Nerve damage can be an unfortunate side effect from an accident, illness or even certain treatments, like chemotherapy. Fortunately, the peripheral nervous system can heal itself to a certain extent, albeit very slowly. Researchers are still trying to understand this natural healing process in order to improve it. A recent study published in Science Translational Medicine sheds new light on this.
This mouse-based study from the University of Michigan adds to the evidence regarding a specific protein inside of the nerves, called Sarm1, that seems key for regeneration. Previous studies have revealed that when Sarm1 is activated, it sets off the degenerative process in nerves. The thinking has been that for conditions like chemotherapy induced peripheral neuropathy, diabetes, or nerve trauma, blocking Sarm1 would beneficially block the breakdown of nerves.
But what else would blocking Sarm1 effect?
“We know that nerve breakdown after an injury is quite efficient, and the breakdown is what Sarm1 controls. So, there must be a biological reason for this breakdown to be so quick and efficient,” said Ligia B. Schmitd, PhD, of the Department of Cell and Developmental Biology, lead author of the study.
Schmidt is a research fellow in the lab of Roman Giger, PhD, co-senior author with Ashley Kalinski of the University of South Carolina.
Using mice bred to lack Sarm1 and subjecting them to peripheral nerve injury, the team could observe drastic changes to the distal nerve environment, including fewer blood-borne immune cells resulting in reduced nerve inflammation.
“These cells are important because they have to enter the injured nerve to clean up all of the debris,” said Schmitd.
More importantly, their study revealed a critical effect on Schwann cells, which line and support the peripheral nerves.
Normally following an injury, Schwann cells will convert to a repair state in which they express different genes and proteins to migrate and proliferate in order to regrow the axon, the long projecting portion of the neuron.
But without Sarm1, “the Schwann cells are just stuck there,” said Schmitd.
In essence, Sarm1 controls both nerve degeneration and regeneration through its effect on Schwann cells.
The team also noted that a lack of Sarm1 seemed to boost the nerve’s efforts to regrow, but without activating the repair Schwann cells, these efforts were much less efficient.
“For a long time, we’ve thought that simply preventing nerve breakdown would be a good thing. What our study now shows is that this early breakdown also sends powerful signals to Schwann cells and immune cells that are needed for efficient repair, so any future therapy that targets Sarm1 will have to preserve that delicate balance between protection and regeneration,” said Giger, professor in the Department of Cell and Developmental Biology.
Schmitd notes that the study needs to be done in other animal models and with other proteins involved in nerve repair, “but if this proves to be an important mechanism for triggering the repair Schwann cell state, then down the road, fixing this response could help humans regenerate peripheral nerves.”
How food insecurity may biologically intensify neuroblastoma growth, bridging social determinants of health and cancer biology
Image Credit: Justine Ross, Michigan Medicine
Neuroblastoma remains one of the deadliest childhood malignancies, accounting for a disproportionate number of paediatric cancer deaths worldwide.
Despite major therapeutic advances, survival rates remain lower for children from socioeconomically disadvantaged families, a pattern long observed and poorly understood at the biological level.
Extending earlier National Institute of Health’s Children’s Oncology Group findings that linked poverty to poorer survival in paediatric cancers, investigators at University of Michigan Health C.S. Mott Children’s Hospital set out to develop the first experimental model to test how social determinants might influence tumour biology itself.
The team led by Erika Newman, MD, Section Head of Pediatric Surgery and Associate Director for Health Equity at the Rogel Comprehensive Cancer Center developed an innovative murine cancer model that simulated food insecurity by intermittently varying chow access, mirroring the unpredictable nutrition many families experience.
The study, recently published in Communications Biology, used established neuroblastoma validated xenograft models to observe how this stressor affected tumour growth and biologic responses.
The results were striking: the experimental group exposed to food insecurity developed significantly larger and bulkier tumours, accompanied by persistent elevation of stress hormones (corticosterone) and activation of tumour survival pathways.
“Our work builds on decades of clinical evidence linking poverty and food insecurity to poorer cancer outcomes,” said Newman.
“We set out to define the biology behind those disparities, to show how social conditions can become embedded in the body and influence how tumours grow.”
The work provides a translational framework linking social determinants of health to molecular pathways of cancer progression, paving the future for studies that explore how interventions addressing nutrition and stress might improve treatment response.
“This model gives us a scientific bridge between social context and cancer biology,” stated Newman.
“It shows that the environments our patients live in, access to food, stability, and safety are not background conditions. They are part of the biology we must confront if we want equitable outcomes.”
The research arrives at a moment of renewed concern over federal nutrition programs, with potential SNAP benefit interruptions amid government budget negotiations.
Newman emphasises that these findings reinforce the urgency of policies ensuring consistent food access for vulnerable children and families.
Newman stresses that health care must account for the realities in which families live.
She calls for systematic screening of social determinants like food insecurity and economic strain within paediatric and oncology practices, ensuring that medical care addresses both biologic and social drivers of outcome disparities.
Prof Llewellyn Padayachy is pioneering work in non-invasive techniques to assess and measure raised pressure inside the skull.
Paediatric neurosurgeon Professor Llewellyn Padayachy, Head of the Department of Neurosurgery at the University of Pretoria’s (UP) Steve Biko Academic Hospital, is redefining how brain-related diseases are diagnosed and treated, especially in low-resource settings. He’s at the forefront of pioneering work in non-invasive techniques to assess and measure raised pressure inside the skull, known as intracranial pressure (ICP).
