Spotlight’s Top 9 Health Stories to Watch in 2026

19th January 2026 | By Marcus Low
From the limited rollout of a new HIV prevention jab to developments with new weight loss medicines, to high-stakes court cases relating to National Health Insurance (NHI), 2026 is set to be another tumultuous year in healthcare. Here are nine stories that Spotlight will keep a close eye on.
1. How will things go with the local rollout of a new HIV prevention jab?
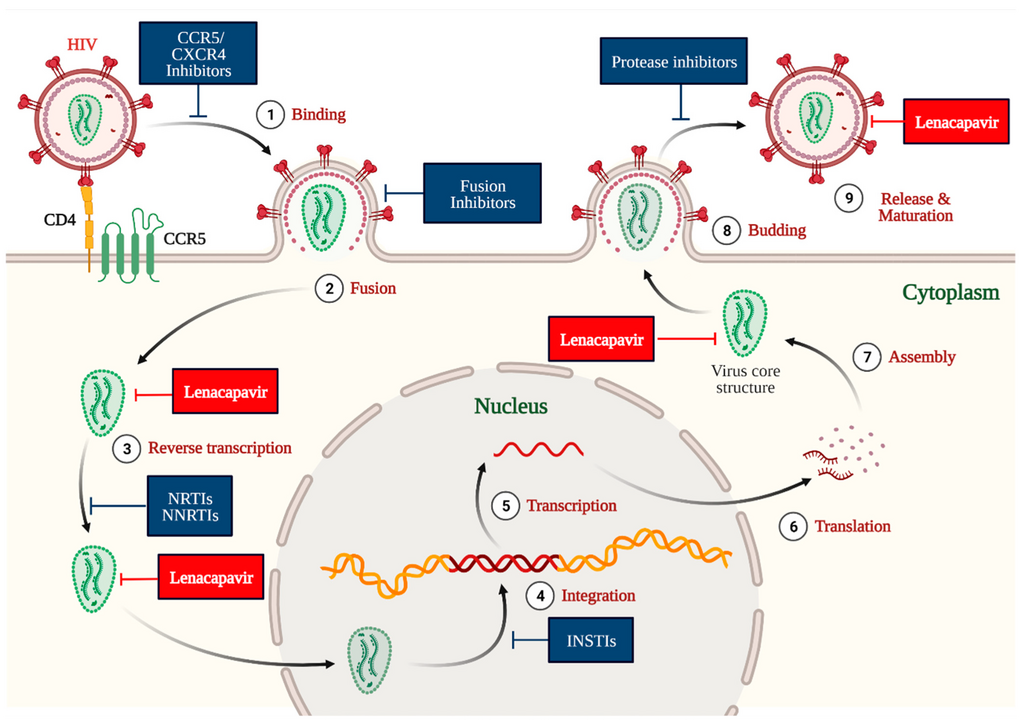
Given the high rates of HIV in South Africa, the biggest HIV story this year is likely to be the rollout of a new HIV prevention jab at around 360 (roughly 10%) of South Africa’s public sector clinics. The jab, which contains the antiretroviral medicine lenacapavir, provides six months of protection against HIV infection at a time. It could be a gamechanger for people who, for whatever reason, struggle to take daily prevention pills. We will be tracking how and to whom the jab is made available and whether uptake meets expectations.
As we reported last year, work is also underway on a new lenacapavir formulation that could provide 12 months of protection per shot. We’ll be scouring journals and conference programmes for new data on this formulation.
2. Will we see better access to weight loss medicines?
The class of diabetes and weight loss drugs called GLP1-RAs have taken the world by storm in recent years. Until recently, drugs like semaglutide (brand names Ozempic or Wegovy) and tirzepatide (brand names Zepbound or Mounjaro) were only available as injections. The GLP1-RA market is, however, set to be upended by the introduction of some of these medicines in pill form. The United States Food and Drug Administration (FDA) recently registered a semaglutide pill for use for weight loss. Another weight loss pill called orforglipron is also expected to be registered this year. One big question is when these pills will be registered and made available in South Africa and at what price.
Another important GLP1-RA development this year will be the expiration of a key patent on semaglutide in India. This will open the door to generic manufacturers bringing their own versions of semaglutide to market – something that usually leads to substantial price reductions. We will be keeping a close eye on how this situation plays out and analysing what the implications are for people in South Africa.
