Research shows that greater subjective well-being can lead to enhanced immune function and a lower incidence of chronic disease. But when does happiness start to exert its positive influence, and is there a point when this effect caps out? Researchers looked at national level data from 123 countries and found there is: on a scale from zero to 10, people started gaining health benefits once they surpassed a threshold that lies at around 2.7. Once above, each 1% of additional happiness could lead to a small decrease in mortality risk from non-communicable diseases.
Heart disease, cancer, asthma, and diabetes: All are chronic or non-communicable diseases (NCD), which accounted for about 75% of non-pandemic related deaths in 2021. They may result from genetic, environmental, and behavioural factors, or a combination thereof. But can other factors also influence disease risk?
Now, a new Frontiers in Medicine study has investigated the relationship between happiness and health to find out if happier always means healthier and to determine if happiness and co-occurring health benefits are linear or follow a specific pattern.
“We show that subjective well-being, or happiness, appears to function as a population health asset only once a minimum threshold of approximately 2.7 on the Life Ladder scale is surpassed,” said first author Prof Iulia Iuga, a researcher at 1 Decembrie 1918 University of Alba Iulia. “Above this tipping point, increased happiness is associated with a decrease in NCD mortality.”
Happy equals healthy
“The life ladder can be imaged as a simple zero to 10 happiness ruler, where zero means the worst possible life and 10 means the best possible life,” explained Iuga. “People imagine where they currently stand on that ladder.” The team used data sourced from different health organisations, global development statistics, and public opinion polls. The data came from 123 countries and was collected between 2006 and 2021.
A score of 2.7 can be found towards the lower end of the ladder, and people or countries finding themselves there are generally considered unhappy or struggling. “An adjective that fits this level could be ‘barely coping’,” said Iuga. Nevertheless, already at this point, improvements in happiness begin to translate into measurable health benefits.
Once the threshold is surpassed and a country’s collective happiness rises above it, the study found that each 1% increase in subjective well-being is linked to an estimated 0.43% decrease in that country’s 30-to-70-year NCD mortality rate. This rate refers to the percentage of deaths due to NCDs among individuals aged between 30 and 70.
“Within the observed range, we found no evidence of adverse effects from ‘excessive’ happiness,” Iuga added. Below the 2.7-point threshold, small improvements in happiness (for example, from a score of 2 to 2.2) do not translate to measurable reduction in NCD deaths, the data indicated. Before measurable changes can be unlocked, very low well-being needs to be remedied, the study suggested.
Countries that exceeded this threshold tend to have higher per person health spending, stronger social safety nets, and more stable governance as opposed to the countries falling below it. The average life ladder score across the examined countries during the study period was 5.45, with a minimum of 2.18 and a maximum of 7.97.
There are several ways that governments could raise countries above a score of 2.7, for example through promoting healthy living by expanding obesity prevention and tightening alcohol availability; improving the environment through stricter air-quality standard; and increasing their per capita health spending. The authors said their insights could help guide health and social policies and might aid to integrate well-being into nations’ agendas.
The authors pointed out that the life ladder scores making up their data were self-reported, which may have resulted in measurement errors, differences in cross-cultural response styles, or reporting bias. It is also possible that subnational differences between populations were captured inadequately. In the future, studies should include more measures, such as years lived with disability or hospital admission records, include subnational micro-data, and expand coverage to low-income or conflict states, which may have been overlooked in the data they used, the team pointed out.
Nevertheless, identifying the protective effects of happiness could be an important step towards healthier people. “Identifying this tipping point could provide more accurate evidence for health policy,” concluded Iuga. “Happiness is not just a personal feeling but also a measurable public health resource.”
A new model combining a dozen metrics measures differences in white matter structure between older CAD patients and healthy controls
Source: Wikimedia CC0
Although coronary artery disease (CAD) increases the risks of strokes, cognitive impairment and dementia, the link between CAD and cognitive function is not fully understood. A new study led by Concordia researchers looks at how the disease affects the brain’s white matter, the network of nerve fibres that connects different regions of the brains and is critical to transmitting information efficiently.
The study, published in the Journal of Neuroscience, applied a novel multivariate approach using 12 separate metrics. The researchers compared test results and MRI scans of 43 patients with CAD to those of 36 healthy individuals. All participants were over age 50.
The researchers found that individuals with CAD had widespread structural changes in their white matter compared to their healthy counterparts. The changes were particularly noticeable in the parts of the brain fed by the middle cerebral (MCA) and anterior cerebral arteries. Both regions are key for cognitive and motor functions.
“This makes sense because those regions, especially the MCA territory, are most prone to strokes,” says PhD candidate Zacharie Potvin-Jutras, the study’s co-lead author. “We made sure that there was no history of strokes in our CAD cohort.