As part of his PhD 15 years ago, Prof Padayachy set out to find safer methods for earlier diagnosis of brain tumours in children, a patient group that often presented far too late, with tumours already dangerously large. This trend of delayed diagnosis shifted his research focus to detecting raised ICP, pressure within the skull – a critical marker when diagnosing life-threatening neurological conditions. Traditionally, assessing this pressure involves invasive procedures and highly specialised equipment, resources that are often unavailable in rural or primary care settings.
“Ultimately, this non-invasive system offers a ‘thermometer for the brain’ – a simple yet powerful diagnostic tool that enables earlier treatment, better outcomes and more equitable healthcare access,” Prof Padayachy explains. “This research provides a lifesaving bridge between innovation and accessibility, especially on a continent where neurosurgery is severely under-resourced.”
At the heart of this innovation is the concept of the eye as a window to the brain. Initially using ultrasound imaging to measure the optic nerve sheath – along with technologies like optical coherence tomography (which uses light waves to take cross-sectional images of eye tissue), intraocular tonometry (to measure pressure inside the eye) and retinal scanning – his team has refined methods for non-invasively assessing ICP, without radiation or surgical intervention. This offers a faster, safer and more portable method for diagnosing neurological diseases.
Prof Padayachy’s initial work has since expanded to include adult patients, and now plays a crucial role in identifying a range of central nervous system disorders, including brain tumours, hydrocephalus, infections and intracranial bleeding, conditions where early detection is essential for effective treatment. This non-invasive approach has major benefits for both patients and health systems.
Early detection of conditions like brain tumours and hydrocephalus allows for intervention when symptoms are still mild and treatment is most effective. Detecting tumours earlier is the best modifier of outcome.
This eye-based technique is designed for point-of-care diagnosis. It is a simple, rapid method that can be employed in GP practices, rural clinics or by assistant nurse, with minimal training. By analysing high volumes of data using machine-learning algorithms, a “traffic light” system has been developed to streamline diagnosis: green for normal, orange for uncertain and red for urgent intervention.
The reduced risk and cost of this approach eliminates the dangers of invasive testing and reliance on expensive imaging tools like magnetic resonance imaging (MRI) and computed tomography (CT) scans, which are often unavailable in rural areas.
It can support broader disease management by aiding in the diagnosis of not just tumours but various central nervous system disorders, including bleeds, infection, strokes and traumatic brain injuries. This technology is also being tested in countries like Norway and Germany, and is applicable to astronauts who experience raised intracranial pressure in microgravity.
A solution for Africa, with global impact
According to the World Health Organization (WHO), more than two billion people around the world lack access to safe surgical care, with low- and middle-income countries carrying the greatest burden. Africa faces immense challenges in neurosurgery, such as severe underfunding, a lack of training positions and a high burden of disease.
There is one neurosurgeon per four million people, far below the WHO’s recommendation of one per 200 000. This shortage, compounded by the lack of a central brain tumour registry and limited access to diagnostics, severely impacts patient outcomes. In South Africa alone, limited infrastructure and only a handful of neurosurgical training posts mean that even the brightest medical talent can be lost in the system.
“We have more than 70 applicants for a single registrar training post,” Prof Padayachy says. “This is completely inadequate. This research demonstrates how innovation born out of necessity can help us overcome these hurdles.”
This non-invasive technique isn’t just capable of transforming care in Africa; its application in diagnosing visual impairment due to raised intracranial pressure in astronauts, where a conventional tool like lumbar puncture is difficult to use, highlights its versatility. Ultrasound, which is portable and radiation-free, is the only imaging modality suitable for space. The same “thermometer for the brain” now being tested in orbit began in the clinics of South Africa.
“With the right support, we can create a self-sustaining model for research in Africa, by Africans,” Prof Padayachy says. “We certainly have the talent, and we can develop the tools to lead the world in non-invasive brain diagnostics.”
Oliver Staub, 2, smiles while recovering from two complex spinal cord surgeries at UChicago Medicine Comer Children’s Hospital that reattached his head to his spinal cord. Image credit: University of Chicago Medicine
With monitors quietly beeping and multiple tubes going into his small body, Oliver Staub lay in a hospital bed as his parents tearfully started saying goodbye.
On April 17, an armoured car going 70mph (112kph) slammed into the family’s minivan during their vacation in Mexico. Everyone in the car was injured, but no one more than Oliver.
The impact disconnected the 2-year-old’s head from his spine, resulting in a transection of his spinal cord.
Doctors offered a grim prognosis. They told Oliver’s parents, Laura and Stefan, that their son’s neck was broken, he was a quadriplegic, brain dead and would die in a matter of days.
But following a surreal turn of events – which included support from German soccer star Toni Kroos, viral Instagram posts, and traveling more than 2,000 miles for two risky spinal cord surgeries at the University of Chicago Medicine Comer Children’s Hospital — Oliver is now talking, laughing, smiling, moving his fingers and toes and starting to breathe on his own.
“To see someone survive an injury like this? Nothing like this has ever been reported in neurosurgery or spinal cord injuries,” said Mohamad Bydon, MD, Chair of the Department of Neurological Surgery at UChicago Medicine and health system leader for Neurological Surgery, who performed Oliver’s surgeries in July with a multidisciplinary team of surgeons.
“We didn’t think he’d ever be able to move, and now he’s moving all four limbs,” Bydon said. “This is a unique and special case. It’s beyond our wildest expectations.”
