Researchers at McGill University have developed a rapid way to engineer blood clots that stop severe bleeding and support tissue healing more effectively. Their technique, called “click clotting,” links red blood cell surface proteins through a chemical reaction, resulting in a biocompatible clot that is 13 times more resistant to fracturing and four times more adhesive than natural blood clots. The team said the method, described in Nature, could be used to develop life-saving biomaterials to help control severe bleeding, as well as benefit people with clotting disorders.
“Natural blood clots can be slow to form and mechanically fragile, which limits their ability to stop severe bleeding and can compromise healing,” said Jianyu Li, senior author and Professor of Mechanical Engineering and Canada Research Chair in Tissue Repair and Regeneration. “Our work shows that, when engineered appropriately, red blood cells can play a central structural role, enabling the design of stronger and more functional biomaterials.”
Shuaibing Jiang led the research during his PhD studies at McGill. He is now a Postdoctoral Associate at Mass General Brigham and Women’s Hospital, Harvard Medical School.
Researchers at the University of British Columbia, the Medical College of Wisconsin, the University of Colorado Boulder, the University of Toronto, and the Versiti Blood Research Institute also contributed.
Connected by chemical reaction
Previous efforts to crosslink red blood cells used chitosan, a polymer derived from crustacean shells, but these led to brittle clots, ruptured cells and inconsistent clotting. In “click clotting,” the clot structure is fundamentally strengthened through a fast, bio-safe chemical reaction that connects proteins on the red blood cell surface, forming a solid gel in just five seconds.
Because the “click” reaction doesn’t interfere with normal blood chemistry, it can work alongside the body’s natural clotting process. As a result, the artificial cell‑based gel, called a “cytogel,” can be added to whole blood, where it becomes embedded within the body’s own fibrin clot.
“The technology enables both autologous clots (using the patient’s own blood) and allogeneic clots (using type-matched donor blood). Autologous clots can be prepared in approximately 20 minutes, while allogeneic clots can be prepared within about 10 minutes. Given typical clinical time constraints, this approach has strong potential for in-patient emergency care, wound management and related settings,” Li said.
The results were confirmed through in vitro testing, as well as by testing on rodents. A highlight was the effective healing and regeneration observed in the injured liver, with performance exceeding that of the clinically used product tested in this study. Analysis showed minimal evidence of immune reactivity and no toxicity in major organs.
Further research required
The researchers say that while further study is required before the cytogel can be used in clinical settings, the research establishes a foundation for its design and application.
“Engineered blood clots have strong potential for broad clinical use and could improve outcomes across many medical situations,” Li said.
Sports injuries are common at all levels, from recreational athletes to elite professionals. Radiology not only helps diagnose injuries but also assists in monitoring recovery, identifying complications early and helping determine when it is safe to return to sport.
Dr Ewoudt van der Linde, a radiologist at SCP Radiology specialising in musculoskeletal (MSK) imaging and sports injuries, discusses common injuries, imaging techniques and the role radiology plays in modern sports medicine.
What is the role of a radiologist in sports injuries?
Radiologists work as part of a multidisciplinary medical team. Imaging helps distinguish between minor and more significant injuries, such as differentiating a low-grade muscle strain from a major tear or identifying ligament injuries that may require surgery.
Imaging also guides treatment decisions and, in selected cases, can be used to monitor healing and recovery, particularly in high-performance athletes.
Are there specific sports that produce distinctive injury patterns?
Yes. Running and field sports commonly result in muscle strains, ligament injuries and stress fractures. Sports involving rapid changes in direction, such as rugby or football, are often associated with knee ligament injuries and ankle sprains.
Padel, tennis and golf frequently produce overuse injuries involving tendons around the shoulder, elbow and wrist, while running and jumping sports commonly affect the Achilles tendon.
Are there particular sports injuries commonly seen in practice?
Common injuries include muscle strains, ligament sprains, tendon injuries and stress-related bone injuries. In the lower limb, ankle sprains, Achilles tendon pathology and knee ligament injuries are frequently encountered. In the upper limb, shoulder and elbow tendon injuries are common, particularly in throwing or racquet sports.
What imaging is used in sports injuries and why?
Different imaging techniques are used depending on the suspected injury:
X-rays are often the first step when a fracture or dislocation is suspected.
Ultrasound is useful for assessing tendons, muscles and soft tissues, and can also guide injections.
MRI provides detailed evaluation of ligaments, cartilage, muscles, tendons and bone marrow.
CT scans are mainly used for complex fractures or detailed bone assessment.
Is imaging important even if an injury does not seem serious?
Yes. Some injuries may appear minor but can involve underlying damage such as stress fractures, small ligament tears or early cartilage injury. Early detection may prevent worsening injury and reduce long-term complications.
Is pain a good indicator of injury severity?
Not always. Some serious injuries may initially cause only mild discomfort, while relatively minor conditions can be very painful.
How do stress fractures differ from acute or occult fractures?
Acute fractures usually occur after sudden injury and are often visible on X-rays.
Stress fractures develop gradually due to repetitive strain and may only be visible on MRI in the early stages.
