An analysis in the Journal of the American Geriatrics Society reveals that older inpatients admitted to physicians who prescribe higher amounts of first-generation antihistamines face an elevated risk of delirium while in the hospital.
First-generation antihistamines, such as diphenhydramine, are among the leading causes of medication-related harms in older adults, and although these medications are indicated for histamine-related conditions such as hives and anaphylaxis, they may be prescribed inappropriately.
When investigators analysed data on 328 140 patients aged 65 years and older who were admitted by 755 attending physicians to 17 hospitals in Ontario, Canada in 2015–2022, they found that the overall prevalence of delirium was 34.8%. Patients admitted to physicians who more commonly prescribed first-generation antihistamines had 41% increased odds of experiencing delirium compared with patients admitted to physicians who rarely prescribed first-generation antihistamines.
“We hope our study raises awareness among hospitalists that sedating antihistamines can be harmful, and should be prescribed with caution,” said corresponding author Aaron M. Drucker, MD, of the University of Toronto and Women’s College Hospital.
Botulinum injection around neuromas may also be effective for other forms of pain
Photo by Raghavendra V Konkathi on Unsplash
Botulinum toxin injections provided greater short-term relief for phantom limb pain than standard medical and surgical care among Ukrainian war amputees, reports a new study led by Northwestern Medicine and Ukrainian physicians.
The study, which involved 160 amputees treated at two hospitals in western Ukraine between 2022 and 2024, could ultimately benefit millions worldwide, according to the research team.
Post-amputation pain affects most amputees. The condition limits prosthetic use, mobility and quality of life. In the US, more than 2 million people live with limb loss. In Ukraine, it is estimated that over 100 000 soldiers and civilians have lost limbs since Russia’s full-scale invasion, which began in 2022.
“Botulinum toxin injected into painful stumps of residual limbs and around neuromas was on some outcome measures more effective than comprehensive medical and surgical treatment at one month post-treatment,” said senior study author Dr Steven P. Cohen, a professor of anaesthesiology and the vice chair of research and pain medicine at Northwestern University Feinberg School of Medicine.
Dr. Steven Cohen is a retired U.S. Army colonel who traveled to Ukraine to collaborate with local doctors.
“Our results show that botulinum toxin potentially could be a powerful short-term tool for treating post-amputation pain when used alongside comprehensive medical and surgical care,” said co-author Dr. Roman Smolynets, an anesthesiologist and intensive care specialist at Multidisciplinary Clinical Hospital of Emergency and Intensive Care in Lviv, Ukraine.
“It could be another step toward helping amputees live with less pain and more dignity. But always as an additional point to comprehensive medical and surgical care, not as a monotherapy.”
All study participants were amputees treated at the First Medical Union of Lviv or Ivano-Frankivsk Regional Hospital. About one-fifth received botulinum toxin injections around painful nerve endings, called neuromas, in addition to standard medical and physical therapy. The other participants received comprehensive medical and surgical treatment, which included surgical revision, nerve blocks, physical and psychological therapy, medications and other interventional procedures.
The research team assessed pain levels at the start of treatment and after one and three months, focusing separately on phantom limb pain (pain in the missing limb) and residual limb pain (pain at the stump site).
At one month, the botulinum toxin group experienced an average reduction of four points in phantom limb pain on a 10-point scale, compared with just one point among patients in the comparison group. Also at one month, 69% of patients who received botulinum toxin achieved a meaningful improvement (defined as at least a 30% drop in pain) in phantom limb pain, versus only 43% in the other patient group.
However, the results shifted at three months: Patients who received comprehensive care showed more durable pain relief than the botulinum toxin group, consistent with previous research showing that botulinum toxin’s pain-relieving effects typically last about three months.
A novel way to inject botulinum toxin
While botulinum toxin injections, a non-surgical treatment that alleviates pain by blocking nerve signals, are most commonly known for their use in cosmetic procedures, they are also an established tool to treat chronic pain.
