A new study published in JAMA Network Open found that removing olfactory groove meningioma, a type of brain tumour located near the base of the brain, may improve blood sugar control in patients with diabetes.
Researchers followed patients with an olfactory groove meningioma and diabetes over five years after surgery, tracking long-term changes in haemoglobin A1c (HbA1c), which is a standard measure of blood sugar control, and body weight after tumour removal surgery.
The research team found:
Blood sugar control improved after tumour removal in most patients.
Improvements often happened soon after surgery and lasted for years.
Many patients also lost weight after surgery.
Improvements occurred even when diabetes medications stayed the same.
“This type of brain tumour affects both frontal lobes simultaneously and is usually thought of as causing symptoms like vision problems, personality changes or loss of smell,” said Andrew Venteicher, MD, PhD, an associate professor at the University of Minnesota Medical School and neurosurgeon with M Health Fairview. “What surprised us was how much blood sugar control improved after surgery in many of these patients. The findings may help us better counsel patients before surgery and raise new questions about how the brain influences metabolism throughout the body.”
The findings suggest that some brain tumours may affect the body’s ability to regulate metabolism and blood sugar, and that removing certain brain tumours may improve blood sugar control and weight in some patients with diabetes, in addition to improving neurological symptoms.
Future studies will explore why these metabolic improvements occur and whether similar effects are seen in patients with other types of brain tumours. Researchers also hope to better understand how brain function, behaviour and metabolism are connected and whether these findings could help guide future treatment decisions.
Nine leading AI models were tested on simple administrative queries drawn from real-world emergency department records—and most failed unless paired with code-generation tools.
A new study finds that large language models (LLMs), used with straightforward prompting, perform poorly on routine number-crunching tasks that hospital administrators depend on every day to track patients and allocate resources. The findings were published this week in the open-access journal PLOS Digital Health by Eyal Klang of the Icahn School of Medicine at Mount Sinai, New York, USA, and colleagues.
Hospitals rely on structured electronic health record (EHR) data to monitor patient counts and resources and to generate administrative reports. These tasks are currently handled by data analysts using programming languages, creating delays when staff need fast answers. AI tools known as large language models, such as GPT-4o and Llama, have been proposed to simplify that process.
In the new study, researchers evaluated nine leading LLMs on two basic administrative tasks—counting patients meeting a condition and filtering records based on multiple criteria—using data drawn from 50 000 real emergency department visits at the Mount Sinai Health System.
The researchers found that straightforward prompting—asking the model a plain question like “how many patients in this table were admitted?”—produced uniformly poor results across all models. Chain-of-thought reasoning, in which the model is prompted to show step-by-step work before giving an answer, offered only modest improvements that degraded sharply as table size increased. Even GPT-4o, the top-performing model, saw accuracy drop from roughly 95% on the smallest datasets to below 60% on larger ones under chain-of-thought conditions.
A tool-based approach—where models were asked to generate code that was then executed—substantially improved accuracy for the most capable models, with GPT-4o and Qwen-2.5-72B achieving near-perfect performance. However, distilled DeepSeek models, optimised for speed and efficiency, struggled even with this approach. One model, Llama-3.1-8B, failed to produce usable output in the majority of trials and was excluded from further analysis.
“Our findings indicate that without using a tool-based strategy, current LLMs are unsuitable for standalone use even on minimally complex administrative tasks in clinical settings,” says Benjamin Glicksberg. “Structured data tasks in clinical workflows will require agentic approaches that combine LLMs with code execution to ensure accuracy and consistency.”
The largest and most comprehensive study of memory and cognition in new parents has found no evidence for ‘baby brain’ in parents
Photography by Drew Hays on Unsplash
New mothers often complain about having ‘baby brain’, where memory and cognition become vague and unreliable. Now a Monash University study – the largest ever done comparing cognitive ability in new parents – has unequivocally found no evidence that ‘baby brain’ reflects underlying problems with cognition that result from becoming a parent.
The study found that – using a comprehensive battery of cognitive assessments – both mothers and fathers showed similar performance to non-parent (male and female) controls on all cognition measures, “suggesting the absence of so-called ‘baby brain’ effects,” Dr Perrykkad said.
As an explanation of the common stereotype of ‘baby brain’, the researchers found a gender bias, with male non-fathers self-reporting better subjective memory than all other groups. However, according to Mr Siddiqui, “this self-promotion bias appeared to be lost in fathers, driven by lack of sleep”.
