Study shows traditional Chinese practice comparable to brisk walking and some medication trials at lowering BP
Pexels Photo by Thirdman
A traditional Chinese mind-body practice that combines slow, structured movement, deep breathing and meditative focus lowered blood pressure as effectively as brisk walking in a large randomised clinical trial published in JACC, the flagship journal of the American College of Cardiology. Blood pressure reductions were seen after three months and sustained for one year.
High blood pressure is one of the leading preventable risk factors for heart disease. Clinical guidelines recommend regular physical activity, yet long-term adherence to exercise programmes is challenging for many people, particularly when routines require equipment, dedicated space, gym memberships or ongoing supervision.
Baduanjin is a widely practised, standardised eight-movement sequence that integrates aerobic, isometric, flexibility and mind–body components. Practised for centuries and commonly performed in community settings across China, the routine typically takes 10–15 minutes and requires no equipment and only minimal initial instruction, allowing it to be performed in a wide range of settings. Because it is low- to moderate-intensity, it is considered safe and accessible for many adults.
“Given its simplicity, safety and ease at which one can maintain long-term adherence, baduanjin can be implemented as an effective, accessible and scalable lifestyle intervention for individuals trying to reduce their blood pressure,” said Jing Li, MD, PhD, senior author of the study and Director, Department of Preventive Medicine, National Center for Cardiovascular Diseases in Beijing, China.
In the first large, multicentre randomised trial to look at the impact of baduanjin on blood pressure, researchers followed 216 participants across seven communities to determine changes in 24-hour systolic blood pressure from baseline to 12 and 52 weeks. Participants were 40 years old or older and had a systolic blood pressure of 130-139mmHg, which according to the ACC/AHA High Blood Pressure Guideline is considered stage 1 hypertension. They were randomly assigned to one of three arms: baduanjin, self-directed exercise alone, or brisk walking for the 52-week intervention.
Compared to self-directed exercise, practicing baduanjin five days a week reduced 24-hour systolic blood pressure approximately 3mmHg and office systolic blood pressure by 5mmHg at both three months and one year, which is comparable to reductions seen with some first-line medications. Baduanjin showed comparable results and safety profile to brisk walking at one year.
Notably, the benefits were sustained even without ongoing monitoring, a key challenge for many lifestyle interventions that struggle to maintain long-term adherence outside structured programs.
“Baduanjin has been practised in China for over 800 years, and this study demonstrates how ancient, accessible, low-cost approaches can be validated through high-quality randomised research,” said Harlan M. Krumholz, MD, FACC, Editor-in-Chief of JACC and the Harold H. Hines, Jr Professor at the Yale School of Medicine. “The blood pressure effect size is similar to that seen in landmark drug trials, but achieved without medication, cost or side effects. This makes it highly scalable for community-based prevention, including in resource-limited settings.”
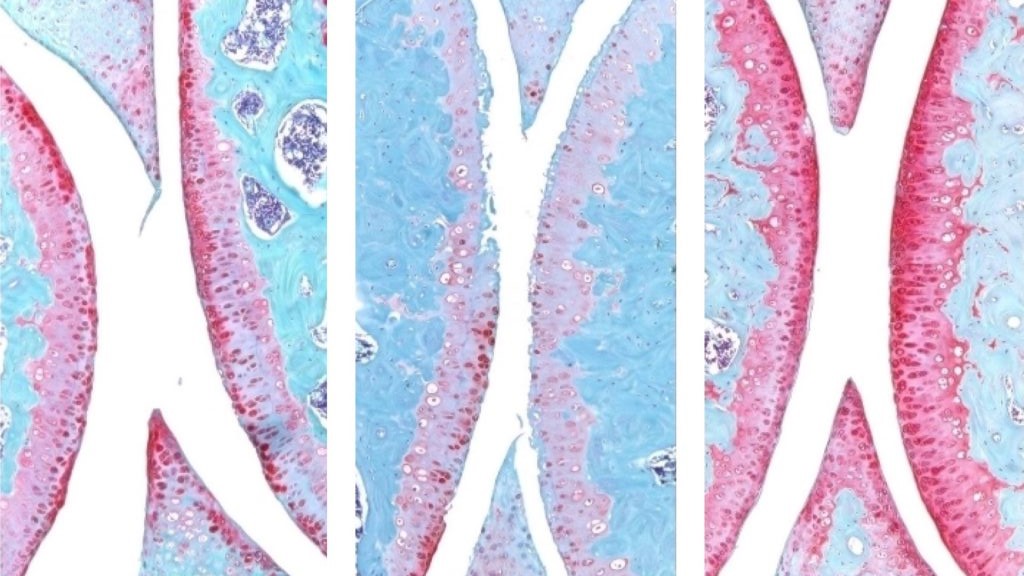
The knee joint of a young mouse (left), aged mouse (middle) and treated aged mouse (right). The red indicates cartilage. Credit: Nidhi Bhutani
An injection that blocks the activity of a protein involved in ageing reverses naturally occurring cartilage loss in the knee joints of old mice, a Stanford Medicine-led study has found. The treatment also prevented the development of arthritis after knee injuries mirroring the ACL tears often experienced by athletes or recreational exercisers. An oral version of the treatment is already in clinical trials with the goal of treating age-related muscle weakness.