In the study, the substance was injected in a novel way. The research team used ultrasound guidance to inject botulinum toxin directly around painful nerve endings and surrounding soft tissues, rather than into muscle or skin. This targeted “peri-neuromal” approach, the scientists believe, may explain the strong short-term reduction in pain by quieting nerve activity and local inflammation. Previous studies have shown botulinum toxin to be effective for neuropathic pain, but none injected it around painful nerves.
The new findings suggest that botulinum toxin injections near nerves may also help relieve other types of nerve pain, such as shingles-related pain, carpal tunnel syndrome and pain following surgeries like mastectomy or thoracotomy.
Friendship with a Ukrainian anaesthesiologist
Cohen, who traveled to Ukraine in 2024 to help launch the study, is a retired U.S. Army colonel who served four overseas tours in support of military operations; his son currently serves with the infantry.
In Ukraine, he partnered with Smolynets, who has treated thousands of soldiers and civilians injured in the war by working in the country’s largest trauma and emergency center, and Dr. Nadiya Segin, who is pioneering the use of Botulinum toxin and nerve stimulation to treat war injuries.
Smolynets will visit Chicago the week of Oct. 19 with a Ukrainian delegation for an observership program, spending time with Cohen at his pain medicine clinic and at a Shirley Ryan AbilityLab in downtown Chicago. The two physicians, now close friends, are available for interviews during that week.
More research in Ukraine
Cohen and his colleagues stress the need for larger, randomized trials to confirm their findings, refine patient selection and optimize botulinum toxin dosing. Future research should also explore whether repeat botulinum toxin injections over time could produce sustained benefits for post-amputation pain, as they appear to do for migraine treatment.
Cohen and Smolynets, who published another study in February about using hydrodissection for post-amputation pain in Ukraine, are also researching more novel war treatments in Ukraine, at Walter Reed, and Northwestern, for traumatic brain injury and PTSD. These studies are underway.
“As a retired colonel and the father of an infantry soldier who could be deployed in future conflicts and suffered from traumatic brain injury while at the U.S. Military Academy, this research carries special personal meaning for me,” Cohen said.
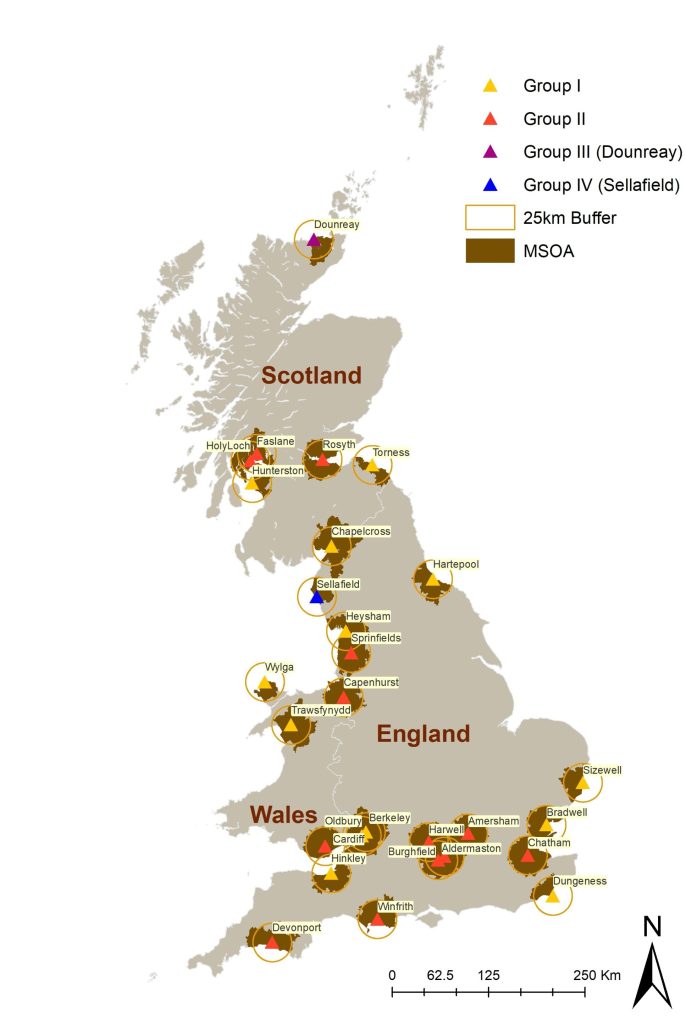
Children living near nuclear power stations in the UK are not at increased risk of childhood cancers, according to a new analysis.