Strikingly, there was no effect of time postpartum on any cognitive measure, with parents’ ability on cognitive tests remaining the same regardless of the baby’s age up to 2 years, when it is assumed that sleep deprivation would be reduced.
While there is evidence of subtle decrements in cognition during pregnancy, according to Dr Perrykkad, “the evidence is inconsistent about the presence of an objective measurable decline in cognitive function during the postpartum period with studies revealing a potential mismatch between the self-reported parental experience and objective measures of cognitive change,” she said.
Mr Siddiqui said that – before the study – they expected that mothers and fathers would show subjective and objective reduction in cognition compared to non-parents. “We expected that there would be little to no difference between the new mums and dads on account of their shared environment post birth and we also expected that cognition would improve in parents with increased time postpartum,” he said.
Dr Perrykkad continued, ‘So why do new parents, especially new mothers, commonly report experiences of baby brain? It is important not to dismiss what new parents are telling us. When we do find evidence for baby brain, it is more related to sleep and wellbeing than a true objective decline in cognition. This indicates it is just as important as ever to support new parents in these formative years. While it isn’t the end of the baby brain story, new parents can take solace in the fact that becoming a new parent doesn’t inherently impair their memory and cognition.”
A 3-month-old African turquoise killifish, left, and a 5-month-old killifish, right, show aging much like that in humans.
Researchers have identified a gene that directly links early-life growth and reproductive success with accelerated ageing and increased cancer risk later in life, offering new insight into a longstanding theory in evolutionary biology.
Now, an international team of researchers provides experimental evidence for the theory of antagonistic pleiotropy, the idea that certain genes can provide advantages early in life while contributing to disease and decline in old age.
What’s fascinating – and slightly terrifying – is that the cancer we see in these fish isn’t a random accident. It’s the direct shadow of their youthful vitality
Prof Itamar Harel
While widely accepted in theory, scientists have struggled to identify specific genes responsible for such trade-offs in vertebrates. Using the African turquoise killifish, a short-lived species recently pioneered by Harel and colleagues for genetic ageing research, the team focused on the gene vgll3, which has been previously linked to the timing of human puberty and maturation in other species, particularly Atlantic salmon.
By modifying this gene using CRISPR technology, the researchers observed clear effects. Fish with altered vgll3 grew faster and reached sexual maturity earlier, traits that could offer a reproductive advantage in natural environments.
However, these benefits came with significant long-term costs. The same fish showed reduced lifespans and a higher incidence of age-related tumours, including melanoma-like cancers.
“We have effectively caught evolution in the act of making a trade-off. For years, we’ve asked why our bodies can’t just maintain themselves indefinitely. This gene gives us a direct answer: nature doesn’t prioritise longevity; it prioritises continuity. We are built to sprint, not to marathon,” said Prof Itamar Harel at Hebrew University.
Further analysis showed that the gene influences key biological processes, including cell division, stem cell activity, and DNA repair. Increased cellular activity may help explain both the rapid development observed in younger fish and the accumulation of damage that leads to disease in older individuals.
The researchers also developed a new immunodeficient killifish model, enabling them to transplant and study tumour cells in ways not previously possible in this system.
“What’s fascinating – and slightly terrifying – is that the cancer we see in these fish isn’t a random accident. It’s the direct shadow of their youthful vitality. The same machinery that drives a cell to build a young body is hijacking the system to build a tumour in the old one. If we can understand this mechanism, we might finally learn how to decouple healthy growth from the disease of ageing,” Dr Harel added.
Because vgll3 is conserved in humans, the findings may have broader implications for understanding human development, ageing, and age-related diseases. While previous association studies have linked the gene to puberty timing and hormone levels, functional data were missing until now.
The discovery could contribute to future efforts in cancer prevention and research aimed at extending healthy lifespan. Researchers say the next step will be to explore whether it is possible to separate the gene’s beneficial early-life effects from its harmful consequences later in life.