Samples of human tissue from knee replacement surgeries – which include both the extracellular scaffolding, or matrix, in the joint as well as cartilage-generating chondrocyte cells – also responded to the treatment by making new, functional cartilage.
The study results suggest it may be possible to regenerate cartilage lost to ageing or arthritis with an oral drug or local injection, rendering knee and hip replacement unnecessary.
The treatment directly targets the cause of osteoarthritis, a disease for which no drug can slow down or reverse its progress; the primary treatments for osteoarthritis are pain control and surgical replacement of the affected joints.
The protein, 15-PGDH – termed a gerozyme due to its increase in prevalence as the body ages – is a master regulator of ageing. Gerozymes, identified by the same researchers in 2023, also drive the loss of tissue function. They are a major force behind age-related loss of muscle strength in mice. Blocking the function of 15-PGDH with a small molecule results in an increase in old animals’ muscle mass and endurance. Conversely, expressing15-PGDH in young mice causes their muscles to shrink and weaken. The gerozyme has also been implicated in the regeneration of bone, nerve and blood cells.
In each of these tissues, regeneration is due to increases in the proliferation and specialisation of tissue-specific stem cells. However, chondrocytes change their patterns of gene expression to assume a more youthful state without the involvement of stem cells.
“This is a new way of regenerating adult tissue, and it has significant clinical promise for treating arthritis due to ageing or injury,” said Helen Blau, PhD, professor of microbiology and immunology. “We were looking for stem cells, but they are clearly not involved. It’s very exciting.”
“Millions of people suffer from joint pain and swelling as they age,” Bhutani said. “It is a huge unmet medical need. Until now, there has been no drug that directly treats the cause of cartilage loss. But this gerozyme inhibitor causes a dramatic regeneration of cartilage beyond that reported in response to any other drug or intervention.”
There are three main types of cartilage in the human body. One, elastic cartilage, is soft and flexible and forms structures like the outer ear. A second, fibrocartilage, is dense and tough, absorbing shock in areas such as between the spinal vertebrae. The third, hyaline cartilage, is smooth and glossy, providing a low-friction surface for lubrication and flexibility in joints like the ankles, hips, shoulders and parts of the knee. Hyaline cartilage, also known as articular cartilage, is the cartilage most commonly affected by osteoarthritis.
Osteoarthritis occurs when a joint is stressed by ageing, injury or obesity. The chondrocytes begin to release pro-inflammatory molecules and to break down collagen, which is the primary structural protein of cartilage. When collagen is lost, the cartilage thins and softens; the accompanying inflammation causes the joint swelling and pain that are hallmarks of the disease. Under normal circumstances, articular cartilage rarely regenerates. Although some populations of putative stem or progenitor cells capable of generating cartilage have been identified in bone, attempts to identify similar populations of cells in the articular cartilage have been unsuccessful.
Previous research from Blau’s lab has shown that a molecule called prostaglandin E2 is essential to muscle stem cell function. 15-PGDH degrades prostaglandin E2. Inhibiting 15-PGDH activity, or increasing levels of prostaglandin E2, supports the regeneration of damaged muscle, nerve, bone, colon, liver and blood cells in young mice.
Blau, Bhutani and their colleagues wondered if 15-PGDH might also play a role in ageing cartilage and joints. They wanted to find out if a similar pathway contributes to cartilage loss from ageing or in response to injury. When they compared the amount of 15-PGDH in the knee cartilage in young versus old mice, they saw that, as in other tissues, levels of the gerozyme increased about two-fold with age.
They next experimented with injecting old animals with a small molecule drug that inhibits 15-PGDH activity – first into the abdomen, which affects the entire body, then directly into the joint. In each case, the knee cartilage, which was markedly thinner and less functional in older animals as compared with younger mice, thickened across the joint surface. Further experiments confirmed that the chondrocytes in the joint were generating hyaline, or articular, cartilage, rather than less-functional fibrocartilage.
“Cartilage regeneration to such an extent in aged mice took us by surprise,” Bhutani said. “The effect was remarkable.”