‘We have a reason to fight’
As family members gathered at the Mexico City hospital to say goodbye, something incredible happened: Oliver began to show signs of recovery.
His eyes would follow his parents when they were in the room. Stefan and Laura raised the issue with his doctors, who ultimately determined that their son did, in fact, have brain function. They kept his life-sustaining ventilator on.
“It was at that moment that I thought, ‘We have a reason to fight,’” Laura said. “My son was there.”
When doctors could do nothing more for Oliver, they trained his parents on how to care for him and operate his ventilator. Wearing a neck collar and vest to stabilise his head – which, internally, was not connected to his body – Oliver was moved to his grandparents’ home eight hours away, near Morelia, Mexico.
With help from a daily nurse visit, Oliver survived for two months without moving and once having an incident of cardiac arrest. Bydon finds this astounding, given how unlikely it is that someone with an unstable, transected spine could survive at all, much less under the care of his parents.
“If Oliver’s parents and caretakers had made one wrong move in those two months, it could have resulted in death,” Bydon said.
A journey to Chicago
Stefan and Laura researched treatments for severe spinal cord injuries, hoping to provide a better life for their son. They contacted top spinal cord specialists around the world, including Bydon, whose groundbreaking stem cell therapy research impressed them.
They were repeatedly told that surgery, and the travel involved, would be too risky. But Bydon saw hope, in part because Oliver had survived this long.
“You should never count out a 2-year-old. They can surprise you,” Bydon said. “But it would require a complex multidisciplinary team, which is where the University of Chicago could help.”
The surgery needed to be done as soon and safely as possible, Bydon told them.
But travel to the United States for the surgery would be difficult and expensive. The Staubs received aid from family, friends and charities, but were still far short of what they needed.
Global outreach and support
A friend encouraged them to write to the Toni Kroos Foundation, the soccer player’s charity which helps seriously ill children. Stefan and Laura knew it was a long shot.
Two days later, the phone rang at midnight. It was foundation director Claudia Bartz. She’d seen Oliver’s journey on Instagram and was so moved by his story, she decided the foundation would cover the cost of Oliver’s surgery and transport to Chicago.
“We cried and cried. We couldn’t believe it,” Laura said, adding that they only posted on Instagram to keep their friends and family updated on Oliver. “None of this would have been possible without Toni Kroos.”
Oliver soon became a top-trending news story in Germany and their Instagram account blew up, going from a few hundred followers to more than 100 000. Strangers across the world continue to hold fundraisers and prayer vigils, sending the family encouraging messages and donations for his medical expenses.
“We would gladly trade all of this to go back to our normal life,” said Laura, who still has large scars on her head from the accident. “What I’m seeing here? It’s miraculous. We call it ‘The Oliver Effect.’ This is bigger than us.”
‘Harrowing’ surgery, major recovery
When Oliver arrived at Comer in July via medical jet, Bydon performed the first surgery, an occipital cervical fusion, with a team of UChicago Medicine surgeons.
This surgery for a 2-year-old is risky, not only because of how long it is, but also because a toddler cannot tolerate blood loss.
The surgery involved reconstructing Oliver’s spine, repairing his spinal cord and stabilising the back of his head to his cervical spine using titanium rods and screws.
The second surgery, two days later, stabilised the front of his spinal cord and repaired a spinal cord herniation.
“Those first few days after the surgeries were harrowing,” Bydon said. “His heart stopped at one point, and he had swelling in the brain.”
But about five days later, Oliver was making progress and smiled for the first time since the accident. One month later, he was able to grab his mom’s hand, push someone away and recognise the sensation that he needs to urinate. Most impressively, Bydon said, he can now take breaths on his own.
“We know the spine is communicating with the brain and body again,” Bydon said.
Moving forward with family
Oliver was discharged from Comer Children’s on August 15. The family will permanently move from Germany to Mexico, near Laura’s family, and now have hope for the future.
Oliver will have regular physical therapy and take medications for inflammation. In about six months, he’ll be able to remove his neck brace, Bydon said.
Laura and Stefan plan to return to Comer in spring 2026, when Bydon may be able to use novel stem cell therapy clinical trials to improve Oliver’s physical functions, pending special FDA approval.
Stefan and Laura said they’ll always be grateful to Bydon and UChicago Medicine.
“He didn’t promise us a miracle,” Laura said, “but he delivered one.”
Placebo-controlled trial shows shunt surgery improves walking, balance and safety for older adults with idiopathic normal pressure hydrocephalus
Photo by Kampus Production on Pexels
Idiopathic normal pressure hydrocephalus (iNPH) is a treatable condition caused by a buildup of cerebrospinal fluid in the brain that leads to walking and balance problems, memory decline, and bladder control issues. Researchers report the disorder affects up to 1.5% of people in their late 60s and as many as 1 in 13 over age 86. Left untreated, iNPH can cause falls, loss of independence and progressive disability.
A new international study led by Johns Hopkins University School of Medicine researchers, and published in The New England Journal of Medicine, has provided definitive proof that shunt surgery restores mobility and physical safety in older adults with iNPH. The Placebo-Controlled Effectiveness in iNPH Shunting (PENS) Trial is the first large, double-blind, placebo-controlled study to resolve decades of debate on whether shunts truly help patients.
