A woman receiving a mammogram, Source: National Cancer Institute
For women with large breast sizes, receiving radiotherapy with prone positioning is less toxic than while supine, according to a study published in JAMA Oncology.
Patients treated in the supine position had significantly higher rates of moist desquamation anywhere in the breast compared with those treated in the prone position (39.6% vs 26.9%).
“Treatment in the prone position has several dosimetric advantages for these patients,” the researchers explained. “It allows for more homogeneous dose distribution owing to the smaller separation when compared with the supine position, which decreases deposition of higher doses in the inframammary fold and axilla.”
Fewer toxic effects of the skin were seen when patients were treated with hypofractionated radiotherapy compared with extended fractionation, they added.
“Prone radiotherapy appears to be an excellent option for patients with large breast size and right-sided breast cancer, and may benefit many women with left-sided breast cancer with large breast size if acceptable cardiac avoidance is feasible,” observed Mayo Clinic’s Dean Shumway, MD, and Cedars-Sinai Medical Center’s Katelyn Atkins, MD, PhD, in an accompanying editorial. “In summary, prone positioning for whole-breast radiotherapy represents a valuable addition to the armamentarium of treatment techniques to reduce the adverse effects associated with whole-breast radiotherapy.”
Of the 357 women (mean age 61 years) included, 182 were treated in the supine position and 175 were treated in the prone position.
From April 2013 until June 2016, 167 patients received 50 Gy in 25 fractions (extended fractionation) with or without boost (range 10-16 Gy). After the trial was amended in June 2016, the majority of patients (93.2%) received the hypofractionation regimen of 42.5 Gy in 16 fractions.
The researchers also found that the supine position was associated with more grade 3 desquamation compared with the prone position (15.4% vs 8.0%; OR 2.09, 95% CI 1.62-2.69, P<0.001).
In addition, when broken down by treatment with either extended fractionation or hypofractionation, extended fractionation was associated with more:
Toxic effects (43.3% vs 23.2%)
Grade 3 desquamation (17.2% vs 6.3%)
Pain (9.4% vs 3.4%)
“These differences were primarily driven by the rates of toxic effects in patients treated in the supine position,” the authors noted.
Specifically, in patients treated in the supine position, extended fractionation was associated with increased desquamation compared with hypofractionation (51.1% vs 27.8%), and grade 3 desquamation (23.9% vs 6.7%).
Extended fractionation was also associated with increased toxicity in patients treated in the prone position, although the link was less pronounced. Desquamation occurred in 35.2% of patients treated with extended fractionation versus 18.4% of patients treated with hypofractionation (OR 2.41), while grade 3 desquamation occurred in 10.2% versus 5.7% of patients (OR 1.87).
No differences in quality of life as measured by global health status, breast symptoms, or pain scales between the supine and prone groups were seen, the researchers noted.
New research published in the journal Behavioural Processes demonstrates that by killing essential gut bacteria, antibiotics ravage athletes’ motivation and endurance. This study, which examined mice, suggests there is a big difference in the gut microbiome of athletes and couch potatoes.
Much research has been done on how exercise impacts the gut microbiome, but this study is one of few to examine the reverse – how gut bacteria also impact voluntary exercise behaviours. Engaging in voluntary exercise involves both motivation and athletic ability.
“We believed an animal’s collection of gut bacteria, its microbiome, would affect digestive processes and muscle function, as well as motivation for various behaviours, including exercise,” said Theodore Garland, UCR evolutionary physiologist in whose lab the research was conducted. “Our study reinforces this belief.”
Researchers confirmed through faecal samples that after 10 days of antibiotics, gut bacteria were reduced both in a group of ‘athletic’ mice bred for running on wheels and those that were not. Since no sickness behaviour was seen in the mice, exercise changes were ascribed solely to changes in antibiotic-induced changes in the gut bacteria.
Wheel running in the athletic mice was reduced by 21%, and the high runner mice did not recover their running behaviour even 12 days after the antibiotic treatment stopped.
Meanwhile, for the normal mice, antibiotics caused no difference in the running behaviour.
“A casual exerciser with a minor injury wouldn’t be affected much. But on a world-class athlete, a small setback can be much more magnified,” said Monica McNamara, UCR evolutionary biology doctoral student and the paper’s first author. “That’s why we wanted to compare the two types of mice.” Knocking out the normal gut microbiome might be compared with an injury.
One way the microbiome might affect exercise in mice or in humans is how carbohydrate metabolites are used by the muscles.
