Researchers at Massachusetts General Hospital have discovered a novel molecular mechanism behind the most common forms of acquired hydrocephalus – which could lead to the first non-surgical treatments for the life-threatening disease. Research in animal models uncovered a pathway through which infection or bleeding in the brain triggers inflammation, causing increased production of cerebrospinal fluid (CSF) by the choroid plexus and lead to swelling of the brain ventricles.
“Finding a nonsurgical treatment for hydrocephalus, given the fact neurosurgery is fraught with tremendous morbidity and complications, has been the holy grail for our field,” says Kristopher Kahle, MD, PhD, a paediatric neurosurgeon at MGH and senior author of the study in the journal Cell. “We’ve identified through a genome-wide analytical approach the mechanism that underlies the swelling of the ventricles which occurs after a brain bleed or brain infection in acquired hydrocephalus. We’re hopeful these findings will pave the way for approval of an anti-inflammatory drug to treat hydrocephalus, which could be a game-changer for populations in the US and around the world that don’t have access to surgery.”
Occurring in about 0.2% of births, acquired hydrocephalus is the most common cause of brain surgery in children, though it can affect people at any age. In underdeveloped regions where bacterial infection is the most prevalent form, hydrocephalus is often deadly for children due to the lack of surgical intervention. Brain surgery, where a shunt is implanted to drain fluid from the brain, is the only known treatment. But about half of all shunts in paediatric patients fail within two years of placement, according to the Hydrocephalus Association, requiring repeat neurosurgical operations and a lifetime of brain surgeries.
Pivotal to the process is the choroid plexus, the brain structure that routinely pumps cerebrospinal fluid into the four ventricles of the brain to keep the organ buoyant and injury-free within the skull. An infection or brain bleed, however, can create a dangerous neuroinflammatory response where the choroid plexus floods the ventricles with cerebral spinal fluid and immune cells from the periphery of the brain in a cytokine storm, swelling the brain ventricles.
“Scientists in the past thought that entirely different mechanisms were involved in hydrocephalus from infection and from haemorrhage in the brain,” explains co-author Bob Carter, MD, PhD, chair of the Department of Neurosurgery at MGH. “Dr Kahle’s lab found that the same pathway was involved in both types and that it can be targeted with immunomodulators like rapamycin, a drug that’s been approved by the US Food and Drug Administration for transplant patients who need to suppress their immune system to prevent organ rejection.”
MGH researchers are continuing to explore how rapamycin and other drugs which quell the inflammation seen in acquired hydrocephalus could be repurposed. “What has me most excited is that this noninvasive therapy could provide a way to help young patients who don’t have access to neurosurgeons or shunts,” says Kahle. “No longer would a diagnosis of hydrocephalus be fatal for these children.”
Scientistshave made an important breakthrough in understanding failures during the progression of inflammatory diseases and in doing so unearthed a potential new therapeutic target. The scientists report in Nature that an enzyme called Fumarate Hydratase is repressed in macrophages. These immune cells are already implicated in a range of diseases including Lupus, arthritis, sepsis and COVID.
Lead author Luke O’Neill, Professor of Biochemistry at Trinity said: “No-one has made a link from Fumarate Hydratase to inflammatory macrophages before and we feel that this process might be targetable to treat debilitating diseases like Lupus, which is a nasty autoimmune disease that damages several parts of the body including the skin, kidneys and joints.”
Joint first-author Christian Peace added: “We have made an important link between Fumarate Hydratase and immune proteins called cytokines that mediate inflammatory diseases. We found that when Fumarate Hydratase is repressed, RNA is released from mitochondria which can bind to key proteins ‘MDA5’ and ‘TLR7’ and trigger the release of cytokines, thereby worsening inflammation. This process could potentially be targeted therapeutically.”
Fumarate Hydratase was shown to be repressed in a model of sepsis, an often-fatal systemic inflammatory condition that can happen during bacterial and viral infections. Similarly, in blood samples from patients with Lupus, Fumarate Hydratase was dramatically decreased.
“Restoring Fumarate Hydratase in these diseases or targeting MDA5 or TLR7 therefore presents an exciting prospect for badly needed new anti-inflammatory therapies,” said Prof O’Neill.
Excitingly, this newly published work is accompanied by another publication by a group led by Professor Christian Frezza, now at the University of Cologne, and Dr Julien Prudent at the MRC Mitochondrial Biology Unit (MBU), who have made similar findings in the context of kidney cancer.
“Because the system can go wrong in certain types of cancer, the scope of any potential therapeutic target could be widened beyond inflammation,” added Prof O’Neill.