“Our goal is to examine conditions at the onset of a heart disease, before there has been any significant impact on the brain,” he says.
Stéfanie Tremblay, a 2023 Concordia Public Scholar now a postdoctoral researcher at McGill University, is the study’s other co-lead author.
Small measurements provide a bigger picture
The multivariate approach of bundling individual white matter metrics into one overarching metric provides advantages over past univariate studies. It allows the researchers to simplify complex aspects of brain health into a single metric that can be compared to the same metric in healthy controls. While individual metric variations between CAD patients and healthy controls may be very small, when seen together, they can provide significant indicators of early stages of cognitive impairment.
“The metrics are often overlapping, meaning they measure things that are related to each other,” says corresponding author Claudine Gauthier, an associate professor in the Department of Physics. “Having one single metric that captures many aspects of brain health allows us to identify differences between patients and controls that reflect a complex combination of changes in a single analysis. Then we can unpack it and see which aspects of white matter health drove the difference more than the others.”
The researchers found that the changes were mainly linked to reduced myelin content, the fatty envelope surrounding nerve fibres. Myelin loss can slow communication between brain cells and is often an early sign of cognitive ageing.
Interestingly, participants with higher measures of myelin integrity (specifically, in a marker called R1) performed better on tests of processing speed, a key aspect of thinking and attention. However, no significant differences were observed between groups in overall cognitive scores, suggesting that brain changes may precede noticeable symptoms.
“This study adds mechanistic insight into our understanding of how CAD affects white matter health,” says Gauthier. “Now that we know that myelin content is a good biomarker for coronary heart disease, the next step is to focus on potential interventions. If we have a preventive lifestyle intervention, we can optimize the intensity to improve myelin health and maintain cognitive function.”
The Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada and Brain Canada supported this research.
When hospitals were randomly assigned to treat patients undergoing higher-risk non-cardiac surgery with tranexamic acid (TXA) or a placebo, patients who received TXA needed significantly fewer blood transfusions and saw no increase in potentially life-threatening blood clots (thrombosis) after 90 days of follow-up, according to research presented at the 67th American Society of Hematology (ASH) Annual Meeting and Exposition.
“Our findings confirm that TXA reduces the need for blood transfusion in patients undergoing higher-risk non-cardiac surgery,” said lead study author Brett Houston, MD, PhD, an assistant professor at the University of Manitoba and a scientist with the Paul Albrechtsen Research Institute in Winnipeg, Canada. “We were also able to show that giving TXA is safe and does not increase the occurrence of dangerous blood clots within the three-month high-risk period after surgery.”
TXA is a generic drug that promotes blood clotting, which is essential to stop blood loss from injuries or during surgery, but blood clots can be life-threatening.
A 2019 international study of 40 000 patients found major bleeding to be the most common life-threatening complication following non-cardiac surgery. Another large international randomised trial, known as POISE-3, showed that, compared with patients who received a placebo, patients who received TXA immediately before and after non-cardiac surgery had significantly less serious bleeding and needed fewer blood transfusions, with no significant increase in heart attacks, strokes, or blood clots at 30 days.
The current study, known as TRACTION, was designed to build on the findings of POISE-3, Dr Houston said. Participating hospitals – 10 medical centres in Canada – were randomly assigned to administer either TXA or a placebo to adult patients undergoing major non-cardiac surgical procedures that posed an elevated risk for post-surgical bleeding complications and blood clots. Every four weeks, hospitals in the TXA group switched to the placebo group and vice versa.
Patients received a first dose of TXA or the placebo intravenously within minutes of surgery initiation. At the discretion of the attending anaesthesiologist, they then received a second dose either at the conclusion of the operation or as a continuous infusion throughout the procedure.
The study’s primary endpoints were the number of patients needing blood transfusions during their hospital stay and the number diagnosed with blood clots within 90 days.
Secondary endpoints included the number of units of blood transfused; the number of patients diagnosed with a heart attack, stroke, or blood clot while in the hospital; the number of patients admitted to intensive care; the number surviving at 90 days after surgery; and patients’ length of stay in the hospital.
The study’s results are based on the evaluation of 8273 patients treated across the 10 participating hospitals. More than 60% of the patients underwent cancer surgery. Among patients treated with TXA, 7.4% received a blood transfusion while in the hospital compared with 9.8% of those treated with the placebo, a statistically significant difference. Patients treated with TXA needed significantly fewer units of blood (0.34 units on average) than those in the placebo group (2.5 units on average). The proportion of patients diagnosed with blood clots within 90 days was the same (2.1%) in both the TXA and placebo groups. No significant differences were seen in any of the secondary endpoints.