“Metabolic end products from bacteria in the gut can be reabsorbed and used as fuel,” Garland said. “Fewer good bacteria means less available fuel.”
The researchers would next like to identify the gut bacteria contributing to increased athletic performance. “If we can pinpoint the right microbes, there exists the possibility of using them as a therapeutic to help average people exercise more,” Garland said.
Lack of exercise is a risk factor for many diseases, and researchers would like to find ways of encouraging it more.
“Though we are studying mice, their physiology is very similar to humans. The more we learn from them, the better our chances of improving our own health,” Garland said.
Research into foods that can increase desirable gut bacteria is ongoing, and Garland recommends a balanced diet in addition to regular exercise to promote health.
According to the Centers for Disease Control and Prevention, men, on average, die five years earlier than women and die at higher rates from three leading causes of death – heart disease, cancer, unintentional injuries – and, more recently, from COVID. During Men’s Health Month, we encourage men to take control of their health and for families to teach young boys healthy habits throughout childhood.
In June every year, we pay special attention to men’s health. Men’s Health Month aims to heighten the awareness of preventable health problems and encourage early detection and treatment of disease among men and boys. This month allows health care providers, public policymakers, the media, and individuals to encourage men and boys to seek regular medical advice and early treatment for disease and injury.
Men are more reluctant to seek healthcare
A health gap exists – men die younger than women, and they are more burdened by illness during life. They fall ill at a younger age and have more chronic conditions than women. Research by Harvard Health Publishing shows that men are more than three times more likely than women to develop kidney stones, become alcoholics, or have bladder cancer. They are about twice as likely to suffer from emphysema or a duodenal ulcer. Although women see doctors more often than men, the healthcare investment required for caring for men amounts to much more, especially beyond the age of 65.
However, society expects men to be seen as tough, push through pain, and rarely show signs of weakness. This mindset subconsciously trains men to believe that seeking help of any kind – including going to the doctor – exhibits weakness. But it is not only society’s influence that plays a part. Further research shows that 21% of men tend to avoid the doctor because of fear. They worry about an adverse diagnosis or a bad outcome. This same research finds that only 40% of men go to the doctor only when they have a severe health issue and never go for routine check-ups. It is far lower than women’s frequency of doctor visits, and it is a concerning figure.
Unfortunately, mental health is also one of the most stigmatised issues affecting men. The American Psychological Association reports that 30.6% of men have suffered from depression in their lifetime, and their hesitation to seek care may be worsening this issue. As a trend, men are notorious for not talking about their feelings. Psychologists have documented that discussing emotions is just another form of vulnerability that can lead to discomfort for men. It can be scary for many men to begin sharing their feelings. But the payoff is worth it: men who express their feelings verbally are less likely to express them violently.
How Medshield supports men
Medshield offers a variety of plans that suit members of every age and budget. Our Managed Care Programmes assist our members with managing chronic conditions in collaboration with the member’s respective treating practitioners. We encourage men to utilise our Wellness Benefits which include cover for annual tests e.g. cholesterol and PSA Screening, for early diagnosis and treatment. Our benefit plans allow you the freedom to visit your doctor for a general appointment at any time to monitor your overall health, and our plans have robust mental health benefits to ensure holistic care.
Many people feel that medical aid schemes cost too much, but having the right planmeans you won’t need to rely on state clinics and hospitals for care. It also means you can have tests, screenings, and procedures done early without waiting to save enough cash for it (and potentially worsening your condition). Healthcare does not always just require hospital stays, either – sometimes other expenses appear in physiotherapy, dental visits, and even costly chronic medication that most would struggle to cover each month. Nobody can predict what the future holds, and unfortunately, sometimes the sudden onset of illness or an accident are common aspects of life.
We encourage men to take charge of their health!
Let’s work together to turn these trends around. This June, we invite all men to take that step toward a healthier lifestyle and to get screened for any potential illnesses. You may be resistant at first, but persistence is powerful, and you’ll be doing your part to improve your health.
Here are ten tips to start on your new health journey:
Avoid tobacco in all its forms.
Eat well. That means eating more healthful foods and fewer harmful foods.
Get at least 30 minutes of moderate exercise nearly every day.
Stay lean. It’s equally hard for men and women, but partial success will help.
If you choose to drink, limit yourself to one to two drinks a day, counting 150ml of wine, 375ml of beer, and 30 ml of spirits as one drink.
Reduce stress by getting enough sleep and building social ties and community support.