The research was led by scientists at Imperial College London and University of Bristol and commissioned by the UK Committee on the Medical Aspects of Radiation in the Environment (COMARE). The results, published in International Journal of Epidemiology, found no evidence of increased risk of childhood cancers among children living near 28 nuclear installations between 1995 and 2016.
Researchers analysed cancer incidence data for nearly 50 000 cases of childhood leukaemia, non-Hodgkin’s lymphoma (LNHL), central nervous system (CNS) tumours, and other solid tumours in children aged 0–14 years.
They looked at data for communities living within 25 kilometres of installations, including those which have been linked to historical concerns about potential health impacts – such as Sellafield in Cumbria and Dounreay in northern Scotland.
The analysis found no evidence of increased risk of childhood cancers among children living near 28 nuclear installations between 1995 and 2016. (Credit: Davies, B. et al. Int J Epidemiol, 2025)
Using these data and advanced statistical modelling, they found no increased incidence of childhood cancers in these areas compared to national averages.[1] They also found no evidence that cancer risk increased the closer children lived to the nuclear sites.
Dr Bethan Davies, from Imperial’s School of Public Health and lead author of the study, said: “For many years there have been public concerns about the potential health impacts of living near nuclear installations. Our analysis suggests that children living near these sites today are not at increased risk.”
The latest study builds on decades of research following reports in the 1980s of clusters of cancer cases near nuclear facilities in England, Scotland and Germany[2] – following which, the UK Government set up COMARE to advise on the health effects of radiation.
Early investigations confirmed clusters of cases of some cancers near nuclear installations, particularly LNHL.
However, subsequent studies failed to show any direct link between these cases and radiation exposure from nuclear facilities.
In 2016, a COMARE report[3] suggested other potential explanations for these case clusters, including infections introduced due to population mixing in the areas.
The new findings come at a time of renewed interest in nuclear energy as part of the UK’s strategy to meet net-zero carbon targets and the government committing £14.2bn to build a new nuclear power station in Suffolk and develop small modular reactors.
The researchers say that while their study offers reassurance, they support COMARE’s recommendations for ongoing surveillance of cancer incidence near nuclear sites.
The authors acknowledge a number of limitations with their study, including the use of residential address at diagnosis as a proxy for exposure.
They were also unable to account for individual-level risk factors – such as genetic or medical conditions. However, they emphasise that the study’s design and comprehensive data make it one of the most detailed assessments to date.
Dr Davies added: “As the UK government announces a multibillion-pound investment for new nuclear energy infrastructure, our findings should provide reassurance that the historical clusters of childhood cancers reported near sites such as Sellafield and Dounreay are no longer evident.”
Professor Mireille Toledano, Mohn Chair in Population Child Health in Imperial’s School of Public Health, said: “These findings are both timely and important. As the UK and other countries expand their nuclear energy capacity, it’s vital that public health remains a central consideration. It’s reassuring that our study found that the historic case clusters have resolved, but it remains important we continue to monitor public health data around such sites across the UK for any emerging trends of concern.”
The full study, published today in the International Journal of Epidemiology, was supported by funding from the National Institute for Health and Care Research (NIHR), Health Data Research UK (HDRUK) and the UK Medical Research Council (UK Research and Innovation (UKRI)).
The work was also supported by the NIHR Imperial Biomedical Research Centre, a translational research partnership between Imperial College Healthcare NHS Trust and Imperial College London.
–
[1] Researchers obtained national incident cases of cancer diagnosed between 1995 and 2016 in children under 15 years of age from NHS England (formerly Public Health England), Welsh Cancer Intelligence and Surveillance Unit and Health Protection Scotland.