A new study details the step-by-step cascade that allows bacteria to break through the brain’s protective layers, the meninges, and cause meningitis, a highly fatal disease. Published inNature, the mouse-based research shows that bacteria exploit nerve cells in the meninges to suppress the immune response and allow the infection to spread into the brain.
“We’ve identified a neuroimmune axis at the protective borders of the brain that is hijacked by bacteria to cause infection – a clever manoeuvre that ensures bacterial survival and leads to widespread disease,” said study senior author Isaac Chiu, associate professor of immunology in the Blavatnik Institute at Harvard Medical School.
The study identifies two central players in this molecular chain of events that leads to infection – a chemical released by nerve cells and an immune cell receptor blocked by the chemical. The study experiments show that blocking either one can interrupt the cascade and thwart the bacterial invasion.
If replicated through further research, the new findings could lead to much-needed therapies for this hard-to-treat condition that often leaves those who survive with serious neurologic damage.
Such treatments would target the critical early steps of infection before bacteria can spread deep into the brain.
“The meninges are the final tissue barrier before pathogens enter the brain, so we have to focus our treatment efforts on what happens at this border tissue,” said study first author Felipe Pinho-Ribeiro, a former post-doctoral researcher in the Chiu lab, now an assistant professor at Washington University in St. Louis.
A recalcitrant disease in need of new treatments
More than 1.2 million cases of bacterial meningitis occur globally each year, according to the US Centers for Disease Control and Prevention. Untreated, it kills seven out of 10 people who contract it. Treatment can reduce mortality to three in 10. However, among those who survive, one in five experience serious consequences, including hearing or vision loss, seizures, chronic headache, and other neurological problems.
The meninges are three membranes that lie atop one another, wrapping the brain and spinal cord to shield the central nervous system from injury, damage, and infection. The dura mater, outermost of the three layers, contains pain neurons that detect signals. Such signals could come in the form of mechanical pressure: blunt force from impact or toxins that make their way into the central nervous system through the bloodstream. The researchers focused on the dura mater as the site of initial interaction between bacteria and protective border tissue.
Recent research has revealed that the dura mater also harbours a wealth of immune cells, and that immune cells and nerve cells reside right next to each other – a clue that captured Chiu’s and Pinho-Ribeiro’s attention.
“When it comes to meningitis, most of the research so far has focused on analysing brain responses, but responses in the meninges – the barrier tissue where infection begins – have remained understudied,” Ribeiro said.
What exactly happens in the meninges when bacteria invade? How do they interact with the immune cells residing there? These questions remain poorly understood, the researchers said.
How bacteria break through the brain’s protective layers
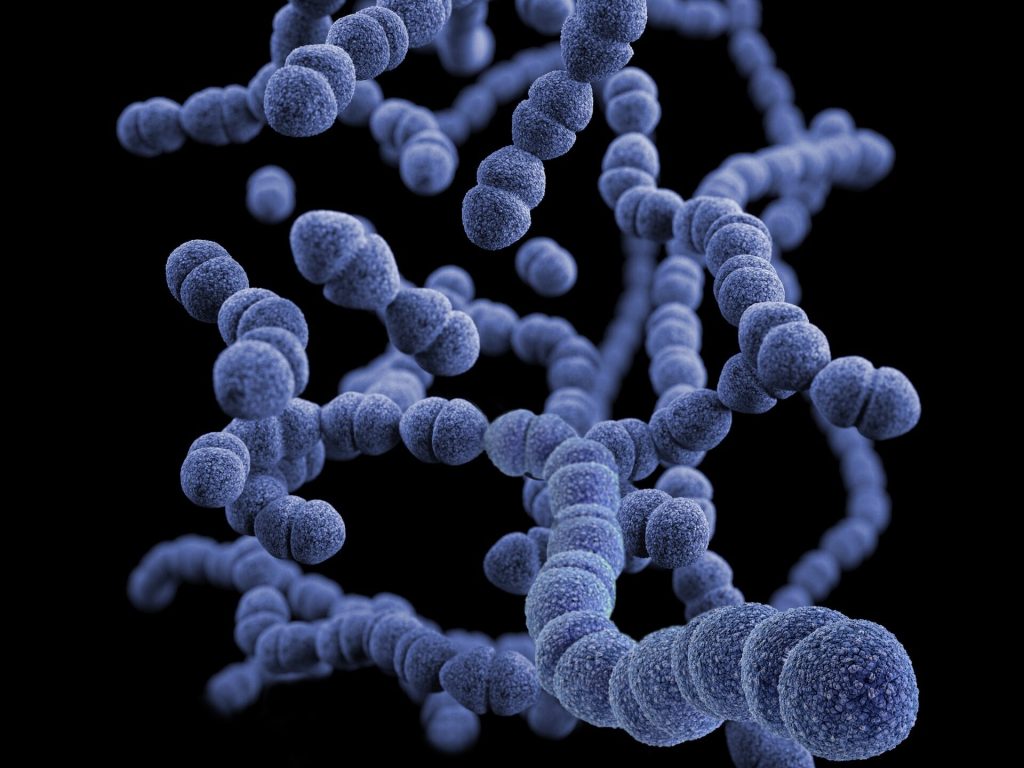
In this particular study, the researchers focused on two pathogens – Streptococcus pneumoniae and Streptococcus agalactiae, leading causes of bacterial meningitis in humans. In a series of experiments, the team found that when bacteria reach the meninges, the pathogens trigger a chain of events that culminates in disseminated infection.
