Throwing a little heat on your meal might be an effective strategy for cutting back on calories, according to a new study led by researchers at Penn State.
Scientists at the University’s Sensory Evaluation Center examined how increasing “oral burn” – the spicy taste from ingredients like chili pepper – affects how much food people consume during a meal. The findings, available online now and slated to publish in the October issue of the journalFood Quality and Preference, suggest that making the meal slightly spicier led participants to eat less, consuming fewer calories.
“We know from previous studies that when people slow down, they eat significantly less,” said Paige Cunningham, a postdoctoral researcher and lead author on the study who earned her doctorate in nutritional sciences from Penn State in 2023. “We suspected that making a meal spicier might slow people down. We thought, let’s test, under controlled experimental conditions in the lab, if adding a small amount of spice, but not so much that the meal is inedible, will make people eat slower and therefore eat less.”
The researchers found that increasing spiciness slightly using dried chili pepper slowed down eating and reduced the amount of food and energy consumed at a meal, all without negatively affecting the palatability of the dish.
“This points to added chilies as a potential strategy for reducing the risk of energy overconsumption,” said John Hayes, Penn State professor of food science and corresponding author on the paper. “While portion control wasn’t the explicit goal of this study, our results suggest this might work. Next time you’re looking to eat a little less, try adding a blast of chilies, as it may slow you down and help you eat less.”
Plastic pollution is one of the defining environmental challenges of our time – and some of nature’s tiniest organisms may offer a surprising way out.
In recent years, microbiologists have discovered bacteria capable of breaking down various types of plastic, hinting at a more sustainable path forward.
These “plastic-eating” microbes could one day help shrink the mountains of waste clogging landfills and oceans. But they are not always a perfect fix. In the wrong environment, they could cause serious problems.
Plastics are widely used in hospitals in things such as sutures (especially the dissolving type), wound dressings and implants. So might the bacteria found in hospitals break down and feed on plastic?
Get your news from actual experts, straight to your inbox.Sign up to our daily newsletter to receive all The Conversation UK’s latest coverage of news and research, from politics and business to the arts and sciences.
To find out, we studied the genomes of known hospital pathogens (harmful bacteria) to see if they had the same plastic-degrading enzymes found in some bacteria in the environment.
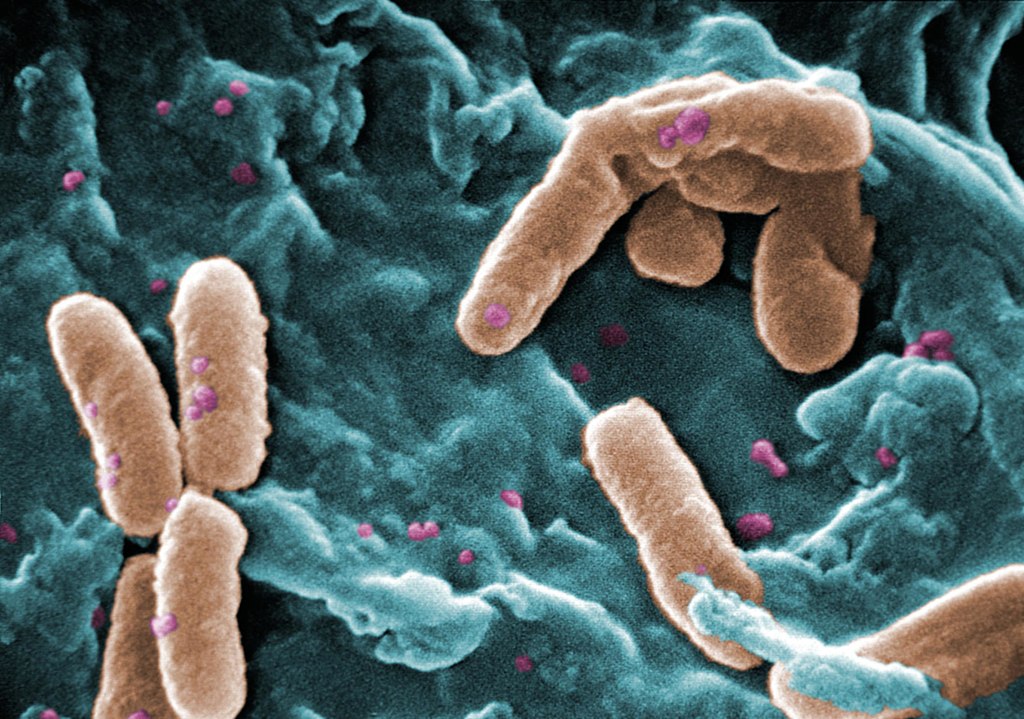
Pseudomonas bacteria. Source: Wikimedia CCO
We were surprised to find that some hospital germs, such as Pseudomonas aeruginosa, might be able to break down plastic.
