As the world continues to face unprecedented challenges, including geopolitical tensions, extreme weather events, disease outbreaks, and economic uncertainty, the mental health of employees has become a pressing concern. This year’s World Mental Health Day theme, “Mental Health at Work”, is a crucial reminder for organisations to take action to safeguard their workforce’s mental health and wellbeing. In alignment with this theme, International SOS, the world’s leading health and security risk services company, encourages organisations worldwide to recognise the critical importance of mental wellbeing and resilience within their workforce.
Heightened anxiety
The increasing frequency and intensity of global crises, coupled with elevated job demands, are contributing to heightened levels of stress and anxiety, further exacerbating mental health concerns among the global workforce. According to the World Health Organization (WHO), an estimated 15% of working-age adults are experiencing a mental disorder at any single point in time.
Additionally, International SOS assistance data(2022 – 2024) reveals that over the past two years, the top five mental health-related assistance requests the organisation received are:
Anxiety
Depression
Panic disorder
Attention Deficit Hyperactivity Disorder (ADHD)
Acute stress
Burnout has also become a prominent issue among employees, with one in four employees worldwide reporting symptoms of burnout. The International SOS Risk Outlook 2024 report highlights employee burnout as a major threat impacting organisations.
Economic impact
Moreover, the economic impact of mental health issues cannot be ignored. The WHO estimates that globally, approximately 12 billion working days are lost annually to depression and anxiety, resulting in US$ 1 trillion in lost productivity per year. These figures highlight the importance for employers to create a workplace that promotes mental wellbeing and underscores the immense cost of neglecting employee mental health and wellbeing at work. Organisations play a pivotal role in shaping the mental health landscape by implementing policies and practices that promote wellbeing.
Dr Chris van Straten, Global Health Advisor Clinical Governance at International SOS said, “World Mental Health Day is a timely reminder for organisations to acknowledge and address the profound importance of mental wellbeing within their workforce. The workplace environment can have a significant impact on employee mental health, both positive and negative, by either fostering wellbeing or contributing to stress and anxiety. Just as we invest in employee physical safety, it is important to also understand that mental health is integral to overall health. It is therefore imperative to prioritise mental resilience.”
“Organisations can empower their employees to navigate challenges, thrive and contribute to a more positive and productive workplace by creating a supportive work environment that fosters open communication, empathy and understanding. Providing access to mental health professionals, counselling services, and employee assistance programmes is essential to ensure employees are equipped to navigate the complexities of today’s global landscape.”
To support the mental health and wellbeing of their workforce, International SOS provides advice for organisations:
Cultivate a supportive work culture with strong leadership commitment: Create a workplace culture and environment that prioritises and promotes open communication on mental health. Ensure mental wellbeing initiatives are seamlessly integrated into relevant policies and practices to provide robust support.
Provide accessible resources: Ensure employees have a toolkit of mental health resources at their fingertips, from counselling to self-guidance materials.
Promote work-life balance: Offer flexible work arrangements and remote work options to help employees manage their personal and professional lives effectively. Encourage regular breaks and empower employees to prioritise their wellbeing.
Training and education: Implement comprehensive mental health awareness campaigns to reduce stigma. Roll out mental health training, enabling everyone to spot, understand and assist with mental health challenges.
Monitor and assess: Seek feedback and continuously monitor the mental health of employees through surveys and assessments, and adapt programmes as needed.
Invest in emotional wellbeing: provide access to mindfulness sessions and stress management training—partner with certified mental health professionals to offer confidential counselling and support services.
Employee Assistance Programmes (EAPs): Provide EAPs that offer confidential counselling and support services to employees. Promoting the availability and benefits of EAPs can encourage employees to seek help without fear of stigma, fostering a culture of openness and support.
The South African Health Products Regulatory Authority (SAHPRA) and the Australian Therapeutic Goods Administration (TGA) have signed a Memorandum of Understanding (MoU), which will strengthen collaboration between the two health product regulators.
The MoU builds on the existing relationship between the health products regulators to improve capabilities in the assessment of medical products and therapeutic goods and their monitoring for continued efficacy, safety and quality once they are registered.
Areas of cooperation
SAHPRA and TGA will engage in data sharing aimed at improving the regulatory functions executed by both regulators. This will particularly focus on the assessment and approval of medical products and therapeutic goods, their monitoring for continued efficacy, and the surveillance for safety and adverse reaction (event) concerns.
According to SAHPRA’s Chief Executive Officer, Dr Boitumelo Semete-Makokotlela, the agreement with the TGA expands the geographical reach for both regulators’ pharmacovigilance programmes and augments their internal expertise.
