
Breakthrough Drug Nearly Doubles Survival with Advanced Pancreatic Cancer
– an Oncologist Explains how Daraxonrasib Overcame an ‘Undruggable’ Disease

Christopher Lieu, University of Colorado Anschutz
For a long time, the likelihood of surviving pancreatic cancer has been extremely low. For patients who were diagnosed with metastatic pancreatic cancer between 2015 and 2021, about 97% died within five years of their diagnosis.
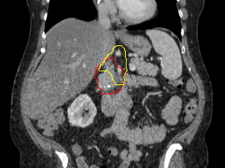
Pancreatic cancer is so deadly in part because there are no effective screening tests, and it rarely causes noticeable symptoms in its earliest stages. By the time a patient experiences signs, such as jaundice – a yellowing of the skin – or abdominal pain, the cancer has often already spread to other organs.
As a gastrointestinal oncologist and researcher specialising in early-phase clinical trials, I have seen the critical need for more effective therapies for patients with pancreatic cancer. For decades, successfully targeting the central mechanism that causes the vast majority of pancreatic cancers was considered impossible.
However, that narrative is rapidly changing with a new drug that can shut down the key protein that drives pancreatic cancer, nearly doubling survival rates for patients with advanced stages of the disease.
‘Undruggable’ tumours
The standard treatment for advanced pancreatic cancer has historically relied on chemotherapy, potent drugs designed to kill rapidly dividing cells. While chemotherapy can slow the progression of the disease, its effectiveness is often limited by the ability of pancreatic cancer cells to develop resistance against these drugs.
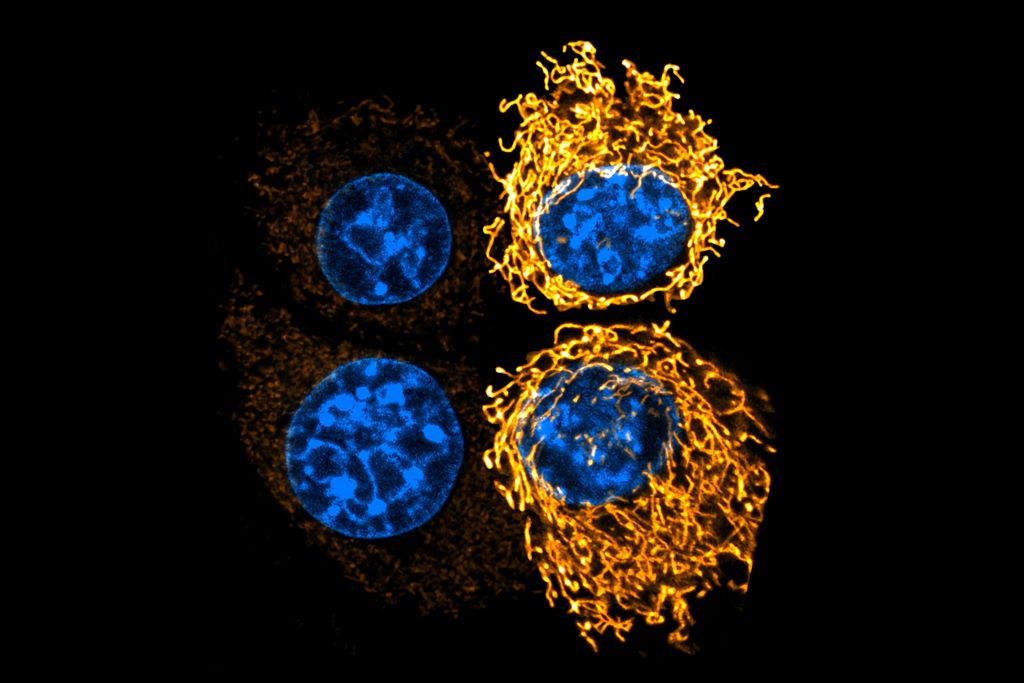
Pancreatic cancer’s success lies in its genetics. More than 90% of pancreatic tumours are driven by mutations in a gene called KRAS. This gene codes for proteins that function as switches that turn cell growth on and off. When the KRAS gene is mutated, the switch becomes permanently stuck in the “on” position, commanding cancer cells to multiply endlessly.
For decades, scientists considered KRAS to be “undruggable.” The surface of the protein is exceptionally smooth, lacking the molecular pockets that standard drugs require to bind to and turn the switch off.
Because existing drugs haven’t been able to target this protein, treatment for pancreatic cancer has primarily relied on toxic drugs that act more like blunt instruments than precise tools. Chemotherapy attempts to control the disease through widespread cell destruction, causing significant collateral damage to healthy tissues that lead to side effects.