P aeruginosa is associated with about 559,000 deaths globally each year. And many of the infections are picked up in hospitals.
Patients on ventilators or with open wounds from surgery or burns are at particular risk of a P aeruginosa infection. As are those who have catheters.
We decided to move forward from our computational search of bacterial databases to test the plastic-eating ability of P aeruginosa in the laboratory.
We focused on one specific strain of this bacterium that had a gene for making a plastic-eating enzyme. It had been isolated from a patient with a wound infection. We discovered that not only could it break down plastic, it could use the plastic as food to grow. This ability comes from an enzyme we named Pap1.
Biofilms
P aeruginosa is considered a high-priority pathogen by the World Health Organization. It can form tough layers called biofilms that protect it from the immune system and antibiotics, which makes it very hard to treat.
Our group has previously shown that when environmental bacteria form biofilms, they can break down plastic faster. So we wondered whether having a plastic-degrading enzyme might help P aeruginosa to be a pathogen. Strikingly, it does. This enzyme made the strain more harmful and helped it build bigger biofilms.
To understand how P aeruginosa was building a bigger biofilm when it was on plastic, we broke the biofilm apart. Then we analysed what the biofilm was made of and found that this pathogen was producing bigger biofilms by including the degraded plastic in this slimy shield – or “matrix”, as it is formally known. P aeruginosa was using the plastic as cement to build a stronger bacterial community.
Pathogens like P aeruginosa can survive for a long time in hospitals, where plastics are everywhere. Could this persistence in hospitals be due to the pathogens’ ability to eat plastics? We think this is a real possibility.
Many medical treatments involve plastics, such as orthopaedic implants, catheters, dental implants and hydrogel pads for treating burns. Our study suggests that a pathogen that can degrade the plastic in these devices could become a serious issue. This can make the treatment fail or make the patient’s condition worse.
Thankfully, scientists are working on solutions, such as adding antimicrobial substances to medical plastics to stop germs from feeding on them. But now that we know that some germs can break down plastic, we’ll need to consider that when choosing materials for future medical use.
A tender for a circumcision device, set to be used in all provincial health care centres and the military, is under legal scrutiny amid claims that the device is untested and unsafe.
Unicirc Pty Ltd has filed papers in the Pretoria High Court seeking to review and set aside the award of the tender to CircumQ RF Pty Ltd amid claims that the CircumQ device is “vastly inferior” compared to its own and others.
In his founding affidavit, Dr Cyril Norman Parker said that the application was “in the public interest” to ensure only safe and proven surgical devices are used in circumcision procedures.
“There is no publicly available information even to suggest that CircumQ’s device is such a device,” he said.
Parker – who has extensive circumcision experience – and his wife, Elizabeth Pillgrab-Parker, co-founded and continue to work in two primary health care centres they established in Mitchells Plain and Sea Point in the Western Cape under the auspices of Simunye Health Care.
Parker says he has worked in the area of male circumcision for 30 years, in particular as an HIV prevention strategy.
They are also the co-directors of Unicirc, which has the licence to distribute and sell a single-use circumcision device for safe and cost effective circumcision. The device “has significant capacity for scaling up circumcision procedures”, Parker said.
Unicirc bid for the tender for the supply of a surgical aid to be used at the nine departments of health and the Department of Defence.
Parker said he and his wife set up the Simunye health care centres when HIV prevalence was high.
“The conclusive results of three landmark clinical trials gave cause for optimism that circumcision could reduce female to male transmission of HIV by between 50 and 60%,” he said.
In terms of a policy decision taken by the National Department of Health, circumcision services were offered to all males aged ten and above.
“Our role, as service providers, is to ensure that we provide that service safety. In so far as ten to 14-year-olds, this means the strict use of device-based methods that avoid the need for sutures which brings complication rates down to less than 1.5%.”
He said he had performed over 3000 circumcisions across all age groups using multiple techniques.
“What is absolutely clear is that in order to provide services to everyone in need, a surgical-only approach has to be abandoned in favour of a device approach. But not all devices are the same.