“This partnership enables us to rely on each other’s strengths and regulatory outputs in the evaluation of health products both before they are registered and once they are approved for public use. This would improve therapeutic outcomes for the populations we exist for and increase the robustness of our post-registration surveillance for efficacy, safety and quality,” says Dr Semete-Makokotlela.
Deputy Secretary at the Australian Government Department of Health and Aged Care and head of the TGA, Professor Anthony Lawler, said: “TGA is very pleased to have strengthened our collaborative relationship with SAHPRA with the signing of this international agreement. We look forward to working alongside our regulatory counterparts in South Africa to share important regulatory information to ensure the continued safety, quality and efficacy of therapeutic products approved for market.”
Auditory hallucinations are likely the result of abnormalities in two brain processes: a “broken” corollary discharge that fails to suppress self-generated sounds, and a “noisy” efference copy that makes the brain hear these sounds more intensely than it should. That is the conclusion of a new study published October 3rd in the open-access journal PLOS Biology by Xing Tian, of New York University Shanghai, China, and colleagues.
Patients with certain mental disorders, including schizophrenia, often hear voices in the absence of sound.
Patients may fail to distinguish between their own thoughts and external voices, resulting in a reduced ability to recognise thoughts as self-generated.
In the new study, researchers carried out electroencephalogram (EEG) experiments measuring the brain waves of twenty patients diagnosed with schizophrenia with auditory hallucinations and twenty patients diagnosed with schizophrenia who had never experienced such hallucinations.
In general, when people are preparing to speak, their brains send a signal known as “corollary discharge” that suppresses the sound of their own voice.
However, the new study showed that when patients with auditory hallucinations were preparing to speak a syllable, their brains not only failed to suppress these internal sounds, but had an enhanced “efference copy” response to internal sounds other than the planned syllable.
The authors conclude that impairments in these two processes likely contribute to auditory hallucinations and that targeting them in the future could lead to new treatments for such hallucinations.
The authors add, “People who suffer from auditory hallucinations can ‘hear’ sounds without external stimuli. A new study suggests that impaired functional connections between motor and auditory systems in the brain mediate the loss of ability to distinguish fancy from reality.”
Researchers from have found a potential new way to improve the treatment of multiple sclerosis (MS) using a novel combined therapy. The results, published in the Journal of Clinical Investigation, builds on two harmonised Phase I clinical trials, focusing on the use of Vitamin D3 tolerogenic dendritic cells (VitD3-tolDCs) to regulate the immune response in MS patient.
Multiple Sclerosis (MS) is a long-term disease where the immune system mistakenly attacks the protective myelin sheath around nerve cells. This leads to nerve damage and worsening disability. Current treatments, like immunosuppressants, help reduce these harmful attacks but also weaken the overall immune system, leaving patients vulnerable to infections and cancer. Scientists are now exploring a more targeted therapy using special immune cells, called tolerogenic dendritic cells (tolDCs), from the same patients.
TolDCs can restore immune balance without affecting the body’s natural defences. However, since a hallmark of MS is precisely the dysfunction of the immune system, the effectiveness of these cells for auto transplantation might be compromised. Therefore, it is essential to better understand how the disease affects the starting material for this cellular therapy before it can be applied.
In this study, researchers from Barcelona’s Germans Trias i Pujol Institute and Josep Carreras Leukaemia Research Institute, examined CD14+ monocytes, mature dendritic cells (mDCs), and Vitamin D3-treated tolerogenic dendritic cells (VitD3-tolDCs) from MS patients who had not yet received treatment, as well as from healthy individuals. The clinical trials (NCT02618902 and NCT02903537) are designed to assess the effectiveness of VitD3-tolDCs, which are loaded with myelin antigens to help “teach” the immune system to stop attacking the nervous system. This approach is groundbreaking as it uses a patient’s own immune cells, modified to induce immune tolerance, in an effort to treat the autoimmune nature of MS.
The study, led by Dr Eva Martinez-Cáceres and Dr Esteban Ballestar, with Federico Fondelli as first author, found that the immune cells from MS patients (monocytes, precursors of tolDCs) have a persistent “pro-inflammatory” signature, even after being transformed into VitD3-tolDCs, the actual therapeutic cell type. This signature makes these cells less effective compared to those derived from healthy individuals, missing part of its potential benefits.
Using state-of-the-art research methodologies, the researchers identified a pathway, known as the Aryl Hydrocarbon Receptor (AhR), that is linked to this altered immune response. By using an AhR-modulating drug, the team was able to restore the normal function of VitD3-tolDCs from MS patients, in vitro. Interestingly, Dimethyl Fumarate, an already approved MS drug, was found to mimic the effect of AhR modulation and restore the cells’ full efficacy, with a safer toxic profile.