Occult fractures are not seen on initial X-rays despite ongoing symptoms and may require MRI or CT for diagnosis. Early diagnosis is important to prevent progression to a complete fracture.
Can imaging distinguish between inflammation, overuse injuries and structural damage?
Yes. Imaging can help differentiate between low-grade inflammation or overuse changes and more significant injuries such as tendon tears, ligament ruptures or cartilage damage. This distinction is important because treatment and recovery timelines differ significantly.
Can imaging help predict recovery time and return to sport?
Imaging cannot provide an exact recovery timeline but does provide valuable information about the severity and extent of injury. In selected cases, imaging may also be used to monitor healing and assist with return-to-play decisions.
Can you discuss concussion briefly?
Concussions are common in sports such as rugby and are primarily a clinical diagnosis. Imaging is usually not required in mild cases. However, CT scans may be performed when there are concerning symptoms to exclude more serious injuries such as a brain bleed or skull fracture.
What role does Interventional Radiology play in sports injuries?
Interventional Radiology involves minimally invasive procedures performed under imaging guidance. In sports medicine, this may include image-guided injections for pain relief or aspiration of fluid collections. These procedures are typically performed using ultrasound or CT guidance and are generally less invasive than surgery.
Are there any new imaging techniques particularly useful in sports medicine?
Modern MRI techniques continue to improve and provide increasingly detailed evaluation of soft tissues, allowing earlier detection of subtle injuries. Ultrasound technology has also advanced significantly, with higher-resolution imaging and expanded use in both diagnosis and image-guided procedures.
Why is specialised MSK imaging important?
Sports injuries often involve complex anatomy and subtle findings. Subspecialised MSK radiologists develop expertise in recognising injury patterns and understanding sport-specific demands, helping provide more accurate diagnoses and clinically relevant reporting.
From unregulated weight loss injections to unsafe pain tablets, substandard and falsified medical products pose a threat to the health of people. Spotlight reports on how regulators are fighting the problem in South Africa.
“I know that there is a risk, but at this point I feel that the benefits outweigh everything else,” says Anna*, who buys unregulated medicine on the black market.
She was prescribed GLP-1 RA medicines by a doctor after being tested for insulin resistance. She has lost around 30kg and says the positive impact on her body, life, and self-esteem has been massive. GLP1 RAs (Glucagon-Like Peptide-1 Receptor Agonists) medicines, sold under brand names like Ozempic and Mounjaro, are increasingly used for weight loss and to prevent and/or treat diabetes.
When global shortages affected GLP-1 RA stocks in local pharmacies, Anna started buying similar drugs directly from unregistered sellers. For around R1 650, a fancy-looking box with a three-month supply of injections is delivered to her in a small cooler box. “I knew then already that what I was buying was unregulated and potentially inferior or even dangerous,” she says, adding, “but I was finally starting to feel good about myself.”
Apart from being aware that the unregulated drugs could potentially harm her, Anna says she found that the regulated products were often out of stock, expensive, and came with stigma from pharmacists who quizzed her on whether she deserved the products. “If I could have kept doing it the proper way, I would have, but there were just too many obstacles,” she says.
Defining the problem
Weight-loss medicines are only one of several types of health products that are frequently purchased outside of formal channels, according to the South African Health Products Regulatory Authority (SAHPRA).
“Commonly affected products include painkillers, antibiotics, weight-loss and sexual enhancement products, skin-lightening products, and some chronic medicines,” Mokgadi Fafudi, SAHPRA’s manager of regulatory compliance, tells Spotlight.
“Combating the threat of substandard and falsified medical products is one of the urgent global challenges of this decade,” says Faridun Nazriev, the external relations and communications officer at the World Health Organization (WHO) Country Office in South Africa.
“Substandard products are those that do not meet quality standards and specifications, often due to poor manufacturing practices or inadequate quality control. Falsified medical products deliberately misrepresent their identity, composition or source”, according to the WHO. These products, it adds, are often created and distributed with the intent to deceive consumers for financial gain.
Two other definitions should not be confused with these, cautions Dr Andy Gray, a senior lecturer in Pharmacology at UKZN and co-director of the WHO Collaborating Centre for Pharmaceutical Policy and Evidence-Based Practice.
Compounded medicines are custom formulations that may be specific to a patient, but are generally not registered by SAHPRA.
Generic medicines are those that have been tested and found to be as safe and effective as originator medicines, but are generally cheaper. Generic medicines on the market have been approved by SAHPRA and are not in any way substandard.
Gray says the term counterfeit is no longer used by the WHO, because it refers specifically to breaches of intellectual property, like trademarks.
Lack of data
While the WHO estimates that 1 in 10 medicines in low-and middle-income countries are substandard or falsified, all regions are affected and have been seeing an increase, according to a 2024 report from the WHO’s Global Surveillance and Monitoring System.
South Africa also appears to have rising rates. SAHPRA’s 2021/2022 annual report notes that 101 health product quality complaint reports were filed. In 2022/23, that figure nearly tripled to 297.
