The Day Hospital Association of South Africa (DHASA) has joined the Hospital Association of South Africa (HASA), the representative organisation of private hospital groups in the country, including Netcare, Mediclinic, Life Healthcare, Lenmed, Joint Medical Holdings, and a range of leading facilities across the country like Zuid-Afrikaans Hospital and Arwyp Medical Centre.
Among the Day Hospital Association of South Africa members are the Advanced Health chain, Cure Day Hospitals, and various leading treatment facilities situated nationwide.
According to HASA Chief Executive Officer Dr Dumisani Bomela, DHASA perspectives on healthcare reform issues, like the National Health Insurance, will contribute to a rich healthcare reform discussion.
He says, “Through HASA, the Day Hospital Association can provide additional critical perspectives that we believe are required in the collaborative approach that we are engaging in with Government to build a strong and accessible healthcare system for all in South Africa. We completely believe that the excellent leadership of DHASA will make full use of their membership in HASA to make their important contribution.”
The Chairman of the Day Hospital Association of South Africa, Raymond Foster, says “We are excited to be associated with HASA. We are confident that HASA will meet the expectations of our members.”
The South African Health Products Regulatory Authority (SAHPRA) has been designated as a Regional Centre of Regulatory Excellence (RCORE) for Vaccines Regulatory Oversight for a period of four (4) years in the following functions:
Overarching Regulatory Systems
Marketing Authorisation and Registration
Vigilance
Market Surveillance and Control
Licensing of Premises
Regulatory Inspections
Laboratory Access and Testing
Clinical Trials
Lot Release
The rationale behind the African Union Development Agency, New Partnership for Africa’s Development (AUDA-NEPAD) designating RCOREs is to support continent-wide regulatory systems strengthening through leveraging capacity in better resourced regulators. The reality of medicine regulatory capacity limitation on the continent continues to hinder access to essential medicines as well as limit progress in regulatory harmonisation efforts. The intention is to address this regulatory gap and ensure the acceleration and strengthening of regional medicines regulatory harmonisation initiatives. RCOREs are required to support regulatory workforce strengthening through training in regulatory functions and enhance skills through hands-on training and exchange programmes amongst National Medicines Regulatory Authorities.
About RCOREs
The Regional Centres of Regulatory Excellence (RCOREs) is an initiative of the AUDA-NEPAD. As part of its mandate to strengthen regulatory capacity development in Africa, AUDA-NEPAD through its AMRH programme has designated 11 RCOREs in eight different regulatory functions which include:
Pharmacovigilance
Training in core regulatory functions
Quality assurance and quality control of medicines
Medicine registration and evaluation, quality assurance/quality control and clinical trials oversight
Licensing of the manufacture, import, export, distribution and inspection and surveillance of manufacturers, importers, wholesalers and dispensers of medicine
Clinical trials oversight
Registration and evaluation and clinical trials oversight
Long overlooked by genetics, the Y chromosome is surprisingly quite challenging to sequence, and so its contributions to health and disease remain largely unknown. For the first time, the complete sequences of 43 human Y chromosomes from lineages from around the globe provides an essential step forward in understanding the roles of the Y chromosome in human evolution and biology. The researchers behind the effort published their findings in two papers in Nature.
Even as the field of human genomics forged ahead at an astonishing pace, the Y chromosome has long remained overlooked. It has been postulated that the human sex chromosomes once originated from a pair of structurally similar chromosomes, but subsequently one of the sex chromosomes, the ancestral Y chromosome, underwent significant degradation, losing 97%of its former complement of genes over many millions of years. This peculiar evolutionary trajectory has given rise to speculation that the human Y chromosomes might eventually disappear completely, albeit millions of years from now, and we already observe that some biological males do lose them in dividing cells as they age, with unclear health consequences.
In practical terms, the Y chromosome contains a large proportion of repetitive and heterochromatic (highly condensed, gene-poor and not transcribed to messenger RNA) sequences, making it exceptionally difficult to fully sequence. Using sequencing methods that can cover long, continuous sequences, the Telomere-to-Telomere (T2T) consortium has now published the first complete Y chromosome assembly from a single individual of European descent in Nature. At the same time, a team led by Jackson Laboratory (JAX) Professor and The Robert Alvine Family Endowed Chair Charles Lee, PhD, FACMG, has published, also in Nature, the assembled Y chromosomes from 43 unrelated males, with nearly half coming from African lineages. These two papers provide intriguing insights into human Y chromosomes, reveal the highly variable nature of Y chromosomes across individuals, and provide an important foundation for future studies on how they may be contributing to certain disorders and diseases.