Avoid risky behaviour, including drug abuse, unsafe sex, dangerous driving, unsafe firearm use, and living in hazardous household conditions.
Get regular medical check-ups, screening tests, and immunisations.
Seek joy and share it with others – laughter is good medicine. Fun and optimism improve health as well as happiness.
People with both Type 1 and Type 2 diabetes are prone to tooth decay, and a new study published in Archives of Oral Biology may explain why: reduced strength and durability of enamel and dentin, the hard substance under enamel that gives structure to teeth.
Researchers induced Type 1 diabetes in 35 mice and used a Vickers microhardness tester to compare their teeth with those of 35 healthy controls over 28 weeks. Although the two groups started with comparable teeth, enamel grew significantly softer in the diabetic mice after 12 weeks, and the gap continued to widen throughout the study. Significant differences in dentin microhardness arose by week 28.
“We’ve long seen elevated rates of cavity formation and tooth loss in patients with diabetes, and we’ve long known that treatments such as fillings do not last as long in such patients, but we did not know exactly why,” said Mohammad Ali Saghiri, an assistant professor of restorative dentistry at the Rutgers School of Dental Medicine.
The study advances a multiyear effort by Assistant Prof Saghiri and other researchers to understand how diabetes affects dental health and to develop treatments that counter its negative impact. Previous studies have established that people with both types of diabetes have significantly elevated rates of most oral health issues, both in the teeth and the soft tissues that surround them. Assistant Prof Saghiri and other researchers also have demonstrated that diabetes can interfere with the ongoing process of adding minerals to teeth as they wear away from normal usage.
“This is a particular focus of mine because the population of people with diabetes continues to grow rapidly,” Assistant Prof Saghiri said. “There is a great need for treatments that will allow patients to keep their teeth healthy, but it has not been a major area for research.”
The delivery of the primary healthcare approach and the achievement of any semblance of universal health coverage are moot if South Africa does not rapidly address the critical skills shortages and working conditions of nurses, especially those with specialised skills, including midwives.
“The pandemic very clearly highlighted the crucial role that nurses play in the frontline of healthcare, and how important they are in ensuring that patients have access to quality health services and disease prevention, management and education. However, a combination of factors is stymieing attempts to grow our nursing capabilities and skills – from changes in the nurse training curriculum, limitations of and delays in the accreditation of training facilities, poor working conditions and workplace safety, lack of equipment and resources, low remuneration by global standards, the regulatory uncertainty around NHI, changing social dynamics which has seen declining nursing recruits, as well as the significant mental health deterioration that nurses have battled for two years of being on the frontline of the pandemic. Add to this the fact that we have a significant number of experienced nurses heading for retirement age without the commensurate follow through of new nursing talent coming through, and we have the makings of a serious crisis,” warns Paul Cox, Managing Director at the Essential Group of Companies including health insurance provider, EssentialMED.
“Making matters worse, South Africa’s nurses are in huge demand in many first world countries that suffer the same skills shortages. These countries offer significantly higher pay and better working and living conditions to attract talent to their shores. This is a significant risk as South Africa is losing some of its most experienced nurses and healthcare workers to emigration, and with it we lose vast amounts of institutional knowledge, specialisation, experience, training investment and mentoring and training skills,” he adds.
Data published by the South African Nursing Council (SANC) in 2021 shows that the country has a nursing staff contingent of one nurse to 213 patients – the World Health Organisation recommends a ratio of 1 nurse to 5 patients in a general hospital. While there are currently around 280,000 nurses in active employment and a further 21 000 nurses in training, the 2030 Human Resources for Health Strategy projects a shortage of 34 000 nurses in primary healthcare by 2025 if nothing is done to attract new talent to the nursing sector. According to SANC’s 2020 statistics, the ageing population of South Africa’s nursing population is another looming crisis. Its statistics show that less than a third of the registered nurses and midwives are under the age of 40, while 47% of registered nurses will have retired within the next 15 years. Primary healthcare will take a big hit given the important role of nurses in primary healthcare delivery, and TB, HIV and diabetes management programmes are likely to falter, with patients in remote and rural areas impacted the most.
Perplexingly, despite these serious skills shortages and looming crisis, nurses never made it onto the Critical Skills List released by the Department of Home Affairs at the end of February 2022, despite the huge demands that Government’s drive to NHI will make on already stretched and overburdened healthcare human resources.