First, researchers found that bacteria release a toxin that activates pain neurons in the meninges. The activation of pain neurons by bacterial toxins, the researchers noted, could explain the severe, intense headache that is a hallmark of meningitis. Next, the activated neurons release a signalling chemical called CGRP. CGRP attaches to an immune-cell receptor called RAMP1. RAMP1 is particularly abundant on the surface of immune cells called macrophages.
Once the chemical engages the receptor, the immune cell is effectively disabled. Under normal conditions, as soon as macrophages detect the presence of bacteria, they spring into action to attack, destroy, and engulf them. Macrophages also send distress signals to other immune cells to provide a second line of defence. The team’s experiments showed that when CGRP gets released and attaches to the RAMP1 receptor on macrophages, it prevented these immune cells from recruiting help from fellow immune cells. As a result, the bacteria proliferated and caused widespread infection.
To confirm that the bacterially induced activation of pain neurons was the critical first step in disabling the brain’s defences, the researchers checked what would happen to infected mice lacking pain neurons.
Mice without pain neurons developed less severe brain infections when infected with two types of bacteria known to cause meningitis. The meninges of these mice, the experiments showed, had high levels of immune cells to combat the bacteria. By contrast, the meninges of mice with intact pain neurons showed meagre immune responses and far fewer activated immune cells, demonstrating that neurons get hijacked by bacteria to subvert immune protection.
To confirm that CGRP was, indeed, the activating signal, researchers compared the levels of CGRP in meningeal tissue from infected mice with intact pain neurons and meningeal tissue from mice lacking pain neurons. The brain cells of mice lacking pain neurons had barely detectable levels of CGRP and few signs of bacterial presence. By contrast, meningeal cells of infected mice with intact pain neurons showed markedly elevated levels of both CGRP and more bacteria.
In another experiment, the researchers used a chemical to block the RAMP1 receptor, preventing it from communicating with CGRP, the chemical released by activated pain neurons. The RAMP1 blocker worked both as preventive treatment before infection and as a treatment once infection had occurred.
Mice pretreated with RAMP1 blockers showed reduced bacterial presence in the meninges. Likewise, mice that received RAMP1 blockers several hours after infection and regularly thereafter had milder symptoms and were more capable of clearing bacteria, compared with untreated animals.
A path to new treatments
The experiments suggest drugs that block either CGRP or RAMP1 could allow immune cells to do their job properly and increase the brain’s border defenses.
Compounds that block CGRP and RAMP1 are found in widely used drugs to treat migraine, a condition believed to originate in the top meningeal layer, the dura mater. Could these compounds become the basis for new medicines to treat meningitis? It’s a question the researchers say merits further investigation.
One line of future research could examine whether CGRP and RAMP1 blockers could be used in conjunction with antibiotics to treat meningitis and augment protection.
“Anything we find that could impact treatment of meningitis during the earliest stages of infection before the disease escalates and spreads could be helpful either to decrease mortality or minimize the subsequent damage,” Pinho-Ribeiro said.
More broadly, the direct physical contact between immune cells and nerve cells in the meninges offers tantalizing new avenues for research.
“There has to be an evolutionary reason why macrophages and pain neurons reside so closely together,” Chiu said. “With our study, we’ve gleaned what happens in the setting of bacterial infection, but beyond that, how do they interact during viral infection, in the presence of tumour cells, or the setting of brain injury? These are all important and fascinating future questions.”