Finally, studies in MS animal models showed that a combination of VitD3-tolDCs and Dimethyl Fumarate led to better results than using either treatment on its own. This combination therapy significantly reduced symptoms in mice, suggesting enhanced potential for treating human patients.
These results could lead to a new, more potent treatment option for multiple sclerosis, offering hope to the millions of patients worldwide who suffer from this debilitating disease. This study represents a significant step forward in the use of personalised cell therapies for autoimmune diseases, potentially revolutionising how multiple sclerosis is treated.
The team is now preparing to move into Phase II trials to further explore these findings.
The idea of mandatory medical scheme coverage for employed people has made a comeback after the case for it was made at a recent conference. The policy move was previously on the cards in South Africa but faded after the ANC opted for National Health Insurance (NHI) at its 2007 national congress where Jacob Zuma was elected as the party’s new leader. Chris Bateman unpacks how a system with mandatory medical scheme membership for the employed might work and asked local experts whether it represents a viable alternative to government’s NHI plans.
A vigorous public debate has ensued since outgoing Netcare CEO, Dr Richard Friedland, on behalf of the Hospital Association of South Africa (HASA) delivered a strongly argued case for a return to what he described as the original ANC healthcare plan. He was speaking on “Viable and Near-term Opportunities to Providing Enhanced Healthcare in South Africa,” at HASA’s annual conference in Sandton held early in September.
Since then, the leadership of Business Unity SA (BUSA) met with President Cyril Ramaphosa and Health Minister Dr Aaron Motsoaledi, and his deputy and other senior officials, in mid-September to discuss “matters of concern” related to the NHI. The President requested BUSA to put forward specific proposals on “the remaining matters of concern” as a basis for re-engagement.
Some observers have suggested to Spotlight that these consultations are a first sign of government openness to changing or tweaking its NHI plans. But whether this means the door is actually open for a system of mandatory health insurance, or for mandatory health insurance as a stepping-stone toward NHI, is still unclear.
The NHI Act, that was signed into law by Ramaphosa in May, envisages a single-payer system where medical schemes are only allowed to cover health services that are not covered by the NHI fund.
How mandatory health insurance would work
Under mandatory health insurance, everyone who is in formal employment, or who earns above a certain threshold, would be forced by law to be a member of a medical scheme. This will result in medical scheme membership swelling substantially and some pressure being taken off the public healthcare system. It is also expected to result in medical scheme premiums being reduced because more healthy, younger people will join the schemes. People who are unemployed or who cannot afford health insurance will still be dependent on the public healthcare system.
Friedland said such mandatory healthcare insurance will triple the medical scheme market from 9.2 million to potentially 27.5 million beneficiaries over time and reduce those dependent on the state from 53.8 million to 35.5 million. In so doing, it would boost public healthcare per capita spending by 52%, (from R5 054 to R7 659), without any additional funding of the public sector budget, alleviate the strain on public hospitals and clinics, shorten waiting lists, and free up money to hire more staff and improve infrastructure. He said it is a “far faster and more efficient tool” for achieving health equity.
Responding to the counter argument that a mandatory health insurance system would entrench existing health inequalities, Professor Alex van den Heever, Chair of Social Security Systems Administration and Management Studies at the University of the Witwatersrand, said the opposite is true. “It accelerates convergence between the two systems faster than the NHI proposals,” he told Spotlight.
The relief for people who can afford medical scheme cover could also be significant. Friedland said mandatory medical scheme membership would bring more young and healthy people into the system, thus reducing the cost of monthly premiums by 25% to 30%.
Mandatory contribution schemes for civil servants have been implemented in more than half of the countries in Africa, while Thailand and many other Asian countries have started with mandatory cover for the formal sector before expanding to the non-formal sector. Such systems with what amounts to many medical schemes, rather than a single large fund, are also in place in several European countries, including the Netherlands and Germany.
Not a new idea
Mandatory health insurance, or an expanded role for medical schemes, are by no means new ideas in South Africa. Friedland told Spotlight that the ANC government’s own broad ranging 2002 inquiry into the various social security aspects of the South African health system concluded that national health insurance or the complete nationalisation of the private sector, could not be seriously considered as a reasonable option. (The inquiry itself was based on the Health Subcommittee Findings of the Committee of Inquiry into a Comprehensive System of Social Security.)
That 2002 report concluded: “National health insurance is not an option that emerges overnight as an alternative to social health insurance. Instead, it becomes feasible within market economies where formal employment levels are high. Prior to this, mixed systems are inevitable.”
