Growing demand for a minimally invasive aortic valve replacement by adults under 65 with aortic stenosis may put many at greater risk for potentially more complicated heart surgeries later, according to University of Rochester Medicine research published in The Annals of Thoracic Surgery.
Scientists recommend patients work with a multidisciplinary heart care team to assess their short- and long-term needs when facing surgery.
The procedure, transcatheter aortic valve replacement (TAVR), is less invasive than open heart surgery, offering a faster recovery. Since its introduction in 2011, TAVR is the recommended alternative for frail adults over 65 who cannot withstand surgical aortic valve replacement (SAVR) and younger adults whose mortality risk is high.
However, analysis of the Vizient Clinical Database of nearly 14 000 aortic stenosis cases between 2018 and 2023 showed nearly half of the lowest risk patients under 65 underwent TAVR despite the recommendation that they undergo SAVR. And SAVR can be performed using less invasive techniques that can reduce recovery times.
“It’s not surprising that people want a ‘quick fix’ that lets them get back to their normal routine. However, TAVR is not without risks,” said Laurent G. Glance, MD, lead author and professor of Anesthesiology and Perioperative Medicine. “The bioprosthetic valve can wear out or leak and lead to additional complicated surgeries later.”
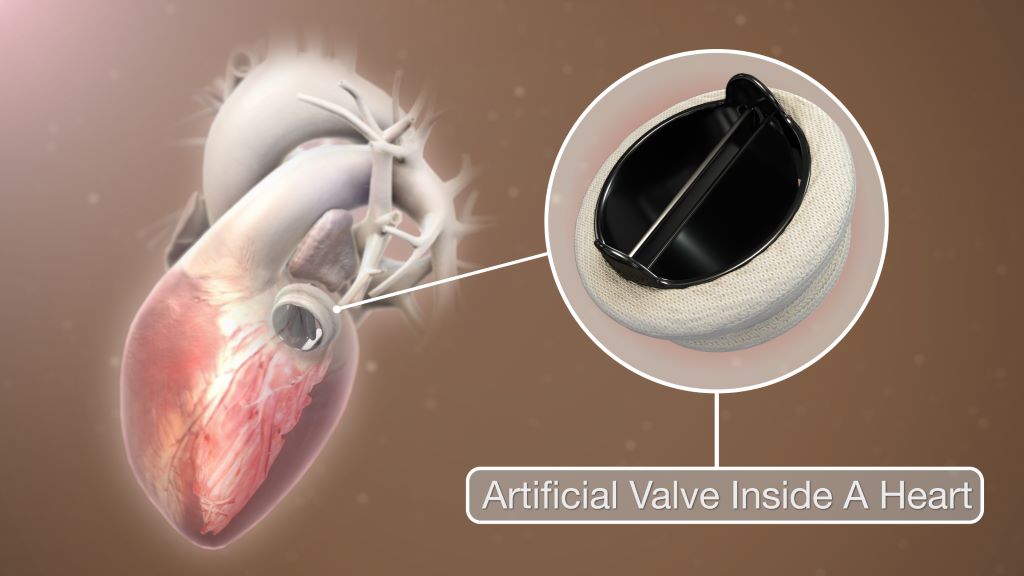
Aortic stenosis is diagnosed when the aortic valve gets thick and narrow, restricting blood flow, forcing the heart to work harder. It causes shortness of breath, fatigue, dizziness and can lead to heart failure.
The TAVR technique delivers the new valve through a catheter in the groin and threaded through the femoral artery into the heart. Once inside, it is placed and expanded inside the failing valve.
Researchers reviewed hospital practice data and risk calculations and concluded “the marked use of TAVR among low-risk younger patients…may not represent the optimal long-term strategy for young patients.”
Explanting and replacing a failed TAVR valve requires SAVR, the open surgical approach, which the younger patients initially aimed to avoid. They face potentially slow and painful recovery and face risk of serious complications such as life-threatening stroke.
Co-author and chief of Cardiac Surgery Peter Knight, MD, said the rapid adoption of TAVR for younger adults has outpaced the data to assess durability of the valve and long-term patient outcomes.
“Careful decision-making is needed and patients should do their homework and talk with their physicians,” Knight said. “You have to look at the short- and long-term needs when making this important choice.”
Researchers have discovered how part of the body’s immune system could better combat a leading cause of death for people with cystic fibrosis (CF).
A team led by The University of Queensland’s Professor Peter Sly and Dr Abdullah Tarique has identified how macrophages – the white blood cells that fight infection in the body – function differently in people with CF, compared to others.
“Macrophages play a critical role in fighting infection, especially in the lungs,” Professor Sly said.
“They’re the ‘Pac-Man’ cells that find and ‘gobble up’ bacteria and pathogens such as mycobacterium abscessus (MABS).