[2] A cluster of cases of leukaemia in children living close to the Sellafield nuclear plant was reported in 1983. An Independent Advisory Group confirmed the cluster and the UK government established COMARE to advise on the health effects of radiation. Subsequent studies identified increased risks of cancers in children and young adults living near Sellafield, Dounreay (Scotland), and Hamburg (Germany) nuclear installations.
[3] Committee on Medical Aspects of Radiation in the Environment (COMARE) – Seventh report (2016) https://assets.publishing.service.gov.uk/media/5a7f70ed40f0b6230268f83c/COMARE_17th_Report.pdf
HealthTech is transforming healthcare through AI, mobile applications, wearable devices, telemedicine, and big data analytics. While these advances offer enormous potential to improve patient outcomes and operational efficiency, they also raise complex legal and regulatory challenges – spanning intellectual property, data privacy, licensing, corporate governance, funding, taxation, and litigation.
Webber Wentzel’s Navigating HealthTech Legal Solutions highlights the firm’s extensive experience in helping innovators, investors, and healthcare providers across Africa address the legal and regulatory complexities of HealthTech. Mapping out the complexities at play across both the technology and the law, this resource brings together Webber Wentzel’s cross-practice teams to give clients a holistic perspective on opportunities, risks, and emerging trends in healthcare innovation.
“Our clients are leading the way in healthcare innovation, and they need legal partners who understand the sector end-to-end,” says Bernadette Versfeld, head of the Consumer sector. “This resource demonstrates how we help businesses navigate regulatory hurdles, adopt new technologies, structure investments effectively, and manage risk, all while enabling growth and innovation.”
Drawing on extensive experience working with healthcare companies, insurers, tech providers, investors, and regulators across Africa, the report provides insights into medical device licensing, HealthTech investment structuring, protecting personal health data, managing litigation risks, and compliance with South Africa’s National Health Insurance Act.
“As part of our ongoing commitment to supporting Africa’s healthcare sector, Webber Wentzel continues to advise on emerging trends, innovative technologies, and regulatory developments. By combining deep sector knowledge with cross-practice expertise, we help clients not just respond to change but shape it, empowering them to navigate the complex intersection of healthcare and technology,” adds Versfeld.
Allen Institute scientists are learning why vaccines can trigger a weaker response in older adults, around age 65, and what can be done to improve them. These insights open the door to designing more effective vaccines.
In the largest study of its kind, published in Nature, scientists discovered that T cells undergo profound and specific changes as we age. These changes, far from being random or a byproduct of chronic disease and inflammation, are a fundamental feature of healthy aging and will happen to all of us as we get older.
“We were surprised that inflammation is not driving healthy aging. We think inflammation is driven by something independent from just the age of a person,” said Claire Gustafson, PhD, assistant investigator at the Allen Institute and one of the lead authors of the study. “This is important because there’s been research showing similar findings that inflammation and aging don’t go hand in hand, and your immune system is just changing with age.”
The changes also point to why vaccines, including the annual flu shot and COVID-19 boosters, tend to be less effective in older adults.
The changes scientists discovered
T cells are a critical part of our immune system that help “train” B cells, to produce antibodies in response to viruses and vaccines. But this study found that memory T cells in older adults undergo a dramatic shift toward what is known as a “Th2-like” state, which is a change in gene expression that fundamentally alters how these cells respond to threats. Researchers found this shift directly affects B cells’ ability to generate strong antibody responses. In other words, the flu shot might still deliver the right viral components, but if the memory T cells aren’t functioning properly, the body struggles to respond effectively.
How this could lead to better vaccines
With this insight, doctors may be able to use a person’s immune profile to predict how well they’ll respond to a vaccine. Now that scientists can pinpoint how T cells become less effective with age, they can also start designing new vaccine formulas or immune-boosting treatments to address these issues.