Addressing ACL tears
Similar results were observed in animals with knee injuries like the ACL tears that frequently occur in people participating in sports such as soccer, basketball and skiing that require sudden pivoting, stopping or jumping. While the tears can be surgically repaired, about 50% of people develop osteoarthritis in the injured joint within about 15 years.
The researchers found that a series of injections twice a week for four weeks of the gerozyme inhibitor after injury dramatically reduced the chance that osteoarthritis develops in the mice. Animals treated with a control drug had levels of 15-PGDH that were twice as high as in their uninjured peers, and they developed osteoarthritis within four weeks.
The animals treated with the gerozyme inhibitor also moved more typically and put more weight on the paw of the affected leg than did untreated animals.
“Interestingly, prostaglandin E2 has been implicated in inflammation and pain,” Blau said. “But this research shows that, at normal biological levels, small increases in prostaglandin E2 can promote regeneration.”
A closer investigation of the chondrocytes in the joints of old mice and young mice showed that old chondrocytes expressed more detrimental genes involved in inflammation and the conversion of hyaline cartilage to unwanted bone, and fewer genes involved in cartilage development.
The researchers were also able to pinpoint subcategories of old chondrocytes that change their patterns of gene expression after treatment. One, which expresses 15-PGDH and genes involved in cartilage degradation, decreased in prevalence from 8% to 3% after treatment. Another, which does not express 15-PGDH but does express genes involved in the production of fibrocartilage, also decreased in prevalence: from 16% to 8% after treatment. A third population, which does not make 15-PGDH and which expresses genes involved in hyaline cartilage formation and the maintenance of the extracellular matrix necessary for its function, increased in prevalence after treatment from 22% to 42%. The findings indicate an overall shift in gene expression after treatment to a more youthful cartilage composition – without the involvement of stem or progenitor cells.
Finally, the researchers studied human cartilage tissue removed from patients with osteoarthritis undergoing total knee replacements. Tissue treated with the 15-PGDH inhibitor for one week exhibited lower levels of 15-PGDH-expressing chondrocytes and lowered cartilage degradation and fibrocartilage genes than control tissue and began to regenerate articular cartilage.
“The mechanism is quite striking and really shifted our perspective about how tissue regeneration can occur,” Bhutani said. “It’s clear that a large pool of already existing cells in cartilage are changing their gene expression patterns. And by targeting these cells for regeneration, we may have an opportunity to have a bigger overall impact clinically.”
Blau added, “Phase 1 clinical trials of a 15-PGDH inhibitor for muscle weakness have shown that it is safe and active in healthy volunteers. Our hope is that a similar trial will be launched soon to test its effect in cartilage regeneration. We are very excited about this potential breakthrough. Imagine regrowing existing cartilage and avoiding joint replacement.”
Complaints such as pain in the Achilles tendon, tennis elbow, swimmer’s shoulder and jumper’s knee are familiar to many young sportspeople, as well as to older individuals. These conditions are all caused by overloading of tendons and are generally very painful.
“Tendons are fundamentally susceptible to overuse,” explains Jess Snedeker, a professor of orthopaedic biomechanics at ETH Zurich and Balgrist University Hospital in Zurich. “They must withstand powerful loads, with all the forces of our muscles being concentrated to the relatively thin tendons that transmit these forces into movement of our skeleton.”
In medical terms, the aforementioned conditions are known as tendinopathies. They are some of the most frequent conditions seen by orthopaedic specialists, but treatment options are extremely limited. Although physiotherapy can help, there are many serious cases for which this treatment does not achieve much. Scientists are therefore keen to research these tendon problems in greater depth with a view to developing effective treatments.
Not just correlation – causation
Now, a team of researchers led by Snedeker and by Katrien De Bock, professor of exercise and health at ETH Zurich, has reached a new milestone. In the HIF1 protein, they have identified a central molecular driver of tendon problems of this kind. A part of HIF1 acts as a transcription factor, which controls the activity of genes in cells.
This protein was already known to be present at elevated levels in diseased tendons. However, it was unclear whether the increase was simply a concomitant phenomenon or whether the conditions are actually triggered by the protein. In experiments in mice and with tendon tissue from humans, the team of researchers has now shown the latter to be the case.
Treatment before it is too late
In mouse experiments, the researchers either activated the HIF1 protein permanently or switched it off completely. Whereas they observed tendon disease even without overloading in the mice with permanently activated HIF1, no tendon disease occurred in the mice if HIF1 was deactivated in tendons, even in the case of overloading.
Both in the mice and in the experiments with human tendon cells, which the researchers obtained from tendon surgeries at the hospital, they were able to show that elevated HIF1 levels in the tissue leads to a pathogenic remodelling of the tendons: More crosslinks form within the collagen fibres that make up the basic structure of the tendons.