“We found people with CF have multiple defects in their macrophages that leave them more vulnerable to infection, even when taking the most effective CF drug treatment available.”
Professor Sly said MABS posed the biggest infection risk for people with CF.
“MABS is resistant to many antibiotics which makes treatment complex and often unsuccessful,” he said.
“The infection can exclude a patient from being eligible for a lung transplant and is a leading cause of death for people with CF.
“And because of antibiotic resistance, MABS infections are increasing at alarming rates.”
Professor Sly said in people with CF, macrophages aren’t as efficient at both recognising and killing off bugs in the body.
“CF involves a defect in the CFTR protein, the channel on the cell’s surface responsible for transporting ions and chlorine in and out of cells,” he said.
“That lack of chlorine transport means macrophages don’t activate their killing functions to ‘eat’ the bugs.
“A second important mechanism in macrophages is also deficient – the zinc transport of proteins.
“Zinc is a potent antibacterial mechanism used to poison bacteria, but with less zinc and less zinc transporter proteins in CF macrophages, they’re less able to fight the infection.”
Professor Sly said a third defect – in the mitochondria – is perhaps the most significant.
“Mitochondria are the batteries or power packs of cells, and produce things called reactive oxygen species to kill bacteria.
“In CF, not only are macrophages less able to make these reactive oxygen species, but they’re also not able to keep reproducing them to increase their mitochondrial mass when infected.”
The research also examined treatments for CF and found even the most effective drug doesn’t boost macrophage’s ability to kill MABS.
“Elexacaftor-tezacaftor-ivacaftor (ETI) has been revolutionary in CF treatment by improving lung function in many people, meaning fewer exacerbations and hospitalisations,” Professor Sly said.
“But it doesn’t fix this part of the immune system, which is why people with CF still get these infections.
“Our findings show we now need to accelerate research into different mechanisms of increasing macrophage function, to identify and initiate killing strategies for MABS.
“This could significantly reduce the impact of these infections for people with CF.”
Read the research in Proceedings of the National Academy of Sciences.
University of Pretoria’s Professor Mashudu Tshifularo is leading a groundbreaking clinical trial for 3D-printed ossicles,
Forty-five patients with conductive hearing loss from middle-ear damage are eagerly awaiting the start of clinical trials, led by University of Pretoria’s Professor Mashudu Tshifularo, on a ground-breaking procedure to restore hearing.
The trials, due to begin within weeks at Steve Biko Academic Hospital in Pretoria, come seven long years after Prof Tshifularo successfully performed the world’s first middle-ear transplant using 3D-printed bones made from titanium. The patient was Thabo ***, whose middle-ear bones – the ossicles – had been injured in an accident, causing almost total hearing loss until he had the transplant in March 2019.
In a video screened at a UP Roundtable event held in April this year to announce the launch of the upcoming clinical trials, a beaming Thabo *** confirmed he had regained his hearing after the transplant and had continued to enjoy excellent hearing ever since.
While this procedure was hailed as a surgical breakthrough at the time, its full acceptance by the South African and global ear, nose and throat (ENT) community depends on formal clinical validation. Despite the many obstacles he knew would lie ahead, Prof Tshifularo, joint head of UP’s Department of Otorhinolaryngology, was determined to take his innovation through clinical trials.
“Today is a culmination that I never thought would come. There was a time when I cried, there was a time when I was very depressed, there was a time when I nearly gave up, but something inside me told me to remain steady,” he said at the Roundtable, where the announcement was made that clinical trials could finally move ahead now that all the necessary regulatory, ethical and licensing clearances have been obtained, including from the South African Health Products Regulatory Authority (SAHPRA).
The years since Prof Tshifularo performed that first transplant have also been spent developing, perfecting, testing and patenting a prototype of the titanium material and implants for the clinical trials. UP’s engineering partner on this project, the Council for Scientific and Industrial Research (CSIR), was responsible for the materials and prototype development, while HH Industries manufactures the implants, using 3D printing technology, and Marcus Medical is providing the robotic technology to be used during the surgery. Seed funding was provided by the Motsepe Foundation.
Ready to transform lives
Now that it is all-systems-go for this all-South African collaborative effort, Prof Tshifularo and his team aim to perform this life-changing surgery in the next 12 months on all 45 patients who have expressed interest in participating in the clinical trials.
The team will then focus on publishing their research and training future researchers and medical teams so that the work can be amplified far and wide for the benefit of humanity.
“My dream is to make deafness history,” Prof Tshifularo said, noting that an estimated two billion youth are living with undiagnosed, mostly noise-induced hearing loss, which would become a severe problem in the next 20 to 25 years. Hearing loss is also common among the world’s rapidly ageing population.