“We conceptualised the development of a new circumcision device to improve safety, efficiency and accessibility.”
He said the Unicirc device, which is manufactured overseas, allowed for a complete circumcision in one visit, performed by a single health care provider, using a local anaesthetic and without any sutures.
The whole procedure is completed in about ten to 12 minutes and with proper training, it can also be performed by nurses.
“It has now been used for more than ten years by a range of different health care providers. More than 7,500 procedures have been performed in all ages in both public and private health care sectors. No severe adverse events have been reported and excellent cosmetic results have been achieved.
“It has resulted in the doubling of the number of circumcisions that can be performed safely in a day, a significant reduction in complications and increased client satisfaction,” Parker said.
When the World Health Organisation (WHO) published its (device) guidelines in 2020, only the Unicirc device came close to meeting the requirements. The manufacturer had now started the process of securing WHO pre-qualification. (WHO pre-qualified devices have to meet strict standards of quality, safety and efficacy.)
The device had also been tested in medical trials.
In contrast, Parker said, very little was known publicly about the CircumQ device.
“I am not aware of any peer-reviewed publications that consider its use. It has not been reviewed in any of the WHO literature I have perused or in any systematic review of circumcision devices that I have read. This is in contrast to the Unicirc device as well as other products.
“While I have come across two studies, I have not been able to find out anything about this research and I have not seen any evidence to suggest that it is close to being prequalified or even evaluated by WHO.”
Parker said however, he had studied its design, read training material and spoken to various experts and researchers and health care workers who had used that device and later attended training on the Unicirc device.
“It is vastly inferior. Sutures are required, increasing healing time and requiring a follow up visit. It increases patient discomfort and the risk of infection, the procedure takes longer and it’s more difficult to scale up because it requires two operators,” he said.
“But it’s not just a question of which device is better. There is simply no scientific data supporting the use of it.
“In the absence of that, it would be highly irresponsible to recommend its use, especially in the vulnerable ten to 14 age group. It places young boys at unnecessary risk of potentially irreparable harm and undermines the circumcision programme as a whole.”
He said while the tender was awarded in August 2023, “the public health system was far from ready to implement it”.
This was apparent from a letter from National Treasury, dated March 2025, in which it was stated that because of delays in training, service providers were allowed to continue using the conventional dorsal slit surgical method.
Parker submitted that the tender should be reviewed and set aside, and a new bidding process should start afresh.
Unicirc has called on the Treasury to provide a record of its decision-making process after which it may file a further affidavit. This will be provided by 30 May.
So far only the Treasury respondents have filed notices of opposition and they have yet to file affidavits.
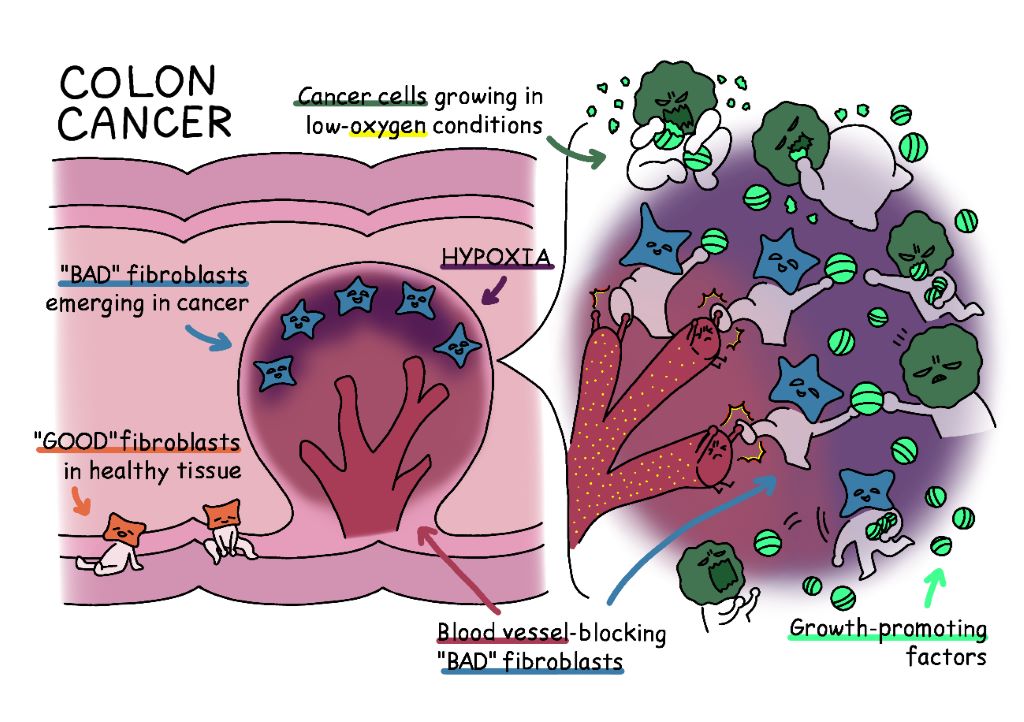
Fig. 1. In healthy colon tissue, “good” fibroblasts help support tissue architecture. However, in colon cancer, these fibroblasts transform into “bad” fibroblasts in low-oxygen areas near the tumour surface. These “bad” fibroblasts block the formation of blood vessels, keeping their surroundings in an oxygen-deprived state, which supports their own survival. At the same time, they release growth-promoting factors that act like supplements for cancer cells. While it may seem unexpected that hypoxia supports tumour growth, this study reveals that localised hypoxic environments can accelerate cancer progression.