The finding that TXA use does not increase risk for blood clots during the 90-day post-surgical period of elevated risk may reassure many practitioners who have previously been hesitant to adopt the drug, Dr Houston said. “We hope this data will also set practitioners’ minds at rest that giving the drug is safe,” she said.
Although the study was limited to Canada, it evaluated bleeding risk across a broad range of types of higher-risk non-cardiac surgery, Dr Houston said, including gynaecologic, urologic, spinal, blood-vessel, and cancer surgery. In addition, participating hospitals included both academic medical centres and community hospitals.
A limitation of the study is that participation was restricted to hospitals with sophisticated electronic medical records systems in place to transmit study data.
Findings from other studies suggest that the use of TXA could be successfully introduced as a hospital-level policy in the same way that other surgical safety practices, such as antibiotic administration to prevent infection and the use of surgical checklists have been adopted, Dr Houston said. As a next step, she and her colleagues plan to work on educating physicians about the TRACTION findings and promoting the adoption of TXA administration as a standard practice during higher-risk non-cardiac surgery.
Changing the amount of sweetness in a person’s diet has no impact on their liking for sweet foods, the results of a new trial suggest. The results also showed no difference in indicators of cardiovascular disease or diabetes risk between people who increased or decreased their intake of sweet-tasting foods over a six-month period.
The research team suggest that consequently public health organisations may need to change their current advice on reducing sweet food consumption to tackle the obesity crisis.
The study, published in the American Journal of Clinical Nutrition, was carried out by Wageningen University and Research in the Netherlands and Bournemouth University in the UK.
“People have a natural love of sweet taste which has led many organisations, including the World Health Organisation, to offer dietary advice on reducing the amount of sweetness in our diets altogether,” said Katherine Appleton, Professor in Psychology at Bournemouth University and corresponding author for the study. “However, our results do not support this advice, which does not consider whether the sweet taste comes from sugar, low calorie sweeteners, or natural sources.” she added.
During the trial, 180 participants were split into three groups. One group consumed a diet containing a high amount of sweet-tasting food, a second group consumed a low amount and a third consumed an average amount. The sweetness in the foods provided for their diets came from a combination of sugar, natural sweetness or low-calorie sweeteners.
After one, three and six months, participants were surveyed on whether their liking and perception of sweet foods had changed. They were also weighed and provided blood and urine samples to measure any changes in their diabetes risk and cardiovascular health.
At the end of the trial, the researchers found no significant differences in any of the measures across the three groups. Participants also reported a spontaneous return to their previous intake of sweet foods after the six months.
Based on their results, the study team are recommending that public health organisations may need to change their current advice on reducing sweet foods to tackle overweight and obesity.
“It’s not about eating less sweet food to reduce obesity levels,” Professor Appleton said. “The health concerns relate to sugar consumption. Some fast-food items may not taste sweet but can contain high levels of sugar. Similarly, many naturally sweet products such as fresh fruit and dairy products can have health benefits. Public advice therefore needs to concentrate on how people can reduce the amount of sugar and energy-dense foods they consume,” she concluded.
After birth, moms and babies are required to visit healthcare facilities for essential services like immunisations, postnatal care and HIV testing. Photo by William Fortunato on Pexels
By Elri Voigt
In South Africa, many mothers and their babies have to visit the clinic more than 10 times in the first six months of the postnatal period. Early findings from an ongoing implementation science project suggests we can get this down to five. The hope is that the new approach will also help reduce HIV transmission from mothers to their babies.
Over the last two decades, South Africa has taken huge strides in reducing HIV transmission from mothers to their babies (often called vertical transmission).
Maternal deaths from non-pregnancy-related infections have decreased, because more women are taking HIV treatment, and HIV rates among babies at birth have also gone down. This has all been possible largely because of integrating HIV services with our antenatal services, Dr Jeanette Wessels, of the University of Pretoria’s Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, told delegates at the recent Southern African HIV Clinicians Society (SAHCS) Conference.
However, a closer look at the data shows us that while vertical transmission at or before birth has come down dramatically, HIV transmission in the months after birth remains alarmingly common. This happens particularly when the mother contracts HIV in this period and the virus is then transmitted to her baby before she is diagnosed, or before the virus can be brought under control with antiretrovirals. As Wessels puts it, “our next frontier to tackle is the breastfeeding period”.
During the antenatal period (before birth), pregnant women are offered HIV tests and prevention pills or HIV treatment when they visit clinics for their pregnancy check-ups. However, during the postnatal period (after birth), HIV services are not integrated in the same way. This fragmentation of care after birth is a key driver of vertical transmissions, suggests specialist paediatrician Dr Nthabiseng Serudu-Nageng. The thinking is that the fragmentation and high number of clinic visits makes it less likely that new HIV infections in mothers will be picked up before the virus can be transmitted to their babies and that it makes it less likely that new mothers will take the HIV prevention pills or HIV treatment they might need.