The need for long reads
Standard short-read genomic sequencing technologies require breaking genomic DNA into short (~250-base-long) fragments. These fragments are then reassembled into the full genome of more than 3 billion base pairs across 46 chromosomes in humans. The method is very accurate and works well for most, but not all, of the genome. Almost all “complete” human genome sequences, including the current reference genome sequence (known as GRCh38), are actually only about 90% complete, because it is difficult to assemble the highly repetitive and other complex sections accurately. GRCh38 falls particularly short for the Y chromosome, as it barely assembles half of that chromosome.
As a result, while the much larger and gene-rich X chromosome has been extensively studied, the Y chromosome has been often overlooked outside of male-based fertility studies. In a significant step forward for the genomics field, scientists from JAX, including first author and JAX Associate Research Scientist, Pille Hallast, PhD, with collaborators from Clemson University, Heinrich Heine University (Germany) and more, have now revealed a full picture of the Y chromosome’s key characteristics and differences between individuals for the first time. Of note is the striking variation in size and structure across the 43 Y chromosomes sequenced that covered 180 000 years of human evolution and range from 45.2 million to 84.9 million base pairs in length.
The inclusion of 43 different individuals representing diverse Y lineages allowed the researchers to redefine inter-chromosomal region boundaries and identify large-scale variations at an unprecedented resolution and clarity. The study also revealed an unexpected degree of structural variation across the Y chromosomes. For example, half of the euchromatin (gene-rich region) of the sequenced chromosomes carries large recurrent inversions (segments that contain the same nucleotide sequences but oriented in the opposite direction) at a rate much higher than anywhere else in the genome. The study further identified regions of the Y chromosome that demonstrate little single nucleotide variation but show high gene copy number variation for specific gene families. Other gene families tended to maintain their copy numbers, however, consistent with their roles in fertility and normal development.
Role in overall health
“Having fully resolved Y chromosome sequences from multiple individuals is essential in order for us to begin to understand how this variation can affect function” says Hallast. “The degree of structural variation between individuals came as a big surprise to me, even though the nucleotide sequences within the Y chromosome genes are comparatively conserved. The variable gene copy numbers in certain gene families and extremely high inversion rates are almost certain to hold significant biological and evolutionary roles.”
The Y chromosome’s contributions to male health are poorly understood. Some unexpected indications of its importance to human health have recently come into focus in two new research studies that collectively implicate the Y chromosome in aggressive features of colorectal and bladder cancers in men. Indeed, one of the studies showed that tumors that had lost the Y chromosomes can more effectively evade T cell immunity, are infiltrated with higher numbers of dysfunctional CD8+ T cells, and are more responsive to anti-PD1 treatments compared to similar tumors retaining the Y chromosome.
“Research is emerging that shows proper Y chromosome gene function is incredibly important for the overall health of men,” says Lee, senior author on the paper. “Our study enables the inclusion of the full Y chromosome in all future studies when sequencing male genomes to understand health and disease.”
Bada Pharasi, CEO of The Innovative Pharmaceutical Association of South Africa (IPASA)
Lessons from the COVID-19 pandemic have underlined the importance of continued investment into pharmaceutical innovation and R&D to not only bring life-saving medications to those in need, but to improve public health outcomes, writes Bada Pharasi, CEO of The Innovative Pharmaceutical Association of South Africa (IPASA).
From treatments for cancer, cardiovascular diseases and more recently, the COVID-19 vaccine, the pharmaceutical industry has made significant progress in the development of over 470 medications in the last 10 years alone.1
While the innovative pharmaceutical process typically takes between 10 and 15 years from discovery to regulatory approval2 – owing to factors including immense R&D costs, regulatory compliance, and the protection of patents3 – the fast-tracked development and approval of COVID-19 vaccines laid bare the need for pharmaceutical companies to be prepared to mitigate the risk of future outbreaks – and this means continued investment in innovation and R&D.
The pandemic underlined the need for countries to be prepared for outbreaks on the horizon. To ensure we can meet the next challenge, pharmaceutical innovations must match the pace at which diseases mutate. This kind of innovation is non-negotiable and requires continued investment as a safeguard against losing lives and endangering South Africa’s fragile healthcare system.
As we are in the midst of a cholera epidemic, as well as the recent measles outbreak,4 it’s important to continue driving innovation to treat diseases, with medicines developed by innovative pharmaceutical companies benefiting millions across the country every day.
This is evidenced by mortality rates for HIV/AIDS and TB in the country falling by 59.2% and 55.7% between 2007 and 2017, with at least 60 new medicines currently in the R&D pipeline to treat TB.5
While patents in pharmaceutical innovation protect the originators’ intellectual property, it is important that innovative medications be developed to ensure a continuous pipeline of access to generics once the patent has lost its exclusivity. This will drive consumer accessibility and affordability of life-saving treatments and medications that may otherwise be unattainable for many.
As we continue racing against the proverbial clock in protecting against current and future diseases, pharmaceutical companies should continue to invest in innovation and R&D to outsmart existing dreaded diseases, and provide agility and preparedness should the next unknown pandemic threaten. Our health, and lives, depend on it.