Fafudi says that the organisation received 588 reports of possible non-compliance in the 2024/2025 year. She says that for the 2025/26 year, this number exceeds 570 cases, though this has not yet been published by SAHPRA.
But such reports are likely only the tip of the iceberg. Gray laments that we don’t have the full picture of how big the problem of substandard and falsified medical products really is.
This is partly because, by its very nature, the sale of substandard and falsified medicines is usually hidden. Fafudi says that these medicines are often sold through informal markets, unregulated outlets, online platforms, and cross-border smuggling networks.
Gray adds that these medications aren’t necessarily always sold through informal means. “They may be infiltrated into wholesalers or state medicine depots, and then distributed,” he says, “Or they may be sold directly to pharmacies or prescribers and then sold to patients.”
A threat to patients
As in Anna’s experience with GLP-1 RAs, there is often a demand for unregulated products because the properly regulated products can’t meet the public demand.
Fentse Maseko, who works in the Department of Pharmacology and Pharmacy at Wits University, researched this issue in her Master’s thesis and advocates in the space. She notes that in many low- and middle-income countries, particularly in remote and underserved areas, limited access to medicines may force patients to seek treatment from informal markets. She adds that in South Africa, porous borders and rising costs also play a role.
Whatever the reasons behind their proliferation, the risks to the healthcare system and individuals are multi-faceted.
“Substandard and falsified medicines are a serious threat to patient safety and public trust,” says Refiloe Mogale, the executive director for the Pharmaceutical Society of South Africa (PSSA). “These products can lead to treatment failure, harm, or even death.”
Maseko warns that it can also add to the growing problem of antibiotic resistance if antibiotics are substandard. It can also strain the healthcare system when second or third-line treatments are needed for issues initially addressed with unregulated products, or caused by them.
The role of the regulator
The main body in South Africa responsible for regulating substandard and falsified medicines is SAHPRA. Fafudi explains that they conduct post-market surveillance and inspections, run a whistleblower reporting system, manage product recalls, and monitor illegal advertising and online sales.
SAHPRA also works with specialised units in the South African Police Service as well as other stakeholders such as customs to enforce joint operations. Fafudi says such joint operations have been conducted on at least a monthly basis.
There are also legal actions, including issuing warnings, seizing or destroying products and criminal prosecution. According to the Medicines and Related Substances Act 101 of 1965, fines or prison sentences not exceeding 10 years may be prescribed.
The PSSA however charges that not enough is being done. “Key gaps are visible in insufficient regulatory capacity, weak border control, limited enforcement scale and the under-resourced National Action Plan,” Mogale says. “The system is overwhelmed by the speed and sophistication of the problem.”
Reporting unregulated products
The public can help address the problem of substandard and falsified medicines. SAHPRA advises buying only from licensed and authorised pharmacies and healthcare providers.
“Be cautious of unusually low prices, miracle cure claims, and poor packaging,” Fafudi warns. “Always check packaging, expiry dates, and consult healthcare professionals before use.”
Suspicious products or sellers can be reported on the SAHPRA website.
Jas Bhana, Chief Executive Officer of the Innovative Pharmaceutical Association of South Africa, adds that the public can also report suspicious products to the National Department of Health or their nearest pharmacy. “Combating this threat requires collective vigilance to safeguard every patient’s right to safe, quality, and effective medicines,” she says.
This goes hand-in-hand with the need for consumers to know the dangers, Maseko explains. “While public education plays an important role in mitigating this risk, effective risk communication remains a challenge, particularly in communities with limited health literacy,” says Maseko.
On a bigger scale, Nazriev explains that the WHO prioritises prevention, detection, and response as the main pillars of action. This includes local regulation as well as collaboration between countries.
“Given the transnational nature of globalised medical product supply chains as well as criminal networks, collaborating across borders and sectors is essential to national, regional and global responses,” he says.
Better regulation
Gray acknowledges that there is a challenge in budgets and laboratory capacity, but even so he calls for more to be done. “SAHPRA needs to move from a largely reactive stance to a more proactive one, sampling medicines from the distribution chain and submitting them for checking, and then report to the public on their findings,” he suggests.
The PSSA recommends implementing a national medicine registry with a track-and-trace system and stricter control of online medicine sales, including mandatory certification and monitoring.
SAHPRA is already planning along some of these lines. “Future plans include strengthening supply chain traceability, enhancing detection systems, regulating online medicine sales, and increasing public awareness campaigns,” says Fafudi.
Part of this direction comes from a National Action Plan (NAP), launched late last year by SAHPRA, with support from the National Department of Health and the WHO.
“All actors within the supply chain, particularly at key pinch points in both the public and private sectors, must be equipped with the knowledge, skills, and equipment to identify and report suspicious products to SAHPRA,” Health Minister Dr Aaron Motsoaledi is reported to have said at the launch of the NAP. “All activities should mitigate the risk of substandard and falsified medical products. This includes increased vigilance at ports of entry, through to post-market surveillance of high-risk products, inspection of manufacturers, distributors and wholesalers.”
Whether all this will be done, and what it will mean for people like Anna who knowingly choose to use unregulated medicines, remains to be seen.