Spotlight previously reported that, according to the latest estimates from Thembisa – the leading mathematical model of HIV and TB in South Africa – of the roughly 7 200 babies who contracted HIV in the country from mid-2023 to mid-2024, only about 2 500 got HIV before or at birth. This means that about 4 700 babies got HIV in the months after birth, and while some of these mothers were on antiretroviral therapy, according to the Thembisa estimates, the majority of mothers had not been diagnosed with HIV yet. Meaning a contributing factor to some of these infections is likely that many of these mothers got HIV after the birth of their babies and were unaware of it.
Wessels told delegates that around 75% of mother-to-child transmission of HIV is happening during breastfeeding, and just over one third (35%) of those are due to new HIV infections in the mother. She added that about 80% of those new infections in babies after birth happen in the first six months.
It is important to realise that in terms of absolute numbers, HIV transmission during the breastfeeding period has gone down, but proportionally more babies are getting HIV after birth, explained Professor Ute Feucht, the Director for the University of Pretoria’s Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies. Feucht is also the Community Paediatrician in the Tshwane District Clinical Specialist Team at the Gauteng Department of Health.
Clinic visits can be halved
To improve care in the postnatal period, researchers in Gauteng have launched an ambitious implementation science project called Sihamba Kunye. Their key idea is that clinic visits for mother and baby can be much better integrated and optimised. This could make it more likely that mother and baby will attend all required clinic visits and get all the healthcare services they need. The project is funded by the Gates Foundation.
During the postnatal period, said Wessels, a mother may have to come to the clinic up to 11 or 12 times in the first six months. This can be to get her baby to the necessary visits for immunisations, as well as family planning, to pick up HIV treatment or prevention pills or postnatal care for herself. Wessels was presenting early observations from the study at the SAHCS conference.
Commenting on this, Feucht, who is the study’s principal investigator, told Spotlight: “That is twice a month, and yes, with a newborn baby!”
To make matters worse, throughout these many visits, mothers and babies are often seen separately, which isn’t optimal since, as Serudu-Nageng pointed out, “whatever affects the mother directly impacts her baby, so integrating their care is essential”. She is the study’s consultant paediatrician.
“One of the biggest challenges mothers face is having to come to the clinic many times in the first six months. This has a huge impact: it affects food security, especially for unemployed mothers, its transport costs, its time away from work or home, and long waiting hours at the facility. Each visit comes with an emotional and financial cost,” said Serudu-Nageng.
“Through the Sihamba Kunye project, we are addressing this [challenge] by aligning and coordinating the mother and baby’s visits so they can be seen together, on the same day and ideally at the same service point,” she said. “This reduces the number of visits, saves time and cost for the mother, eases the workload for the facility because it means less feet through the clinic all while maintaining quality care for both mother and baby.”
By coordinating these different visits, the total number of times a mother and baby might need to go the facility is reduced to only five visits.
How it works
The researchers conducted time-and-motion studies – where industrial engineering students from the University of Pretoria followed patients around with stopwatches to time how long it took them to move through the clinic from arrival to exit. They also conducted interviews with mothers and infant pairs, had consultations with facility managers, and conducted workshops with healthcare workers, as well as created curated resources and tools to assist with the transition to offering integrated care.
Integration of services was classified into two levels, depending how much the services could be streamlined, said Serudu-Nageng. Level two integration means that a mom and her baby are seen on the same day, but at different parts of the facility and likely by different nurses. Level three integration means they are seen together, on the same day, by the same nurse.
“We worked closely with facility managers, sub-district programme managers and clinicians to redesign processes and adapt the model to fit each facility’s realities,” she said.
The time-and-motion studies helped identify bottlenecks and improve the flow and efficacy at the clinics, Serudu-Nageng said. One big time waster was that if a mom comes in with her baby and the healthcare staff only draw baby’s file but later see mom also needs care, she’ll have to go back to get her own file. To resolve this, the project recommends drawing both mom and baby’s files when they visit the facility, regardless of the reason for the visit.
One major component of integrating care, Serudu-Nageng said, was task-shifting. This is to ensure that professional nurses have the time to spend doing clinical consultations with mom and baby together, since their consultation time has essentially doubled. This means designating tasks like checking vital signs, weighing, giving immunisations and vitamin A and deworming to support staff, leaving professional nurses to do tasks only they are qualified to do.
“[T]he professional nurses can be used for other things like clinical decision making and we can rather delegate work that doesn’t require clinical decision making to lower cadres of nurses of staff,” she said. “Together, these efforts have helped facilities streamline workflow, strengthen teamwork and deliver this integrated postnatal care package for both mothers and babies.”