To effectively battle cancer, scientists must study the battlefield. Now, in a recent study published in Nature Communications, a multi-institutional research team including The University of Osaka has discovered some crucial intel: localised hypoxia in the colon cancer microenvironment can promote tumour growth.
Until recently hypoxia was thought to suppress tumour progression. Consequently, drugs that block the supply of oxygen to tumours were being used to treat cancers. But these treatments had mixed results; sometimes even accelerating tumour growth. Understanding why this happens has become an urgent question in cancer research.
“We uncovered a surprising mechanism by which hypoxia may promote tumour growth, and it involves the formation of cells called inflammatory fibroblasts,” explains lead author of the study, Akikazu Harada.
The research team found that when oxygen becomes scarce in certain areas of a colon tumour, the surrounding fibroblasts (normally ‘good’ cells that support tissue structure) transform into harmful inflammatory fibroblasts. The altered cells release factors that help tumours grow, such as epiregulin. In addition, they release Wnt5a protein, which helps maintain a low-oxygen state by inhibiting new blood-vessel formation at the site of its release, thereby maintaining hypoxia.
To validate the findings from the mouse model in human samples, the researchers pooled data from human samples obtained from patients with a healthy colon, colon cancer, and those with inflammatory bowel disease. Later, they analysed the data and compared their findings with data from mice.
“We found that the malignant transformation of fibroblasts and the induction of Wnt5a-secreting fibroblasts are commonly observed in both mouse models and human samples,” says Akira Kikuchi, senior author of the study.
This insight into the potential pathology of colon cancer and inflammation can provide the blueprints for a new cancer battle strategy: drug therapies that target Wnt5a-producing fibroblasts. As a result, fibroblasts are now being recognised as a key ‘third’ therapeutic target, complementing traditional treatments targeting cancer cells and immune cells.
This finding holds special importance for colon cancer, which is the leading type of cancer in Japan. Additionally, the observed pathological changes of fibroblasts could also apply to chronic inflammatory disorders like inflammatory bowel disease, offering fresh insights into their mechanisms and potential new treatment strategies for these challenging conditions.
Johannesburg, 26 May 2025: Despite national guidelines and access to essential medicines, severe asthma remains under-recognised and inconsistently managed within South Africa’s healthcare system. It is therefore critical to address ongoing patient challenges, particularly regarding access to diagnostic tools, limited use of phenotyping, and the imperative to align clinical practice with international best practice recommendations.