“Although shunts have been used for 50 years, scepticism persisted because of the placebo effect and the risks of operating in frail, elderly patients,” says Mark Luciano, MD, PhD, principal investigator and director of the Johns Hopkins Hydrocephalus and Cerebral Fluid Center. “This study shows surgery is both effective and has an acceptable safety profile. We’ve proven this treatment works, definitively and safely, in the most rigorous type of study possible.”
The National Institutes of Health–supported trial enrolled 99 patients across 17 centres in the US, Canada, and Sweden. All patients underwent shunt surgery and received a functioning shunt. However, in half, the shunt was initially adjusted to a placebo setting. Neither patients nor their doctors knew which group they were in.
After three months, patients with functioning shunts walked significantly faster than they did before surgery, while the placebo group showed virtually no change. On average, walking speed in the shunt group improved by 0.23 metres per second — more than double the threshold considered by researchers to be a meaningful change in older adults. Eighty percent of patients with a functioning shunt achieved meaningful improvement, compared with just 24% of those in the placebo group.
“When a person walks better and doesn’t fall, everything improves: their independence, their safety and their quality of life,” says Luciano.
Patients in the treatment group also displayed improved balance and reported fewer falls. Forty-six percent of patients in the placebo group reported falling during the trial, compared with just 25% of those who received a functioning shunt. These gains are especially impactful for older adults, as poor mobility and frequent falls are directly tied to loss of independence, increased injury as well as higher mortality risk.
Despite its potential for treatment, iNPH is often overlooked. Researchers report that only about 20% of patients who could benefit from surgery are referred for evaluation because their symptoms are dismissed as normal signs of aging. That said, diagnosis can be simple.
“If there appears to be imbalance that’s increasing, or memory loss that’s increasing, it’s a diagnosis that can be explored with a routine brain scan,” says Luciano. “If the ventricles are enlarged and the symptoms are there, then patients can be referred to specialists who can further evaluate and treat.”
Looking ahead, the PENS Trial will continue to follow participants for 12 months to measure long-term outcomes, including cognition, daily functioning and quality of life. Early findings already suggest gains beyond walking.
“It has always been suspected that cognitive changes take longer to improve and need more detailed testing,” says Luciano. “At the 12-month period, we’ll have more to say not only about cognition, but how much patients are improving in their activities and independence.”
The research team is also working to develop noninvasive diagnostic methods that could replace current spinal fluid drainage trials, making it easier for clinicians to diagnose patients with iNPH and connect them to treatment.
New research shows attention lapses due to sleep deprivation coincide with a flushing of fluid from the brain — a process that normally occurs during sleep.
Anne Trafton | MIT News
Photo by Tim Gouw on Unsplash
Nearly everyone has experienced it: After a night of poor sleep, you don’t feel as alert as you should. Your brain might seem foggy, and your mind drifts off when you should be paying attention.
A new study from MIT reveals what happens inside the brain as these momentary failures of attention occur. The scientists found that during these lapses, a wave of cerebrospinal fluid (CSF) flows out of the brain – a process that typically occurs during sleep and helps to wash away waste products that have built up during the day. This flushing is believed to be necessary for maintaining a healthy, normally functioning brain.
When a person is sleep-deprived, it appears that their body attempts to catch up on this cleansing process by initiating pulses of CSF flow. However, this comes at a cost of dramatically impaired attention.
“If you don’t sleep, the CSF waves start to intrude into wakefulness where normally you wouldn’t see them. However, they come with an attentional tradeoff, where attention fails during the moments that you have this wave of fluid flow,” says Laura Lewis, the Athinoula A. Martinos Associate Professor of Electrical Engineering and Computer Science, a member of MIT’s Institute for Medical Engineering and Science and the Research Laboratory of Electronics, and an associate member of the Picower Institute for Learning and Memory.
Lewis is the senior author of the study, which appears today in Nature Neuroscience. MIT visiting graduate student Zinong Yang is the lead author of the paper.
Flushing the brain
Although sleep is a critical biological process, it’s not known exactly why it is so important. It appears to be essential for maintaining alertness, and it has been well-documented that sleep deprivation leads to impairments of attention and other cognitive functions.
During sleep, the cerebrospinal fluid that cushions the brain helps to remove waste that has built up during the day. In a 2019 study, Lewis and colleagues showed that CSF flow during sleep follows a rhythmic pattern in and out of the brain, and that these flows are linked to changes in brain waves during sleep.
That finding led Lewis to wonder what might happen to CSF flow after sleep deprivation. To explore that question, she and her colleagues recruited 26 volunteers who were tested twice — once following a night of sleep deprivation in the lab, and once when they were well-rested.
In the morning, the researchers monitored several different measures of brain and body function as the participants performed a task that is commonly used to evaluate the effects of sleep deprivation.
During the task, each participant wore an electroencephalogram (EEG) cap that could record brain waves while they were also in a functional magnetic resonance imaging (fMRI) scanner. The researchers used a modified version of fMRI that allowed them to measure not only blood oxygenation in the brain, but also the flow of CSF in and out of the brain. They also measured each subject’s heart rate, breathing rate, and pupil diameter.
The participants performed two attentional tasks while in the fMRI scanner, one visual and one auditory. For the visual task, they had to look at a screen that had a fixed cross. At random intervals, the cross would turn into a square, and the participants were told to press a button whenever they saw this happen. For the auditory task, they would hear a beep instead of seeing a visual transformation.
Sleep-deprived participants performed much worse than well-rested participants on these tasks, as expected. Their response times were slower, and for some of the stimuli, the participants never registered the change at all.