Another thing the researchers did was to compile two important tools that pulled together information from all the relevant national guidelines for primary healthcare – like the HIV, TB, ideal clinic and immunisation guidelines – and putting them together in one place called the the First 1000-day Roadmap. This is used alongside an Integration Wheel that helps nurses coordinate the different visits moms might need to come to the clinic for.
Wessels in her presentation explained that the roadmap has different sections categorised according to the type of visit mom and baby are at the clinic for. She gave the example of the 10-week visit, where babies normally receive some of their key childhood immunisations. One section of the roadmap will include “all the care needed for the mom, her general postnatal care, nutrition, VTP [Vertical Transmission Prevention] and screening like TB screening, STIs, mental health, her contraception and extra care”. The other section will cover all the things the baby will need.
The roadmap is used alongside the Integration Wheel, which is designed like a pregnancy wheel. The front of the wheel can spin to the visit the mom and baby are at the clinic for. “It outlines [among other things] what you do for an HIV positive mom, for an HIV negative mom, what contraception do you get every mom,” Wessels said. At the back, the wheel has information on the different visits mom and baby would still need to come to the clinic for and helps nurses align those visits.
The front of the Integration wheel can be spun to the specific visit mom and baby are at the clinic for and help align their next visits to reduce the number of times they have to come to the facility. Source: Screenshot from Professor Ute Feucht’s presentation on the Sihamba Kunye Project at the 2025 SA AIDS conference.The back of the Integration wheel shows nurses everything they need to do for both mom and baby, depending on their HIV status, baby’s age and mom’s family planning needs and postnatal care. Source: Screenshot from Professor Ute Feucht’s presentation on the Sihamba Kunye Project at the 2025 SA AIDS conference.
With these resources, according to Wessels, nurses at the participating facilities are able to align mom and baby’s visits from their six-day postnatal visit and can reduce those visits to only five in the first six months.
What’s next?
The response to the project has been very positive and created a bit of a “snowball effect”, Feucht said. “The district has actually been asking us, when can we go to the rest [of the clinics in Tshwane]?”
The first phase, she added, was to figure out what is possible in terms of integrating care and how can it be done. “[T]he next step is then taking that toolkit out to the other provinces as well.”
The research team hopes to have several publications showcasing their findings ready to present at key health conferences next year. But they also hope to see the model being more widely used in the future.
“It’s got potential to transform the postnatal period and make it as good as the antenatal period,” Serudu-Nageng said. “[I]ntegrating care and putting the patient at the centre will really, really, be great for outcomes, but for mom and baby as well.”
“Based on my experience, this approach is highly feasible within the broader public healthcare system because it builds on existing structures and staff,” she added. “It is practical and scalable, and we are hopeful that it will serve as a proof of concept for future scale-up across South Africa’s public health system.”
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council and subject to the Press Code.
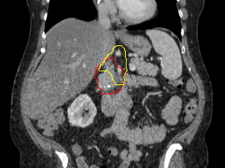
Image of a what is targeted with radiation. Red represents the pancreatic tumor, which is contacting with a major nearby artery. Yellow represents the Baltimore Triangle, which is now targeted in all patients, in addition to red volume. Credit: Amol Narang, M.D.
Using targeted radiation during surgery – referred to as intraoperative radiation – to eliminate pancreatic cancer cells that have spread to areas around the pancreas, investigators at Johns Hopkins have been able to reduce the recurrence rate around the pancreas to 5%. This is believed to be the lowest ever reported for this population of patients, according to a preliminary study by the team from the Johns Hopkins Kimmel Cancer Center.
The study was presented at the American Society for Radiation Oncology annual meeting in September 2025.
The study enrolled 20 patients with borderline resectable or locally advanced pancreatic cancer. Patients received presurgical chemotherapy and radiation targeted to shrink the tumours away from the blood vessels. Then, during surgery to remove their tumours, patients received another dose of precisely targeted radiation using a robotic device that carries small radioactive beads inserted through catheters. The device enabled the team to pinpoint a triangular area near the pancreas, where recurrences commonly occur. Only one of the 20 patients experienced a recurrence around the pancreas at the 24-month mark – a major achievement for a cancer that, until recently, had lagged behind other cancers in treatment success.
By the time most pancreatic cancers are diagnosed, the tumours have spread to affect important blood vessels around the pancreas. Historically, patients with pancreatic cancers whose blood vessels were affected could not undergo surgical removal of their tumours. But in the past decade, clinicians at the Johns Hopkins Kimmel Cancer Center’s Skip Viragh Center for Pancreas Cancer Clinical Research and Patient Care have pioneered new approaches that use chemotherapy and radiation to shrink the tumours away from blood vessels, enabling more patients to undergo surgical removal of their tumours.