“This makes the tendons more brittle and impairs their mechanical function,” explains Greta Moschini, a doctoral student in De Bock and Snedeker’s groups and lead author of the study. In addition, blood vessels and nerves growth into the tendon tissue. “This could be the explanation for the pain commonly observed in tendinopathy,” says Moschini.
“Our study not only provides new insight into how the disease develops. It also shows that it’s important to treat tendon problems early,” says Snedeker. He is thinking particularly of young athletes, who frequently struggle with tendinopathies. In these cases, it is often still possible to treat the problems. “However, the damage caused by HIF1 in tendon tissue can accumulate and become irreversible over time. Physiotherapy then no longer helps, and the only treatment at this moment is to surgically remove the diseased tendon.”
A starting point to search for treatments
The fact that HIF1 has now been identified as a molecular driver raises the question whether it is possible to develop medicines that deactivate HIF1 and therefore can prevent or cure tendon disease. It is not quite that easy, explains ETH Professor De Bock. In many organs of the body, HIF1 is responsible for detecting hypoxia and activating a physiological adaptation. “Switching HIF1 off throughout the body would likely lead to side effects,” she says.
It may be possible to look for methods that specifically deactivate HIF1 only in the tendon tissue. In De Bock’s view, however, the more promising approach would be to explore the biochemical processes around HIF1 in the cells in greater detail. This could help to identify other molecules that are influenced or controlled by HIF1 and that could be more suitable targets for the treatment of tendinopathy. The researchers will now embark on precisely that search.
Studies have reported on survival probabilities of people born with open spina bifida, a condition where the spinal cord and nerves are exposed through an opening in the back. Research published in Developmental Medicine & Child Neurology now provides life expectancies, with results reported by age, sex, and different levels of impairment.
In the study of 1659 patients with open spina bifida who received support from the California Department of Developmental Services in 1986–2019, survival varied significantly by walking and feeding ability and by bowel/bladder continence.
As an example, at age 5, the life expectancy was 27 additional years for males in the most severely impaired group and 65 years in the least severely impaired, compared with 70 years in the general population. Life expectancies also decreased markedly with age and were modestly lower for males compared with females.
“This is the first long-term study of spina bifida patients to report life expectancies by age, sex, and severity of impairment,” the authors wrote. “We hope the results… will aid patients and caregivers alike in the proper planning for and treatment of those living with spina bifida.”
The psychedelic effects recreational users often seek from taking ketamine do not predict the therapeutic benefits for people being treated for alcohol use disorder, according to new research from King’s College London and University of Exeter.
The popular theory, which says that ketamine may have its therapeutic benefits because it produces strong psychedelic effects, has been called into question by the new study, published in Addiction. The findings suggest the treatment response may be down to other effects of the drug.
The research, led by the Institute of Psychiatry, Psychology & Neuroscience at King’s, is the largest randomised controlled trial to date examining the use of intravenous ketamine-assisted psychotherapy for individuals with moderate to severe alcohol use disorder. It uses data from the Ketamine for reduction of Alcoholic Relapse (KARE) clinical trial at the University of Exeter and University College London.
For the first time, we thoroughly investigated the acute psychoactive effects of repeated ketamine infusions in people with alcohol use disorder. The effects didn’t predict ketamine’s therapeutic benefit, which leaves open other psychological or neural mechanisms that need to be investigated.
Dr Will Lawn, Senior Lecturer at King’s College London and study lead
Researchers carried out a secondary analysis of the KARE clinical trial which was conducted at two clinical research facilities in England involving 96 adult participants and sought to clarify the role of ketamine’s psychoactive effects in supporting abstinence from alcohol.
Participants receiving three weekly infusions of intravenous ketamine reported marked psychoactive experiences, including altered reality, out-of-body sensations, and perceptual distortions, compared to those receiving placebo. These effects were consistently strong across all three dosing sessions. This suggests little to no development of tolerance to ketamine’s subjective effects over the short dosing schedule.
But despite the pronounced psychoactive effects, the study found no significant evidence that these experiences mediated ketamine’s therapeutic benefit in reducing alcohol consumption. The percentage of days abstinent from alcohol over six months was not predicted by the intensity of subjective drug effects.
A larger trial will explore ketamine’s effects in brain connection and function changes, as well as dosing.