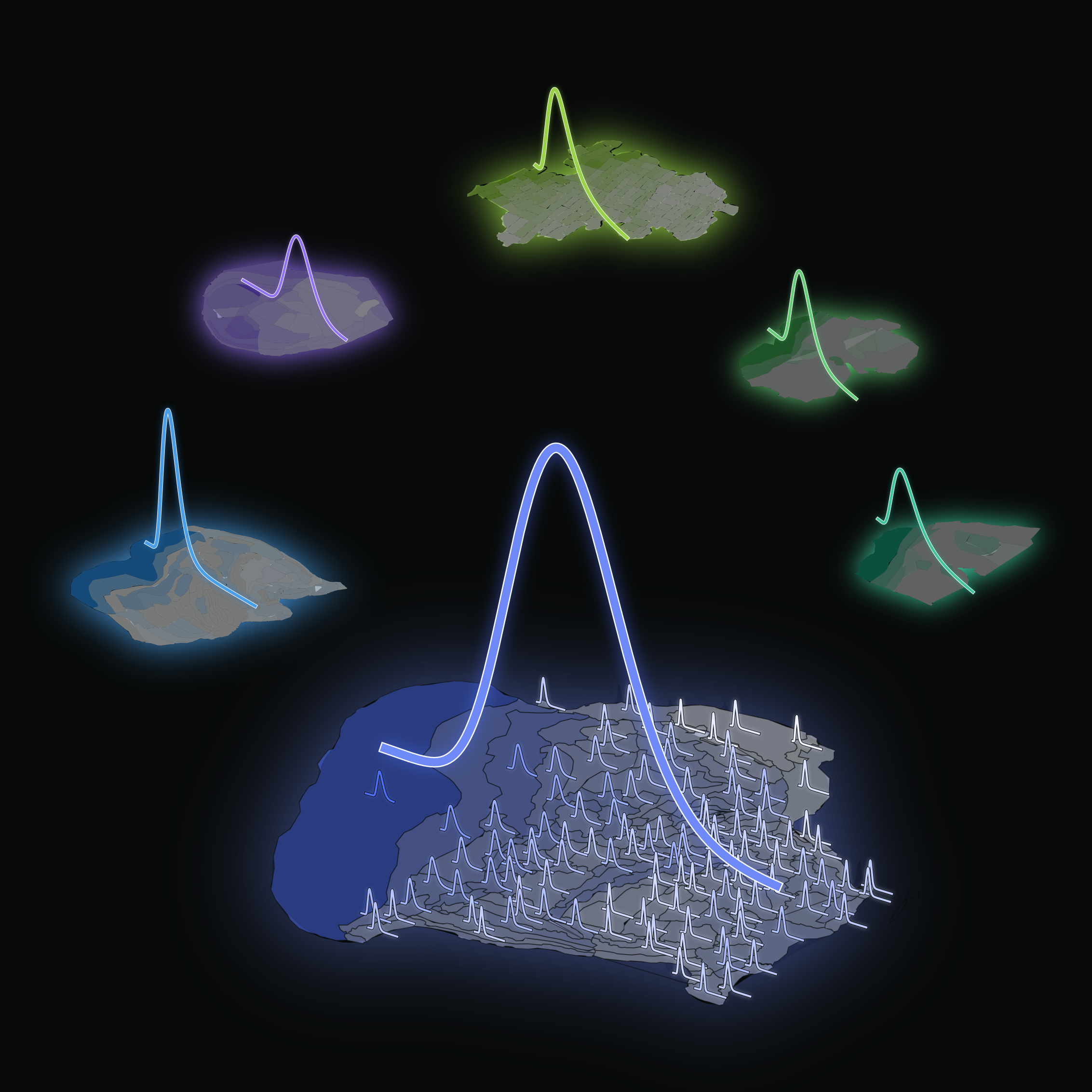
Neuron densities in cortical areas in the mammalian brain follow a consistent distribution pattern. Image: Morales-Gregorio
Human Brain Project (HBP) researchers have uncovered how neuron densities are distributed across and within cortical areas in the mammalian brain. As reported in Cerebral Cortex, they have revealed a fundamental organisational principle of cortical cytoarchitecture: the ubiquitous lognormal distribution of neuron densities.
Numbers of neurons and their spatial arrangement play a crucial role in shaping the brain’s structure and function. Yet, despite the wealth of available cytoarchitectonic data, the statistical distributions of neuron densities remain largely undescribed. This new study from the HBP at Forschungszentrum Jülich and the University of Cologne (Germany) study advances our understanding of the organisation of mammalian brains.
The team accessed 9 publicly available datasets of seven species: mouse, marmoset, macaque, galago, owl monkey, baboon and human. After analysing the cortical areas of each, they found that neuron densities within these areas follow a consistent pattern – a lognormal distribution, pointing to a fundamental organisational principle underlying the densities of neurons in the mammalian brain.