“The implications of the current skills shortages and deteriorating working and safety conditions, notably in the public sector which takes care of more than 80% of the population, are plain to see. We already have a situation where healthcare facilities are struggling to fill posts – there are some 21,000 specialist medical personnel posts vacant across all provinces and which the Department of Health has thus far been unable to fill. What more then will the implications be for healthcare delivery under the proposed universal healthcare system of NHI? The Department of Health has acknowledged that the NHI will need skilled personnel to function not only across healthcare professionals, but general skilled human resources to underpin the health system. Right now, even the most fundamental of primary care delivery is in crisis due to skills shortages, exacerbated by the deleterious state of many public healthcare facilities and regular medicine stock-outs. More skilled and experienced nursing professionals are heading offshore, and at the same time, the sector is struggling to attract and train new nursing recruits to a profession and working environment that are increasingly unattractive to young South Africans. The planned introduction of the National Health Insurance scheme adds further grist to the wheel, with industry experts warning of a mass exodus of healthcare skills due to the valid concerns around the lack of financial and operational clarity of the plan,” adds Cox.
The current and future dwindling nurse staffing levels are a serious threat to patient health, safety and quality of care. Equally so to the health and safety of nurses due to increasing pressure on the remaining workforce to meet ever growing healthcare needs, fatigue and burnout, mental health issues and deteriorating work conditions. Poor resource allocation and poor maintenance of healthcare facilities need to be urgently addressed, and there needs to be the political will to dramatically improve the working conditions of the nurses who form the backbone of healthcare delivery. It is crucial that both public and private sector stakeholders collaborate to help bridge the skills challenges. A major acceleration of training is needed, and to do this it’s essential to fast-track the new education requirements and processes and accredit more nurse training colleges, allowing the private sector to contribute to closing the skills gap.
“Nurses are the single largest group of healthcare providers in our country representing 56% of all healthcare providers. The performance of our healthcare system – both public and private – is dependent on the quality of care provided by these professionals. Nurses are central to addressing the complex burden of disease, achieving the primary healthcare (PHC) approach as purported under universal health coverage, as well as improving health system performance across both the public and private healthcare sectors. The pandemic has shown unequivocally the need to value our nurses, to invest in nursing, resolve the nursing education challenges as a matter of priority, as well as address their working conditions, remuneration, practice environment, resources, management and leadership. Without a strong, skilled and growing nursing profession, any semblance of NHI and universal health coverage success in South Africa is questionable,” concludes Cox.
As falling infection rates are beginning to indicate the end of the fifth wave, a paper in the South African Journal of Sciences asks the question – how was it ever feasible for marginalised South Africans to be able to engage in social distancing?
According to a recent seroprevalence study, the vast majority of people in South Africa now have antibodies against COVID in their blood, many acquired through infection and not immunity. The editorial review by Professors Jonathan Jansen and Shabir Madhi, at Stellenbosch University and Wits University, explores the realities of the majority of the population as they struggled under the lockdown.
Just over two years ago, SA garnered praise for instituting one of the harshest lockdowns in the world. In late 2021, while the world panicked over emergence of the Omicron variant, SA led the way with a sharp change in thinking: there was no way now to practically contain COVID with social distancing measures, so it was best to return to as close to normal as possible. This came with an admission that lockdown in SA had failed, and was it doomed from the start with its structural inequalities. SA’s lauded lockdown came with the grotesque spectacle of soldiers forcing people back into their shacks, after all.
Jansen and Madhi considered that a joint UK–SA study found that difficulty adhering to lockdowns or outright noncompliance was largely reported by black Africans in temporary housing. Such conditions entailed lack of savings and access to basic amenities such as private toilets, making lockdown adherence virtually impossible.
Jansen and Madhi observed that inequities were readily apparent, with in-hospital COVID mortality rates being 1.2- to 1.3-fold higher in black African patients, coloured patients and patients of Indian descent compared to white patients. Patients were also 1.5 times more likely to die in public healthcare as opposed to private healthcare, with greater likelihood of ICU admission and mechanical ventilation.
Looking at the impact of gender, voices of experts were mostly (70%) male, Jansen and Madhi noted, and researchers found that COVID had disproportionate impacts on female academics.
The pandemic also brought the ethical question of vaccine mandates, where it was argued that it was permissible for the greater good. But there was a stumbling block of how would consent for enrolment be gained? The SISONKE trial showed that, even among healthcare professionals, informed consent was a problem. Most (71.5%) participated for access to the vaccine, but nearly a third (32%) did not realise that breakthrough infections and adverse events had to be reported two years on.