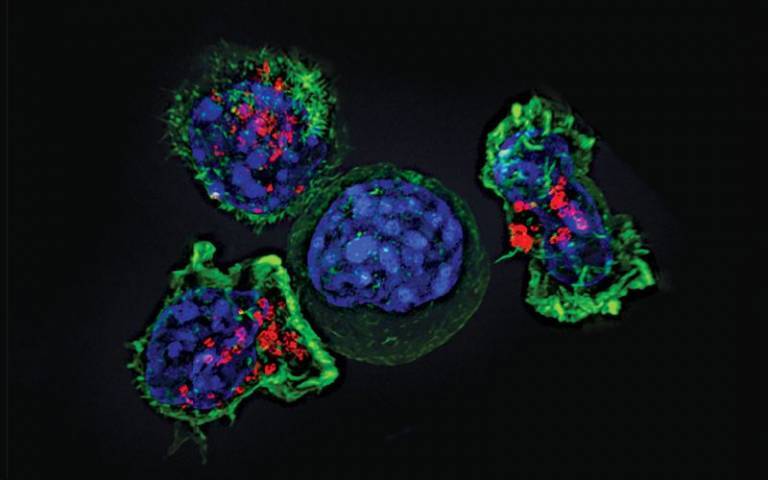
Killer T cells surround a cancer cell. Credit: Alex Ritter, Jennifer Lippincott Schwartz and Gillian Griffiths, National Institutes of Health (CC BY 2.0).
Immunotherapy given before or after surgery is increasingly used across several cancer areas. In an article published in the Journal of Internal Medicine, researchers at Karolinska Institutet present a comprehensive review of studies across seven tumour areas, showing how the field is moving towards earlier treatment.
For several years, immunotherapy has transformed the treatment of advanced cancer that can no longer be removed surgically. It is now used more frequently in earlier stages of disease as well – before surgery, known as neoadjuvant treatment, or after surgery, known as adjuvant treatment. In the new article, the researchers summarise findings from studies on several cancer diagnoses, grouped into seven tumour areas: skin cancer, lung cancer, breast cancer, gastrointestinal cancer, gynaecological cancer, head and neck cancer, and urological cancer.
Suggested benefits of treatment both before and after surgery
Several studies in recent years have shown that adjuvant immunotherapy after surgery can reduce the risk of the disease returning. Additional studies indicate that neoadjuvant treatment, given while the tumour is still in place, in many cases can provide the immune system with better conditions to recognise tumour cells. In several tumour areas, the results also suggest that immunotherapy given both before and after surgery may offer advantages compared with adjuvant treatment alone.
At the same time, the authors emphasise that the results vary between different cancer types and that the treatment involves challenges, such as the risk of side effects and the possibility that some patients may receive more treatment than necessary if surgery alone would have been sufficient.
“We see that immunotherapy in early stages of disease is developing rapidly across many tumour areas. By bringing together studies from many cancer types, it becomes clearer how the field is evolving and what experiences can be shared between different specialties,” says last author Hildur Helgadottir, researcher at the Department of Oncology-Pathology at Karolinska Institutet.
How the researchers carried out the review
The work behind the article is a collaboration between 14 researchers at the Department of Oncology-Pathology, Karolinska Institutet. All of them also work with cancer treatment in clinical care. Because the researchers come from seven different tumour areas, the article gathers experiences from many parts of cancer care.
“It is valuable that we have come together from so many different tumour areas. This gives a broader understanding of how immunotherapy is used across cancer care and can, in the long term, support both clinical decision-making and future research,” says Hildur Helgadottir.
The researchers also point to areas where more knowledge is needed. One of these is the development of biomarkers, measurable characteristics that can help healthcare determine which patients benefit from immunotherapy, both before and after surgery. They also discuss how introducing immunotherapy at earlier stages raises questions about costs, side effects, and whether healthcare resources will be sufficient, questions that current studies do not yet clearly answer.
Information about funders and potential conflicts of interest can be found in the scientific publication.
Bicuspid aortic valve (BAV) is a common congenital heart defect where the aortic valve has two leaflets (cusps) instead of the usual three, resulting in abnormal blood flow and development of aortic valve diseases such as aortic stenosis and incompetence. In addition, the BAV is sometimes accompanied by development of an enlarged aorta – the main artery in the body. Both the bicuspid aortic valve and an enlarged aorta often require cardiac surgery, usually after the age of 50 years. Despite this, only a limited number of genes have been associated with the disease and the molecular mechanisms remain unexplained in most cases.
In a new study aimed to further understand the genetic architecture of BAV, an international group of researchers led by Boston University Chobanian & Avedisian School of Medicine and Laval University in Quebec City, Canada, along with the Bicuspid Aortic Valve Consortium, the Genetic Aortic Network (a division of The Marfan Foundation) and participating Institutions, believe the condition is strongly influenced by the cumulative effect of variation in many different genes(polygenic contribution).