A lognormal distribution is a statistical distribution characterised by a skewed bell-shaped curve. It arises, for instance, when taking the exponential of a normally distributed variable. It differs from a normal distribution in several ways. Most importantly, the curve of a normal distribution is symmetric, while the lognormal one is asymmetric with a heavy tail.
These findings are relevant for modelling the brain accurately. “Not least because the distribution of neuron densities influences the network connectivity,” says Sacha van Albada, leader of the Theoretical Neuroanatomy group at Forschungszentrum Jülich and senior author of the paper. “For instance, if the density of synapses is constant, regions with lower neuron density will receive more synapses per neuron,” she explains. Such aspects are also relevant for the design of brain-inspired technology such as neuromorphic hardware.
“Furthermore, as cortical areas are often distinguished on the basis of cytoarchitecture, knowing the distribution of neuron densities can be relevant for statistically assessing differences between areas and the locations of the borders between areas,” van Albada adds.
These results are in agreement with the observation that surprisingly many characteristics of the brain follow a lognormal distribution. “One reason why it may be very common in nature is because it emerges when taking the product of many independent variables,” says Alexander van Meegen, joint first author of the study. In other words, the lognormal distribution arises naturally as a result of multiplicative processes, similarly to how the normal distribution emerges when many independent variables are summed.
“Using a simple model, we were able to show how the multiplicative proliferation of neurons during development may lead to the observed neuron density distributions” explains van Meegen.
According to the study, in principle, cortex-wide organisational structures might be by-products of development or evolution that serve no computational function; but the fact that the same organisational structures can be observed for several species and across most cortical areas suggests that the lognormal distribution serves some purpose.
“We cannot be sure how the lognormal distribution of neuron densities will influence brain function, but it will likely be associated with high network heterogeneity, which may be computationally beneficial,” says Aitor Morales-Gregorio, first author of the study, citing previous works that suggest that heterogeneity in the brain’s connectivity may promote efficient information transmission. In addition, heterogeneous networks support robust learning and enhance the memory capacity of neural circuits.
Circadian disruption is a hallmark of Alzheimer’s disease, affecting nearly 80% of patients with issues such as difficulty sleeping and worsening cognitive function at night. Currently there are no treatments for Alzheimer’s that target this aspect of the disease.
A new study in Cell Metabolism from researchers at University of California San Diego School of Medicine has shown in mice that it is possible to correct the circadian disruptions seen in Alzheimer’s disease with time-restricted feeding, a type of intermittent fasting focused on limiting the daily eating window without limiting the amount of food consumed.
In the study, mice that were fed on a time-restricted schedule showed improvements in memory and reduced accumulation of amyloid proteins in the brain. The authors say the findings will likely result in a human clinical trial.
“For many years, we assumed that the circadian disruptions seen in people with Alzheimer’s are a result of neurodegeneration, but we’re now learning it may be the other way around – circadian disruption may be one of the main drivers of Alzheimer’s pathology,” said senior study author Paula Desplats, PhD, professor at UC San Diego School of Medicine. “This makes circadian disruptions a promising target for new Alzheimer’s treatments, and our findings provide the proof-of-concept for an easy and accessible way to correct these disruptions.”
People with Alzheimer’s experience a variety of disruptions to their circadian rhythms, including changes to their sleep/wake cycle, increased cognitive impairment and confusion in the evenings, and difficulty falling and staying asleep.
“Circadian disruptions in Alzheimer’s are the leading cause of nursing home placement,” said Desplats. “Anything we can do to help patients restore their circadian rhythm will make a huge difference in how we manage Alzheimer’s in the clinic and how caregivers help patients manage the disease at home.”
Boosting the circadian clock is an emerging approach to improving health outcomes, and one way to accomplish this is by controlling the daily cycle of feeding and fasting. The researchers tested this strategy in a mouse model of Alzheimer’s disease, feeding the mice on a time-restricted schedule where they were only allowed to eat within a six-hour window each day. For humans, this would translate to about 14 hours of fasting each day.
Compared to control mice who were provided food at all hours, mice fed on the time-restricted schedule had better memory, were less hyperactive at night, followed a more regular sleep schedule and experienced fewer disruptions during sleep. The test mice also performed better on cognitive assessments than control mice, demonstrating that the time-restricted feeding schedule was able to help mitigate the behavioral symptoms of Alzheimer’s disease.
The researchers also observed improvements in the mice on a molecular level. In mice fed on a restricted schedule, the researchers found that multiple genes associated with Alzheimer’s and neuroinflammation were expressed differently. They also found that the feeding schedule helped reduce the amount of amyloid protein that accumulated in the brain. Amyloid deposits are one of the most well-known features of Alzheimer’s disease.