3. Might we see earlier than expected findings from pivotal TB vaccine trials?
The one TB vaccine we have is over a hundred years old and only provides limited protection for kids. Several experimental vaccines are, however, currently being evaluated in late-stage clinical trials. Arguably, the most notable of these is the M72 vaccine, which is being assessed in a massive phase 3 study, partly conducted in South Africa.
While timelines suggest most of the key TB vaccine studies will not yet have anything to report this year, it is possible that we might see a surprise or two. Findings are sometimes reported early if it becomes apparent ahead of schedule that a medicine or vaccine is clearly working, or clearly not working, as the case may be. Whether or not we see findings this year, it is important to start thinking about what a rollout might look like in our health system should results be as good as hoped. The M72 vaccine had around 50% efficacy in phase 2 trials, so there is reason for optimism.
4. Will we see a concrete plan to address public sector healthcare worker shortages?
Arguably, the most important dynamic in South Africa’s public healthcare system today is that provincial health departments are not employing enough healthcare workers across multiple categories. One reason for this is simply that budgets have generally shrunk over the last decade – obviously corruption and mismanagement in several provincial departments have made things even worse. There was a glimmer of hope in last year’s budget in which we saw a meaningful upturn in health funding for the first time in years, but that was at best a good first step toward recovery. As we enter 2026, our understanding is that all of the nine provinces are still facing severe healthcare worker shortages.
More money for health in the next budget will certainly help, but there is a broader sense that government doesn’t really have a big picture vision for how to address the crisis. We do have a 2030 Human Resources for Health Strategy, but as with many such strategies, it seems to have so far gone largely unimplemented.
5. Will enablers be held accountable for corruption such as that at Thembisa Hospital?
One of last year’s big media moments was a Special Investigating Unit (SIU) press conference in which they described the extensive corruption said to have taken place at Thembisa Hospital. One snag, however, is that while the SIU can recoup funds and take matters to the Special Tribunal, the SIU does not conduct criminal prosecutions – though they can refer matters to the National Prosecuting Authority (NPA) for prosecution. Whether we will see successful NPA prosecutions relating to the Thembisa Hospital corruption is one of the year’s top questions.
Unfortunately, even when the SIU does sterling work and delivers cases to the NPA on a plate, there is no guarantee that the NPA will do its job. One depressing example is that of Buthelezi EMS. Last year, the Special Tribunal ordered Buthelezi EMS (and other companies with similar names) to pay over half-a-billion Rand back to the state. The SIU also referred a related matter to the NPA in 2024 for prosecution, but Spotlight understands that the NPA has rather mind-bogglingly decided to drop the matter.
6. Which, if any, senior health leaders will lose their jobs this year?
While we won’t have national or provincial elections this year, that is no guarantee that we won’t see any health leaders losing their jobs. Over the last two decades, there have after all been many examples of people being ousted between elections, be it for purely political reasons or due to corruption scandals.
Possibly the political leader in the health sector at greatest risk is KwaZulu-Natal MEC for Health, Nomagugu Simelane. Should the currently governing coalition of political parties in the province crumble, as it seems it might do, chances are several new MECs will be deployed, including for the health portfolio.
There is also an outside chance that the country’s top health official, Dr Sandile Buthelezi, Director-General for Health in the National Department of Health, might be forced to step down. As reported by AmaBhungane, Buthelezi played a central role in an “irregular” R836-million oxygen procurement process and is also “at the centre of a Hawks investigation into allegations that he solicited a R500 000 bribe”. Our understanding is that Buthelezi has not been charged and that in the absence of charges he will stay in the job.
7. What will happen in the landmark NHI court cases?
Despite a new call for dialogue from Finance Minister Enoch Godongwana, chances for a political settlement over National Health Insurance (NHI) remains very low. The bottom line remains that Health Minister Dr Aaron Motsoaledi refuses to yield an inch on the version of NHI described in the Act and President Cyril Ramaphosa is not willing to force the matter.