“We found that variation in 36 genetic regions increases the risk of a bicuspid aortic valve. These findings support the notion that bicuspid aortic valve disease is an inherited disease caused by a combination of many common genetic variants, not merely a single mutation in a single gene,” explains co-corresponding author Simon C. Body, MD, MPH, professor of anesthesiology at Boston University Chobanian & Avedisian School of Medicine.
From a group of 65 677 US, Canadian and European participants, the researchers performed a genome-wide association study (GWAS) meta-analysis on 9631 individuals with BAV. After identifying general genetic regions through GWAS, they used RNA sequencing to study gene activity (expression levels) in specific, relevant tissues.
They observed 36 regions with genetic variants associated with a bicuspid aortic valve, four of which had been previously identified. They prioritised 55 genes in these regions based upon expression in human aortic valve tissues from individuals who had surgery, then tested the effect of changing four selected genes, upon heart development in an experimental model, demonstrating that all four altered genes had effects on development of the valve. The researchers also looked at the effect of these genes in a statistical model finding a three-fold increase in risk for a BAV in individuals in the top 10% and association with aortic aneurysmal disease, a bulge in the aortic wall that can rupture. Some of these 36 genetic regions are also involved in aortic stenosis and aortic aneurysm development, which could lead to better prediction of these complications in people with BAV and point to biological mechanisms responsible for these joint effects.
According to the researchers, while these findings support the notion that BAV is an inherited disease, the findings do not currently support genetic testing, either prenatally or later in life, for predicting a bicuspid aortic valve. “Echocardiography and other imaging modalities remain the gold standard for diagnosis. In addition, the identified heritability supports performing screening echocardiography on first-degree relatives of a person with an identified bicuspid valve,” adds Body.
These findings appear online in the journal Circulation.
A new randomised controlled study funded by the Crohn’s & Colitis Foundation found that time-restricted feeding, a form of intermittent fasting, significantly reduced symptomatic disease activity and systematic inflammation in adults with Crohn’s disease and overweight or obesity. The University of Calgary-led trial is the first to show that eating only within an 8-hour window can reduce Crohn’s disease activity by 40% and abdominal discomfort by 50% in just 12 weeks, compared to a standard eating schedule.
Participants practicing intermittent fasting not only lost about 2.5kg while controls gained approximately 1.7kg, but also showed notable improvements in blood markers of inflammation and immune health, including lower levels of leptin and PAI-1 – all without cutting calories.
Results of the study were published in Gastroenterology. People with IBD should talk with their healthcare team before changing their eating schedule to determine whether intermittent fasting is appropriate for them.
Time-restricted feeding (TRF) involves eating all meals within a set 8-hour window each day, followed by fasting for the remaining 16 hours. This 12-week randomised trial included 35 adults with Crohn’s disease and living with obesity or overweight, with 20 assigned to TRF and 15 to their regular diet. Researchers measured disease activity, inflammation, and body composition at the start and end of the study.
“This study shows that while weight loss is an important outcome in people with overweight and Crohn’s disease, time-restricted feeding offers additional benefits beyond just the scale,” said Maitreyi Raman, MD, Associate Professor of Medicine at the University of Calgary, the study’s senior author. “We saw meaningful improvements in disease symptoms, reduced abdominal discomfort, favourable shifts in metabolism and inflammation, and promising changes in gut bacteria – all suggesting that intermittent fasting may help patients maintain lasting remission from Crohn’s disease.”
The research was supported by the Crohn’s & Colitis Foundation’s Litwin IBD Pioneers program. “Time-restricted feeding is showing real promise as a new way to help people with Crohn’s disease manage not only their symptoms but also their overall health,” said Andres Lorenzo Hurtado, PhD, Senior Vice President of Translational Research & IBD Ventures at the Crohn’s & Colitis Foundation. “This research suggests that changing when we eat – not just what we eat – can improve metabolism, help the immune system work better, and support long-term remission from Crohn’s disease. We are excited to support studies like this that put patients at the centre of new solutions and encourage more research to make these benefits last for everyone living with IBD.”
“People with Crohn’s disease often look for practical tools to support their health alongside medication,” said Natasha Haskey, PhD, RD, Research Associate at the University of British Columbia and lead investigator in the study. “Our research suggests time-restricted eating may be a sustainable option grounded in biology, offering patients more ways to manage their own wellness.”
In addition to reducing Crohn’s disease activity, the study found a marked decrease in harmful visceral fat and key inflammatory signals in the blood of those who practiced intermittent fasting. The changes were not simply due to diet quality or calorie restriction, as both groups ate similar foods and amounts—indicating the timing of meals themselves may play a unique role in supporting digestive and immune health.
Researchers note that, while these results are promising, larger trials are needed to confirm the long-term safety and effectiveness of this approach for broader groups of patients with IBD.