“Despite the numerous lockdowns and restrictions in South Africa, the benefits thereof are questionable.”
Overall, studies challenged the benefit of the lockdown. Jansen and Madhi argue that, “Despite the numerous lockdowns and restrictions in South Africa, the benefits thereof are questionable.” Even before the Omicron wave, 73% of South Africans were estimated to have been infected at least once.
SA nevertheless was able to leverage its skills and resources to enter into COVID vaccine manufacture and knowledge sharing, but sustainability ultimately depends on commitment to vaccine programmes in Africa.
Jansen and Madhi stress that the economic costs of the lockdown are ongoing, an by 2021 only 42% of the working population remained employed in SA. Modelling shows that employment might only return to 2018 levels by around 2024 to 2026.
“Consequently, the full societal impact of the COVID-19 pandemic is yet to materialise; and imposing and retaining ongoing regulations under the pretence of trying to prevent SARS-CoV-2 infections, when all indications are that they have failed dismally in the South African context, warrant immediate abandonment.”
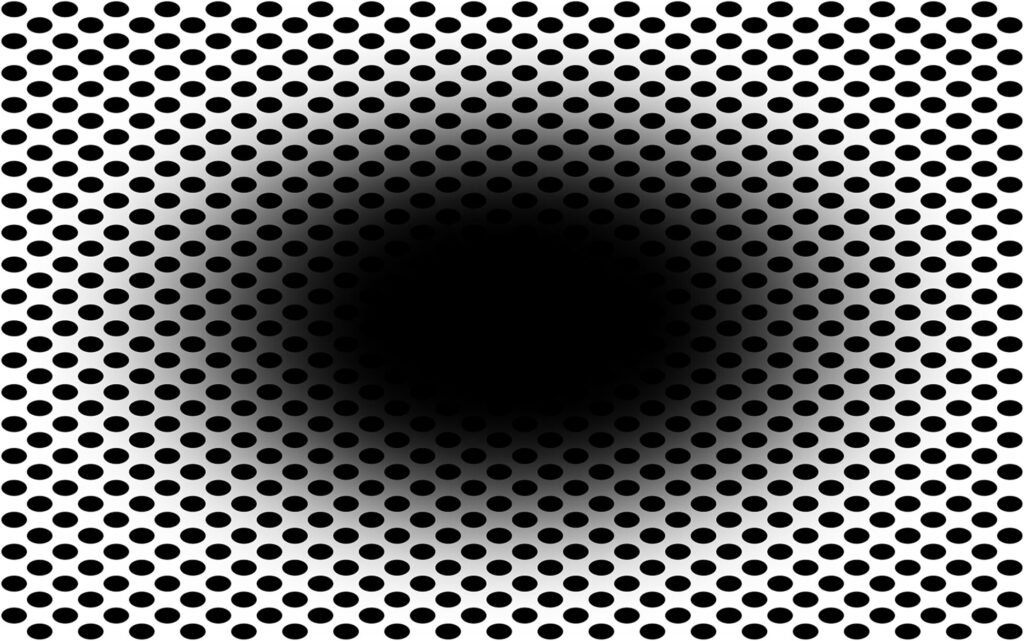
Looking at this image, do you perceive that the central black hole is expanding, as if you’re moving into a dark environment, or falling into a hole? If so, you’re not alone: a new study published in Frontiers in Human Neuroscience shows that this ‘expanding hole’ illusion, which is new to science, is perceived by approximately 86% of people.
The study’s first author, Professor Bruno Laeng at the University of Oslo, explained: “The ‘expanding hole’ is a highly dynamic illusion: The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel.”
Optical illusions aren’t simple curiosities: researchers study them to better understand the complex processes our visual system uses to anticipate and make sense of the visual world.
In the new study, Prof Laeng and colleagues demonstrated that the ‘expanding hole’ illusion deceives the brain so well that it even prompts a dilation reflex of the pupils to let in more light, just as if the observer was entering a dark area.
“Here we show based on the new ‘expanding hole’ illusion that that the pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye. The illusion of the expanding hole prompts a corresponding dilation of the pupil, as it would happen if darkness really increased,” said Prof Laeng.
Prof Laeng and colleagues explored how the colour of the hole (besides black: blue, cyan, green, magenta, red, yellow, or white) and of the surrounding dots affect how strongly we mentally and physiologically react to the illusion. On a screen they presented variations of the “expanding hole” image to 50 women and men with normal vision, asking them to rate subjectively how strongly they perceived the illusion. While participants gazed at the image, the researchers measured their eye movements and their pupils’ unconscious constrictions and dilations. As controls, the participants were shown “scrambled” versions of the expanding hole image, with equal luminance and colours, but without any pattern.