During these momentary lapses of attention, the researchers identified several physiological changes that occurred at the same time. Most significantly, they found a flux of CSF out of the brain just as those lapses occurred. After each lapse, CSF flowed back into the brain.
“The results are suggesting that at the moment that attention fails, this fluid is actually being expelled outward away from the brain. And when attention recovers, it’s drawn back in,” Lewis says.
The researchers hypothesise that when the brain is sleep-deprived, it begins to compensate for the loss of the cleansing that normally occurs during sleep, even though these pulses of CSF flow come with the cost of attention loss.
“One way to think about those events is because your brain is so in need of sleep, it tries its best to enter into a sleep-like state to restore some cognitive functions,” Yang says. “Your brain’s fluid system is trying to restore function by pushing the brain to iterate between high-attention and high-flow states.”
A unified circuit
The researchers also found several other physiological events linked to attentional lapses, including decreases in breathing and heart rate, along with constriction of the pupils. They found that pupil constriction began about 12 seconds before CSF flowed out of the brain, and pupils dilated again after the attentional lapse.
“What’s interesting is it seems like this isn’t just a phenomenon in the brain, it’s also a body-wide event. It suggests that there’s a tight coordination of these systems, where when your attention fails, you might feel it perceptually and psychologically, but it’s also reflecting an event that’s happening throughout the brain and body,” Lewis says.
This close linkage between disparate events may indicate that there is a single circuit that controls both attention and bodily functions such as fluid flow, heart rate, and arousal, according to the researchers.
“These results suggest to us that there’s a unified circuit that’s governing both what we think of as very high-level functions of the brain — our attention, our ability to perceive and respond to the world — and then also really basic fundamental physiological processes like fluid dynamics of the brain, brain-wide blood flow, and blood vessel constriction,” Lewis says.
In this study, the researchers did not explore what circuit might be controlling this switching, but one good candidate, they say, is the noradrenergic system. Recent research has shown that this system, which regulates many cognitive and bodily functions through the neurotransmitter norepinephrine, oscillates during normal sleep.
The research was funded by the National Institutes of Health, a National Defense Science and Engineering Graduate Research Fellowship, a NAWA Fellowship, a McKnight Scholar Award, a Sloan Fellowship, a Pew Biomedical Scholar Award, a One Mind Rising Star Award, and the Simons Collaboration on Plasticity in the Aging Brain.
This story is republished courtesy of MIT News (web.mit.edu/newsoffice/), a popular site that covers news about MIT research, innovation and teaching.
A new international study led by researchers at Karolinska Institutet demonstrates that it is possible to detect subtle changes in the brain and identify early signs of hereditary frontotemporal dementia using advanced brain imaging techniques. The study has recently been published in Molecular Psychiatry.
Frontotemporal dementia, or FTD, is a neurodegenerative disease that often affects people in middle age and is a common cause of dementia before the age of 65. The disease is particularly difficult to diagnose in its early stages, as the earliest symptoms are behavioural changes and may resemble primary psychiatric disease and symptoms later on can resemble conditions such as Alzheimer’s disease and Parkinson’s disease. In about a third of cases, frontotemporal dementia is hereditary, making families with known mutations an important resource for research.
New type of MRI technique
In the current study, researchers from Karolinska Institutet, together with an international research network, examined the brain’s microstructure in over 700 individuals – both carriers of FTD mutations and control subjects. The researchers used a new type of MRI technique that measures how water molecules spread within the grey matter of the brain, where greater diffusion indicates microstructural damage to brain tissue. In this way, the technique can reveal early damage in the cerebral cortex before the brain begins to shrink, known as brain atrophy, or cognitive problems arise.
The results revealed that the new method is more sensitive than the established imaging technique that measures the thickness of the cerebral cortex. Among individuals with a mutation in the C9orf72 gene, the researchers could detect changes in the brain even before any clinical symptoms appeared. For mutations in the MAPT gene, changes were observed at mild symptom stages, whereas for carriers of GRN mutations, alterations emerged only at more advanced stages.
Identifying individuals at risk
“Our findings show that changes in the brain’s microstructure can be detected before visible brain atrophy, and these changes are closely linked to how the disease develops,” explains corresponding author Elena Rodriguez-Vieitez, researcher at the Department of Neurobiology, Care Sciences and Society, Karolinska Institutet.
“This could be valuable for identifying individuals at risk and for evaluating new therapies in clinical trials.”
The researchers also followed the participants over time and showed that a greater spread of water molecules in brain tissue at the start of the study was linked to a faster decline in behaviour and cognitive ability. This was true for all three mutation types.
“Our results suggest that measurements of the brain’s microstructure could become an important tool for identifying individuals at risk of frontotemporal dementia and for monitoring disease progression in clinical trials,” says Caroline Graff, professor at the same department and last author of the study.
