
Irradiation May Help CAR-T Cell Therapy Work Better Against Solid Tumours
New study shows focused irradiation helps immune cells keep cancer-fighting CAR T cells active and contained inside tumours
Researchers from the Icahn School of Medicine at Mount Sinai have discovered a promising new way to improve CAR-T cell therapy for solid tumours such as lung cancer and melanoma. The study, published in Nature Cancer, found that focused irradiation, a targeted therapy that delivers high-energy beams to stun rapidly growing cells such as cancer, can help CAR-T cells survive longer and work more effectively inside tumours.
CAR-T cell therapy involves removing the patient’s T cells (a type of immune cell), reprogramming them in the lab to fight cancer, and then infusing them back into the patient. It has transformed treatment for some blood cancers, but has not worked as well for solid tumours such as lung cancer and melanoma. Patients with solid tumours typically have bulky, treatment-resistant disease, and one of the central reasons CAR-T cells fail in this setting is that they do not persist or expand at the tumour long enough to eliminate it. Even when CAR-T cells initially reach the tumour, their numbers dwindle before they can finish the job.
The research team discovered that tumour irradiation does something unexpected: it turns dendritic cells, the immune system’s most powerful antigen-presenting cells, into a local source of stimulation for CAR-T cells inside the tumour.
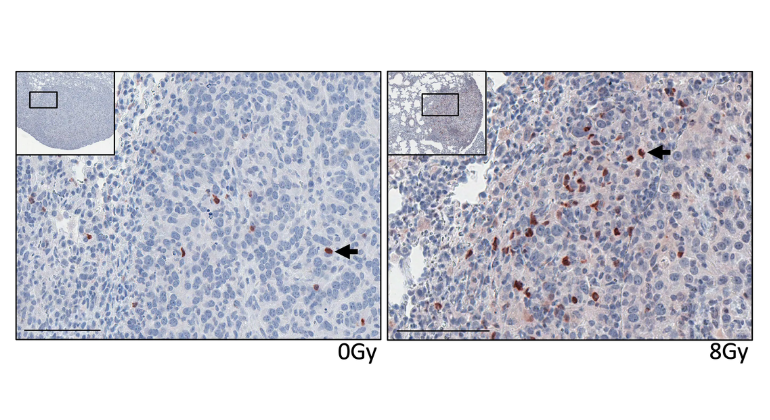
In mouse models of advanced lung cancer and melanoma, irradiation promoted dendritic cells to capture intact tumour surface proteins and display them on their own membranes, a process called “antigen dressing.” These antigen-dressed dendritic cells then engaged the chimeric receptor on the CAR-T cells – the laboratory-engineered protein that gives these cells the ability to target specific proteins – keeping them alive and multiplying within the tumour over several weeks.
The result was durable control of advanced lung tumors that CAR-T cells alone could not eliminate.
“This study shows that irradiation can do more than kill cancer cells; it can enhance cell therapy,” said corresponding author Jalal Ahmed, MD, PhD, who led the study and is Assistant Professor of Immunology and Immunotherapy, and Radiation Oncology, at the Icahn School of Medicine at Mount Sinai. “We found that dendritic cells can dress themselves in tumor proteins and use them to directly expand CAR-T cells through the engineered receptor. This was completely unexpected – dendritic cells normally engage T cells through an entirely different mechanism.”
A second finding addresses one of the most pressing safety challenges in the field. The researchers found that the CAR-T cell response stayed largely confined to the irradiated tumour. CAR-T cells expanded within the tumour but did not become more active in nearby healthy tissues, even when those tissues expressed the same protein targeted by the CAR-T cells. On-target activity against healthy organs has been one of the most serious safety barriers in solid tumour CAR-T cell therapy and has led to the termination of clinical trials. By selectively concentrating CAR-T cell activity at the tumour, focused irradiation may allow treatment of advanced tumours at lower and safer CAR-T cell doses.
“What is striking is that irradiation does not just amplify the immune response – it tells the immune system where to act,” said study co-author Miriam Merad, MD, PhD, Robin Chemers Neustein Professor of Immunology and Chair of Immunology and Immunotherapy at the Icahn School of Medicine at Mount Sinai. “Confining CAR-T cell expansion to the tumour could open up a new generation of safer cell therapies for solid cancers.”
This approach is particularly relevant for patients with metastatic solid tumours, who currently have few options. The irradiation treatment used in the study is available in cancer care centres around the world. This means the strategy could be tested in clinical trials without requiring new equipment, new drugs, or new infrastructure.
“This work suggests that preparing the tumour environment is important to optimise the efficacy of CAR-T cells,” said study co-author Michel Sadelain, MD, PhD, who was previously at Memorial Sloan Kettering Cancer Center and is currently the founding director of Columbia University’s Institute for Cell Engineering and Therapy. “Irradiation may provide a practical way to help CAR-T cells succeed in solid tumours.”
The researchers caution that the findings are still preclinical and must be tested in human clinical trials. The team is now working to define the molecular mechanism of antigen dressing, identify the signals dendritic cells use to sustain CAR-T cells, and translate the approach into trials for patients with advanced solid tumours.
Source: Mount Sinai