One indication of how committed government was to such a mixed system with an expanded role for medical schemes in the early and mid-2000s, is the fact that the legislative framework to enable the expansion of medical scheme coverage was incorporated into the 2008 Medical Schemes Amendment Bill. That bill did not go as far as making scheme membership mandatory, but a mandatory system was clearly a next step on the reform agenda, as outlined in the very wide-ranging 2002 Taylor report on social security in South Africa. But presumably because of the NHI proposals, the 2008 amendments were allowed to lapse – and the scaffolding for a progressive expansion of medical scheme coverage collapsed.
There have since been several committees of inquiry and technical processes that validated an ongoing role for medical schemes, of which the Competition Commission’s Health Market Inquiry (HMI), that ran for five years (2014 to 2019), was the most technically detailed, consultative and authoritative. The HMI report did not recommend that medical scheme membership be made mandatory for people who are employed, but it did recommend a continued role for medical schemes and suggested that the most viable path to NHI may well involve first fixing the regulation of medical schemes.
Van den Heever said South Africa needs to quickly return to the pre-2008 reform trajectory to help stabilise the health system, “before more harm is done”. Government needs to summon up the political will to address the systemic governance failures of the public health system, removing the “bad actors and provincial cabals” that were destroying the integrity of South Africa’s free public health services, he added.
Better regulation also needed
For a system of mandatory health insurance to work, medical schemes will have to be more effectively regulated. Here the HMI report found that government had dropped the ball. It attributed the private health market failure and rampant medical inflation directly to government neglecting to regulate the private healthcare industry.
Health actuarial consultant, Barry Childs, joint CEO of Insight Actuaries and Consultants, told Spotlight private healthcare sector reforms urged by the HMI were ignored, resulting in ongoing confusion, high costs, complicated products and waste, among other problems. “Our incomplete medical scheme regulation keeps costs up, (for example anti selection, Prescribed Minimum Benefits), with benefits out of reach of most. We still don’t have a proper framework for lower cost-lower benefit products for those who cannot afford medical schemes,” he said.
The HMI report recommended a framework that went “way beyond naïve approaches to price control”, said Van den Heever, and addressed the powerful incentive structures driving unproductive forms of competition. In addition, he said, the industry-wide pooling approaches (risk equalisation and social reinsurance) followed international best practice and fully addressed issues of pooling fragmentation.
In the five years since the publication of the Commission’s HMI report, none of its major recommendations have been implemented.
Jobs and taxes
One common thread running back to the 2002 report, is the idea that South Africa is not economically ready for NHI and that a mixed system, possibly with mandatory health insurance, is more compatible with the current realities of high unemployment and a relatively small tax base.
“The root cause of inequity and inequality is not just a new form of apartheid. The real reason is the catastrophic level of unemployment. Until we address that, we will not solve an entire range of inequities, including food security, housing, education, and healthcare,” said Friedland.
On joblessness, Childs said South Africa was on track with the rest of the world’s growth up to 2008 but thereafter flat lined for over a decade. “We have dramatically underperformed the rest of the world and our peer group of middle-income countries in long term economic growth.”
In South Africa, unemployment is at an extremely high 33.5%, while in 2002 it was at 26%.
“If an NHI was unaffordable in 2002, how much more so is it today?” Friedland asked. He said that in this context, strong partnership, collaboration, and co-operation between the public and private sector is needed to bridge the polarisation that has arisen.
Analysis commissioned by BUSA found that raising the extra R200bn the health department says it needs to fund NHI would entail unrealistic and unaffordable tax hikes. It would either increase personal income tax by 31%, push VAT from 15% to 21.5%, or require the collection of a payroll tax of R1 565 per month from everyone in formal employment.
Van den Heever said that while government has a discretion to increase tax rates to any level it chooses, it cannot control the resulting amount of funds raised. He said that once tax capacity is reached, a hard ceiling on government revenue results at any given level of economic growth. The only way to grow revenues thereafter is through economic growth, failing which, revenues stagnate beyond government control.
The “big idea”, he said, was that new taxes would fund the move of medical scheme members to the public sector, in the form of a single NHI Fund, such that both public sector and medical scheme populations were covered in the same system – with net gains in coverage for both.
However, contrary to what was “correctly understood” from 1994 to the 2002 Taylor Commission, “the maths for such an approach, just does not add up”, said Van den Heever.
“The fastest way to de-segment the system is to allocate all new government revenues arising from economic growth to the people who need it most. This is not what the NHI proposals envisage. They want to dilute the public spend by trying to cover higher income groups. It is dangerous magical thinking that allows government to avoid dealing with the complex problems of the health system. Government needs to get back to its day job and do the heavy lifting needed to get our health system working again.”
Government response
Spotlight shared an earlier draft of this article with the National Department of Health for comment. While the department did not comment directly on mandatory health insurance, Foster Mohale, the department’s Director of Communications, emphatically reiterated their support for NHI and the NHI Act that was signed into law in May.