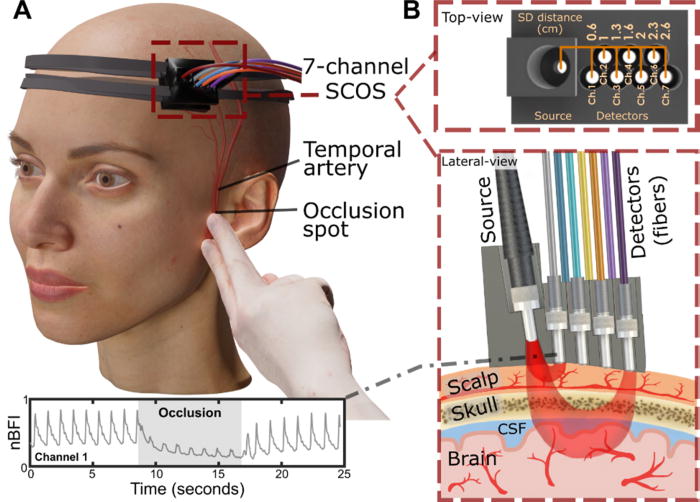
This optical measurement could offer an affordable and scalable way to diagnose stroke, brain injury and other conditions
Experimental arrangement of the SCOS system for measuring cerebral blood dynamics during superficial temporal artery (STA) occlusion. (a) 3D visualization of the SCOS device positioned over the temple region and the occlusion site near the ear bone. (b) Top and lateral views of the device, illustrating different detecting channels for sensing the scalp, skull, and brain layers. Credit: Liu et al., APL Bioengineering, 2025
Measuring blood flow in the brain is critical for responding to a range of neurological problems, including stroke, traumatic brain injury (TBI) and vascular dementia. But existing techniques, including magnetic resonance imaging and computed tomography, are expensive and therefore not widely available.
Researchers from the USC Neurorestoration Center and the California Institute of Technology (Caltech) have built a simple, noninvasive alternative. The device takes a technique currently used in animal studies known as speckle contrast optical spectroscopy (SCOS) and adapts it for potential clinical use in humans. It works by capturing images of scattered laser light with an affordable, high-resolution camera.
“It’s really that simple. Tiny blood cells pass through a laser beam, and the way the light scatters allows us to measure blood flow and volume in the brain,” said Charles Liu, MD, PhD, professor of clinical neurological surgery, urology and surgery at the Keck School of Medicine of USC, director of the USC Neurorestoration Center and co-senior author of the new research.
The device has already been tested with humans in small proof of concept studies demonstrating the tool’s utility for assessing stroke risk and detecting brain injury. In the current study, published in APL Bioengineering, Liu and his team sought to confirm that SCOS is truly measuring blood flow in the brain, rather than in the scalp, which also contains many blood vessels. The question has long plagued researchers who use light-based technology to visualize the brain.
Liu’s team took an innovative approach: By temporarily blocking blood flow to the scalp, they confirmed that SCOS readings were indeed measuring signals from blood vessels in the brain. Readings from 20 participants showed that positioning the detector at least 2.3cm away from the laser source provided the clearest measurement of brain blood flow. The study, funded in part by the National Institutes of Health, the Alfred Mann Foundation and the USC Neurorestoration Center, was just published in the journal APL Bioengineering.
“For the first time in humans, this experimental evidence shows that a laser speckle optical device can probe beyond the scalp layers to access cerebral signals,” said Simon Mahler, PhD, who is now an assistant professor in the Department of Biomedical Engineering at the Stevens Institute of Technology and one of the paper’s coauthors. “This is an important step toward using SCOS to non-invasively measure blood flow in the brain.”
Tracking brain blood flow
For years, researchers measuring brain signals with light-based technology, such as lasers and fibre optics, have used statistical simulations to estimate which signals originate in the brain versus the scalp. The USC Neurorestoration Center team found a direct way to test the difference, thanks to a collaboration between surgeons, engineers and neurologists.
“I perform surgeries to increase blood flow in the brain, and many of these involve temporarily stopping blood flow in the scalp,” said Jonathan Russin, MD, now professor and chief of neurosurgery at the University of Vermont, who continues to collaborate with the USC Neurorestoration Center. “That gave us a simple way to test the technology – by creating a change that affected only the scalp’s circulation while leaving the brain’s blood flow untouched.”
In 20 participants, the researchers temporarily stopped blood flow to the scalp, then collected a series of SCOS readings. By gradually moving the detector further from the head, they captured signals reaching progressively deeper towards the brain. They found that positioning the detector 2.3cm from the head allowed them to measure brain blood flow while minimising interference from the scalp.
The findings confirm the utility of SCOS for non-invasively detecting brain blood flow and provide important guidance for other researchers working with light-based technology, Liu said.
Bringing SCOS to patients
Beyond advancing research, the study helps confirm the clinical potential of SCOS for detecting and responding to stroke, brain injury and dementia. Because all of the team’s research has been done with humans, the tool is poised for rapid translation from the lab to the clinic.
“We look directly at humans in essentially the same way the tool will be applied, so there’s nothing lost in translation,” Liu said. “We are never more than one step away from the problem we’re trying to solve.”
The technique is already being used by some of the team’s collaborators to help diagnose stroke and TBI. Next, the researchers will continue to refine the technology and software, working to improve the resolution of images and the quality of data extracted from readings.
“With the knowledge that we’re now measuring exactly what we intend to measure, we’re also going to expand our testing of this technique with patients in clinical settings,” Liu said.