The team learned that the pancreatic cancer cells were spreading along nerves near the pancreas to a fatty, nerve-dense triangular area just above the pancreas, which Narang calls the “Baltimore triangle.” When he and his colleagues started targeting the Baltimore triangle with radiation before surgery to kill these stray cancer cells, pancreatic cancer recurrence rates in their patients dropped from 47% to 12% at two years post-surgery. Yet, in the 12% who experienced recurrences around the pancreas, the recurrences continued to occur in the Baltimore triangle.
To further lower recurrence rates, Narang and his colleagues decided to deliver an additional round of Baltimore triangle-targeted radiation to patients during surgery after removal of the pancreatic tumour. He explained that, during the surgery, surgeons remove a part of the duodenum, next to the pancreas, making it easier to access the Baltimore triangle without risking harm to surrounding organs. The combination of radiation targeted to the Baltimore Triangle prior to surgery as well as intraoperative radiation to the triangle during surgery allowed Narang to deliver ablative doses of radiation to this region.
“The combination of intraoperative radiation and targeting the Baltimore triangle has gotten us to a 5% recurrence rate, which is the lowest-ever reported recurrence rate around the pancreas for this population of patients to our knowledge. But I think we can drop to 0% in our next study,” Narang says. “We must do whatever we can to prevent recurrences from happening, because when pancreatic cancer comes back, it is often incurable. These results give us hope, though, that this can be done for a cancer where even decade ago, most thought this wasn’t possible.”
The only recurrence in the study occurred in the part of the Baltimore triangle that the team had difficulty reaching during the intraoperative treatment. Currently, the team is developing strategies to target this hard-to-reach part of the triangle, with the hopes of reducing recurrences to zero. Once they’ve mastered that refined approach, they would like to team up with other cancer centres across the US to run a larger clinical trial to confirm their results.
When a child falls ill, caregivers often change how and where the infant sleeps – wanting to keep them close through the night. But new research from Johns Hopkins Children’s Center suggests that some of these changes – although well-intentioned – contradict proven safe sleep practices for infants, and may do more harm than good.
In interviews with more than 100 caregivers of infants ages birth to 12 months presenting to the emergency department for infant illness, researchers found that unsafe sleep practices became more common during periods of illness – and often persisted even after the illness resolved. These changes to sleep practices increase an infant’s risk of sudden unexpected infant death (SUID), a broad term that includes sudden infant death syndrome (SIDS). SUID, defined as the unexpected sudden death of a seemingly healthy infant from known and unknown causes, resulted in the deaths of 3700 infants in 2022, according to federal health statistics.
Numerous studies over past decades have tied unsafe sleep practices to both SIDS and SUID. Findings from the new study published in Pediatrics add to evidence that infant illness is a risk factor for SUID.
Caregivers were asked about the infants’ usual sleep practices, and if they changed when the babies were sick. The caregivers reported that adherence to safe habits, such as putting their infants in a crib or playpen, declined overall from 61.8% before illness to 48.1% during illness. In addition, the proportion of caregivers reporting their infants sleeping in a bed or on a couch rose from 56.5% before illness to 62.6% during illness, and further increased to 75% at the one-month follow-up. Similarly, bed-sharing rates increased overall from 57.3% before illness to 68.7% during illness, and further increased to 83.6% at the one-month follow-up.
Many caregivers in the study reported shifts away from recommended safe sleep practices, such as placing infants on their backs to sleep, during infant illness. The most common changes included increased bed-sharing, sleeping on non-recommended sleep surfaces, and prone or side positioning, which are not in line with the American Academy of Pediatrics safe sleep recommendations.
The fact that the alterations persisted beyond the illness period highlights the need for targeted interventions to reinforce safe sleep practices during illness, says Mary Beth Howard, MD, MSc, paediatric emergency medicine physician at Johns Hopkins Children’s Center and lead researcher on the study.
“Parents often make these changes because they want to comfort or closely watch their sick baby, but these well-intentioned adjustments actually raise the risks of sudden, unexpected death. Illness is a particularly vulnerable time, making it even more important to stick to safe sleep guidelines,” says Howard.
The Johns Hopkins investigators note that October is Sudden Infant Death Syndrome (SIDS) Awareness Month, a time to encourage safe infant sleep practices. According to the American Academy of Pediatrics, safe sleep practices include placing infants on their backs to sleep, having infants sleep alone without blankets, pillows or stuffed animals, and having babies sleep in a crib or bassinet.
A new ACC Scientific Statement on Inflammation and Cardiovascular Disease (CVD) highlights new groundbreaking research linking inflammation atherosclerotic cardiovascular disease (ASCVD) and provides consensus-based recommendations for evaluation, treatment and prevention reflecting this new era.
“The evidence linking inflammation with ASCVD is no longer exploratory but is compelling and clinically actionable,” write the authors, led by Writing Committee Chair George A. Mensah, MD, FACC. “The time for taking action has now arrived.”