Instead, it seems the battle over NHI will this year be fought mainly in the courts. At our count, there are at least eight cases challenging the NHI Act, parts of the Act, or the process resulting in the Act. A first development to look out for is whether or not some of the cases will be combined and heard together. In case you missed it, last year we published a two-part series in which we tried to pin down the issues on which these court cases are likely to turn (see part 1 and part 2).
While we will cover the NHI court cases in some depth, we will also try to foster constructive discussions on health reforms on our opinion pages and in our analysis. In our view, it is dangerously limiting to reduce the debate over South Africa’s healthcare reforms to a simple binary of whether one is for or against NHI.
8. What will be left of the FDA, NIH, and CDC by the end of 2026?
It used to be the case that United States Food and Drug Administration (FDA) decisions and health advice from the United States Centres for Disease Control and Prevention (CDC) carried a lot of weight around the world. In recent months, however, there have been increasing signs of political interference at these institutions and a turn away from evidence-based policy making. It seems inevitable that we will see more of the same in 2026 and the credibility of both the CDC and probably also the FDA will be further diminished.
Similarly, the US National Institutes for Health (NIH) has been the world’s leading funder of health research for many years. But as with the CDC, the work of the NIH has been overly politicised over the last year and its reputation for rigour and scientific excellence has already been severely degraded. As with the FDA and CDC, the outlook is bleak.
9. How well will SA and other countries recover from last year’s US aid cuts?
With the dust settling after last year’s severe and abrupt cuts to US healthcare aid and US funding for medical research, the longer-term impacts of those cuts in South Africa and neighbouring countries should become clearer this year. Among others, we will get the first reliable estimates of key HIV and TB indicators for 2025 (reliable figures for a specific year are typically only published in the subsequent year). New HIV estimates from the Thembisa mathematical model (Spotlight’s preferred source for HIV estimates) should be out around the middle of the year, while new World Health Organization (WHO) TB estimates are usually released in November.
Last year Motsoaledi was widely criticised by activists for underplaying the seriousness of the cuts for South Africa’s HIV response and the scale of specialised services and capacity that was destroyed here. Eventually some extra funds were made available in response to the cuts, but it amounted to only a small fraction of what was lost. The harsh reality is that in some places the aftermath of the aid cuts will be felt for years to come.
At an international level, we are also not convinced that a clear roadmap has been set out for building back better after US withdrawal, though we’d be happy to be proven wrong. What is clear though is that entities like the WHO and UNAIDS are facing unprecedented financial and political pressures – it seems possible that UNAIDS will no longer exist a year from now. Much reform has already been undertaken at the WHO. By the end of the year, we should have some sense of whether things have stabilised and whether a coalition of willing nations is truly committed to keeping the WHO and multilateralism in health alive.
We have outlined only nine health issues in the above, but there are of course many more questions that we could have added to this list. Some of those include:
- Whether we will see meaningful improvement in the South African government’s response to non-communicable diseases such as diabetes, cancers, and mental health conditions.
- How well implementation of South Africa’s latest TB recovery plan is going, and in particular how we are doing against the target of testing five million people in 12 months.
- How climate change will impact people’s health and whether the South African government is prepared for it.
- Whether South Africa will see real progress in addressing antimicrobial resistance. After adopting a good policy a few years ago, it appears momentum has been lost.
- Whether the state will start taking xenophobia in the healthcare system and around clinics and hospitals more seriously, as a recent court judgment requires it to do.
- Whether a serious effort will be made to better regulate private healthcare and to bring down the cost of private healthcare services and medical scheme membership – that after a half-baked effort to create a new tariff-determination framework was launched and then canned last year.
- Whether we will see legislation introduced amending the Patents Act in line with a policy adopted by government in 2018 and whether we’ll see progress on the much-delayed State Liability Bill, which should have relevance for the state’s vulnerability to medico-legal claims.
- Whether we will see concrete steps forward with the new electronic health records and data systems government is developing.
- What progress we might see with the local production of vaccines and pharmaceuticals – one of the areas in which we are quite optimistic, despite the lack of coherent and enabling government policy.
- What impact AI will, or will not, have in our healthcare system this year.
Are there issues not mentioned here that you think Spotlight should cover in 2026? Let us know by commenting below this article or by tagging us on BlueSky.
*Low is the editor of Spotlight.
Republished from Spotlight under a Creative Commons licence.
Read the original article.