What is daraxonrasib?
A new drug called daraxonrasib offers a critical advance in treating metastatic pancreatic cancer.
Daraxonrasib is taken daily by mouth. Instead of binding to KRAS directly, it attaches to a molecule called cyclophilin A in cells that helps fold proteins into their final 3D structures. This protein complex is then able to bind to the active KRAS protein and shut down its ability to signal cancer cells to multiply.
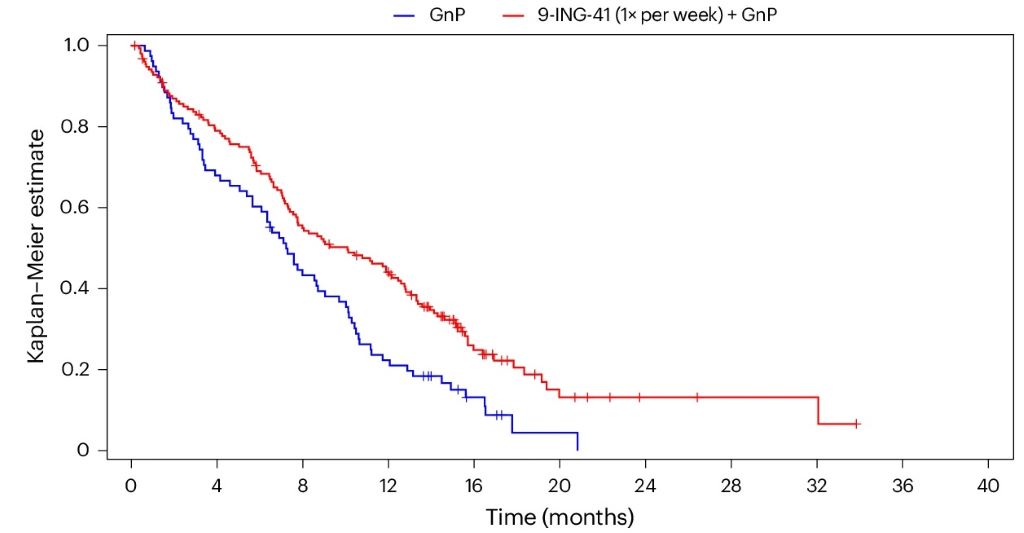
The company developing the drug, Revolution Medicines, presented results on May 31, 2026, from its Phase 3 clinical trial of 500 patients with metastatic pancreatic cancer who had received prior treatment. Compared to standard chemotherapy, daraxonrasib nearly doubled overall survival from 6.7 months to 13.2 months after diagnosis. Overall, daraxonrasib reduced the risk of death for metastatic pancreatic cancer patients by 60%. https://www.youtube.com/embed/sIspXSWQn1w?wmode=transparent&start=0 Daraxonrasib nearly doubled survival for patients with advanced pancreatic cancer compared to chemotherapy.
The most common side effect is a prominent skin rash, which affected more than 86% of patients in the study. Patients also frequently dealt with stomatitis – painful swelling and sores inside the mouth – as well as diarrhoea, nausea and vomiting. However, patients taking daraxonrasib were far less likely to stop treatment due to severe side effects compared to chemotherapy, and they had improved quality of life with reduced pain.
Next steps for daraxonrasib
By successfully targeting the specific genetic mutation that drives the vast majority of pancreatic cancers, researchers have demonstrated that this “undruggable” disease is treatable with targeted therapy.
The immediate next step is regulatory review of the drug’s readiness for the clinic. With data now officially published, Revolution Medicines will use these findings to seek formal approval from the Food and Drug Administration and other global regulatory bodies.
Because advanced pancreatic cancer is notoriously difficult to treat, breakthrough therapies that demonstrate this kind of significant survival benefit are often granted expedited or priority review. When daroxonrasib becomes available to patients will depend on the review timeline. Should the drug obtain approval, it could be available in clinics within months.
For the broader landscape of drug development, this milestone represents a likely shift in pancreatic cancer treatment. I expect more clinical trials exploring combination therapies pairing KRAS inhibitors with other drugs to prevent tumours from developing resistance to treatment.
Should daraxonrasib succeed, it could help set the stage for more precise, personalised and effective treatments for pancreatic cancer in the years to come.
Christopher Lieu, Professor of Medical Oncology, University of Colorado Anschutz
This article is republished from The Conversation under a Creative Commons license. Read the original article.



{kind=link}