According to recent data from the Global Bipolar Cohort, only 29% of people with bipolar disorder are prescribed lithium. Despite being the “gold standard” for treating this mental health condition, we often prioritise perceptions over scientific reality, and neglect the best available treatment.
Lithium is not some complex molecule synthesised in a state-of-the-art laboratory. It is just an element, the third in the periodic table, and ever since the Australian psychiatrist John Cade discovered its therapeutic properties in 1949, it has maintained a relevance that no other psychotropic drug has been able to match.
This longevity is not a relic of the past, but a reflection of its clinical robustness. Despite decades of research and the constant emergence of new drugs, no alternative has shown comparable efficacy in the long-term prevention of manic and depressive episodes in bipolar disorder.
According to a review published in 2024, lithium is still “the mainstay treatment of mood disorders in general and in bipolar disorder specifically”. It is also the benchmark against which all other treatment options are compared, both for stabilising mood and reducing the risk of relapse.
It is the only mood stabiliser with proven efficacy in treating mania and depression, as well as in preventing relapses. Furthermore, recent studies confirm that it may also have neuroprotective properties, from the modulation of cellular pathways involved in neural plasticity to potential effects in preventing mild cognitive impairment and dementia.
These characteristics explain why international guidelines still rank it as the first-line treatment for bipolar disorder. A consensus published in 2025 stated that it should be prescribed more frequently, contrary to the unfounded reservations that still persist in clinical practice.
Suicide reduction
Above all, there is one aspect that sets lithium apart from other psychopharmaceutical drugs: its ability to reduce the risk of suicide. No other medication has demonstrated such a consistently protective effect.
A 2024 review highlighted that, despite the methodological difficulties in studying this statistically rare event, the body of evidence from clinical trials, observational studies and meta-analyses all points in the same direction: lithium reduces mortality and suicide attempts.
This is likely due to its ability to reduce impulsivity, stabilise extreme mood swings and prevent depressive relapses, all of which create the moments of greatest risk.
Beyond episodic treatment
Current research is also looking into lithium’s ability to alter the course of bipolar disorder. Not only does it stop episodes, but it also protects the brain, and evidence suggests that, unlike some antipsychotics, it improves brain connectivity and preserves verbal fluency.
In fact, there is very interesting data suggesting that it could reduce the risk of dementia by up to 50%. Even residual levels in drinking water appear to have a protective effect at a population level. Lithium is, in short, a molecule with exceptional neuroprotective potential.
But the neuroprotective effects do not stop there. Recent studies also suggest that lithium stimulates the production of brain-derived neurotrophic factor, a protein essential for neuronal survival and growth that is often reduced in patients with bipolar disorder.
In other words, it doesn’t just prevent the brain from deteriorating – it actively helps it to heal.
Blood monitoring and ‘precision medicine’
It is often argued that the need for blood tests to monitor lithium levels (the optimal therapeutic range is 0.6-0.8 millimoles per litre) is an inconvenience. However, from a rigorous clinical perspective, this monitoring is a safeguard, not a risk. It is what allows the dose to be adjusted to the exact biology of each patient, a form of “precision medicine” that we were already practising long before the term became fashionable.
We should also remember that many commonly used medicines – from anticoagulants to immunosuppressants – require the same kind of laboratory monitoring, yet they are not considered dangerous for that reason.
What lithium management requires is not fear, but rigour. So why is it prescribed less often? The answer is complex. It is partly due to pressure from the pharmaceutical industry to promote new, patentable molecules – lithium, being a natural element, cannot be patented. There is also a degree of clinical reluctance due to its narrow therapeutic window – it needs to be carefully controlled to ensure a safe yet effective dose.
However, international guidelines are clear: lithium should be the first choice. We cannot overlook it in favour of less effective alternatives simply because they appear more modern. This kind of mistake should not influence clinical practice.
Newer is not always better
Good psychopharmacology is not a question of chasing the latest developments, but of using the most appropriate treatment for each individual at every stage of their illness.
Lithium has a proven track record that spans decades, across areas that no other mood stabiliser can address simultaneously. It controls manic and depressive episodes, prevents suicide, and provides active neuroprotection. Three areas, in one single drug.
This does not mean it is right for absolutely everyone. Good psychopharmacology should always push back against fads and dogma alike, but discarding lithium’s use without ever seriously considering it deprives patients of an option that is, according to the evidence, categorically the best therapeutic option.
Our challenge today is not to reinvent the wheel, but to understand how best to use the therapeutic tools we already have. A drug doesn’t become outdated just because time has passed; it becomes outdated when new evidence emerges and supersedes it. In the case of lithium, new evidence only confirms its value.
Current exercise guidelines are too low, suggest researchers
Photo by Ketut Subiyanto on Pexels
Adults should aim to do between 560 and 610 minutes a week of moderate to vigorous physical activity to achieve a substantial reduction in the risk of heart attacks and stroke, suggest the findings of an observational study published online in the British Journal of Sports Medicine.
This is between 3-4 times higher than the current public health recommendation that adults do at least 150 minutes a week of moderate to vigorous physical exercise such as brisk walking, running or cycling.