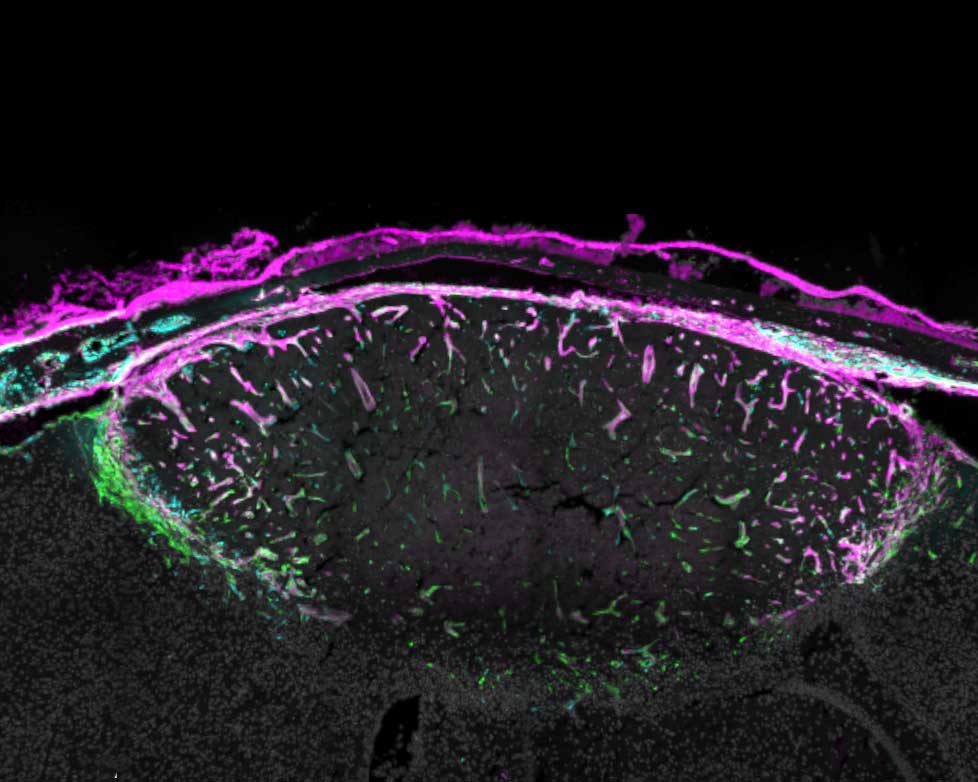
A mouse brain cortex seven days after a stroke that caused injury. Fibroblasts (green) have created collagen (pink) to form a protective scar layer around the injury. All images by Molofsky Lab, UCSF
Healing from any injury involves a delicate balance between scarring and inflammation – two processes that can wreak havoc as well as make repairs.
When the injury is to the brain, the balance is that much more important, yet scientists know almost nothing of how this process works.
Now, a study from UC San Francisco spotlights how a cell type called a fibroblast, that plays a healing role in other parts of the body also performs a similar function in the brain. The discovery is a step toward finding new ways to treat brain injuries, which are the nation’s leading cause of death and disability and for which there aren’t any drugs that can intervene.
Fibroblasts were only identified in the brain in the last decade. They reside mostly in the meninges, a set of protective membranes that surround the brain and spinal cord. Until now, scientists thought they mostly served to maintain the structure of the meninges and its network of blood vessels.
Ari Molofsky, MD, PhD, a professor of laboratory medicine, suspected the fibroblasts might be doing much more than that. He and Tom Arnold, MD, a professor of paediatrics, discovered that when the brain is injured – whether from a blow or a stroke – fibroblasts navigate from the meninges and surround the injured tissue where they create a protective barrier, or scar.
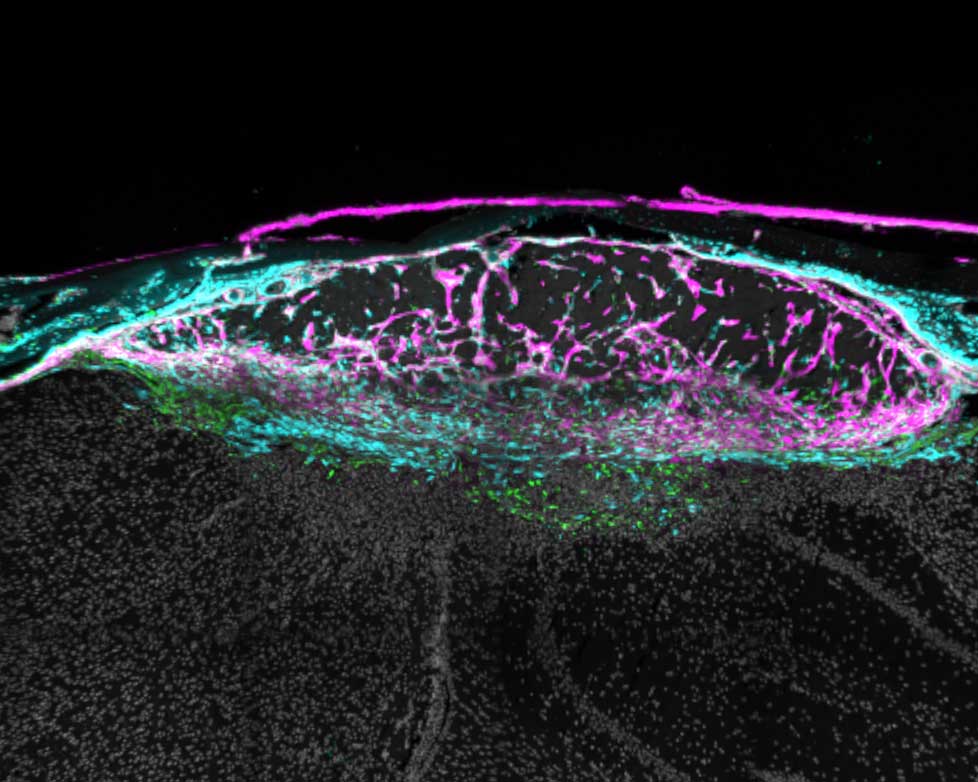
The same injury 14 days after the stroke. The scar now surrounds the whole injury, which is less swollen. Some fibroblasts have returned to their usual location in the meninges. Those that remain have switched roles and are now recruiting immune cells to moderate inflammation.