Since T cells in older adults function differently, scientists could reformulate vaccines to compensate specifically for age-related cellular changes rather than using a one-size-fits-all approach. Gene-editing tools like CRISPR could also be used to reprogram a person’s T cells before vaccination, essentially re-programming older immune cells to make them respond to vaccines like younger cells do—like CAR-T cell therapy that reprograms immune cells to fight cancer.
Researchers say this work goes beyond just vaccines and reveals how our immune systems change in all of us as we get older and how our bodies fight age-related disease and viruses. It also opens the door to interventions like new therapies to restore key immune cells.
How researchers made the discovery
Scientists tracked more than 96 healthy adults ages 25–65 for over two years in collaboration with Benaroya Research Institute. The researchers then used cutting-edge techniques like single-cell RNA sequencing, proteomics, and spectral flow cytometry to profile the immune system of these individuals over time. The scientists then used this data on the immune system to create a detailed Human Immune Health Atlas, an online resource mapping 71 different immune cell types and how they change over time, and why those changes matter. Then, they applied this Atlas to study over 16 million individual immune cells from healthy adults 25–90+ years of age, offering an unprecedented tool for researchers worldwide to better understand, and support, the aging immune system. This online resource is the largest of its kind and freely available to researchers worldwide.
“This research illustrates how working collaboratively can make a significant impact on our understanding of the immune system, both now and in the future,” said Jane Buckner, MD, president of the Benaroya Research Institute. “It was made possible through the combined efforts of several Seattle-based research institutions, dedicated scientists, clinicians and research coordinators, as well as the individuals who generously volunteered their time, samples, and health information.”
The significance of this work extends beyond aging research and provides a roadmap for understanding how immune dysfunction develops over time, offering concrete targets for intervention and potentially transforming how we approach immune health across the entire human lifespan.
“There’s so much more information to be gained by looking at this dataset we’ve produced,” said Gustafson. “My hope is that it will be used for a long time to enable other researchers to look more deeply and find more insights into human immunity.”
The study is the largest global analysis of in-flight medical events
Photo by Daniel Eledut on Unsplash
With nearly five billion people flying each year, medical emergencies in the air may be more common than most realise and they can be deadly.
A new study led by Duke Health researchers analysed more than 77, 00 in-flight medical events reported to the world’s busiest airline medical support centre. The findings show that while most incidents are minor, thousands of passengers required hospital care after landing, and hundreds died or triggered aircraft diversions.
The study, published in JAMA Network Open, was conducted in partnership with MedAire, an aviation and maritime health and safety solutions company, which also provided the data for analysis. The paper offers a rare look into how airlines respond to medical crises and why some flights are forced to divert.
“It gives us a real-world snapshot of what happens when someone gets sick in the sky and how starkly the options differ from those in a hospital,” Rotta said.
Researchers reviewed medical calls from 84 airlines across six continents, covering over 3.1 billion passenger boardings between January 2022 and December 2023.
They found that one in every 212 flights involved a medical emergency. Of those flights, about 8% of passengers were taken to the hospital after landing, and 1.7% of the total medical events were so serious they caused the plane to divert.
The most common reasons for diversion were suspected strokes, seizures, chest pain, and altered mental status. Cardiac arrest occurred in 293 cases, with survival rates far lower than on land.
Medical volunteers (often physicians) assisted in nearly one-third of emergencies. Their involvement was linked to a higher likelihood of diversion, likely because they were called upon during more serious events.
“It’s humbling to practice medicine in the air,” said Rotta, who became interested in the topic after being called upon as medical volunteer during several flights. “You’re working with limited equipment, no lab tests and no backup. Even minor issues can become major challenges.”
Rotta emphasised that airlines are generally well-prepared, especially in the US, where regulations require defibrillators and basic medical kits. However, he noted that not all airlines partner with ground-based medical support centres, an approach he believes is essential.
“Airplanes aren’t hospitals, and we shouldn’t expect them to be,” he said. “But having expert guidance from the ground can make all the difference when someone’s life is at risk.”
The findings could help shape airline policies, improve crew training and inform passengers with chronic conditions about how to prepare for travel.