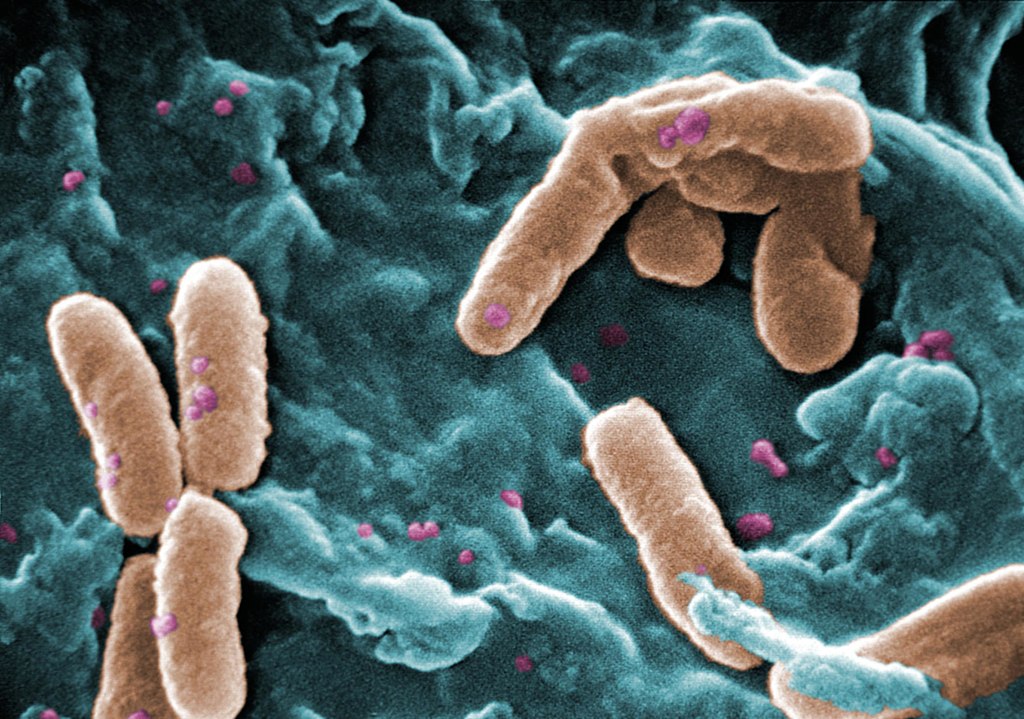
Scanning Electron Micrograph of Pseudomonas aeruginosa. Credit: CDC/Janice Carr
Pseudomonas aeruginosa bacteria are a common menace in hospital wards, causing life-threatening infections, and are often resistant to antibiotics. Researchers have discovered a mechanism that likely contributes to the severity of P. aeruginosa infections, which could also be a target for future treatments. The results were recently appeared in the journal EMBO Reports.
Many bacterial species use sugar-binding molecules called lectins to attach to and invade host cells. Lectins can also influence the immune response to bacterial infections. However, these functions have hardly been researched so far. A research consortium led by Prof Dr Winfried Römer at the University of Freiburg and Prof Dr Christopher G. Mueller at the CNRS/University of Strasbourg has investigated the effect of the lectin LecB from P. aeruginosa on the immune system. It found that isolated LecB can render immune cells ineffective: The cells are then no longer able to migrate through the body and trigger an immune response. The administration of a substance directed against LecB prevented this effect and led to the immune cells being able to move unhindered again.
LecB blockades immune cells
As soon as they perceive an infection, cells of the innate immune system migrate to a nearby lymph node, where they activate T and B cells, triggering a targeted immune response. LecB, according to the current study, prevents this migration. “We assume that LecB not only acts on the immune cells themselves in this process, but also has an unexpected effect on the cells lining the inside of the blood and lymph vessels,” Römer explains. “When LecB binds to these cells, it triggers extensive changes in them.” Indeed, the researchers observed that important structural molecules were relocated to the interior of the cells and degraded. At the same time, the cell skeleton became more rigid. “The cell layer thus becomes an impenetrable barrier for the immune cells,” Römer said.
An effective agent against LecB
Can this effect be prevented? To find out, the researchers tested a specific LecB inhibitor that resembles the sugar building blocks to which LecB otherwise binds. “The inhibitor prevented the changes in the cells, and T-cell activation was possible again,” Mueller said. The inhibitor was developed by Prof Dr Alexander Titz, who conducts research at the Helmholtz Institute for Pharmaceutical Research Saarland and Saarland University.
Further studies are needed to determine how clinically relevant the inhibition of the immune system by LecB is to the spread of P. aeruginosa infection and whether the LecB inhibitor has potential for therapeutic application. “The current results provide further evidence that lectins are a useful target for the development of new therapies, especially for antibiotic-resistant pathogens such as P. aeruginosa,” the authors conclude.