People who are less fit need to do slightly more exercise than those who are very fit to get the same cardiovascular benefits, the study suggests.
The researchers say that the current one-size fits-all advice on exercise may need to be changed and replaced with personalised targets according to an individual’s fitness level.
Cardiorespiratory fitness varies greatly and is a strong predictor of cardiovascular health. Low cardiorespiratory fitness is strongly associated with an increased risk of heart attacks, strokes and early death, the researchers point out.
A simple way to assess cardiorespiratory fitness is by measuring VO2 max – the maximum rate of oxygen the body consumes and uses during intense exercise. This measures how efficiently the heart, lungs and muscles deliver and use oxygen.
Less fit individuals need to do more exercise to get the same benefits
Researchers from Macao Polytechnic University, China, set out to look at how both exercise levels and cardiorespiratory fitness, as measured by VO2 max, affected the risk of cardiovascular disease.
The study included data from 17 088 people who were taking part in a UK Biobank study between 2013 and 2015. The average age was 57 years and 56% were female and 96% were white.
The study participants wore a device on their wrist for seven consecutive days to record their typical exercise levels and had completed a cycle test to measure their estimated VO2 max.
Data on smoking status, alcohol intake, self-related health and diet, body mass index, resting heart rate and blood pressure were also included in the analysis.
During an average follow up period of 7.8 years, there were 1233 cardiovascular events, including 874 atrial fibrillation, 156 myocardial infarction, 111 heart failure and 92 stroke events.
Those adults who met the 150 minute a week guideline on exercise experienced a modest 8-9% reduction in cardiovascular risk, the study found. This was consistent across all levels of fitness.
In order to achieve substantial protection, classed as a greater than 30% risk reduction, between 560 and 610 minutes of moderate to vigorous exercise a week was needed. However, this level of exercise was only achieved by 12% of people in the study.
The analysis found that those individuals with the lowest fitness needed approximately 30-50 additional minutes per week compared with those with high fitness to achieve equivalent benefits.
For example, to achieve a 20% reduction in the risk of cardiovascular events, 370 minutes of moderate to vigorous exercise was needed for those at the lowest fitness compared to 340 minutes for those at the highest fitness levels.
The researchers say, “This finding highlights the steeper challenge faced by deconditioned populations.”
This is an observational study and as such no firm conclusions can be drawn about cause and effect. The researchers acknowledge that the study group could have been healthier and fitter than the general population. Another limitation was that cardiorespiratory fitness was estimated and sedentary time or less vigorous exercise was not measured.
The researchers say their findings confirm that current guidelines provide a robust universal minimum for cardiovascular protection. But they add that there should be stratified advice to help guide motivated patients to do more to protect their heart health.
“Future guidelines may need to differentiate between the minimal moderate to vigorous exercise volume required for a basic safety margin and the substantially higher volumes necessary for optimal cardiovascular risk reduction,” they conclude.
A research project led by the Institute for Research in Nutrition and Food Safety (INSA) and the Faculty of Pharmacy and Food Sciences at the University of Barcelona, together with the Molecular Biology Institute of Barcelona (IBMB) of the CSIC (which stands for Consejo Superior de Investigaciones Científicas), has successfully designed and tested a gluten-degrading molecule that is a promising ally in the management of coeliac disease, an autoimmune disease whose symptoms are triggered by the consumption of gluten and other prolamins found in cereals. At present, there is a complete lack of treatment options beyond a diet free from gluten, which is difficult to maintain in Western societies where diets rely heavily on wheat products.
The major breakthrough is that the molecule is effective at very low concentrations and at a pH of 2 (the pH of the stomach) a condition that none of the molecules currently available or under development had previously achieved with efficiency. Although some of them are marketed as nutritional supplements, they are not an effective alternative to gluten-free diets.
The study has been published in the journal EMBO Molecular Medicine ahead of the International Day of Coeliac Disease on 16 May and is led by researchers Francisco J. Pérez-Cano (INSA-UB), and F. Xavier Gomis-Rüth (IBMB-CSIC). The co-first authors are Marina Girbal-González and Arturo Rodríguez-Banqueri (INSA-UB and IBMB-CSIC, respectively). Teams from the Institute for Food Science Research (CSIC-UAM), the University of Salzburg (Austria) and the Technical University of Munich (Germany) have also participated.
Counteracting the ‘trigger’ of coeliac disease
The trigger for coeliac disease are the prolamins, proteins found in most common cereals in our diet, such as wheat gluten. When these are digested in the stomach, they break down into smaller fragments (peptides). Some of these can be toxic, such as the gluten immunogenic peptides (GIPs), which can withstand the stomach’s gastric acids and reach the small intestine. Among these, one of the most immunogenic is the the ‘33-mer’, a fragment of the α-gliadin in wheat gluten that is highly immunogenic.
This poses a problem for people with coeliac disease, because once in the small intestine, the 33-mer and other GIPs bind particularly easily to a receptor of the immune system (the human leukocyte antigen, or HLA), triggering the inflammatory autoimmune response that causes the characteristic symptoms of the disease.