Because the time-restricted feeding schedule was able to substantially change the course of Alzheimer’s in the mice, the researchers are optimistic that the findings could be easily translatable to the clinic, especially since the new treatment approach relies on a lifestyle change rather than a drug.
“Time-restricted feeding is a strategy that people can easily and immediately integrate into their lives,” said Desplats. “If we can reproduce our results in humans, this approach could be a simple way to dramatically improve the lives of people living with Alzheimer’s and those who care for them.”
Hours of inactivity during childhood could be setting the stage for heart attacks and strokes later in life, according to research presented at ESC Congress 2023. The large cohort study found that sedentary time accumulated from childhood to young adulthood was associated with heart damage – even in those with normal weight and blood pressure.
“All those hours of screen time in young people add up to a heavier heart, which we know from studies in adults raises the likelihood of heart attack and stroke,” said study author Dr Andrew Agbaje of the University of Eastern Finland, Kuopio, Finland. “Children and teenagers need to move more to protect their long-term health.”
This was the first study to investigate the cumulative effect of smartwatch-assessed sedentary time in young people and cardiac damage later in life. It was conducted as part of the Children of the 90s study, which began in 1990/1991 and is one of the world’s largest cohorts with lifestyle measurements from birth.
At 11 years of age, children wore a smartwatch with an activity tracker for seven days. This was repeated at 15 years of age and again at 24 years of age. The weight of the heart’s left ventricle was assessed by echocardiography, a type of ultrasound scan, at 17 and 24 years of age and reported in grams relative to height (g/m2.7). The researchers analysed the association between sedentary time between 11 and 24 years of age and heart measurements between 17 and 24 years of age after adjusting for factors that could influence the relationship including age, sex, blood pressure, body fat, smoking, physical activity and socioeconomic status.
The study included 766 children, of whom 55% were girls and 45% were boys. At 11 years of age, children were sedentary for an average of 362 minutes a day, rising to 474 minutes a day in adolescence (15 years of age), and 531 minutes a day in young adulthood (24 years of age). This means that sedentary time increased by an average of 169 minutes (2.8 hours) a day between childhood and young adulthood.
Each one-minute increase in sedentary time from 11 to 24 years of age was associated with a 0.004g/m2.7 increase in left ventricular mass between 17 to 24 years of age. When multiplied by 169 minutes of additional inactivity this equates to a 0.7g/m2.7 daily rise, the equivalent of a 3 gram increase in left ventricular mass between echocardiography measurements at the average height gain. A previous study in adults found that a similar increase in left ventricular mass (1g/m2.7) over a seven-year period was associated with a two-fold increased risk of heart disease, stroke, and death.4
Dr. Agbaje said: “Children were sedentary for more than six hours a day and this increased by nearly three hours a day by the time they reached young adulthood. Our study indicates that the accumulation of inactive time is related to heart damage regardless of body weight and blood pressure. Parents should encourage children and teenagers to move more by taking them out for a walk and limiting time spent on social media and video games. As Martin Luther King Jr. once said, ‘If you can’t fly, run. If you can’t run, walk. If you can’t walk, crawl. But by all means keep moving.'”
By HualinXMN – Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=133759262
According to results from the SELECT trial run by Novo Nordisk, semaglutide dramatically reduces the risk of major adverse cardiovascular events (MACEs) in addition to its obesity benefits. This is bolstered by the results of another trial, STEP-1, which also suggested significant reduction in future cardiovascular events. These results have captured the attention of researchers, who commented in Nature that they could change the practice of cardiology.
Semaglutide, sold in the US for the treatment of both obesity (Wegovy) and diabetes (Ozempic), is an agonist for glucagon-like peptide 1 (GLP-1), a hormone associated with appetite.
”It’s hard to think of other [drugs], apart from statins, that have shown such a profound effect,” says Martha Gulati, director of preventive cardiology at Cedars-Sinai Medical Center in Los Angeles, USA.
It was expected that semaglutide would have cardiovascular benefits through promoting weight loss, but evidence shows that drugs mimicking GLP-1 can improve fatty-acid metabolism and reduce inflammation, for example, says Gulati. “This is what’s so fascinating about these drugs. They work on the brain, the pancreas, the cardiovascular system, the gastrointestinal tract … There’s more to them than simply weight loss.”
Recent studies have been encouraging in terms of semaglutide’s benefits for reducing cardiovascular disease risk. Earlier this month, Novo Nordisk announced the headline results from the SELECT cardiovascular outcomes trial. The double-blinded trial compared subcutaneous once-weekly semaglutide 2.4mg with placebo as an adjunct to standard of care for prevention of MACEs over a period of up to five years. The trial enrolled 17 604 adults aged 45 years or older with overweight or obesity and established cardiovascular disease (CVD) with no prior history of diabetes.
The trial showed 20% reduction in MACEs for people treated with semaglutide 2.4mg compared to placebo. The primary endpoint was a composite outcome of the first occurrence of MACE cardiovascular death, non-fatal myocardial infarction or non-fatal stroke. All three of these components contributed to the MACE reduction. 1270 first MACEs were accrued.