The Severe Asthma Index 2025 found that South Africa scored below the global average in four out of five domains, revealing persistent gaps in policy coordination, equitable access, diagnostic capacity, and environmental health.¹ᵃ Of concern is the continued reliance on oral corticosteroids (OCS) without proper assessment or referral, especially where evidence-based, targeted biologics remain inaccessible or unfunded.1b+2a
Understanding asthma in South Africa
South Africa has robust asthma guidelines, but the absence of a national asthma strategy and lack of participation in global severe asthma registries limit insight into outcomes and weaken care coordination. Specialist care and phenotyping are largely confined to urban centres, and national data on hospitalisations and treatment outcomes is scarce. Although reported asthma-related societal costs and disability adjusted life years (DALYs) are relatively low, this likely masks the true burden among patients with severe, underdiagnosed, or poorly controlled disease.¹ᵇ Traditionally, asthma mortality in Southern Africa has been considered as relatively high due in large part to short-acting beta-agonists (SABAs) overuse.3
Environmental factors compound these challenges. High levels of particulate matter (PM2.5) and poor indoor air quality contribute significantly to disease severity, particularly in low-income areas. Meanwhile, access to advanced diagnostics and therapies remains limited. Biologic add-on therapies and fractional exhaled nitric oxide (FeNO) testing are not routinely available in the public sector, leaving most patients dependent on standard treatments with few options for escalation if the disease remains uncontrolled.¹ᵇ
Rethinking corticosteroid use
The Severe Asthma Index 2025 highlights the widespread use of oral corticosteroids (OCS) in South Africa as a persistent pattern that may pose long-term health risks if not carefully managed or replaced by more targeted therapies. While OCS play a critical role in treating acute exacerbations, frequent or prolonged use is linked to serious side effects, including osteoporosis, adrenal suppression, diabetes, and infections.²ᶜ
“There’s growing awareness that long-term OCS use can lead to significant health risks,” says Dwayne Koot, Medical Manager at Sanofi South Africa. “For severe asthma, the shift is towards biologic therapies that specifically target the underlying inflammation, not just the symptoms.1c As a simple regimen (where available), inhaled corticosteroid–formoterol combinations are now recommended as the preferred reliever across all severity levels.3 If high-dose ICS-LABA is needed, its use should be limited to 3 – 6 months, prompting phenotyping and biologic therapy add-on if asthma is not controlled. Low-dose maintenance OCS should only be considered as a last resort if no other options are available.”
Improving diagnosis and referral
Access to diagnostic tools remains uneven across South Africa, particularly in the public sector. Spirometry is not routinely available at primary care level, while FeNO testing, oscillometry, and biomarker analysis are largely limited to research centres or private practices.¹ᵇ
“This makes it difficult to accurately diagnose, phenotype, and manage asthma, potentially leading to suboptimal treatment decisions and poorer patient outcomes,” says Koot.
“There’s an opportunity to enhance the referral pathway to specialists and expand access to advanced diagnostic tools by defining referral criteria and partnering with specialised centres,” Koot says. “Routine phenotyping at GINA step 5, crucial for tailoring treatment plans and identifying suitable candidates for biologic therapies, is currently limited in many healthcare settings. Expanding these capabilities would enable a more personalised approach to asthma management.”3
To help close these gaps, the Severe Asthma Index 2025 recommends piloting basic phenotyping tools such as eosinophil counts at regional hospitals, establishing asthma registries to monitor outcomes and access, and expanding clinician training in severe asthma diagnosis and escalation pathways.¹ᵇ “Better data and better training could transform how we identify and treat severe asthma,” says Koot.
Next steps for clinical practice
Healthcare professionals have a pivotal role to play in strengthening asthma care — from recognising poor control early to ensuring patients access the most appropriate treatment in a timely manner. This includes reassessing those with persistent symptoms, reinforcing correct inhaler technique, referring for further investigation when needed, and considering alternative therapies when conventional options are no longer sufficient.3
South Africa already has many of the essential components in place: national treatment guidelines, access to key medicines, and clinical expertise. The next step is to ensure that patients with severe asthma are consistently identified, supported, and offered the full range of available interventions.
“As the World Asthma Day 2025 theme reminds us, the goal is to ‘Make Inhaled Treatments Accessible for ALL’, because inhaled medications are vital not just for preventing attacks, but for controlling chronic inflammation,” says Koot. “We encourage healthcare practitioners and policy makers to help make appropriate, evidence-based asthma care a reality for every South African asthmatic .”
For more information about asthma management and Sanofi’s commitment to respiratory health, please visit www.sanofi.co.za
Minister of Health Dr Aaron Motsoaledi. Source: GCIS
By Anna Grimsrud and Sibongile Tshabalala-Madhlala
Minister of Health Dr Aaron Motsoaledi’s recent claim that over half a million people have been newly started on HIV treatment in less than six months has raised eyebrows in health circles. In this open letter, Anna Grimsrud and Sibongile Tshabalala-Madhlala, associated with CHANGE – South Africa, ask the Minister to explain numbers that, on the face of it, seem contradictory.
Dear Minister Motsoaledi,
We write to you in response to your 15 May 2025 press statement and subsequent remarks in Parliament on the current status of the national HIV, AIDS, and TB campaign.