Published in JACC, the Statement includes specific recommendations for screening, evaluation, and CVD risk assessment; inflammatory biomarkers in cardiovascular imaging; inflammation inhibition in behavioural and lifestyle risks; and anti-inflammatory approaches in primary and secondary prevention, as well as in heart failure and other cardiovascular diseases.
Among the key takeaways:
High-sensitivity C-reactive protein (hsCRP) is an inexpensive and widely available blood test. While there has been debate within the medical community regarding the utility of hsCRP, this statement details the data confirming its value in clinical decision making in primary and secondary prevention.
In patients with known CVD, hsCRP level is at least as predictive of future events as LDL cholesterol levels, even in patients treated with statin therapy.
The important role of lifestyle interventions to reduce systemic inflammation is emphasised, including regular exercise (at least 150 minutes/week), Mediterranean or DASH Diet, and intake of omega-3 fatty acids, including two to three meals per week of fatty fish high in EPA and DHA. This advice aligns with lifestyle management recommendations in the 2025 ACC/AHA High Blood Pressure Guideline
The Statement also discusses current challenges and opportunities based on the new evidence, exploring topics like the advancing field of cardioimmunology and areas for further research, such as the interplay between inflammation and key physiological systems, the role of novel special pro-resolving bioactive lipid molecules in promoting the resolution of inflammation and CVD risk reduction, and more.
The authors close with a call for action to “embrace anti-inflammatory interventions in patients with established ASCVD” and for clinical practice guidelines that implement “broad screening of primary and secondary prevention patients for hsCRP, in combination with LDL cholesterol.” Additionally, they note: “The time is also ripe for the development of strategies to promote increased physician awareness of the crucial role of inflammation in CVD and accelerate the adoption of evidence-based, guideline-directed anti-inflammatory therapy through dissemination and implementation research.”
A groundbreaking new treatment using genome-edited immune cells, developed by scientists at University College London and Great Ormond Street Hospital (GOSH), has shown promising results in helping children and adults fight a rare and aggressive form of blood cancer.
Using base-editing technology, the pioneering gene therapy (BE-CAR7), has been used to treat a previously untreatable type of blood cancer called T-cell acute lymphoblastic leukaemia (T-ALL). Base-editing is an advanced version of CRISPR technology, that can precisely change single letters of DNA code inside living cells.
BE-CAR7 was designed and developed by a team of researchers, led by Professor Waseem Qasim (UCL Great Ormond Street Institute of Child Health), who is also an Honorary Consultant at Great Ormond Street Hospital (GOSH), and the treatment is the first in-human application of base-edited cells.
In 2022, Alyssa Tapley, from Leicestershire, (then aged 13) became the first person in the world to receive the treatment as part of a clinical trial at GOSH. Doctors had exhausted all other treatments for her and she and her family say the innovative therapy saved her life.
Now, a further eight children and two adults have undergone the treatment as part of the trial.
82% of patients achieved very deep remissions after BE-CAR7, enabling them to proceed to stem cell transplant without disease
64% remain disease-free, with the first patients now three years disease-free and off treatment
Anticipated side effects including low blood counts, cytokine release syndrome and rashes were tolerable, with the greatest risks arising from virus infections until immunity recovered
Professor Qasim, a Professor of Cell and Gene Therapy at UCL, who led the research, said: “A few years ago this would have been science fiction. Now we can take white blood cells from a healthy donor and change a single letter of DNA code in those cells and given them back to patients to try to tackle this hard-to-treat leukaemia.
“We designed and developed the treatment from lab to clinic and are now trialling it on children from across the UK – in a unique bench-to-bedside approach.”
Alyssa, now aged 16, who has a brother, said: “It is incredible how much my life has changed. I went from four months straight in GOSH to now only coming back for medical appointments once a year. It is amazing how much freedom I have now.
“I am really grateful for all the opportunities the gene therapy treatment has given me. I feel like I have been able to help everyone else who went on the clinical trial after me.
“I’ve now been able to do some of the things I thought earlier in my life it would be impossible for me to do. I really did think I was going to die and that I wouldn’t be able to grow up and do everything that every child deserves to be able to do.”
That has included going sailing and spending time away from home doing her Duke of Edinburgh Award.
Her dad, James, said: “We are eternally grateful. We’ve gone from being completely hopeless to where we are now. We could never have imagined that then.
“Back then we were at the point where we thought we were going to be a three-person family. Now we’re all making the most of family life. It is the little things you don’t take for granted anymore. Alyssa is amazing.
“The scientists at UCL and GOSH have been incredible. It has been really powerful seeing them in the laboratory developing the treatment and hearing the stories including about the difficulties they faced in getting this far.