Then, about a week later, after the scar has formed, the fibroblasts adopt new roles. Some recruit immune cells that are required for healing; others ensure that the immune response doesn’t cause too much inflammation; and still others return to the meninges. Understanding these distinct stages could spur new interventions to help people with serious injuries.
Various views of a mouse brain cortex seven days after a stroke that caused injury. Green dots show fibroblast cells; pink areas show collagen produced by the fibroblasts to create a protective scar layer; and blue shows blood vessels with fibroblasts.
“Our study reveals opportunities to enhance the natural repair process,” said Molofsky, the senior author of the study, which appeared in Nature. “The goal is to give someone who’s experienced a traumatic brain injury or stroke the best outcome possible, based on the stage of healing they’re in.”
Therapies currently in clinical trials for lung and liver fibrosis target a molecule that prompts fibroblasts to create scarring. This suggests that other similar drugs could enhance healing in the early stages of a brain injury.
Molofsky’s study also offers an ideal venue for scientists to learn how fibroblasts are doing their work elsewhere in the body. Being largely devoid of immune cells, the brain offers a much clearer view than other organs like the lungs or liver, where immune cells may be too crowded around fibroblasts to see what they are doing.
“There’s a lot of potential here,” Molofsky said. “These overlooked cells seem adept at solving the common challenge of balancing healing and inflammation.”
The time to carry out diagnostic MRI scans for dementia can be cut to one third of their standard length, according to a new study led by UCL researchers.
The findings, published in Alzheimer’s & Dementia, have been described as a step towards ending ‘the postcode lottery in dementia diagnosis’. Shorter scans would be easier and more comfortable for patients and also enable more people to be scanned at a lower cost. The team behind the study say this could at least double the number of dementia scans able to be done in one day.
Senior author Professor Nick Fox, Director of the UCL Dementia Research Centre at the UCL Queen Square Institute of Neurology, said: “As more treatments that can slow or change the course of dementia are being developed, it’s important to make sure MRI scans are available to everyone. This is because people living with dementia often need an MRI scan as part of their diagnosis before they can access these treatments.
“To help make this possible, our team carried out the first study looking at how new imaging techniques – called parallel imaging – could speed up MRI scans in clinics. Their goal is to move closer to a future where every person with dementia can get a diagnosis through a scan.”
MRI scans often play a key role in an accurate dementia diagnosis, including ruling out other causes of symptoms and assisting in diagnosing the type of dementia. Emerging disease-modifying treatments such as lecanemab and donanemab also require an MRI scan before starting treatment and for safety monitoring during the course of treatment. Reducing the cost of scanning would contribute to lowering the total cost of delivering for such treatments.
The ADMIRA study (Accelerated Magnetic Resonance Imaging for Alzheimer’s disease), part funded by Alzheimer’s Society’s Heather Corrie Impact Fund, aimed to understand the reliability of fast MRI scans compared to standard-of-care clinical scans. The neurologists on the study were joined by co-authors from the UCL Hawkes Institute and the UCL Advanced Research Computing Centre in the faculty of Engineering.
The research team scanned 92 people in an outpatient setting where an MRI brain scan was planned as part of their routine clinical assessment. The accelerated scans were carried out and enhanced to increase the quality of the image using new scanning methods. Three neuroradiologists examined these scans, and weren’t aware if they were looking at fast or standard-of-care scans.
Co-author Professor Geoff Parker (UCL Hawkes Institute and UCL Medical Physics and Biomedical Engineering) said: “Our research has taken advantage of recent breakthroughs in scanner technology. Our task was to work out just how fast we could scan while maintaining image quality good enough for diagnosis.”
The team found that the quicker scans reduced time in the scanner by 63% and they were as reliable as the standard-of-care scans for diagnosis and visual ratings.
First author Dr Miguel Rosa-Grilo (UCL Queen Square Institute of Neurology) said: “We were confident that the new scan would prove non-inferior to the standard scan, given the high image quality – but it was remarkable how well it performed.”
Richard Oakley, Associate Director of Research and Innovation at Alzheimer’s Society, said: “Dementia is the UK’s biggest killer, but one in three people living with the condition haven’t had a diagnosis. An early and accurate diagnosis isn’t just a label, it’s the first step to getting vital care, support and treatment.
“While MRIs aren’t the only way to diagnosis dementia, very few people with concerns about their cognitive health are offered one as part of the diagnosis process, mainly because they are expensive and not widely available. These faster MRIs, which take less than half the time of standard scans, could help end this postcode lottery in dementia diagnosis, cut costs and potentially give more people access to them.
“MRI scans can be an uncomfortable and daunting experience for patients, so anything we can do to make it an easier process is really positive.
“So far, this shortened MRI scan has been tested at one specialist centre with one type of MRI scanner, so more research is needed to make sure this works across different types of scanners and a diverse range of people. We’re hugely encouraged by this progress and eager to see how it continues.”
The team will now build on their early results by making sure the approach works across different types of MRI machines, so it can benefit as many hospitals and clinics as possible.