You stated that since the launch of the Close the Gap campaign, 520 700 people have been initiated on HIV treatment, reaching “more than 50% of the target”. You also stated that 5.9 million people are currently on antiretroviral therapy (ART). However, at the campaign’s launch on 25 February 2025, you reported the same number on HIV treatment — 5.9 million. This raises a critical question: if over half a million people have started or restarted treatment, why has the total number of people on treatment not increased?
If both figures are accurate, this would mean that approximately 520 000 people have been lost from care over the past few months — a deeply concerning and unprecedented level of attrition. We respectfully request that you provide the underlying data and clarify the current total number of people remaining on HIV treatment.
There are several reasons why we are concerned:
Static treatment numbers: As noted, the number on treatment was reported as 5.9 million in both February and May 2025. If 520 700 people have been initiated or re-initiated during this period, the same number must have exited care — a scenario that requires urgent explanation.
Slow growth in the number of people on treatment: According to official statements, the total number of people on HIV treatment increased by only 100 000 between March and December 2023 — from over 5.7 million to 5.8 million. The claim that the cohort has now grown by over 500 000 in a matter of months contradicts recent trends.
Declining lab numbers: National Health Laboratory Service data reported by the Daily Maverick and Reuters, show notable declines in viral load testing and early infant diagnosis in March and April 2025 compared to the same months in 2024. These indicators should increase alongside meaningful growth in treatment uptake — not decrease.
In light of these concerns, we believe it is essential that you provide a transparent accounting of the current number of people on treatment and the metrics being used to assess progress under the Close the Gap campaign. Specifically, we request data demonstrating that the programme is on track to meet its stated goal: increasing the number of people on treatment from 5.9 million to 7 million.
We share your commitment to a strong and effective HIV response, especially in this period of financial and operational strain. Like you, we believe it is vital that accurate and complete information is shared with the public and Parliament at this critical moment.
*Anna Grimsrud is an epidemiologist with a PhD in Public Health and writes in her personal capacity. Sibongile Tshabalala-Madhlala is openly living with HIV and currently serves as the National Chairperson of the Treatment Action Campaign (TAC).” CHANGE is a coalition of more than 1 500 people from civil society organizations in South Africa and around the work — people living with HIV, activists, community health workers, researchers, programme members, epidemiologists, clinicians, economists, and others. CHANGE stands for Community Health & HIV Advocate Navigating Global Emergencies.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
Republished from Spotlight under a Creative Commons licence. Views expressed in the original article are not necessarily shared by Quicknews.
Research confirms that social isolation and loneliness significantly impact health and mortality, even if not listed on death certificates. Brigham Young University psychology and neuroscience professor, Julianne Holt-Lunstad, has published extensively on the topic, including a landmark 2010 meta-analysis and a 2023 framework on assessment and treatment. She also served as lead scientist on the 2023 Surgeon General Advisory and is advising the World Health Organization on an upcoming report that addresses the pressing health threat of loneliness and isolation and a global agenda on social connection.
Social connection is now a legitimate health factor, but Holt-Lunstad and doctoral student, Andrew Proctor, recently published two studies showing that most of us (the general population and medical providers) still don’t think social connection affects physical health. And even the professionals who recognise the importance report that they don’t have time or tools to help patients address social concerns.
Proctor, who authored a study recently published in Springer Nature, explained that before the study, they had been watching how the pandemic was influencing internet searches around the topics of isolation and loneliness.
“I have a marketing background, so I thought that maybe the public perception had changed since COVID. Social distancing, isolation and loneliness were huge buzzwords on the internet as seen through Google Trends and BuzzSumo (an online trend analyzer). Everything around these search terms was super viral during that time, and so we wondered if perceptions about social connection had changed,” said Proctor.
With loneliness and isolation trending on the internet, the researchers set up a study. In a nationally representative sample of US adults, as well as samples from the UK and Australia, they surveyed 2,392 people about their perceptions of health risks associated with isolation and loneliness. The data showed that, despite the pandemic and other campaigns, people still underestimate the importance of social connection for physical health. And the underestimation exists equally among the lonely and the socially connected.
“The study identified blind spots in medical care,” said Proctor. “Social connection is like a vital sign. What if we didn’t care about high blood pressure? Or what if we never knew smoking was bad for us? Social connection is like a key vital sign. We just don’t tend to recognize it.”
In a closely connected study, Holt-Lunstad and Proctor, along with coauthors from top research medical centers, surveyed 681 healthcare providers (primarily doctors) about perceptions of health risks associated with poor social connection. Similar to the general population from the first study, healthcare providers underestimated social connection as a medically relevant health factor.