“In terms of the timing of the trial, it aligned perfectly for us. Other families weren’t so lucky.”
New technology
Immunotherapy using CAR-T cells has recently become available to treat several types of blood cancer. This therapy uses immune cells, called T-cells, and modifies them to have specific proteins on their surface called chimeric antigen receptors (CARs).
The CARs can recognise and target specific ‘flags’ on the surface of cancer cells, and the T-cell can then destroy that cancer cell. Developing CAR T-cell therapy for leukaemia which itself has arisen from abnormal T-cells has been challenging.
BE-CAR7 T-cells are engineered using base editing, a new-generation of genome editing that avoids cutting DNA, reducing the risk of chromosomal damage.
Very precise chemical reactions were carried out using CRISPR guidance systems to change single letters of DNA code in order to modify the T cells. These complex DNA changes generate storable banks of ‘universal’ CAR T-cells that can find and attack T-cell leukaemia when given to patients.
The ‘universal’ CAR T-cells in this study were made from healthy donor white blood cells and engineering steps were undertaken in a clean room facility using custom made RNA, mRNA and a lentiviral vector in an automated process previously developed by the research team.
These steps were: 1. Removing existing receptors so that T-cells from a donor can be banked and used without matching the recipient– making them ‘universal’. 2. Removing a ‘flag’ called CD7 that identifies them as T-cells (CD7 T-cell marker). Without this step, T-cells programmed to kill T-cells would simply end up destroying the product through ‘friendly-fire’. 3. Removing a second ‘flag’ called CD52. This makes the edited cells invisible to one of the strong antibody drugs given to patients to subdue their immune system. 4. Adding a Chimeric Antigen Receptor (CAR) which recognises the CD7 T-cell flag on leukemic T-cells. A disabled virus added extra DNA code into the cells so they become armed against CD7 and recognise and fight T-cell leukaemia.
When base-edited CAR T-cells are given to the patient they rapidly find and destroy all T-cells in the body, including leukemic T-cells. If the leukaemia is eradicated within four weeks, the patient’s immune system is then rebuilt from a bone marrow transplant over a period of several months.
Professor Qasim added: “Many teams were involved across the hospital & university and everyone is delighted for patients clearing their disease, but at the same time, deeply mindful that outcomes were not as hoped for some children. These are intense and difficult treatments – patients and families have been generous in recognising the importance of learning as much as possible from each experience.”
Dr Rob Chiesa, Study investigator and Bone Marrow Transplant consultant at GOSH said: “Although most children with T-cell leukaemia will respond well to standard treatments, around 20% may not. It’s these patients who desperately need better options and this research provides hope for a better prognosis for everyone diagnosed with this rare but aggressive form of blood cancer.
“Seeing Alyssa go from strength-to-strength is incredible and a testament to her tenacity and the dedication of an array of small army of people at GOSH. Team working between bone marrow transplant, haematology, ward staff, teachers, play workers, physiotherapists, lab and research teams, among others, is essential for supporting our patients.”
Dr Deborah Yallop, consultant Haematologist at KCH said “We’ve seen impressive responses in clearing leukaemia that seemed incurable – it’s a very powerful approach.”
Dopamine neurons, the cells that drive reward and motivation while we’re awake, become surprisingly active during nonrapid eye movement sleep right after we learn something new.
According to a new University of Michigan study, this night surge that is synchronised with memory-boosting sleep spindles, helps strengthen motor memories and improves motor skills.
The findings challenge long-held assumptions about dopamine’s role in the brain, showing that these neurons don’t just support learning during the day – they actively help lock in new skills while we sleep, said study co-author Ada Eban-Rothschild, U-M associate professor of psychology.
“As alterations in dopamine signalling are associated with neurodegenerative diseases that also involve motor deficits and sleep disturbances, understanding these links could pave the way for improved therapeutics and advancements in human health,” she said.
The study focused on specific midbrain dopamine neurons that become active after learning, but only during nonrapid eye movement, or NREM, sleep. This burst of activity helps the brain fine-tune and reinforce newly learned movements, contributing to more precise motor performance once awake.
Understanding how dopamine supports motor learning at night also sheds light on the broader importance of sleep in shaping behavior, said Eban-Rothschild and colleagues.
“The findings highlight that sleep is an active biological period during which key neural circuits strengthen the skills and patterns we rely on every day,” she said.
By revealing how dopamine helps consolidate motor memories during sleep, the researchers say the findings open a new window into brain health: It may eventually guide the development of therapies that target both sleep and dopamine pathways, offering new hope for improving motor function and quality of life in affected individuals.
The study was published in the Journal Science Advances. In addition to Eban-Rothschild, the study’s authors are Bibi Alika Sulaman, Eric Chen, Aaron Crane, Sangjin Lee and Gideon Rothschild