The results demonstrate that celiacase, a molecule stable in the stomach environment, could be an adjunctive therapeutic candidate to support a gluten-free diet.
Four years ago, the Proteolysis Group at IBMB-CSIC, led by F. Xavier Gomis-Rüth, described in an article in Nature Communications that nephrosin – a molecule found naturally in the digestive juices of the carnivorous plant Nepenthes ventrata – was capable of cleaving GIPs, building on results from the group of David Schriemer from the University of Alberta in Canada. In collaboration with the Autoimmunity, Immunonutrition and Tolerance Group at the UB’s Faculty of Pharmacy and Food Sciences, led by Professor Francisco José Pérez-Cano, they demonstrated that nephrosin can degrade the 33-mer peptide and other GIPs before they reach the intestine, thereby potentially preventing this autoimmune inflammatory response.
Designed using molecular engineering
In this study, the team has designed and tested a molecule based on nephrosin. Named celiacase, this new molecule exhibits its maximum activity at the gastric pH of the stomach, where, in synergy with the pepsin in our digestive system, it breaks down the GIPs in cereals and the gliadin in wheat before they pass into the duodenum.
“There are other proteases, generically termed glutenases, which break down gluten, but they are not fully active at pH 2 – the pH of the stomach – but rather at pH 7 – the pH of the duodenum – when the bolus has already left the stomach,” explains Gomis-Rüth. “Therefore, it is necessary to increase the doses to levels that make them unviable for therapeutic use.”
The team has tested the molecule in vivo using a mouse model developed by the University of Chicago, which is currently the model that most accurately replicates coeliac disease. The results show that celiacase is effective at very low doses, being able to mitigate the symptoms of the disease in gluten-fed mice, even at high gluten intake levels. “Intestinal atrophy, inflammation, the antibody response and dysbiosis – that is, the alteration in the composition of the microbiota – were reduced,” says Pérez-Cano. “Furthermore, immunoregulatory markers were restored to normal levels, as were microbial metabolic pathways.”
Another advantage of celiacase is that it is no longer active once it reaches the duodenum. “Once it has accomplished its function, there is no need for it to remain active, so that it does not interfere with other proteins in the body,” adds Gomis-Rüth.
The molecule and its potential applications have been patented, and the team is taking the first steps towards setting up a spin-off company and taking the development to more advanced stages.
This study has been partially funded by programmes run by the Ministry of Science and Innovation, the Government of Catalonia’s Agency for Management of University and Grants (AGAUR) AGAUR, the Catalan Coeliac Association, and the CSIC’s Conexión Trigo network.
Researchers have discovered why influenza can lead to life-threatening complications during pregnancy.
Source: Pixabay CC0
In most people, influenza stays in the upper respiratory tract – mainly the nose – and clears without spreading further. But during pregnancy, the virus can extend beyond the lungs into the cardiovascular system, increasing the risk of severe complications for mothers and babies.
Now a new preclinical study using animal models reveals precisely why the virus can spill into the bloodstream during pregnancy, opening the door for targeted treatment. The study is a bilateral partnership between Trinity College Dublin, with collaborators from RMIT University and the University of Adelaide and is published in Science Advances.
Researchers identified a viral sensor in the immune system, known as TLR7, that can become overactive during pregnancy, amplifying inflammation and spreading disease into the bloodstream.
Blocking TLR7 could help prevent the harmful inflammation that makes flu in pregnancy so dangerous. This work can help protect developing babies by stopping the placenta from becoming overly inflamed during flu infection.
Professor John O’Leary, School of Medicine, Trinity, said: “This international research is of high impact in relation to our understanding of viruses and pregnancy and the role of the maternal immune response.”
What is the potential impact of this research?
Earlier studies from RMIT have shown that severe flu in pregnancy can have long‑term impacts on babies’ brain development, by inflaming blood vessels and reducing the flow of oxygen and nutrients from mother to baby.
This new study pinpoints the underlying cause of that damage, reshaping our understanding of flu‑related risk in pregnancy and opening the door to more targeted therapies.
RMIT co-lead author, Prof. Stavros Selemidis, said future treatments could focus on the immune system rather than the virus itself.
“Our study shows that in pregnancy, the problem isn’t just the flu virus – it’s the immune system overreacting. That’s where future treatments could really make a difference,” he explained.
“We’re ready to work with partners to help develop the next generation of therapies and clinical guidelines.”
Next steps for this work: The team is planning further research on how to target TLR7 to reduce the risk of severe influenza and pregnancy complications.