Expanding GLP-1 analogues to cardiovascular disease prevention may not be without challenges, as the European Medicines Agency opened investigations into semaglutide and liraglutide over reports of suicidal thoughts and self-harm.
A separate study based on the STEP 1 trial data found that 93 million adults in the US could benefit from semaglutide, from a combination of weight loss and reduced cardiovascular benefits. They estimate a reduction in relative risk of 18% with the drug.
Dr Mark Blaylock, medical manager at Manguzi Hospital. PHOTO: Supplied.
By Sue Segar for Spotlight
There was a time, about 20 years ago, when, at the Manguzi district hospital in Northern KwaZulu-Natal, (and, of course, at hospitals throughout South Africa too) mothers and their babies were dying of AIDS at shockingly high rates.
“We used to get these patients who were slow progressors,” Mark Blaylock, medical manager at Manguzi, tells Spotlight. “Then there were the rapid progressors – babies who were HIV-positive who would get sick very quickly. There wasn’t much we could do for them. We’d give them vitamins and Bactrim, but ultimately they died. Then we had the ones who got sick a bit later, and those were even worse because now mum has had this baby for five years and they’ve bonded, and are a little family and now they are coming in with AIDS. Obviously, a huge number of mums died too. It was heartbreaking.
“It was the pregnancies that knocked their vulnerable immune systems. We’d watch it over and over again. The mums would come in looking ok and then they’d get pregnant and just go downhill. This was in the pre-ARV era. Pregnancy was a death sentence. I think people have forgotten what it was like in those days.”
Blaylock is talking to Spotlight from Northern KwaZulu-Natal, relaying how things have changed for the better since that terrible era. “It’s quite astounding,” he says. Blaylock returned to the hospital ten years ago after having been away for four.
“I was going through the stats recently, and in those days, 40 percent of all mothers who delivered were HIV positive, and about 40 percent of those babies born to HIV- positive mothers ended up with HIV either from birth or breastfeeding. About 20 percent would pick up HIV at birth and another 20 percent would pick it up subsequently through breastfeeding.
“These days, if we have one baby who is delivered HIV-positive or who picks up HIV, we get really upset. Our six-month HIV-positive rate now for babies is less than 0.6 percent and that is a dramatic change. It makes me so happy. Unfortunately, the young girls are still positive, but at least their babies are not becoming positive.”
Blaylock puts the changes down, “purely”, to prevention of mother-to-child transmission (PMCT) using antiretroviral therapy (ART). “Remember how, at one stage, we only gave HIV treatment if a patient was below a certain CD4 count? That was changed to test-and-treat, so regardless of their CD4 count, patients will get HIV treatment which brings the viral load down dramatically,” he says. “And now we have dolutegravir (an ARV), which is the backbone of our current HIV treatment. The success is due to prevention of mother-to-child transmission (PMTC) as well as the test-and-treat policy.”
‘A mixed bag’
It’s Sunday, a day off for Blaylock, and he’s speaking from a place with the best reception near his house on the edge of the Shengeza Lake. He lives here with his wife, Liz and their 13-year-old home-schooled daughter, Una. The sound of birds in the background makes it hard to hear him on the call. “It’s peaceful. There are hippos all around and lots of birds. It’s Eskom-free, which is even better. I love it. We live with three dogs, three cats, a genet, and I can’t tell you how many snakes. It’s paradise.”
It’s taken a long time to clinch this interview, but Blaylock has finally relented and forwarded us the provincial health department’s media protocol he has to adhere to. On problems in KwaZulu-Natal’s health system, he is reticent, saying only that it’s a “mixed bag”. “There’s a lot of dead wood, but there are real areas of excellence,” he says.
His reticence is understandable.
There was a time, also about 15 years ago, amidst the noise and turmoil of the last few years of state-backed AIDS denialism, when Blaylock was going through his own personal trauma. In April 2008, whilst working as chief medical officer at Manguzi, he was suspended for throwing an official photograph of then-Health MEC Peggy Nkonyeni into a dustbin in the hospital’s foyer. He did this out of anger and frustration, after his colleague at the hospital, Colin Pfaff was charged with misconduct for sourcing funding for antiretroviral drugs for pregnant women, and for implementing dual antiretroviral therapy to save babies from HIV – because politicians were not doing so.
He was also furious about comments made by Nkonyeni, questioning the integrity of rural doctors and suggesting they were racist. The South African National AIDS Council soon after asked the Human Rights Commission to probe the ‘racial tone’ of Nkonyeni’s remarks and to curb her ‘harassment’ of Manguzi doctors.
At the time, Blaylock (and Pfaff) were hailed by many working in the health sector as heroes with a deep commitment to their patients. In a letter to the provincial health department at the time, Blaylock said he had given his “heart and soul” to the under-resourced hospital, going beyond the call of duty.