The illusion appeared most effective when the hole was black. Fourteen percent of participants didn’t perceive any illusory expansion when the hole was black, while 20% didn’t if the hole was in color. Among those who did perceive an expansion, the subjective strength of the illusion differed markedly.
The researchers also found that black holes promoted strong reflex dilations of the participants’ pupils, while coloured holes prompted pupil to constriction. For black holes, but not for coloured holes, the stronger participants rated their perception of the illusion, the more their pupil diameter tended to change.
Minority not susceptible
Just why a minority seem unsusceptible to the “expanding hole” illusion is still unclear. It is also not known whether other vertebrate species, or even nonvertebrate animals with camera eyes such as octopuses, might perceive the same illusion as we do.
“Our results show that pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy. Future studies could reveal other types of physiological or bodily changes that can ‘throw light’ onto how illusions work,” concluded Prof Laeng.
Scanning Electron Micrograph of a breast cancer cell. Credit: NIH
Breast cancer and diabetes have long been suspected to have some kind of relationship, but now new research in Nature Cell Biology reveals how breast cancer cells sabotage insulin production to fuel their own cravings for glucose.
Diabetes risk begins to increase two years after a breast cancer diagnosis, and by 10 years post-diagnosis, the risk is 20% higher in breast cancer survivors than in age-matched women without breast cancer.
But these epidemiological linkages are not clear-cut or definitive, and some studies have found no associations at all. In the paper, a research team describe a possible biological mechanism connecting the two diseases, in which breast cancer suppresses the production of insulin, resulting in diabetes, and the impairment of blood sugar control promotes tumour growth.
“No disease is an island because no cell lives alone,” said corresponding study author Shizhen Emily Wang, PhD, professor of pathology at UC San Diego School of Medicine. “In this study, we describe how breast cancer cells impair the function of pancreatic islets to make them produce less insulin than needed, leading to higher blood glucose levels in breast cancer patients compared to females without cancer.”
The researchers name the culprit as extracellular vesicles (EV), which carry DNA, RNA, proteins, fats and other materials between cells, a sort of cargo communication system.
The cancer cells were found to be secreting microRNA-122 into the vesicles. When vesicles reach the pancreas, Prof Wang said, they can enter the islet cells, offload their miR-122 cargo and damage the islets’ critical function in maintaining a normal blood glucose level.
“Cancer cells have a sweet tooth,” Prof Wang said. “They use more glucose than healthy cells in order to fuel tumor growth, and this has been the basis for PET scans in cancer detection. By increasing blood glucose that can be easily used by cancer cells, breast tumors make their own favorite food and, meanwhile, deprive this essential nutrient from normal cells.”
Feeding mice slow-releasing insulin pellets or an SGLT2 inhibitor restored normal control of glucose in the presence of a breast tumour, in turn suppressed the tumour’s growth.
“These findings support a greater need for diabetes screening and prevention among breast cancer patients and survivors,” remarked Prof Wang, noting that a miR-122 inhibitor is currently in clinical trial as a potential treatment for chronic hepatitis C. It has been found to be effective in restoring normal insulin production and suppressing tumour growth in mouse models of breast cancer.
“These miR-122 inhibitors, which happen to be the first miRNA-based drugs to enter clinical trials, might have a new use in breast cancer therapy,” Prof Wang posited.
Judge Edwin Cameron, Inspecting Judge of Correctional Services, writes about the need for healthcare professionals working in prisons should be shifted to the Department of Health.
Our country’s healthcare system is a cumbersome double-deckerbus: on top are those of us who have access of some kind to private healthcare (a high estimate is around 27% of the population). The great majority of necessity rely on public healthcare. But, within public healthcare, there is a further divide, an overlooked layer at the very lowermost – the healthcare afforded to people in prison.
During apartheid, healthcare for those inside prison and in police custody was used as a “tool of manipulation and coercion”. There was medical negligence, poor quality care, false medical and autopsy reports, and warped medical ethics. (Bram Fischer, in his dying days, received no treatment for his crippling cancer).
Some doctors and other medics were complicit in abuses, turning a blind eye to what was happening before them.