A disease is defined as ’rare’ when it affects fewer than 1 in 2000 people,1 and there are currently more than 7000 known rare diseases (lysosomal storage diseases), affecting more than 300 million people worldwide.1-2 Most (70–80%) lysosomal storage diseases are genetic and inherited, while some may be acquired, and 70% are exclusively paediatric in onset.2
Patients with lysosomal storage diseases present unique challenges to healthcare professionals (HCPs), including diagnostic delays and a lack of information, expertise, and treatment options for many lysosomal storage diseases. Appropriate referrals to specialists, timely diagnosis and treatment, coordinated cross-functional care, and assisting patients in obtaining the proper support are vital roles for HCPs in enhancing quality of life for lysosomal storage disease patients and their families.3,4
Monique Nel, Medical Advisor – Rare Diseases at Sanofi, says: “We understand that HCPs may face difficulties when it comes to the diagnosis of a lysosomal storage disease, and that a coordinated approach to diagnosis and care for people living with lysosomal storage diseases is needed. Lysosomal storage diseases deserve the same amount of time, resources and dedication to finding effective treatments and therapies as any other condition. This is a mission that Sanofi strives to uphold every day, to help HCPs to improve diagnosis, especially as we are starting to see more patients diagnosed with lysosomal storage diseases in both the public and private sectors.”
“Sanofi is focused on education around innovative treatment and research efforts that improve real-world outcomes, investing in education and research to better manage and understand these conditions, and identifying areas requiring more attention,” says Nel.
In the 10 years of its existence, patient advocacy group Rare Diseases SA has made great strides in advocacy for lysosomal storage disease patients. Founder and CEO, Kelly du Plessis, says: “We need to acknowledge that local doctors and healthcare practitioners may have limited knowledge and experience of lysosomal storage diseases. What we would like to see is that they are upskilled on the following three aspects: knowing that lysosomal storage diseases exist, knowing the impact that these have on the patient, and knowing where to refer a patient who they think may have a rare condition. If we can tick these three boxes, great strides will have been made for the diagnostic odyssey that patients with lysosomal storage diseases go through.”
Says du Plessis: “Most importantly, we need a lysosomal storage disease policy to be recognised and enforced in SA, and we need National Treasury to assign a budget to treat these patients so that once an official diagnosis is made, they can receive immediate care. There is also a need for mechanisms to escalate product registration where there are no existing products or alternatives available for lysosomal storage disease patients.”
Partnerships with various stakeholders are paramount in terms of bringing innovative medicines and access to treatment to lysosomal storage disease patients. Says Nel: “For more than 40 years, Sanofi has been a pioneer in science and innovation, rallying its people and resources to help improve the lives of those living with lysosomal storage diseases. Through its commitment to faster diagnoses, innovative treatments, sustainable access and integrated support along the patient journey, Sanofi strives to enable more fulfilling futures.”
Sanofi also has a Rare Humanitarian Programme, which has been running for 32 years and provides humanitarian support to people living with lysosomal storage diseases.Says Nel: “This isan integral part of Sanofi’s mission to develop sustainable healthcare systems, increase access, and improve standards of care for lysosomal storage diseases worldwide. Over 1,000 people in over 70 countries are currently receiving access to free therapy.6
“By building meaningful connections with all stakeholders through various platforms, we continuously strive to transform the practice of medicine, sharing experiences and breaking down barriers,” says Nel.
A useful resource for HCPs and patients is the list of lysosomal storage diseases maintained by the Genetic and Rare Diseases Information Center (GARD) of the US National Institutes of Health.7
2. Nguengang Wakap S, Lambert DM, Olry A, et al. Estimating cumulative point prevalence of rare diseases: analysis of the Orphanet database. Eur J Hum Genet 2020;28:165–173.
4. Dudding-Byth T. A powerful team: the family physician advocating for patients with a rare disease. Aust Fam Physician. 2015 Sep;44(9):634. http://www.ncbi.nlm.nih.gov/pubmed/26488040. NIH.
Analysing an infant’s genome has allowed scientists to find a new way genetics influences the body’s antiviral response by studying a life-threatening disease caused by a common virus: herpes simplex virus 1 (HSV-1). The findings, published in Science Immunology, hold potential as a genetic marker doctors could use to gauge a child’s risk of herpes encephalitis, although such mutations are generally very rare in the population.
The researchers analysed genetic data from a patient with immunodeficiency and hospitalised at nine months old with herpes encephalitis, a rare but life-threatening brain inflammation after HSV-1 infection. They identified novel mutations in the gene GTF3A, and found that these mutations impair the innate immune response.