Doctors who use artificial intelligence at work risk having their colleagues deem them less competent for it, according to a recent Johns Hopkins University study.
While generative AI holds significant promise for advancing health care, a new study finds its use in medical decision-making impacts how physicians are perceived by their colleagues. The research shows that doctors who primarily rely on generative AI for decision-making face considerable scepticism from fellow clinicians, who correlate their use of AI with a lack of clinical skill and overall competence, resulting in a diminished perceived quality of patient care.
The research included a diverse group of clinicians from a major hospital system, involving attending physicians, residents, fellows, and advanced practice providers. Results of the study were published in Nature Digital Medicine.
Stigma stunts better care
The findings may indicate a social barrier to AI adoption in health care settings, which could slow advances that might improve patient care.
“AI is already unmistakably part of medicine,” says Tinglong Dai, professor of business at the Johns Hopkins Carey Business School and co-corresponding author of the study. “What surprised us is that doctors who use it in making medical decisions can be perceived by their peers as less capable. That kind of stigma, not the technology itself, may be an obstacle to better care.”
The study, conducted by researchers at Johns Hopkins University, involved a randomised experiment where 276 practicing clinicians evaluated different scenarios: a physician using no AI, one using AI as a primary decision-making tool, and another using it for verification. The research found that as physicians were more dependent on AI, they faced an increasing “competence penalty,” meaning they were viewed more sceptically by their peers than those physicians who did not rely on AI.
“In the age of AI, human psychology remains the ultimate variable,” says Haiyang Yang, first author of the study and academic program director of the Masters of Science in Management program at the Carey Business School. “The way people perceive AI use can matter just as much as, or even more than, the performance of the technology itself.”
Skipping AI equalled more respect
According to the study, peer perception suffers for doctors who rely on AI. Framing generative AI as a “second opinion” or a verification tool partially improved negative perceptions from peers, but it did not fully eliminate them. Not using GenAI, however, resulted in the most favourable peer perceptions.
The findings align with theories that suggest perceived dependence on an external source like AI can be seen as a weakness by clinicians.
Ironically, while GenAI’s visible use can undermine a physician’s perceived clinical expertise among peers, the study also found that clinicians still recognise AI as a beneficial tool for enhancing precision in clinical assessment. The research showed that clinicians still generally acknowledge the value of GenAI for improving the accuracy of clinical assessments, and they view institutionally customized GenAI as even more useful.
The collaborative nature of the study led to thoughtful suggestions for GenAI implementation in health care settings, which are crucial to balance innovation with maintaining professional trust and physician reputation, the researchers note.
“Physicians place a high value on clinical expertise, and as AI becomes part of the future of medicine, it’s important to recognise its potential to complement – not replace – clinical judgment, ultimately strengthening decision making and improving patient care,” said Risa Wolf, co-corresponding author of the research and associate professor of pediatric endocrinology at Johns Hopkins School of Medicine with a joint appointment at the Carey Business School.
A new study, led by clinical researchers from Imperial’s Department of Metabolism, Digestion and Reproduction and Imperial College Healthcare NHS Trust, has uncovered a link between a pregnant woman’s blood group and her risk of spontaneous premature birth, which the team hopes could in future lead to more personalised approaches to preventing early labour.
“The treatments we currently offer to prevent preterm birth have barely changed in decades. This research opens the door to more targeted, biologically-informed interventions.”
Dr Lynne Sykes Clinical Associate Professor, Department of Metabolism, Digestion and Reproduction
The findings, published in npj Biofilms and Microbiomes, draw on more than 74 000 anonymised maternity records from Imperial College Healthcare NHS Trust and data from high-risk pregnancies. The team found that women with blood groups B and O were associated with a higher risk of spontaneous preterm birth, while those from blood group A were associated with a lower risk.
The clinical researchers believe this is because women with blood group A are more likely to carry higher proportions of a protective bacterium and show less inflammation, both associated with healthy pregnancies.
