness and how the medicine affects the body. It doesn’t just tell us whether a treatment has worked, but also why or why not.
“Such knowledge can make new treatment options possible. This type of research should therefore be prioritised in future clinical studies,” Dahl says.
Reference
Huse C, Murphy SL, Yang K, Balzer NR, Stokke MK, Anstensrud AK, et al. The effects of interleukin-6-receptor inhibition on monocytes in STEMI: a substudy of the ASSAIL-MI trial. EBioMedicine. 2025. doi:10.1016/j.ebiom. 2025.105960
By Julie Nybakk Kvaal, Institute of Clinical Medicine
Dihydropyridine calcium-channel blockers linked to poorer kidney outcomes in people with type 2 diabetes
Photo by Towfiqu Barbhuiya on Unsplash
Commonly prescribed blood pressure medications known as dihydropyridine calcium-channel blockers (DCCBs) may be associated with poorer kidney outcomes in people with Type 2 diabetes (T2D) and diabetic kidney disease (DKD), according to new research presented at the 63rd European Renal Association (ERA) Congress in Glasgow, Scotland.1
Kidney Outcomes Worse with DCCBs in T2D
The findings suggest that patients receiving DCCBs alongside current standard-of-care kidney-protective therapies face a significantly higher risk of major adverse kidney events compared with those treated with alternative antihypertensive medications.
DKD remains one of the leading causes of kidney failure worldwide and is driven by chronic damage to the kidney’s filtering system caused by prolonged hyperglycaemia.2 Effective blood pressure control is a cornerstone of management, particularly alongside renin-angiotensin system (RAS) inhibitors and sodium-glucose cotransporter-2 (SGLT2) inhibitors, which have transformed outcomes for patients by slowing kidney disease progression and reducing the risk of kidney failure.
Researchers analysed data from 31 031 adults with T2D treated between 2016 and 2021. All participants were receiving both RAS and SGLT2 inhibitors. Of these, 12 172 patients were also prescribed DCCBs, while 18 859 received alternative blood pressure therapies. Participants were followed for a median of approximately 3.5 years.
After adjusting for baseline demographic and clinical differences, DCCB use was associated with a 33% increased risk of major adverse kidney events compared with other antihypertensive treatments. The composite outcome included a decline of at least 40% in estimated glomerular filtration rate (eGFR) or progression to end-stage kidney disease requiring dialysis or kidney transplantation.
Lead author Dr Timna Agur noted that DCCBs are widely used as second-line blood pressure therapies in DKD, making the findings particularly relevant to current clinical practice. The researchers propose that the observed association may stem from the drugs’ effects on kidney haemodynamics. By preferentially dilating blood vessels entering the kidney’s filtering units, DCCBs may increase pressure within these structures, potentially contributing to ongoing damage despite concurrent kidney-protective therapies.
Blood Pressure Treatment Choice May Matter
Although the study was observational and cannot establish causality, the investigators emphasised that the results warrant further investigation. Prospective studies and randomised controlled trials will be needed to determine whether alternative blood pressure treatment strategies could offer greater kidney protection for patients with DKD.
References
Li J et al. Epidemiological status, development trends, and risk factors of disability-adjusted life years due to diabetic kidney disease: a systematic analysis of Global Burden of Disease Study 2021. Chin Med J. 2025;138(5):568-578.
Agur T et al. DCCB therapy and risk of CKD progression in type 2 diabetes on RASi and SGLT2i. Abstract 597. ERA Congress, 3-6 June 2026.
The plan complements national response plans launched by the Governments of the Democratic Republic of the Congo and Uganda
The Africa Centres for Disease Control and Prevention (Africa CDC) (www.AfricaCDC.org) and the World Health Organization (WHO) today launched a joint continental preparedness and response plan on the ongoing Ebola outbreak caused by the Bundibugyo virus. The plan aims to raise US$ 518 million to support African countries together with partners to prepare for, rapidly detect and respond to the outbreak.
The six-month plan, covering June to November 2026, brings together governments, partners and communities under a unified ‘One Response’ approach to strengthen outbreak response measures, including emergency coordination, disease surveillance, laboratory testing, infection prevention and control, clinical care, community engagement, research, logistics and support for essential health services.
The plan complements national response plans launched by the Governments of the Democratic Republic of the Congo and Uganda.
“Ebola moves fast. Africa must move faster. This joint plan gives the continent a clear path to act with speed and unity: to save lives, support the affected countries and protect neighbouring communities, said Africa CDC Director-General Dr Jean Kaseya. “With Member States, WHO and partners, Africa CDC is turning commitment into action and resources into response for the communities at risk.”
WHO Director-General Dr Tedros Adhanom Ghebreyesus said: “The only way to beat this outbreak is through close partnership, working together under the leadership of the affected countries in one coordinated effort, guided by a simple principle: one plan, one budget, one team.”
He added: “Containing Ebola depends on political commitment, sustained financing, and the trust and engagement of communities. This plan places communities at the centre, because without their participation, contact tracing falters, safe care is delayed, and transmission continues.”
The plan also focuses on protecting vulnerable populations, strengthening cross-border collaboration, and supporting countries to respond quickly to new cases. At a time when there are no licensed vaccines or therapeutics specifically approved for the Bundibugyo species of Ebola, the plan aims to strengthen health systems to ensure resilience even as countries respond to acute health emergencies.
Implementation of preparedness and response activities is already underway across affected and at-risk countries. Furthermore, in 10 priority countries critical measures are being strengthened to enhance public health emergency preparedness and ensure early detection and swift response
.The plan emphasizes the need to maintain support for other ongoing health emergencies, including mpox, cholera and measles, to prevent disruptions to critical response efforts and safeguard progress towards stronger, more resilient health systems.
This coordinated effort comes as response operations accelerate in the Democratic Republic of the Congo, where authorities, with support from Africa CDC, WHO and partners, are ramping up efforts to curb the spread of the virus and end the outbreak.
Africa CDC and WHO urge Member States to strengthen screening and public health measures at points of entry and enhance cross-border coordination and solidarity to support a timely, effective and evidence-based response to the outbreak.
Through the joint preparedness and response plan, the continent is mobilising its collective expertise and resources to reinforce response measures, acting as one to control the outbreak and protect communities across the region. Its successful implementation will require strong political commitment, sustained investment and close collaboration among governments, health workers, communities and partners.
Drawing on lessons learned from previous Ebola outbreaks and recent public health emergencies, the plan also provides a pathway to broadly strengthen Africa’s capacity to prevent, detect and respond to future health threats while protecting lives and livelihoods.