The Truth and Reconciliation Commission (TRC) Special Hearings on Prisons showed how basic access to medical treatment was used to punish. Henry Magkothi recounted how difficult it was to gain access on Robben Island to the hospital. “The doctor didn’t come often enough and even then there were so many obstacles they placed in your way.”
Not only did doctors have to have security clearance to work in prisons, but there were split institutional loyalties. Some health professionals were employed by the Department of Health and others by the Department of Prisons (now the Department of Correctional Services — DCS). This led to a dilemma of “dual obligations”, where the lines of authority for healthcare and custodial care were blurred. Health professionals owed loyalty to their patients (the inmates). But they had obligations to, and pressure from, their employers (the prison authorities).
Healthcare must be separated from prison administration
This blighted history led Dr Judith van Heerden, an expert in this area, to recommend to the TRC that prison healthcare “must be separated completely from custodial care”. All healthcare professionals in prisons “should be appointed, paid and responsible to the Department of Health” – and no longer to the prison authorities.
The TRC embraced this sound advice in its recommendations. It suggested that: the Department of Health should assume control over prison healthcare; prison health responsibilities and obligations should be clearly defined with an independent line of authority.
These recommendations accord with international guidelines. The UN Mandela Rules entail a demarcation between healthcare and custodial care; there shall be “full clinical independence”. Healthcare professionals “shall not have any role in the imposition of disciplinary sanctions or other restrictive measures”. And clinical decisions may only be taken by healthcare professionals “and may not be overruled or ignored by non-medical prison staff”.
Experts have underscored the importance of providing health services in prison that are separate from the prison administration. The World Health Organisation and the United Nations Office on Drugs and Crime note that healthcare professionals should act “completely independent of prison authorities” and in “alignment with public health services.”
Furthermore, the Association for the Prevention of Torture advocates for the “integration of the prison health service into the national health service” to guard the “professional and ethical independence of the health staff” and “provide recourse to an independent body in case of conflicts.”
Did democratic South Africa heed this advice? No.
Medical ethicist Professor Solomon Benatar observes that the Department of Health “began to dismantle the District Surgeon Services” and “[i]t became possible for DCS to appoint nurses and other medical staff to deliver healthcare” in our prisons.
This is evident in the plain wording of the Correctional Services Act of 1998. Section 12(1) states that DCS “must provide, within its available resources, adequate health care services” and section 12(2)(b) outlines that medical treatment “must be provided by a correctional medical practitioner, medical practitioners or by a specialist or health care institution or person or institution identified by such correctional medical practitioner”. And according to section 12(3), if an inmate opts to be “visited and examined by a medical practitioner of [their] choice” it is “subject to the permission of the Head of Centre”.
Post-apartheid, healthcare in prisons is still not independent. Benatar slates this “retrogressive step”; “diverting some responsibilities for healthcare away from the Department of Health” and towards DCS, diminishes the “loyalty of some health professionals” as it ranks “allegiance to prison authorities higher than professional responsibility to patients.”
A special duty of care
In his book Health and Health Promotion in Prisons, Professor Michael Ross states that depriving inmates of liberty does not mean we may deprive them of access to healthcare. On the contrary, their deprivation of liberty means we owe them a “special duty of care”. Critically, Ross acknowledges that we provide “good care to bad people because we are professional, and because we, and they, are human” and if bad care is given “the humanity we degrade is also ours, not only theirs”.
Those in prison should have the same quality of healthcare as the public outside. This is the “equivalence of care” principle. It means that you don’t add poor healthcare treatment on top of imprisonment to punish. As I have written before, “prison health affects our health” and “equivalence of care” should be considered a minimum threshold. In light of the higher mortality rates in prisons; government may have to provide higher standards of healthcare in prisons.
We know that injuries and the use of anti-depressants are warning signs of trouble. Many cases of claimed abuse (especially sexual violations, assaults, use of force and torture) are reported to nurses and doctors. Later, investigators, both internal and external, rely on medical reports. Ross emphasises that one must ensure health assessments of inmates are based on medical criteria and inmates ought to trust their healthcare providers and feel safe to report and speak out about abuse.
In addition, nurses, psychologists and other medical practitioners play a role in how prisons are run. For example, they are expected to visit inmates in segregation (sometimes in solitary confinement). The Act provides that segregation “must be discontinued” if medical practitioners determine that “it poses a threat to the health of the inmate”.
Further, independent healthcare can provide another significant layer of independent monitoring over our closed-off prisons.