Many people are infected in childhood with the HSV-1 virus but the vast majority don’t suffer from encephalitis. The most common symptom of HSV-1 is oral cold sores, but many people show no signs at all. HSV-1 is more threatening to children and adults who are immunodeficient, whose immune system cannot control the virus well.
“Genetic and mechanistic analyses of uncommon viral diseases like herpes encephalitis are quite rare. In fact, the causes underlying severe herpes encephalitis are often unknown,” says Michaela Gack, PhD, FRIC’s scientific director. “This information provides us with invaluable insight into the fundamental molecular processes that govern our immune response and opens up opportunities for future research on severe disease outcomes.”
The Ghent research team led by Filomeen Haerynck, MD, PhD, reached out to Dr Gack’s team after finding the mutations in the gene. Dr Gack’s lab studies interactions between the human immune system and viruses on a molecular level.
The GTF3A mutations shape how cells respond to viral activity through the genetic makeup of a protein called TFIIIA. TFIIIA plays a role in helping a human enzyme produce certain types of RNA that can determine specific functions inside cells. Some RNAs can elicit an anti-herpes viral immune response.
Dr Gack’s team tested cells that have the mutations, and found that because of defects in certain immunostimulatory RNAs, the cells were more susceptible to HSV-1 infection and lost the ability to control the HSV-1 virus.
The affected gene is part of the body’s defence system that produces interferons to combat viruses. Interferons are crucial to the human immune response and for suppressing virus infection and spread.
This new genetic pathway could be helpful in understanding the immune response to other viruses, like Epstein-Barr virus, a common virus linked to mononucleosis and associated with certain types of cancer and multiple sclerosis.
“Understanding the molecular processes underlying antiviral responses is key to treating or possibly preventing severe viral infections that change patients’ and families’ lives,” Dr Gack said. “Our findings on critical immune defence proteins may translate into new therapies in the future.”
In patients with Huntington’s disease, neurons in a part of the brain called the striatum are some of the worst affected. Degeneration of these neurons contributes to patients’ loss of motor control, which is one of the major hallmarks of the disease.
Neuroscientists at MIT have now shown that two distinct cell populations in the striatum are affected differently by Huntington’s disease. Reporting their results in Nature Communication, they believe that neurodegeneration of one of these populations leads to motor impairments, while damage to the other population, located in structures called striosomes, may explain the mood disorders that are often see in the early stages of the disease.
“As many as 10 years ahead of the motor diagnosis, Huntington’s patients can experience mood disorders, and one possibility is that the striosomes might be involved in these,” says Ann Graybiel, an MIT Institute Professor and one of the senior authors of the study.
Using single-cell RNA sequencing to analyse the genes expressed in mouse models of Huntington’s disease and postmortem brain samples from Huntington’s patients, the researchers found that cells of the striosomes and another structure, the matrix, begin to lose their distinguishing features as the disease progresses. The researchers hope that their mapping of the striatum and how it is affected by Huntington’s could help lead to new treatments that target specific cells within the brain.
This kind of analysis could also shed light on other brain disorders that affect the striatum, such as Parkinson’s disease and autism spectrum disorder, the researchers say.
Neuron vulnerability
Huntington’s disease leads to degeneration of brain structures called the basal ganglia, which are responsible for control of movement and also play roles in other behaviors, as well as emotions. For many years, Graybiel has been studying the striatum, a part of the basal ganglia that is involved in making decisions that require evaluating the outcomes of a particular action.
Many years ago, Graybiel discovered that the striatum is divided into striosomes, which are clusters of neurons, and the matrix, which surrounds the striosomes. She has also shown that striosomes are necessary for making decisions that require an anxiety-provoking cost-benefit analysis.
In a 2007 study, Richard Faull of the University of Auckland discovered that in postmortem brain tissue from Huntington’s patients, the striosomes showed a great deal of degeneration. Faull also found that while those patients were alive, many of them had shown signs of mood disorders such as depression before their motor symptoms developed.
To further explore the connections between the striatum and the mood and motor effects of Huntington’s, Graybiel teamed up with Kellis and Heiman to study the gene expression patterns of striosomal and matrix cells. To do that, the researchers used single-cell RNA sequencing to analyze human brain samples and brain tissue from two mouse models of Huntington’s disease.
Within the striatum, neurons can be classified as either D1 or D2 neurons. D1 neurons are involved in the “go” pathway, which initiates an action, and D2 neurons are part of the “no-go” pathway, which suppresses an action. D1 and D2 neurons can both be found within either the striosomes and the matrix.
The analysis of RNA expression in each of these types of cells revealed that striosomal neurons are harder hit by Huntington’s than matrix neurons. Furthermore, within the striosomes, D2 neurons are more vulnerable than D1.