Needing a change
Blaylock was reinstated but, in December 2008, he decided to leave, saying he needed a change and because the KwaZulu-Natal Department of Health was in “absolute disarray”. He says his old colleague Pfaff went to work as a missionary doctor in Malawi.
There was more to Blaylock’s decision to leave Manguzi than just the public disagreement with Nkonyeni. In our interview, he describes those days as “a really tough decade”. “Working in paediatrics, as I did for my first couple of years at Manguzi, I couldn’t take it anymore, emotionally. I just couldn’t do it, so I taught myself surgery. That was easier, as you could fix people. We were also so broken from losing so many friends, colleagues, and patients from HIV at the time. It was definitely traumatising and emotionally exhausting, not just for me but for Liz.
“There’s no doubt most of us were burnt out,” he says. “We kind of knew it, but we pushed on anyway. We were also quite a bit wilder and younger. We’d blow off steam by recklessly taking tiny boats across the lake, in the big waves, with lots of hippos – or we’d go for runs along the beach or naked midnight swims.”
The years outside SA
After leaving Manguzi, Blaylock moved to Ghana, where he took up a position as a general doctor at ABA Hospital in Tarkwa, north-east of Accra. “The hospital was part of the national health system but contracted to a mine, so we would treat people and then try and charge the government, fairly unsuccessfully, for the treatment,” he says. “I’d always fancied the idea of Ghana. I had this fantasy about Kwame Nkrumah and it being the first country to throw off Britain in Africa – but I didn’t enjoy it as much as I’d hoped. Everywhere you went, the police were pulling you over and asking for bribes.”
A defining moment was when Blaylock says he noticed the anti-malaria medication the hospital was giving patients was “just not working”. “Our malaria patients kept coming back full of parasites. I knew there were similar drugs in South Africa which were fantastic, so there was definitely something wrong.” He says he sent a sample to South Africa for testing and realised that “they weren’t as full of the good stuff as they were meant to be”. “I handed in the report and said ‘deal with it.”
From Ghana, where he married Liz and where his daughter Una was born, the family moved to the Kansanshi Mine Hospital in Zambia where they lived on a “beautiful golf estate, surrounded by poverty”.
“It didn’t feel right at all and was quite unfulfilling work,” he recalls. “I did GP work and there was lots of babbalaria – that’s when mostly the expat wives have a hangover on a Monday morning and they think they have malaria.”
Being “medically bored” in Zambia, Blaylock returned to Newcastle in KZN with the aim of specialising in anaesthetics. He worked in Madadeni Hospital’s anaesthetics department, before getting into a registrar’s programme on the anaesthetics circuit at various hospitals in Durban.
‘Like walking back home’
Then, in 2012, his friend and colleague Etienne Immelman, then working as medical manager of Manguzi, suggested that Blaylock should “come home”. “Etienne had been at Manguzi for more than 20 years when he retired six years ago. We’d always had a friendship and a mutual loyalty. He wanted someone to take over.”
Blaylock decided that indeed, it was time. It meant losing the opportunity to specialise, but he says it “felt right”. He went back as medical officer, before becoming manager.
“When I first arrived back, we were a small team, working hard. We all had the same commitment. It gave me a sense of purpose and belonging which hasn’t left.”
Blaylock said the hospital went through a “wonderful period” with a core team of great doctors. “But I burnt them all out during COVID – we had 164 deaths, but we pulled a lot of people through and many of the doctors have moved on. We have a young team now and they are getting there, but we don’t have the broad skill range we used to have. That is common across most district hospitals nowadays.”
So, is he happy to have come full circle, back to the place that was once a source of deep distress to him? “Yes,” he says. “For me, it’s about the community. This place gives me that, as well as a sense of stability and purpose. If you go into a little shop in Manguzi, everyone knows who you are. You say hallo to each other. You shout at a taxi driver and he says, ‘Hey Mark, don’t be so naughty’. When I came back ten years ago, it was like walking back home. It’s just a nice feeling.”
He says a lot has changed in the area. “People say there’s been no development, but when I first arrived at Manguzi in 2002, we knew every car on the road. Today, the town is overwhelmed with vehicles. There’s more money around. We almost never see malnutrition anymore. A lot of government programmes are working, as much as we like to diss them.”
Taking a stand
Given the toll that taking a stand has taken on doctors like Blaylock and Pfaff, one might be forgiven for wondering whether it was all worth it.
Did it make a difference to how things turned out? “Absolutely,” says Blaylock. “There were people scattered people around South Africa at the time who were doing great things. In our part of the world, it was Victor Friedland at Mseleni Hospital and Colin Pfaff (at Manguzi) who were the big drivers, pushing for the right actions to provide the services that the HIV Clinicians Society at the time thought was the correct one and was affordable. The Western Cape had already started, so we weren’t doing anything that groundbreaking except that it hadn’t been official policy yet,” he says.