The procedure itself takes about three hours and uses advanced robotics to remove the damaged middle-ear bones and replace them with the 3D printed titanium bones. This is minimally invasive, carries significantly less risk than conventional procedures and leaves minimal scarring. The titanium used to manufacture the ossicles is biocompatible, meaning it can be introduced into the ear without causing harmful reactions.
“This innovation will ultimately transform the lives of many people, including newborn babies born with congenital middle-ear defects,” said Prof Themba Mosia, Vice-Principal: Student Life, who gave the opening address at the Roundtable. “It exemplifies the spirit of innovation and collaboration at the university, combined with the deep medical expertise needed to restore hearing.”
UP at the forefront of healthcare advancements
Prof Flavia Senkubuge, Dean of UP’s Faculty of Health Sciences, said innovations such as Prof Tshifularo’s middleear surgical procedure place the university “front and centre” of healthcare advancements on the African continent and the world stage.
She reiterated UP’s commitment to deploying its innovations for the benefit of local communities, such as by establishing a “one-stop shop” – most likely in the form of a private day hospital – where community members could benefit from advanced clinical technologies and the expertise of its researchers.
Paying tribute to Prof Tshifularo, long-time colleague Dr Christian Quitter thanked Prof Tshifularo “for having the guts” to persevere with his innovation, even when it was not always supported by the ENT establishment.
He also thanked the university for supporting researchers who “think out of the box in seeking to improve the lives of all humanity”.
With colorectal cancer a growing concern among younger people, the American Cancer Society has endorsed two new types of stool tests to encourage people to get screened while also recommending a limited role for new blood tests many patients find appealing.
The recommendations are an update to the ACS’s screening guidelines – an update led by Andrew Wolf, MD, a cancer-prevention expert at UVA Health. He and a blue-ribbon panel of cancer experts conducted a systemic review of the available colorectal cancer tests to determine which are most effective. In addition to recommending a next-generation DNA stool test and a new type of RNA stool test, the group is advising doctors to recommend blood tests only to patients who decline all other options.
The recommendations come with a dose of pragmatism: “The most effective screening test,” the panel concludes, “is the one that the patient completes.”
“The new guidance adds a stool RNA test and an updated stool DNA test to the menu of preferred options for colorectal cancer screening, which currently include colonoscopy and stool tests that detect tiny amounts of blood, among other options,” said Wolf, a professor emeritus at the University of Virginia School of Medicine. “Although the idea of a blood test for colorectal cancer sounds very attractive, they aren’t yet as good as the other tests at detecting precancerous growths and early-stage cancer, so we don’t believe they are as effective as a screening test. That said, we’re very hopeful that broadening the array of options will get more folks screened and reduce the burden of suffering from colorectal cancer.”
About Colorectal Cancer
Colorectal cancer is the second-leading cause of cancer deaths in the United States, killing 55 000 people in 2026. Improvements in detection, screening and treatment have contributed to declining colorectal cancer death rates over the last several decades, but that decline has been accompanied since 2013 by an alarming increase in the cancer among people under the age of 50. Among that age group, colorectal cancer is now the leading cause of cancer death for men and the second-leading cause for women.
In response, the American Cancer Society in 2018 lowered the recommended age for initial colorectal cancer screening from 50 to 45 for people at average risk. It also affirmed the importance of screening tools such as stool-based tests as well as visual exams such as colonoscopies. Since then, however, new, multi-target stool tests and blood-based screening tests have become available. The new blood tests proved popular in a patient survey, with 53% of respondents saying they would prefer blood testing every three years to taking a stool test every year or receiving a colonoscopy every 10.
For the latest guideline update, Wolf and his colleagues examined the effectiveness of the new tests to provide doctors with guidance on if, how and when they should be used. The experts conclude that the DNA and RNA tests had high sensitivity for detecting colorectal cancer and moderate sensitivity for detecting advanced precancerous lesions that are about to turn into cancer. The blood tests, on the other hand, showed lower sensitivity for both advanced precancerous lesions and stage 1 cancers.
“While colorectal screening blood tests may not be as effective as other options, they are certainly better than not screening,” Wolf said. “So if a patient declines a stool test or a visual exam like a colonoscopy, a blood test would be the way to go, as long as the patient understands it is not as effective, and, if it is positive, they will still need to have a colonoscopy.”
Based on their results, the experts endorse the stool tests for patients at average risk but urge doctors to reserve the blood tests for patients who refuse other screening options. And they recommend that anyone who tests positive on any stool or blood test should receive a colonoscopy promptly.
It’s important, they note, that doctors explain to patients the strengths and weaknesses of the available tests so that patients can make informed decisions.
“Currently, almost a third of adults are not up to date with colorectal cancer screening, and among those ages 45 to 49, it’s twice that number,” Wolf said. “We hope these new options will help to close this gap. The most important message is that colorectal cancer is a disease you don’t have to die from, and there’s a screening test out there that’s right for you.”