“There is no better time than now to reform South Africa’s health system. It is time to do away with the apartheid type of health system, and to reconfigure it into one that ensures that every South African gets the health care that they need, when they need, where they need and without incurring financial hardship. With the enactment of the NHI Act, the time for piecemeal approaches that retain benefits for the few and leave the majority to the whims of the market is no more,” Mohale told Spotlight.
He said that many countries, including Japan and the United Kingdom, have implemented health system reforms directed at achieving universal health coverage during times of crisis and low economic growth. “Therefore, to say that South Africa must sit and wait for some oracle numbers to emerge before instituting NHI is merely to argue that we must consciously let those that are carving profits and dividends from the anomalies that characterise our health system to continue. This is an irresponsible position that the Department cannot adopt as health is a constitutionally enshrined right for every South African, not just a privileged few,” he said.
On the questions of taxes, Mohale said: “We will not delve into the projected tax implications because we believe this is a matter that squarely falls under the purview of the National Treasury and the Minister of Finance. Suffice to say at the right time, and after necessary deliberations through formal government structures and processes, any information relating to this will be communicated to the public for comments prior to finalisation.”
Note: The 2002 Tailor report titled ‘Transforming the present – Protecting the future’ is not readily available online. There is this PDF version (unfortunately not searchable and with poor accessibility). For ease of use, we have created a Word version of the document that you can access here. Health is discussed in chapter 8.
A therapy showing promise to help control tuberculosis (TB) does not interfere with combined antiretroviral therapy (cART), according to research by Texas Biomedical Research Institute (Texas Biomed) which was recently published in JCI Insight.
“This is an important hurdle that this host-directed therapy had to clear in order to help patients battling both HIV and TB,” said study leader Professor Smriti Mehra, PhD of Texas Biomed.
TB is responsible for more than 1.3 million deaths worldwide every year. Dr. Mehra and her team have been investigating a therapy currently used in cancer as a potential treatment for patients with drug-resistant TB and/or comorbid HIV. While many cases of TB can be controlled with months of antibiotics, the infection can return in people who are immunocompromised as a result of HIV. Now that cART is so effective at controlling HIV, a resurging TB infection can often be deadly to those individuals.
Dr Mehra is studying a host-directed therapy that blocks or inhibits an immune system protein naturally found in the body. The protein, called IDO (short for Indoleamine-2,3-dioxygenase), normally suppresses the immune system, preventing it from causing excessive inflammation and organ damage. Inhibiting IDO for short intervals of time has led to more successful cancer treatments. Dr. Mehra’s team has previously shown the same approach improves control of TB in conjunction with antibiotics.
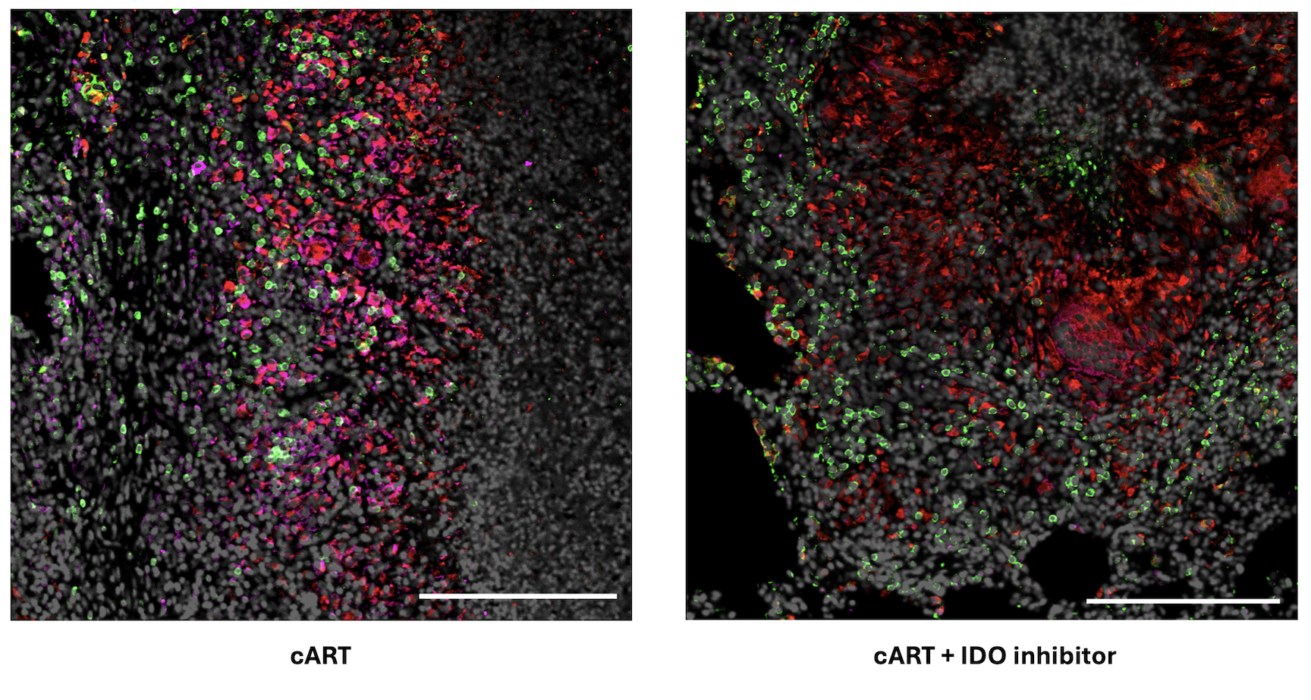
This current study in nonhuman primates with both TB and simian immunodeficiency virus, the nonhuman primate version of HIV, showed the IDO inhibitor does not interfere with cART.