Statins do not cause the majority of the conditions that have been listed in their package leaflets, including memory loss, depression, sleep disturbance, and erectile and sexual dysfunction, according to the most comprehensive review of possible side effects. The study was led by researchers at Oxford Population Health and published in The Lancet.
Cardiovascular disease results in around 20 million deaths worldwide and causes around a quarter of all deaths in the UK. Statins are highly effective drugs that lower LDL (‘bad’) cholesterol levels and have been repeatedly proven to reduce the risk of cardiovascular disease. However, there have been concerns about possible side effects.
The researchers gathered data from 23 large-scale randomised studies from the Cholesterol Treatment Trialists’ Collaboration: 123 940 participants in 19 large-scale clinical trials comparing the effects of statin therapies against a placebo, and 30 724 participants in four trials comparing more intensive versus less intensive statin therapy.
They found similar numbers of reports for those taking the statins and those taking the placebo for almost all the conditions listed in package leaflets as possible side effects. For example, each year, the number of reports of cognitive or memory impairment was 0.2% in those taking the statins, but also 0.2% in those taking the placebo. This means that while people may notice these problems whilst taking statins, there is no good evidence that they are caused by the statin.
Key findings:
There was no statistically significant excess risk from statin therapy for almost all the conditions listed in package leaflets as potential side effects.
Taking a statin did not cause any meaningful excess of memory loss or dementia, depression, sleep disturbance, erectile dysfunction, weight gain, nausea, fatigue or headache, and many other conditions.
There was a small increase in risk (about 0.1%) for liver blood test abnormalities. However, there was no increase in liver disease such as hepatitis or liver failure, indicating that the liver blood test changes do not typically lead to more serious liver problems.
Christina Reith, Associate Professor at Oxford Population Health and lead author of the study, said: ‘Statins are life-saving drugs used by hundreds of millions of people over the past 30 years. However, concerns about the safety of statins have deterred many people who are at risk of severe disability or death from a heart attack or stroke. Our study provides reassurance that, for most people, the risk of side effects is greatly outweighed by the benefits of statins.’
Previous work by the same researchers established that most muscle symptoms are not caused by statins; statin therapy caused muscle symptoms in only 1% of people during the first year of treatment with no excess thereafter. It has also shown that statins can cause a small increase in blood sugar levels, so people already at high risk may develop diabetes sooner.
Professor Bryan Williams, Chief Scientific and Medical Officer at the British Heart Foundation, said: ‘These findings are hugely important and provide authoritative, evidence-based reassurance for patients. Statins are lifesaving drugs, which have been proven to protect against heart attacks and strokes. Among the large number of patients assessed in this well-conducted analysis, only four side effects out of 66 were found to have any association with taking statins, and only in a very small proportion of patients.
‘This evidence is a much-needed counter to the misinformation around statins and should help prevent unnecessary deaths from cardiovascular disease. Recognising which side effects might genuinely be associated with statins is also important as it will help doctors make decisions about when to use alternative treatments.’
Professor Sir Rory Collins, Emeritus Professor of Medicine and Epidemiology at Oxford Population Health and senior author of the paper said: ‘Statin product labels list certain adverse health outcomes as potential treatment-related effects based mainly on information from non-randomised studies which may be subject to bias. We brought together all of the information from large randomised trials to assess the evidence reliably. Now that we know that statins do not cause the majority of side effects listed in package leaflets, statin information requires rapid revision to help patients and doctors make better-informed health decisions.’
All of the trials included in the analyses were large-scale (involving at least 1000 participants) and tracked patient outcomes for a median of nearly five years. The trials were double-blind, meaning that neither the trial participants nor those managing the participants or leading the study knew who was receiving which treatment, to avoid potential biases due to knowledge of treatment allocation. The list of possible side effects was compiled from those listed for the five most commonly prescribed statins.
Increasing use of blood tests to detect prostate cancer is leading to overworked doctors. NTNU has now created an AI diagnostic tool that can help lighten the burden.
Diagnostic tools based on artificial intelligence are now making their way into Norwegian hospitals. AI can independently read X-ray images and detect bone fractures, or assess cancer tumours in both the breast and prostate.
“AI tools can take over the detection of simple and clear-cut cases, allowing doctors to spend their time on more complex ones,” said Tone Frost Bathen. She is a professor at NTNU and the project manager of an AI-powered analysis tool for prostate cancer called PROVIZ.
Tests on patients at St Olavs Hospital indicate that the tool is very promising.
“AI can enable radiologists to determine more quickly and more accurately whether a patient needs a biopsy, and where in the prostate it should be taken from,” explained Bathen.