The researchers also found that these four major cell types begin to lose their identifying molecular identities and become more difficult to distinguish from one another in Huntington’s disease. “Overall, the distinction between striosomes and matrix becomes really blurry,” Graybiel says.
Striosomal disorders
The findings suggest that damage to the striosomes, which are known to be involved in regulating mood, may be responsible for the mood disorders that strike Huntington’s patients in the early stages of the disease. Later on, degeneration of the matrix neurons likely contributes to the decline of motor function, the researchers say.
In future work, the researchers hope to explore how degeneration or abnormal gene expression in the striosomes may contribute to other brain disorders.
Previous research has shown that overactivity of striosomes can lead to the development of repetitive behaviors such as those seen in autism, obsessive compulsive disorder, and Tourette’s syndrome. In this study, at least one of the genes that the researchers discovered was overexpressed in the striosomes of Huntington’s brains is also linked to autism.
Additionally, many striosome neurons project to the part of the brain that is most affected by Parkinson’s disease (the substantia nigra, which produces most of the brain’s dopamine).
“There are many, many disorders that probably involve the striatum, and now, partly through transcriptomics, we’re working to understand how all of this could fit together,” Graybiel says.
A new approach for treating systemic lupus erythematosus (SLE) could lie in targeting iron metabolism in immune system cells. Researchers found that blocking an iron uptake receptor reduces disease pathology and promotes the activity of anti-inflammatory regulatory T cells in a mouse model of SLE. The findings were published in the journal Science Immunology.
Treatments for lupus aim to control symptoms, reduce immune system attack of tissues, and protect organs from damage. Only one targeted biologic agent has been approved for treating SLE, belimumab in 2011.
“It has been a real challenge to come up with new therapies for lupus,” said Jeffrey Rathmell, PhD, Vanderbilt University professor. “The patient population and the disease are heterogeneous, which makes it difficult to design and conduct clinical trials.”
Rathmell’s group has had a long-standing interest in lupus as part of a broader effort to understand mechanisms of autoimmunity.
When postdoctoral fellow Kelsey Voss, PhD, began studying T cell metabolism in lupus, she noticed that iron appeared to be a “common denominator in many of the problems in T cells,” she said. She was also intrigued by the finding that T cells from patients with lupus have high iron levels, even though patients are often anaemic.
“It was not clear why the T cells were high in iron, or what that meant,” said Voss.
To explore T cell iron metabolism in lupus, Voss and Rathmell drew on the expertise of other investigators at VUMC.
First, Voss used a CRISPR genome editing screen to evaluate iron-handling genes in T cells. She identified the transferrin receptor, which imports iron into cells, as critical for inflammatory T cells and inhibitory for anti-inflammatory regulatory T cells.
The researchers found that the transferrin receptor was more highly expressed on T cells from SLE-prone mice and T cells from patients with SLE, which caused the cells to accumulate too much iron.
“We see a lot of complications coming from that – the mitochondria don’t function properly, and other signalling pathways are altered,” Voss said.
An antibody that blocks the transferrin receptor reduced intracellular iron levels, inhibited inflammatory T cell activity, and enhanced regulatory T cell activity. Treatment of SLE-prone mice with the antibody reduced kidney and liver pathology and increased production of the anti-inflammatory factor, IL-10.
“It was really surprising and exciting to find different effects of the transferrin receptor in different types of T cells,” Voss said. “If you’re trying to target an autoimmune disease by affecting T cell function, you want to inhibit inflammatory T cells but not harm regulatory T cells. That’s exactly what targeting the transferrin receptor did.”
In T cells from patients with lupus, expression of the transferrin receptor correlated with disease severity, and blocking the receptor in vitro enhanced production of IL-10.
Since the transferrin receptor mediates iron uptake in many cell types, the researchers want to develop transferrin receptor antibodies that bind specifically to T cells, to minimise off-target effects. They are also interested in studying the details of their unexpected discovery that blocking the transferrin receptor enhances regulatory T cell activity.
Scanning Electron Micrograph image of a human T cell. Credit: NIH/NIAID
Researchers from the University of Queensland have identified a pathway in cells that could be used to reprogram the body’s immune system to fight back against both chronic inflammatory and infectious diseases such as E. Coli.
Reporting their findings in the open-access journal PNAS, Dr Kaustav Das Gupta and Professor Matt Sweet found that a glucose-derived molecule in immune cells can both stop bacteria growing and dampen inflammatory responses.
According to Dr Das Gupta, the discovery is a critical step towards future therapeutics that train immune cells.