The research also found that the blood group associations vary depending on underlying risk factors, including previous cervical surgery or a history of late miscarriage or premature birth. In women whose only risk factor was previous cervical surgery, blood group B was associated with a higher likelihood of preterm delivery. In contrast, in women with a history of late miscarriage or prior premature birth, blood group O was associated with the highest risk.
The team used advanced microbiome analysis on a subset of 596 high-risk women to investigate possible biological mechanisms at work. They found that women with blood group A were more likely to carry higher proportions of Lactobacillus crispatus, a ‘good’ bacterium associated with healthy pregnancies. In contrast, women of blood group B and O were more likely to harbour a more diverse bacterial signature. In women with blood group O, a direct link was observed between this bacterial signature, inflammation, and spontaneous preterm birth.
Speaking about the findings, Dr Lynne Sykes, lead researcher and Clinical Associate Professor at Imperial College London, and Consultant Obstetrician at Imperial College Healthcare NHS Trust, said: “Although we did not establish causation, we have identified a genetic link that can influence the risk of spontaneous premature birth in women. This could potentially impact women in the future by identifying risk earlier in pregnancy and by offering more tailored interventions. While we need further research, the prospect of moving towards personalised care in this area is hugely exciting.”
Next steps
The team demonstrated that blood group sugars are secreted into the vaginal fluid and that binding of these sugars can occur to key good and bad bacteria found in the vagina. However, one important limitation of the study was that researchers did not have “secretor status” data for participants, a genetic factor that affects whether blood group sugars are secreted in vaginal fluid. 80% of the population are “secretors”, whereas 20% do not secrete blood group sugars, so future studies that incorporate this information may strengthen the findings.
The research suggests that the ABO blood group, routinely tested early in pregnancy, could be used to help stratify preterm birth risk, especially when considered alongside other clinical factors. Importantly, the team accounted for ethnicity, known to affect both blood group prevalence and preterm birth risk, ensuring these results were not driven by population differences.
Dr Sykes added: “What excites me most is the opportunity this presents for truly personalised medicine in pregnancy, something that has been sorely lacking in our field. The treatments we currently offer to prevent preterm birth have barely changed in decades. This research opens the door to more targeted, biologically-informed interventions.”
The study also lays the groundwork for new therapeutic approaches. A clinical trial beginning this autumn, funded by March of Dimes in the US, will explore whether probiotic treatment with Lactobacillus crispatus (Lactin-V) can help reduce premature birth in high-risk women – and whether response to the treatment may vary by blood group.
A new study co-authored by a University of Wisconsin-Madison professor finds that life expectancy gains made by high-income countries in the first half of the 20th century have slowed significantly, and that none of the generations born after 1939 will reach 100 years of age on average.
Published in the journal Proceedings of the National Academy of Sciences, the study by Héctor Pifarré i Arolas of the La Follette School of Public Affairs, José Andrade of the Max Planck Institute for Demographic Research, and Carlo Giovanni Camarda of the Institut national d’études démographiques analysed life expectancy for 23 high-income and low-mortality countries using data from the Human Mortality Database and six different mortality forecasting methods.
“The unprecedented increase in life expectancy we achieved in the first half of the 20th century appears to be a phenomenon we are unlikely to achieve again in the foreseeable future,” according to Pifarré i Arolas. “In the absence of any major breakthroughs that significantly extend human life, life expectancy would still not match the rapid increases seen in the early 20th century even if adult survival improved twice as fast as we predict.”
From 1900 to 1938, life expectancy rose by about five and a half months with each new generation. The life expectancy for an individual born in a high-income country in 1900 was an average of 62 years. For someone born just 38 years later in similar conditions, life expectancy had jumped to 80 years on average.
For those born between 1939 and 2000, the increase slowed to roughly two and a half to three and a half months per generation, depending on the forecasting method. Mortality forecasting methods are statistical techniques that make informed predictions about future lifespans based on past and current mortality information. These models enabled the research team to estimate how life expectancy will develop under a variety of plausible future scenarios.
“We forecast that those born in 1980 will not live to be 100 on average, and none of the cohorts in our study will reach this milestone. This decline is largely due to the fact that past surges in longevity were driven by remarkable improvements in survival at very young ages,” according to corresponding author Andrade.