Researchers compare the impacts of cART by itself versus cART plus the IDO inhibitor in lung tissue of nonhuman primates with both TB and SIV. Left: Following just cART, significantly more IDO is detected in pink. Right: With the IDO inhibitor and cART, immune cells recruited to fight bacteria are observed inside the granuloma, a hallmark structure of TB. Specifically, CD4+ T cells are in green and CD68 proteins expressed by macrophages are in red.
“There was no increase in viral load in animals given cART and the IDO inhibitor, compared with animals only given cART, proving the inhibitor is safe to give to patients with HIV,” Dr. Mehra said.
Now that the researchers have shown the inhibitor works well in conjunction with TB antibiotics and with cART separately, they plan to study how it performs when given in conjunction with both antibiotics and cART together. This treatment regimen is standard for patients with both HIV and active TB. Dr. Mehra said that longer-term studies are also needed to confirm there are no unintended side effects.
The IDO inhibitor is already FDA-approved for use in patients with cancer, which shortens the path to potential approval for patients with TB/HIV when compared with developing a brand-new drug.
A small University at Buffalo clinical trial has found that at low doses, lithium aspartate is ineffective in treating the fatigue and brain fog that is often a persistent feature of long COVID; however, a supplemental dose-finding study found some evidence that higher doses may be effective.
Published in JAMA Network Open, the study was led by Thomas J. Guttuso, Jr., MD, professor of neurology in the Jacobs School of Medicine and Biomedical Sciences at UB and a physician with UBMD Neurology.
“It’s a negative study with a positive twist,” Guttuso concludes.
Because long COVID is believed to stem from chronic inflammation and lithium has known anti-inflammatory actions, Guttuso had recommended that a patient of his try low-dose lithium for persistent long COVID symptoms. He was surprised when this patient reported a near full resolution of fatigue and brain fog within a few days of initiating lithium aspartate at 5mg a day.
Relief from symptoms
Based on this single case, Guttuso became interested in lithium aspartate as a potential treatment for long COVID and recommended it to other such patients.
According to Guttuso, 9 of 10 long COVID patients he treated with lithium aspartate 5-15mg a day saw very good benefit in terms of improvements to their fatigue and brain fog symptoms.
“Based on those nine patients, I had high hopes that we would see an effect from this randomized controlled trial,” says Guttuso. “But that’s the nature of research. Sometimes you are unpleasantly surprised.”
The randomised controlled trial showed no benefit from 10-15mg a day of lithium aspartate compared to patients receiving a placebo.
After one patient from the study subsequently increased the lithium aspartate dosage to 40mg a day and experienced a marked reduction in fatigue and brain fog symptoms, Guttuso decided to then conduct a dose-finding study designed to explore if a higher dose of lithium aspartate may be effective.
The three participants who completed the dose-finding study reported greater declines in fatigue and brain fog with the higher dose of 40-45mg per day. This was especially true in the two patients with blood lithium concentrations of 0.18 and 0.49mmol/L compared to one patient with a level of 0.10mmol/L who saw partial improvements.
“This is a very small number of patients, so these findings can only be seen as preliminary,” says Guttuso. “Perhaps achieving higher blood levels of lithium may provide improvements to fatigue and brain fog in long COVID.”
Dosage may be too low
He notes that it is possible the randomized controlled trial was ineffective because the dose of lithium aspartate that was used was too low.
“The take-home message is that very low dose lithium aspartate, 10-15 milligrams a day, is ineffective in treating the fatigue and brain fog of long COVID,” says Guttuso. “Perhaps we need to do another randomised controlled trial that uses higher lithium aspartate dosages that achieve blood lithium levels of 0.18-0.50mmol/L to determine if they could be effective.”