“The effects of this molecule called ribulose-5-phosphate on bacteria are striking – it can cooperate with other immune factors to stop disease-causing strains of the E. coli bacteria from growing,” Dr Das Gupta said.
“It also reprograms the immune system to switch off destructive inflammation, which contributes to both life-threatening infectious diseases such as sepsis as well as chronic inflammatory diseases like respiratory diseases, chronic liver disease, inflammatory bowel disease, rheumatoid arthritis, heart disease, stroke, diabetes and dementia.”
The research was carried out on a strain of E. coli bacteria, responsible for 80% of urinary tract infections and also a common cause of sepsis. Pre-clinical trials confirmed the role of this pathway in controlling bacterial infections.
Professor Sweet said that human cells were also used to demonstrate that ribulose-5-phosphate reduces the production of molecules that drive chronic inflammatory diseases.
“Host-directed therapies which train our immune systems to fight infections, will become increasingly important as more types of bacteria become resistant to known antibiotics,” Professor Sweet said.
“A bonus is that this strategy also switches off destructive inflammation, which gives it the potential to combat chronic disease.
“By boosting the immune pathway that generates ribulose-5-phosphate, we may be able to give the body the power to fight back against inflammatory and infectious diseases – not one, but two of the major global challenges for human health.”
Many current anti-inflammatory therapies target proteins on the outside of cells but because this pathway occurs inside cells, the researchers devised a new approach to target the pathway using mRNA technology.
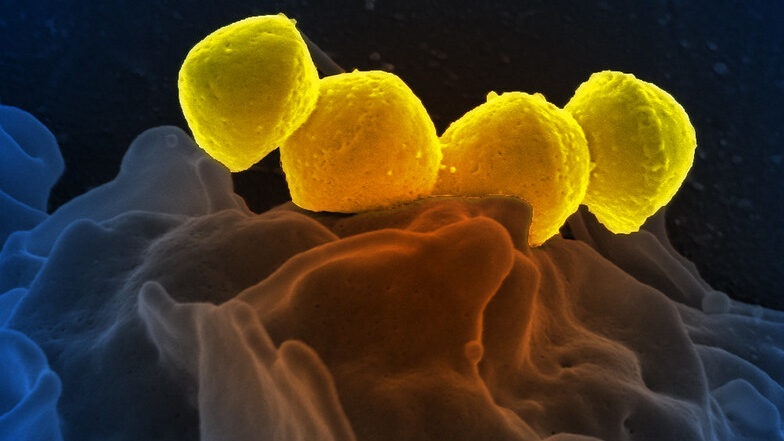
Streptococcus pyogenese bound to a human neutrophil.
Credit: National Institute of Allergy and Infectious Diseases, National Institutes of Health
Griffith University researchers have unlocked one of the secrets as to why some forms of Streptococcus Group A (Strep A) are associated with severe invasive infection. The results, published in mBio, suggest that a toxin it secretes not only damages cells but helps Strep A resist host defence.
Around the world, invasive Strep A diseases are responsible for more than 163 000 deaths annually and a recent increase in cases of invasive Strep A disease has been observed internationally.
For the past 10 years, Institute for Glycomics Associate Professor Manisha Pandey and Professor Michael Good have been researching the pathways in which Strep A can spread through the body.
“The findings from this study will have far-reaching implications as Strep A is responsible for a significant number of invasive and non-invasive infections which cause significant morbidity and mortality globally,” Associate Professor Pandey said.
“The reason for this is that invasive organisms express significantly more of the toxin, streptolysin O (SLO), which was the main focus of this study.
“SLO exerts potent cell and tissue destructive activity and promotes Strep A resistance to clearance by white cells in the body which is the critical first element of host defence against invasive Strep A infection.”
Professor Good said: “We found SLO alters interactions with host cell populations and increases Strep A viability at sites in the body such as the blood and spleen, and that its absence results in significantly less virulence.”
“Essentially, the less SLO present, the less severe the case of Strep A.”
SLO is secreted by nearly all Strep A isolates, but those that secrete the most SLO are the most virulent.
This work underscores the importance of SLO in Strep A virulence while highlighting the complex nature of Strep A pathogenesis.
This improved insight into host-pathogen interactions will enable a better understanding of host immune evasion mechanisms and inform streptococcal vaccine development programs.
Dr Pandey said a key finding was the presence of SLO in invasive organisms did not impair the ability of the Strep A vaccine candidate developed by Griffith University’s Institute for Glycomics and which is now in a clinical trial.
The Strep A virulence study was part of a PhD project undertaken by Dr Emma Langshaw.