The researchers gleaned some unexpected insights due to an unintentional time lag in data collection in the second study.
“We completed the data collection at two different time points because we were waiting for institutional approvals. Our first cohort was healthcare providers through the University of Utah Health System. Slightly later, we had a second major cohort of University of California San Francisco (UCSF) physicians,” said Holt-Lunstad. “What was interesting is that the perceived importance of social factors was a bit higher among the UCSF group.”
A Geisinger study provides new insight into height differences between adult men and women, demonstrating that Y chromosome genes contribute more to height than their X chromosome counterparts, independent of male sex determination. The results were published this week in the Proceedings of the National Academy of Sciences.
Typical females have two X chromosomes, while typical males have one X and one Y chromosome. The differences between the X and Y chromosomes cause hormonal differences between males and females, but these differences have been insufficient to explain the average 13cm height difference between the sexes.
“Because height shows a large and reproducible difference between sexes and is widely measured, it serves as a valuable model for investigating the genomic factors underlying sex differences,” said Matthew Oetjens, Ph.D., assistant professor in Geisinger’s Department of Developmental Medicine and one of the study leads.
The Geisinger research team sought to determine the effects of sex-related factors on human height by examining height in people with an abnormal number of X or Y chromosomes, a genetic condition known as sex chromosome aneuploidy.
The team analysed genetic and clinical data on nearly one million participants enrolled in Geisinger’s MyCode Community Health Initiative, the National Institutes of Health’s All of Us cohort and the UK Biobank. Of these participants, 1225 had a sex chromosome aneuploidy. By incorporating people with more or fewer than two sex chromosomes into a model of height, they found that exchanging an X for a Y chromosome increased height by 3.1cm, independent of other sex-related factors, including hormonal differences. This result suggests that an estimated 23% of the average difference in height between men and women is explained by increased expression of shared genes on the Y chromosome relative to the X chromosome.
“Beyond its implications for understanding human height, this study provides broader insights into how sex chromosome aneuploidy research can uncover the mechanisms behind observed sex differences in various medical conditions,” said Alexander Berry, PhD, bioinformatics scientist and study co-lead.
SHOX, a gene found on both the X and Y chromosomes, is a known contributor to human height, but because two copies are found in both men and women, it has not been considered a likely contributor to the sex difference in height. However, recent studies have shown that SHOX is partially silenced on the second X chromosome in individuals with two or more X chromosomes. The Geisinger study’s results are consistent with the hypothesis that reduced SHOX expression in females results in a net difference in height between the sexes.
Genetic mutations and cell maturity as key factors in acute myeloid leukaemia drug resistance
Photo by Tima Miroshnichenko on Pexels
An international study led by the University of Colorado Cancer Center has uncovered why a widely used treatment for acute myeloid leukaemia (AML) doesn’t work for everyone. The findings could help doctors better match patients with the therapies most likely to work for them.
Researchers analysed data from 678 AML patients, the largest group studied to date for this treatment, and found that both gene mutations and the maturity of leukaemia cells affect how patients respond to a drug combination of venetoclax and hypomethylating agents (HMA).
“Venetoclax-based therapies are now the most common treatment for newly diagnosed AML,” said Daniel Pollyea, MD, MS, professor of medicine at University of Colorado. “But not all patients respond the same way. Our goal was to figure out why and give doctors better tools to predict outcomes at the start.”
Mutations and maturity of leukaemia cells
AML is a fast-growing cancer of the blood and bone marrow, most often seen in older adults. Many patients can’t tolerate traditional chemotherapy, so doctors treat them with venetoclax plus HMA. This combination has improved survival for many, but some patients still relapse or don’t respond.
The study found that patients with a certain type of AML, called “monocytic,” had worse outcomes especially if they did not have a helpful gene mutation known as NPM1. These patients were also more likely to carry other mutations, such as KRAS, that are linked to drug resistance.
“Patients with monocytic AML and no NPM1 mutation were nearly twice as likely to die from the disease,” said Pollyea. “So, it’s not just about the gene mutations. It’s also about how developed or mature the cancer cells are when treatment begins.”
Previous research often focused only on either genetic mutations or cell type. Pollyea’s team looked at both, giving them a clearer understanding of how these two factors work together to influence treatment response.
Designing therapies that shut down cancer cell escape routes
“We learned that some cancer cells basically find a back door to evade the treatment,” said Pollyea. “By identifying how and why that happens, we can begin designing therapies that shut down those escape routes.”