“Can you believe that when HIV treatment first came to South Africa, it was going to be done at tertiary hospitals only? Imagine the repercussions for us sending a patient to Durban – in those days the Hluhluwe road was 160 kilometres of dirt road – to go and get their HIV treatment once a month. It was not sustainable.
“The HIV (Clinicians) Society pushed hard to get it decentralised to all hospitals. Then it was just going to be done by doctors and they said we absolutely cannot do it just with doctors. It has to be a nurse-run programme. Their vision became our current system. They weren’t the only people, but they were at the forefront of it at the time.”
‘Keeping it going’
Apart from the many advances in HIV treatment, much else has changed at Manguzi over the last 15 years. Blaylock says these days the hospital’s gastro wards are empty “thanks to the rotavirus vaccine”. “We’ve also seen a turnaround in acute respiratory tract infection,” he says. “The pneumococcal conjugate vaccine has changed that dramatically. We have also seen the pushing out of Continuous Positive Pressure Airway Ventilation (CPAP) for neonatal respiratory distressed newborns to district hospitals. This is a non-invasive way of ventilating babies with immature lungs,” he says.
“Our next great hope is the HPV vaccine, which will be a groundbreaker. It’s been rolled out in the past couple of years, but we’ll only see the effects in ten years or so because cervical cancer takes a few decades to come about. The other thing I really want to get in,” he insists, “is that our therapy department (offers occupational therapy, speech and hearing, and physiotherapy) at Manguzi is astonishingly fantastic. There are a lot of good things happening,” he says. “It is so easy to sit on the things that irritate you, but it is worth trying to remember the wins.”
As with several other rural doctors Spotlight has interviewed over the years, Blaylock seems deeply committed to building on what works at Manguzi and simply getting things done. As he says, “When you’ve invested so much into a hospital, you want to keep going as much as you can.”
A new study suggests that depression after traumatic brain injury (TBI) could be a clinically distinct disorder rather than traditional major depressive disorder. The findings, which are published in Science Translational Medicine, hold important implications for patient treatment.
“Our findings help explain how the physical trauma to specific brain circuits can lead to development of depression. If we’re right, it means that we should be treating depression after TBI like a distinct disease,” said corresponding author Shan Siddiqi, MD, from Brigham and Women’s Hospital,. “Many clinicians have suspected that this is a clinically distinct disorder with a unique pattern of symptoms and unique treatment response, including poor response to conventional antidepressants – but until now, we didn’t have clear physiological evidence to prove this.”
Siddiqi, who led the study, was motivated by a patient he shared with David Brody, MD, PhD, a co-author on the study and a neurologist at Uniformed Services University. The two started a small clinical trial that used personalised brain mapping to target brain stimulation as a treatment for TBI patients with depression. In the process, they noticed a specific pattern of abnormalities in these patients’ brain maps.
The current study included 273 adults with TBI, usually from sports injuries, military injuries, or car accidents. People in this group were compared to other groups who did not have a TBI or depression, people with depression without TBI, and people with posttraumatic stress disorder. Study participants went through a resting-state functional connectivity MRI, a brain scan that looks at how oxygen is moving in the brain. These scans gave information about oxygenation in up to 200 000 points in the brain at about 1000 different points in time, leading to about 200 million data points in each person. Based on this information, a machine learning algorithm was used to generate an individualised map of each person’s brain.
The location of the brain circuit involved in depression was the same among people with TBI as people without TBI, but the nature of the abnormalities was different. Connectivity in this circuit was decreased in depression without TBI and was increased in TBI-associated depression. This implies that TBI-associated depression may be a different disease process, leading the study authors to propose a new name: “TBI affective syndrome.”
“I’ve always suspected it isn’t the same as regular major depressive disorder or other mental health conditions that are not related to traumatic brain injury,” said Brody. “There’s still a lot we don’t understand, but we’re starting to make progress.”
With so much data, the researchers were not able to do detailed assessments of each patient beyond brain mapping. To overcome this limitation, investigators would like to assess participants’ behaviour in a more sophisticated way and potentially define different kinds of TBI-associated neuropsychiatric syndromes.
Siddiqi and Brody are also using this approach to develop personalized treatments. Originally, they set out to design a new treatment in which they used this brain mapping technology to target a specific brain region for people with TBI and depression, using transcranial magnetic stimulation (TMS). They enrolled 15 people in the pilot and saw success with the treatment. Since then, they have received funding to replicate the study in a multicentre military trial.
“We hope our discovery guides a precision medicine approach to managing depression and mild TBI, and perhaps even intervene in neuro-vulnerable trauma survivors before the onset of chronic symptoms,” said Rajendra Morey, MD, a professor of psychiatry at Duke University School of Medicine, and co-author on the study.