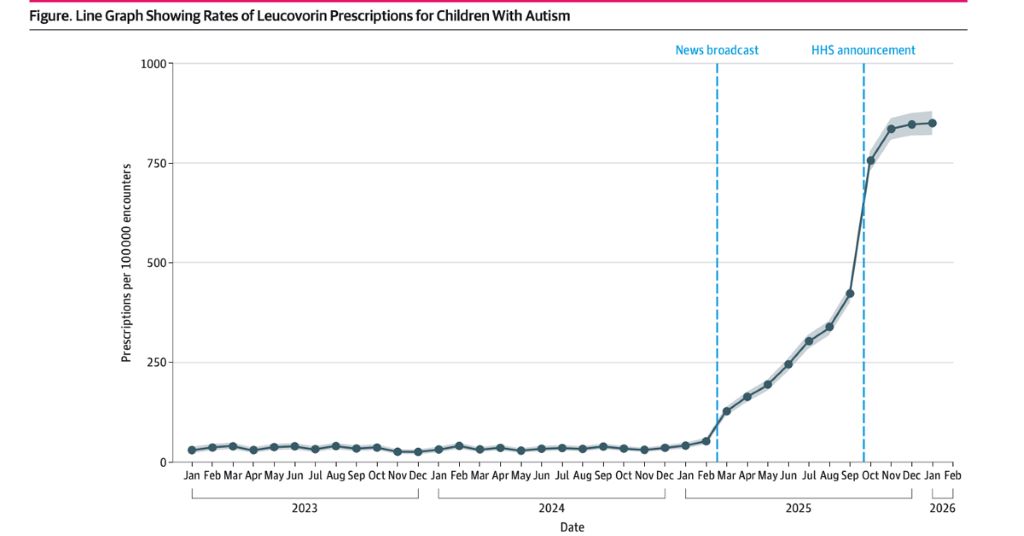
National study found use of the drug rose sharply following major media coverage and later White House promotion, despite limited large-scale evidence for autism treatment
Leucovorin prescriptions for children with autism rose more than 2000% by late 2025. Courtesy of UC San Diego Health Sciences.
Researchers from the University of California San Diego found that prescriptions for leucovorin, a drug sometimes used off-label for autism spectrum disorder (ASD), rose sharply among children after widespread media attention and public statements from White House officials. The study, published May 18, 2026 in JAMA Network Open, analysed national electronic health record data and found prescribing rates increased more than 2000% compared with prior years.
“Families of children with autism are often searching for therapies that might improve communication and quality of life, especially when treatment options are limited,” said Joshua Rothman, MD, clinical assistant professor of pediatrics at the UC San Diego School of Medicine and first author of the study. “What this study shows is how quickly information shared through news coverage, social media and public figures can influence real-world prescribing patterns, even before large clinical trials establish whether a treatment is truly safe and effective for broad use.”
Leucovorin, also known as folinic acid, is a biologically active form of folic acid. Small clinical trials have suggested that some children with autism and folate-related deficiencies may experience improvements in verbal communication after taking the medication. However, researchers note that large-scale studies confirming the drug’s effectiveness and long-term safety for children with ASD have not yet been completed.
To better understand prescribing trends, the researchers analysed records from the Epic Cosmos database, which includes more than 300 million patient records from over 1800 hospitals and 41 500 clinics across all 50 states and Washington, D.C. The study focused on 838 801 children with autism who accounted for more than 11.9 million outpatient encounters between January 2023 and January 2026.
For roughly two years, leucovorin prescribing rates remained relatively stable, averaging about 34 prescriptions per 100 000 outpatient encounters among children with autism. Rates then began climbing steadily in early 2025 before surging later that year. By August 2025, prescribing rates had risen to 335 prescriptions per 100 000 encounters. In November 2025, rates climbed again to more than 835 prescriptions per 100,000 encounters.
The researchers observed that the initial rise in prescribing coincided with a February 2025 national television news segment featuring a family who reported dramatic language improvements in their child after treatment with leucovorin. Interest in the medication expanded further after White House officials publicly promoted leucovorin in September 2025 as part of broader autism-related initiatives.
“Families of children with autism are often searching for therapies that might improve communication and quality of life, especially when treatment options are limited. What this study shows is how quickly information shared through news coverage, social media and public figures can influence real-world prescribing patterns, even before large clinical trials establish whether a treatment is truly safe and effective for broad use.”
— Joshua Rothman, MD, clinical assistant professor of paediatrics at the UC San Diego School of Medicine and first author of the study
“The timing was striking,” Rothman said. “The increases began after a widely viewed media story and accelerated again after federal officials publicly discussed the medication. It highlights how rapidly clinical practice can shift when a treatment captures public attention.”
The study does not determine whether leucovorin improves symptoms of autism, nor does it evaluate patient outcomes after treatment. Researchers also cautioned that prescriptions recorded in the database could not always be linked to a confirmed medical indication.
Still, the authors say the rapid increase in use raises important questions for clinicians, policymakers and families. In March 2026, the US Food and Drug Administration approved leucovorin for cerebral folate transport deficiency, an ultra-rare genetic neurological disease associated with specific genetic changes, but the drug was not approved for autism spectrum disorder.
Researchers say the findings underscore the need for continued monitoring of prescribing trends and for larger randomised clinical trials evaluating whether leucovorin is beneficial for specific groups of children with autism.
“We now have a real-world example of how public attention can accelerate adoption of a therapy before the evidence fully catches up,” Rothman said. “The next step is making sure we generate the rigorous data needed to help families and clinicians make informed decisions.”