This is a powerful new way to classify AML patients by risk, enabling doctors to better predict who is likely to respond to venetoclax and who might need another approach.
“This is a major step toward personalised medicine in AML,” said Pollyea. “We’re moving closer to a world where we can look at a patient’s leukaemia on day one and know which therapy gives them the best chance and ultimately improve survival rates.”
Pollyea and his team are working to expand the study with even more patient data and hope to design a clinical trial that uses this model to guide treatment decisions.
Selective serotonin reuptake inhibitors (SSRIs) could help the immune system fight cancer, according to recent UCLA research. The study, published in Cell, found that SSRIs significantly enhanced the ability of T cells to fight cancer and suppressed tumour growth across a range of cancer types in both mouse and human tumour models.
“It turns out SSRIs don’t just make our brains happier; they also make our T cells happier – even while they’re fighting tumours,” said Lili Yang, PhD, senior author of the new study. “These drugs have been widely and safely used to treat depression for decades, so repurposing them for cancer would be a lot easier than developing an entirely new therapy.”
According to the CDC, one out of eight adults in the US takes an antidepressant, and SSRIs are the most commonly prescribed. These drugs increase levels of serotonin the brain’s “happiness hormone” by blocking the activity of a protein called serotonin transporter, or SERT.
While serotonin is best known for the role it plays in the brain, it’s also a critical player in processes that occur throughout the body, including digestion, metabolism and immune activity.
Dr Yang and her team first began investigating serotonin’s role in fighting cancer after noticing that immune cells isolated from tumours had higher levels of serotonin-regulating molecules. At first, they focused on MAO-A, an enzyme that breaks down serotonin and other neurotransmitters, including norepinephrine and dopamine.
In 2021, they reported that T cells produce MAO-A when they recognise tumours, which makes it harder for them to fight cancer. They found that treating mice with melanoma and colon cancer using MAO inhibitors, also called MAOIs – the first class of antidepressant drugs to be invented – helped T cells attack tumours more effectively.
However, because MAOIs have safety concerns, including serious side effects and interactions with certain foods and medications, the team turned its attention to a different serotonin-regulating molecule: SERT.
“Unlike MAO-A, which breaks down multiple neurotransmitters, SERT has one job – to transport serotonin,” explained Bo Li, PhD, first author of the study and a senior research scientist in the Yang lab. “SERT made for an especially attractive target because the drugs that act on it – SSRIs – are widely used with minimal side effects.”
The researchers tested SSRIs in mouse and human tumour models representing melanoma, breast, prostate, colon and bladder cancer. They found that SSRI treatment reduced average tumour size by over 50% and made the cancer-fighting T cells, known as killer T cells, more effective at killing cancer cells.
“SSRIs made the killer T cells happier in the otherwise oppressive tumour environment by increasing their access to serotonin signals, reinvigorating them to fight and kill cancer cells,” said Dr Yang, who is also a professor of microbiology, immunology and molecular genetics and a member of the UCLA Health Jonsson Comprehensive Cancer Center.
How SSRIs could boost the effectiveness of cancer therapies
The team also investigated whether combining SSRIs with existing cancer therapies could improve treatment outcomes. They tested a combination of an SSRI and anti-PD-1 antibody – a common immune checkpoint blockade (ICB) therapy – in mouse models of melanoma and colon cancer. ICB therapies block immune checkpoint molecules that normally suppress immune cell activity, allowing T cells to attack tumours more effectively.
The results were striking: the combination significantly reduced tumour size in all treated mice and even achieved complete remission in some cases.
“Immune checkpoint blockades are effective in fewer than 25% of patients,” said James Elsten-Brown, a graduate student in the Yang lab and co-author of the study. “If a safe, widely available drug like an SSRI could make these therapies more effective, it would be hugely impactful.”
To confirm these findings, the team will investigate whether real-world cancer patients taking SSRIs have better outcomes, especially those receiving ICB therapies. About 20% of cancer patients are already taking the medication, Dr Yang said.
Dr Yang added that using existing FDA-approved drugs could speed up the process of bringing new cancer treatments to patients, making this research especially promising.
“Studies estimate the bench-to-bedside pipeline for new cancer therapies costs an average of $1.5 billion,” she said. “When you compare this to the estimated $300 million cost to repurpose FDA-approved drugs, it’s clear why this approach has so much potential.”