An estimated 17 million people have long COVID in the US, and worldwide the number is estimated at 65 million.
“There currently are no evidence-based therapies for long COVID,” says Guttuso. He hopes that the National Institutes of Health will view lithium as worth studying through a trial with higher dosages; the NIH is allocating an additional $500 million to study long COVID therapies that appear to be promising.
Guttuso adds that if a subsequent randomised controlled trial finds that higher dosages of lithium aspartate are effective, long COVID patients would still need to discuss taking it with their health care providers; in addition, he says, if they do begin taking it at higher dosages, blood lithium levels should be monitored.
Oestrogen, the major female ovarian hormone, can trigger nerve impulses within milliseconds to regulate a variety of physiological processes. At Baylor College of Medicine, Louisiana State University and collaborating institutions, researchers discovered that oestrogen’s fast actions are mediated by the coupling of the oestrogen receptor-alpha (ER-alpha) with an ion channel protein called Clic1.
Clic1 controls the fast flux of electrically charged chloride ions through the cell membrane, which neurons use for receiving, conducting and transmitting signals. The researchers propose that interacting with the ER-alpha-Clic1 complex enables oestrogen to trigger fast neuronal responses through Clic1 ion currents. The study appeared in Science Advances.
“Oestrogen can act in the brain to regulate a variety of physiological processes, including female fertility, sexual behaviours, mood, reward, stress response, cognition, cardiovascular activities and body weight balance. Many of these functions are mediated by oestrogen binding to one of its receptors, ER-alpha,” said co-corresponding author Dr Yong Xu, professor of pediatrics – nutrition and associate director for basic sciences at the USDA/ARS Children’s Nutrition Research Center at Baylor.
Fast and slow
It is well known that, upon stimulation by oestrogen, ER-alpha enters the cell nucleus where it mediates the transcription of genes. This classical mode of action as a nuclear receptor takes minutes to hours.
“Oestrogen also can change the firing activity of neurons in a manner of milliseconds, but it was not clear how this happens,” Xu said. “In this case, it did not make sense to us that the minutes-long nuclear receptor function of ER-alpha was involved in such a rapid action. We explored the possibility that ion channels, proteins in the cell membrane that regulate the fast flux of ions, mediated oestrogen’s quick actions.”
In the current study, working with cell lines and animal models, the team searched for cell membrane proteins that interact with ER-alpha. They found that protein Clic1, for chloride intracellular channel protein-1, can physically interact with ER-alpha. Clic1has been implicated in the regulation of neuronal excitability, so the researchers considered it a candidate to mediate oestrogen-triggered fast actions.
“We discovered that oestrogen enhances Clic1-mediated ion currents, and eliminating oestrogen reduced such currents,” Xu said. “In addition, Clic1 currents are required for oestrogen to induce rapid responses in neurons. Also, disrupting the Clic1 gene in animal models blunted oestrogen regulation of female body weight balance.”
The findings suggest that other nuclear receptors could also interact with ion channels, a possibility the researchers look forward to studying in the future.
“This study was conducted with female mice. However, Clic1 is also present in males. We are interested in investigating its role in male physiology,” Xu said.
Chloride channels are not as well studied as other ion channels, such as potassium, sodium or calcium channels. “We are among the first to study the role Clic1 plays in female physiology,” Xu said. “We hope that our findings will inspire other groups in the field to expand these promising investigations.”
Photo by Wendy Wei: https://www.pexels.com/photo/mother-breastfeeding-her-child-3074935/
A study led by researchers at the found that breast milk provides protection against rotavirus, a common gastrointestinal disease in infants. Babies whose mothers had high levels of specific antibodies in their breast milk were able to fend off the infection for a longer period than infants whose mothers had lower levels. The researchers also uncovered an unexpected relationship between BMI and antibody levels.
Published in the Journal of Clinical Investigation, the University of Rochester Medical Center-led study also found significant differences in antibody profiles in breast milk between mothers in high-income countries (HICs) and low- and middle-income countries (LMICs). Researchers analysed human milk samples from 695 women in Finland, the US, Pakistan, Peru, and Bangladesh, and measured specific IgA and IgG antibodies, which are common antibodies produced in breast milk, against 1607 proteins from 30 pathogens.
The research, led by Dr Kirsi Jarvinen-Seppo, MD, PhD, professor at UR Medicine Golisano Children’s Hospital (GCH), tracked antibody levels and kinetics over time to analyse antibody responses to a wide range of respiratory, diarrhoeal and sepsis pathogens in human milk. The primary aim of the study, funded by the Bill and Melinda Gates Foundation, was to understand the protective properties of these antibodies and how they vary across different geographic and economic regions.
