
New ‘Quantum Glass’ Improves X-ray Resolution with Less Radiation
A glass screen that moulds to the patient could allow more comfortable mammograms
X-rays allow professionals to diagnose injuries or ailments and peer inside suitcases at the airport, along with a variety of other applications. A team reporting in ACS Energy Letters has improved the glass screen that “translates” between X-rays and visible light, creating an X-ray system that produces high-resolution images with less radiation – it even works underwater. The screen can be moulded into curved shapes, a feature that could one day lead to more comfortable mammograms.
“Because our glass screens are highly efficient at converting X-rays into visible light, they can capture diagnostic images using less radiation.”
Osman Bakr. corresponding author of the paper
A screen made of glass, called a scintillator, catches X-rays that pass through an object and converts them into flashes of visible light, explains Osman Bakr, one of the paper’s corresponding authors. “The more efficient the scintillator is at this conversion, the clearer the final digital image becomes and the lower the dose of radiation required to create it,” he adds.
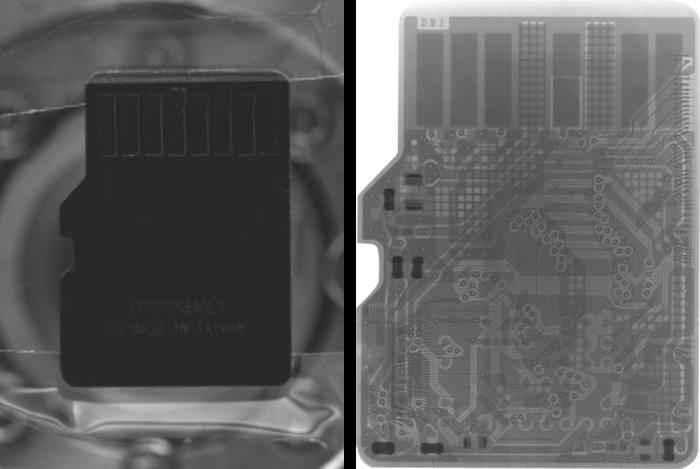
To improve the efficiency of glass-based scintillators, Bakr, Mehmet Bayindir and colleagues combined nanoclusters of copper, iodine, and an organic ligand into the glass. Then they formed their new glass into screens and captured X-ray images of a memory card and a bug, revealing intricate details within.
“By designing these materials from the bottom up, we’ve created a ‘quantum glass’ that occupies the perfect sweet spot between molecules and nanocrystals,” explains Bayindir. Bashir Hasanov, the first author of this study, adds that “this allows the screen to be as moldable as plastic while maintaining the high-performance imaging capabilities of a rigid crystal, opening a new frontier for three-dimensional X-ray diagnostics using curved surfaces.”
The presence of water typically makes X-ray imaging extremely challenging. However, the new, highly efficient scintillator captured a very clear scan of a fish’s tail in water. In fact, the image was indistinguishable from an image taken in air.
Another property of the new nanocluster glass is that when heated to 42 degrees Celsius, it becomes almost rubbery, allowing the researchers to form a curved screen. This could allow future researchers to create X-ray imaging systems that curve to fit a person’s anatomy – a major drawback of current mammography machines, which require breast tissue to be compressed between flat panels for a proper scan.
“We hope to mitigate the physical discomfort of life-saving screenings like mammography, encouraging more consistent patient participation,” says Bakr. “Because our glass screens are highly efficient at converting X-rays into visible light, they can capture diagnostic images using less radiation.” The researchers anticipate that the advances in this work could pave the way for safer, more frequent screenings that can start earlier, helping to catch cancer at an earlier stage.
Source: EurekAlert!