Time to restore kindness and compassion in healthcare to improve patient and staff well-being
Source: Pixabay CC0
Healthcare has lost its human, moral, and relational foundations and must reconnect with its core values to improve both patient and staff well-being, argue experts in The BMJ today.
Despite unprecedented advances in diagnostic precision, therapeutic capability, and computational power, a deep paradox exists, say authors Don Berwick, Maureen Bisognano and Bob Klaber. Patients increasingly feel processed rather than cared for, staff report moral distress and loss of meaning, and the workforce is haemorrhaging people at an unsustainable rate.
The core problem, they write, is that we have accumulated extraordinary technical power while quietly losing the human, moral, and relational foundations of care on which its effectiveness ultimately depends.
Several powerful forces have helped create this imbalance, they explain. For instance, in some countries the pursuit of profit has choked healthcare’s moral purpose, while across the globe modern healthcare has become an industrialised system that processes patients through standardised protocols in ways that risk disregarding the unique texture of individual lives.
This has happened through an imbalanced emphasis on a “rational” lexicon (focused on measurement, targets and efficiency) over a “relational” one (concerned with feelings, kindness and human connection).
Yet re-establishing the relational balance is not a sentimental or “soft” approach; it is vital for quality and safety, they argue.
They point to research on NHS culture and behaviour that found organisations where staff felt supported and valued had consistently lower patient death rates, while the Institute for Healthcare Improvement (IHI) framework shows that the conditions for increasing joy in work – clarity of purpose, psychological safety, and feeling that what matters to you is actually valued – are both achievable and measurable.
Kindness – linked empirically to better staff retention, higher teamworking scores, and improved patient outcomes – should also be repositioned at the business end of delivering high quality care, they add.
The “What matters to you?” movement, inspired by an article in the New England Journal of Medicine, exemplifies this shift, changing the clinical encounter from a diagnostic focus to a partnership based on the patient’s lived reality.
While the forces pulling healthcare away from its human dimension are structural and powerful, they are not irreversible, they say. Every ward round, clinical consultation, and leadership conversation is a small but powerful opportunity for all of us working in healthcare to balance relational practice with rational systems and processes.
The evidence is clear: patients do better and staff thrive when healthcare systems invest in joy, kindness, and compassionate leadership, they write. “We do not need to wait for system reform. We can begin now on our collective leadership challenge to reconnect healthcare with its mission and purpose.”
Opinions ranged widely, with some physicians concerned that preparation for preservation could interfere with best practices for a patient’s care.
AI image of a brain being cryogenically preserved. [Ed: The patient better have some hefty medical aid to pay for a new body in the year 3000…]
Surveyed US physicians believed preservation has a one in four chance of working, though opinions amongst physicians varied. Ariel Zeleznikow-Johnston of Monash University, Australia, and colleagues present their findings in the study, published on May 20, 2026 in the open-access journal PLOS One.
It’s unclear whether there is a consensus amongst doctors regarding preservation – the storing of bodies at extremely low temperatures, or using preservative chemicals, in the hopes of future revival. Preservation is not the only way in which physicians have to balance concerns about unproven treatments with patients’ preferences, but it is one with high stakes as it pertains to the end of someone’s life. The technologies necessary to revive someone have not yet been realised, though current preservation organisations report several hundred patients preserved globally, with thousands more signed up for future preservation.
In this study, Zeleznikow-Johnston and colleagues conducted a survey of over 300 physicians, nearly half of whom were primary care providers, the rest being various kinds of specialists including neurologists, intensive care doctors, anaesthesiologists, and doctors who specialise in palliative care. The survey was designed to address three main themes: the perceived feasibility of preservation procedures, clinical interventions that could improve preservation outcomes, and the ethical and legal standing of preservation as an end-of-life option.
About one in four of the physicians said they believed it was plausible, or even very plausible, that someone could be revived in the future after preservation. Just under half said it was unlikely. Neurosurgeons, on average, rated the possibility of revival highest, though most of the other specialties showed a wide spread of opinions that slanted more towards scepticism.
The way doctors are most likely to interact with preservation in their professional capacity is in the choices a patient may make for end-of-life care. A majority of physicians supported prescribing anti-coagulants to dying patients, which could help with the quality of preservation. However, fewer respondents were comfortable with more extreme procedures, such as patients going through medically assisted death and opting to begin the preservation before cardiac arrest. The doctors who most commonly have conversations about end-of-life care were overall more supportive of this kind of choice. About one in five doctors were concerned that decisions to increase the odds of successful cryopreservation would clash with providing the best standards of care.
Currently, pre-cardiac arrest preservation in humans is, to the best of our knowledge, not legally permitted anywhere in the world, but if the technology develops further, may become an issue healthcare professionals must grapple with. The authors emphasise that clarifying the clinical, legal, and ethical frameworks for use of preservation as an end-of life procedure is important, and note that the speculative nature of the findings should be carefully considered.
Zeleznikow-Johnston adds: “A lot of physician hesitancy may come from simple unfamiliarity with the scientific basis of modern preservation methods. The doctors who have actually thought about this – and who regularly sit with dying patients – tend to be more receptive, not less.”