At the beginning of the 20th century, infant mortality fell rapidly due to medical advances and other improvements in quality of life for high-income countries. This contributed significantly to the rapid increase in life expectancy. However, infant and child mortality are now so low that the forecasted improvements in mortality in older age groups will not be enough to sustain the previous pace of longevity gains.
While mortality forecasts can never be certain as the future may unfold in unexpected ways – by way of pandemics, new medical treatments or other unforeseen societal changes – this study provides critical insight for governments looking to anticipate the needs of their healthcare systems, pension planning and social policies.
Although a population-level analysis, this research also has implications for individuals, as life expectancy influences personal decisions about saving, retirement and long-term planning. If life expectancy increases more slowly as this study shows is likely, both governments and individuals may need to recalibrate their expectations for the future.
Researchers wanted to know what allows the infection to hang on or come back, and whether it develops new tricks or resistances while living inside the lungs.
Researchers at Trinity Translational Medicine Institute (TTMI) and the Irish Mycobacterial Reference Laboratory at St James’s Hospital have uncovered how the bacterium Mycobacterium avium – a leading cause of difficult-to-treat chronic lung infections – changes and adapts inside patients over many years of illness. Their findings, published in Genome Medicine, could help doctors understand why M. avium infections come back and why antibiotics sometimes fail.
The team undertook this research to understand how M. avium manages to survive for years in people’s lungs, even during long courses of antibiotics. This bacterium causes a type of chronic lung infection that’s becoming more common around the world. By looking closely at its genetic code, the team hoped to see how it changes inside the body and why it can be so difficult to clear.
Treating M. avium lung disease is difficult – patients often need 12 months or more of several antibiotics, and treatment still fails in up to half of cases. Many patients get sick again even after therapy.
The team used whole-genome sequencing to analyse nearly 300 bacterial samples from patients in Ireland, the UK and Germany, including 20 Irish patients treated at St James’s Hospital. By reading the DNA of these bacteria over time, the scientists tracked how M. avium evolves, swaps strains and develops resistance while living in the human lung.
They found that infection is often not caused by one single long-term strain, but by repeated reinfection with new ones, sometimes closely related to strains seen in other European countries—hinting at shared environmental sources. The bacterium acquires roughly one new genetic change per year, and most importantly, the team found that thirteen specific genes showed signs of adaptation to antibiotics, immune attack and low-oxygen stress.
Lead author Dr Aaron Walsh, researcher in the Trinity Translational Medicine Institute said:
“Our study shows that M. avium can evolve in real time inside the lung. Understanding which genes help it survive may point us towards new treatment targets for this increasingly common and stubborn infection.”
This is the first study to use whole-genome sequencing to follow M. avium infections inside patients over many years, revealing how the germ evolves within the lungs.
Key findings from study
Reinfection is common: Many patients picked up new strains over time, suggesting they were reinfected from the environment rather than suffering relapse of the same infection.
International connections: Some Irish strains were genetically almost the same as ones from UK and Germany.
Thirteen key genes changed under pressure: These genes help the bacterium cope with antibiotics, low oxygen, or attack by the immune system.
Resistance can appear during treatment: We saw changes in a gene linked to rifampicin resistance in two patients receiving that drug.
Uniquely, in this study researchers found that thirteen genes under “positive selection” was new for M. avium.
Dr Emma Roycroft, Specialist Medical Scientist in the Irish Mycobacterial Reference Laboratory. “Some of those genes weren’t previously linked to survival of M. avium inside the body. For example, one involved in handling oxidative stress and another in forming biofilms. This has highlighted important pathways that could be targeted with new treatments. It was also striking that Irish, British and German samples were so closely related, even though the patients had never met.”
The team’s next steps are:
Test in the lab how those thirteen genes help the bacterium survive.
Use long-read sequencing to see genetic changes that short-read methods miss.
Study environmental samples to find where reinfections come from.
Expand their research to other patient groups to see if the same patterns occur.