Two parallel healthcare systems are not advisable. Does DCS have adequate training facilities to ensure training and updates on clinical care for clinicians on its payroll? The Judicial Inspectorate for Correctional Services (JICS), which I head, believes not. DCS clinicians often miss out on training opportunities. Further, DCS’s data systems are standalone – they are not linked to the Department of Health’s facilities (connecting them would ensure continuity of care when inmates are released).
And a heartening thought – why not allocate community service doctors to prisons? This would alleviate costs and skills scarcity.
The state of healthcare in our prisons
Grievously, our prisons are a microcosm of all our country’s social ills. This is true of healthcare, but perhaps it is worse, since, notoriously, prisons are epidemiologic pumps for the spread of infectious viruses and diseases.
The 2020-2021 annual report of the Judicial Inspectorate for Correctional Services paints an agonising picture of the state of prison healthcare.
Inmates do not get regular access to nurses and doctors, clinics in prisons are cramped and there is limited privacy for consultations, correctional officials are not always available to escort inmates to healthcare facilities, medications are not always dispensed on time, some medications have expired, health check-ups and screenings upon admission are not always conducted and medical files are not always updated.
Healthcare professionals in prisons, especially psychologists and social workers, are working with a desperate population. In the single year covered in the report, JICS reported 86 hunger strikes, 66 attempted suicides and 27 suicides. According to DCS’s annual report “suicide is the leading cause of [unnatural] deaths in correctional facilities”.
JICS’s recent quarterly report lists 40 unnatural deaths. We don’t know the cause of most; seemingly healthy inmates died. This requires JICS’s close investigative scrutiny of the post-mortem and medico-legal documents, which are in the hands of DCS and sometimes mysteriously go missing.
Further, there were 113 deaths as a result of natural causes, including pneumonia, cancer, meningitis, septicaemia and asthma. Could some of these deaths have been avoided with early detection, close monitoring and regular access to medical assistance? JICS thinks so.
JICS is also alarmed by the 116 declared state patients in prison; these are individuals whom the courts have found are suffering from mental unwellness challenges. As they wait indefinite periods for a transfer to a psychiatric hospital, they are wrongly housed in correctional facilities. State patients should not be a DCS responsibility. JICS has raised its voice on this: correctional facilities are not conducive for state patients, and correctional officials and fellow inmates are not trained to properly accommodate them.
To end off
While inspecting prisons, I have met passionate nurses and committed doctors. Prisons are tough, dangerous and complicated places. I acknowledge that DCS has worked hard to progress in dealing with Covid, HIV and TB behind bars. But we have to do better.
We need institutional reform. Healthcare professionals working in prisons ought to be independent of DCS. This means shifting all healthcare professionals to the Department of Health and ensuring proper channels of authority and oversight within prisons. In addition, healthcare professionals need specific and ongoing training for the prison environment. We also need more healthcare professionals working in prisons – and they must be accessible, proactive and willing to speak out.
That takes us back to where we started. Our Department of Health must be well-resourced, well-capacitated and well-run – and healthcare professionals must be trained and supported and have job security. And this goes to the heart of whether we have a capable state, strong institutions and a culture of accountability.
Judge Cameron is Inspecting Judge of Correctional Services.
Views expressed are not necessarily those of GroundUp.
Scanning Electron Micrograph image of a human T cell. Credit: NIH/NIAID
While T cells are the body’s warriors against infection, without rest and maintenance T cells can die, leaving their hosts more susceptible to pathogens, researchers reported in the journal Science.
“We may have to change how we teach T cell biology,” said Professor Lieping Chen, who is the senior author of the study.
T cells remain in a quiescent state until pathogens are detected, but the molecular mechanisms of this state were previously unknown.
In the new study, researchers showed that a protein known as CD8a – which is found in a subset of T cells called CD8 cells – is crucial to keeping the cells in this dormant state. When scientists deleted this protein in mice, the protective CD8 cells were unable to enter a quiescent state and died, leaving the host vulnerable to infections.
Further, they identified another protein, PILRa, that provides a biochemical signal to CD8a. By disrupting this protein pair, both “memory” CD8 cells – previously been exposed to pathogens – and naïve cells died because they lacked the ability to stay in a quiescent state.
The researchers hope that understanding why this resting state is crucial to maintenance and survival of T cells can lead to improved immune system function.
Chen noted that as people age they tend to lose both naïve and memory T cells, making older individuals more susceptible to infections. It is possible that the inability of T cells to remain in a quiescent state could lead to people becoming more susceptible to infections and cancer, the authors suggest.