“We would expect to find differences in antibody levels in different countries, due to different diseases circulating among areas of the world, but this is one of the first times that there’s been a head-to-head comparison for dozens of pathogens across several continents,” said Jarvinen-Seppo. “It was encouraging to see such a clear link between higher antibody levels and a delay to rotavirus infection, and this was consistently observed among an independent validation cohort.”
Other notable findings from the study:
Milk from women in LMICs had higher levels of IgA and IgG antibodies against various intestinal and respiratory pathogens compared to milk from HICs. This difference was particularly notable for pathogens such as Shigella and pneumococcus, which are major contributors to morbidity and mortality in young children.
Higher body mass index (BMI) was associated with lower antibody levels, which went against expectations.
“The variation in antibody profiles between regions highlights the impact of economic and environmental factors on maternal immunity,” said Jarvinen-Seppo.
In addition to Rotavirus findings, the discovery that a higher BMI was associated with lower antibody counts in breast milk was also unexpected.
“We had anticipated that underweight mothers might have lower antibody levels due to poorer nutritional status,” said Jarvinen-Seppo. “Due to rising obesity rates worldwide, this could be a significant finding, but this is preliminary and additional research is needed since this is the first time this has been measured.”
“While the data on rotavirus protection is compelling, the geographical and BMI-related variations highlight areas where further research is essential. The study sets the stage for additional investigations that could lead to better understanding and interventions for improving infant health globally,” said Jarvinen-Seppo.
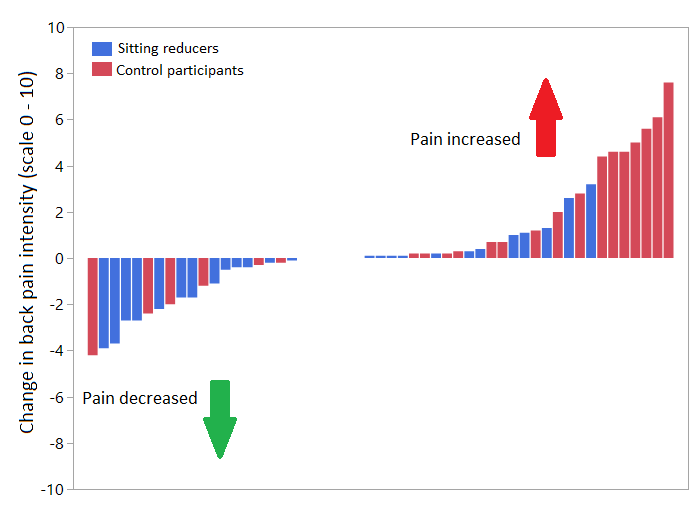
A new study from the University of Turku showed that reducing daily sitting prevented back pain from worsening over six months. The results, published in BMJ Open, strengthen the current understanding of the link between activity and back pain as well as the mechanisms related to back pain.
Intuitively, it is easy to think that reducing sitting would help with back pain, but previous research data is surprisingly scarce. The study from the Turku PET Centre and UKK Institute in Finland investigated whether reducing daily sitting could prevent or relieve back pain among overweight or obese adults who spend the majority of their days sitting. The participants were able to reduce their sitting by 40 min/day, on average, during the six-month study.
“Our participants were quite normal middle-aged adults, who sat a great deal, exercised little, and had gained some extra weight. These factors not only increase the risk for cardiovascular disease but also for back pain,” says Doctoral Researcher and Physiotherapist Jooa Norha from the University of Turku in Finland.
Previous results from the same and other research groups have suggested that sitting may be detrimental for back health but the data has been preliminary.
The figure presents the change in back pain intensity on a scale from 0 to 10. The blue bars represent individuals in the intervention group that reduced sitting and the red bars represent the control participants who did not change their sitting habits. Most of the participants in the intervention group decreased their back pain whereas the back pain in the control participants tended to increase.
Robust methods for studying the mechanisms behind back pain
The researchers also examined potential mechanisms behind the prevention of back pain.
”However, we did not observe that the changes in back pain were related to changes in the fattiness or glucose metabolism of the back muscles,” Norha says.
Individuals with back pain have excessive fat deposits within the back muscles, and impaired glucose metabolism, or insulin sensitivity, can predispose to pain. Nevertheless, back pain can be prevented or relieved even if no improvements in the muscle composition or metabolism take place. The researchers used magnetic resonance imaging (MRI) and PET imaging that is based on a radioactive tracer to measure the back muscles.
“If you have a tendency for back pain or excessive sitting and are concerned for your back health, you can try to figure out ways for reducing sitting at work or during leisure time. However, it is important to note that physical activity, such as walking or more brisk exercise, is better than simply standing up,” Norha points out.
The researchers wish to remind that switching between postures is more important than only looking for the perfect posture.