Better preventing, detecting and treating cancer is the core mission of UVA Comprehensive Cancer Center, one of only 57 cancer centers in the nation to earn the prestigious “comprehensive” designation from the National Cancer Institute. That designation is awarded only to elite cancer centers with the most outstanding cancer care and research programs in the country.
In our research in the British Library’s medieval collections, we have identified a previously unnoticed document that provides fresh insights into the survivors of the outbreak of plague known as the Black Death (1346–53).
The document – a scrap of parchment inserted into an account of the Ramsey Abbey manor of Warboys in Huntingdonshire – records how much time peasants were absent from work when struck down by the plague. It also reveals the names of those who survived and how long their employers believed recovery could take.
In our recent paper with Barney Sloane we shed new light on a group of 22 tenants who probably contracted plague, languished on their sickbeds for several weeks, and then recovered.
As one of the deadliest pandemics in recorded history, it has been estimated that between a third and two-thirds of the population of medieval Europe died during the Black Death.
The Triumph of Death by Pieter Bruegel the Elder (1562) shows the social upheaval that followed the plague. Museo del Prado
Given the sheer scale, many historians have focused on discovering details about those who died. Yet this has left the histories of those who contracted plague and recovered largely untold.
Despite the deadliness of the disease, it was possible to recover from plague, and medieval chroniclers mention the possibility – however unlikely – of survival. For example, Geoffrey le Baker, a clerk of Swinbrook in Oxfordshire, wrote in the following decade that he thought recovery depended on people’s symptoms:
People who one day had been full of happiness, on the next were found dead. Some were tormented by boils which broke out suddenly in various parts of the body, and were so hard and dry that when they were lanced hardly any liquid flowed out. Many of these people escaped, by lancing the boils or by long suffering. Other victims had little black pustules scattered over the skin of the whole body. Of these people very few, indeed hardly any, recovered life and health.
But who recovered? Why did so many succumb to the disease when others survived? And just how long was this “long suffering”? Unfortunately, there is remarkably little documentary evidence because most medieval sources record information about mortality rather than ill health.
Unique list of plague survivors
A unique inclusion in the account of the manor of Warboys details a group of people who fell ill between the end of April and the start of August 1349. The monks of Ramsey Abbey wrote a list of their tenants who had fallen sufficiently sick that they could not work on the lord’s lands and detailed the length of time that they were absent.
People were clearly affected differently by their experience of plague.
The quickest recovery was that of Henry Broun who missed just a single week of work. By contrast, John Derworth and Agnes Mold had much more protracted illnesses and were both absent for nine weeks.
The average length of illness was between three and four weeks, with three-quarters of people returning to work in under a month. The speed of their recoveries is all the more surprising given that they were entitled to up to a year and a day of sick leave from work.
This list of survivors includes a preponderance of tenants who occupied larger holdings on the manor. It has long been debated by historians and archaeologists whether the plague killed indiscriminately, with no regard to status, sex or age, or whether the poor and elderly were more vulnerable.
The survival of so many wealthier tenants could indicate that their higher living standards enabled them to recover more readily than their poorer neighbours, perhaps because they were able to stave off secondary infections and complications. We should not read any significance into the fact that 19 out of the 22 people were men: this reflects the gender bias of manorial landholding rather than any sex-selectivity of plague.
Although 22 people may not seem like many, in a regular year during the 1340s, only two or three absences were recorded during the summer months. It, therefore, represents a tenfold increase in regular illnesses on the manor. Put another way, these sick tenants were absent for 91 weeks’ worth of labour services during just a 13-week period.
Our understanding of the impact of the Black Death has been influenced by the appalling scale of death. Yet it is only when we add those who fell ill and recovered back into the picture that we can truly understand the seismic shock the pandemic had on society. The dead, dying and sick must have considerably outnumbered the living in villages and cities across Europe.
The consequences of this can be seen in medieval accounts and chronicles, one of which records that “there was so great a shortage of servants and labourers that there was no one who knew what needed to be done”. As a result of this combination of high mortality, unprecedented illness and abysmal weather, the two harvests of 1349 and 1350 have been described as the worst experienced in medieval England, worse even than those that caused the great famine of 1315-17.
This archival discovery allows us to write the history of sickness and recovery back into the Black Death, demonstrating that recovery was possible even during one of the worst pandemics in recorded history.
This new evidence reveals the remarkable resilience of medieval peasants. Many of them lay languishing on their sickbeds, exhibiting buboes (the painful, swollen and inflamed lymph nodes on the groin and neck that were typical of the Black Death), vomiting blood and wracked by fevers and not only survived but returned to work in just a few short weeks.







.jpg){kind=link}
{kind=link}
{kind=link}