“The PROVIZ project started as early as 2018. It takes a long time to develop diagnostic tools in medicine because safety standards must be high. The application alone to be allowed to test the tool on patients was 500 pages. It is important to create a tool that clearly shows how the result was reached, and that fits into a busy hospital workday,” says Tone Frost Bathen, Professor at NTNU. Photo: Anne Sliper Midling / NTNU
A recent study shows that patients trust medical test results only if an experienced doctor confirms what has been detected.
“Trust in doctors and health professionals is key for artificial intelligence to gain a place in the diagnosis of prostate cancer. Technology alone is not enough. Human contact and professional assessment remain indispensable,” said Simon A. Berger, a PhD research fellow at NTNU.
Prostate cancer is a natural part of getting older
Prostate cancer is the most common form of cancer among men in Western countries.
Examinations have detected prostate cancer in 10% of 50-year-olds, 50% of 60-year-olds and approximately 70% of men over the age of 80.
This shows that the disease is naturally linked to ageing.
“Prostate cancer is something most men die with, not from,” added Berger.
A blood test called PSA can help detect prostate cancer. Since it has become more common for men to take this blood test, the number of new prostate cancer cases has risen sharply. There are now approximately 5000 new cases each year.
When more people are tested for something that many individuals naturally have as part of the ageing process, the next medical step after the blood test must also be carried out more often, so that doctors can obtain a broader clinical picture of its severity.
Most trust in doctors
Currently, this next step involves taking an MRI scan, which provides a detailed image of the prostate gland and the surrounding tissue. These images need to be interpreted manually by an experienced radiologist. As the number of images taken has increased sharply, this has created a need for new and more efficient ways of making diagnoses.
Through the PROVIZ project, NTNU researchers have developed an AI-powered tool that can help doctors interpret MRI images of the prostate. PROVIZ is currently available only for use as part of the ongoing research project, but efforts are underway to apply for a patent and make the tool commercially available.
High international competition for commercial AI tools
Several research groups around the world are now working on developing AI-based diagnostic tools for prostate cancer.
PROVIZ has completed its first clinical testing in collaboration with St. Olavs Hospital, and the results were good. The next step is a much larger clinical trial, as well as a regulatory approval process.
“Right now, we are seeking approximately 20 million NOK to finance this phase. Once funding is in place, the tool could be on the market in the US within a year, and in Europe in just over a year,” says Gabriel Addio Nketiah, a researcher at NTNU and responsible for the commercialisation of PROVIZ.
For a tool like this to be efficiency-enhancing in routine hospital practice, patients must also trust the findings detected through the use of AI.
“Patients have high expectations that AI can be used for faster diagnostics and to reduce healthcare waiting lists. Many see AI as a kind of safety valve – an additional resource that doctors can use alongside their professional judgment,” says Simon A. Berger, a PhD research fellow at NTNU.
Berger interviewed 18 men who had been diagnosed with prostate cancer through the use of PROVIZ. The study shows that trust in doctors and health professionals plays a decisive role in whether patients accept AI in the health services.
“Patients trust AI in lower-risk cases such as bone fractures, but not in cases where the perceived risk is higher, such as cancer. When the perceived risk is high, we place the greatest trust in specialized doctors who can confirm what AI has found,” explained Berger.
Doctors as guarantors
In his interviews, Berger identified three different dimensions of trust.
Foundational trust in the healthcare system: many patients had positive experiences from previous encounters with the healthcare system. This laid a positive foundation.
Inter-personal trust in health professionals: patients trusted the doctors and their assessments. This trust was crucial for accepting AI because the doctors explained and vouched for the technology.
Possible trust in AI: even though patients recognized the potential of AI, they always wanted a human assessment as well in prostate cancer diagnostics. They were concerned about accountability, professional judgement and AI’s (in)ability to see the whole clinical picture.
“The relationship between patient and doctor is still key. For AI to be accepted in clinical practice, health professionals must be active communicators and guarantors of safety. In order for doctors to serve as guarantors, they must first understand how AI arrived at its conclusions so they can verify that it has made the correct assessment. Patients accept the use of AI within a framework they already trust,” concluded Berger.
NTNU owns an MRI scanner at St. Olavs Hospital that is currently undergoing a major upgrade. It helps researchers obtain the best possible images to be used in, among other things, PROVIZ. “Unfortunately, there are few investors in medical technology right now, but we hope that someone sees the societal value of our project,” says Professor Tone Frost Bathen at NTNU. Photo: Anne Sliper Midling / NTNU
Berger SA, Håland E, Solbjør M. Patient Perspectives on Trust in Artificial Intelligence-Powered Tools in Prostate Cancer Diagnostics. Qualitative Health Research. 2025;0(0). doi:10.1177/10497323251387545









{kind=link}
{kind=link}
{kind=link}