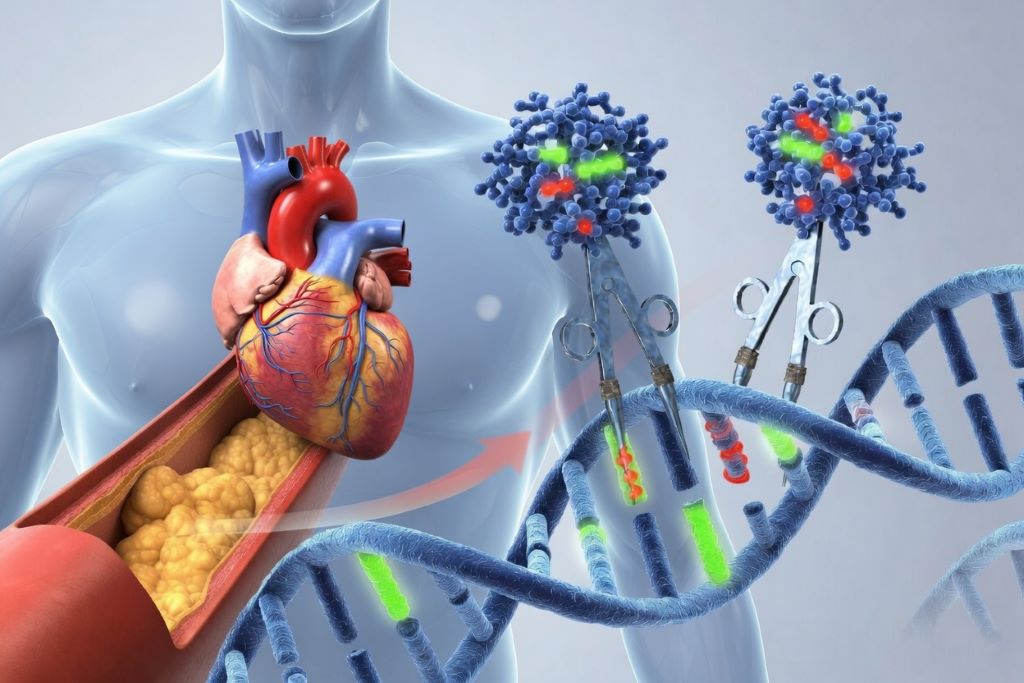
Australian hospitals will lead a first-in-human clinical trial of a new investigational genetic therapy that aims to lower cholesterol in people at increased risk of cardiovascular disease. The Victorian Heart Hospital, operated by Monash Health in partnership with Monash University, will be the first clinical trial site globally to begin testing the investigational therapy STX-1150, developed by Scribe Therapeutics.
The therapy is designed to reduce LDL (‘bad’) cholesterol by targeting a gene in the liver called PCSK9, a well-established regulator of cholesterol levels and cardiovascular risk. Elevated LDL cholesterol is a major cause of atherosclerotic cardiovascular disease, including heart attacks and strokes.
STX-1150 uses a next-generation CRISPR-based approach known as epigenetic silencing. Delivered as a one-time infusion, the therapy is designed to reduce cholesterol levels for an extended period without permanently altering a person’s DNA.
Principal Investigator of the study Professor Stephen Nicholls, Director of the Victorian Heart Hospital and Victorian Heart Institute, and Professor of Cardiology at Monash University, said the trial represented another major step forward in developing more durable approaches to cardiovascular prevention.
‘The best way to treat heart disease, the leading cause of death globally, is to prevent it,’ Professor Nicholls said.
‘While existing cholesterol-lowering therapies are highly effective, many people still struggle to maintain long-term treatment due to cost, access, side effects, or the burden of ongoing medication.’
‘This new investigational therapy is designed to provide sustained cholesterol reduction following a single treatment, which could significantly change how we manage cardiovascular risk in the future. This represents the new frontier of cardiovascular medicine.’
‘It is incredibly exciting that Victorians and Australians will again play a leading role in the development of next-generation genetic therapies for heart disease.’
The Phase 1 study will assess the safety, tolerability and biological effects of STX-1150 in adults with elevated LDL cholesterol who are at increased cardiovascular risk.
The trial plans to enrol up to 64 participants across sites in Australia and New Zealand, with participants monitored for one year following treatment.
The study follows regulatory clearance from Australia’s Therapeutic Goods Administration and builds on growing international interest in genetic approaches to cardiovascular disease prevention.
About the study
The Phase 1 trial will evaluate STX-1150 in adults with elevated LDL cholesterol and increased cardiovascular risk.
The study is designed as an open-label, single ascending dose trial followed by a dose expansion phase.
Up to 64 participants are planned to be enrolled across Australia and New Zealand.
The Victorian Heart Hospital will serve as the initial clinical trial site.
Participants will be followed for one year after treatment.
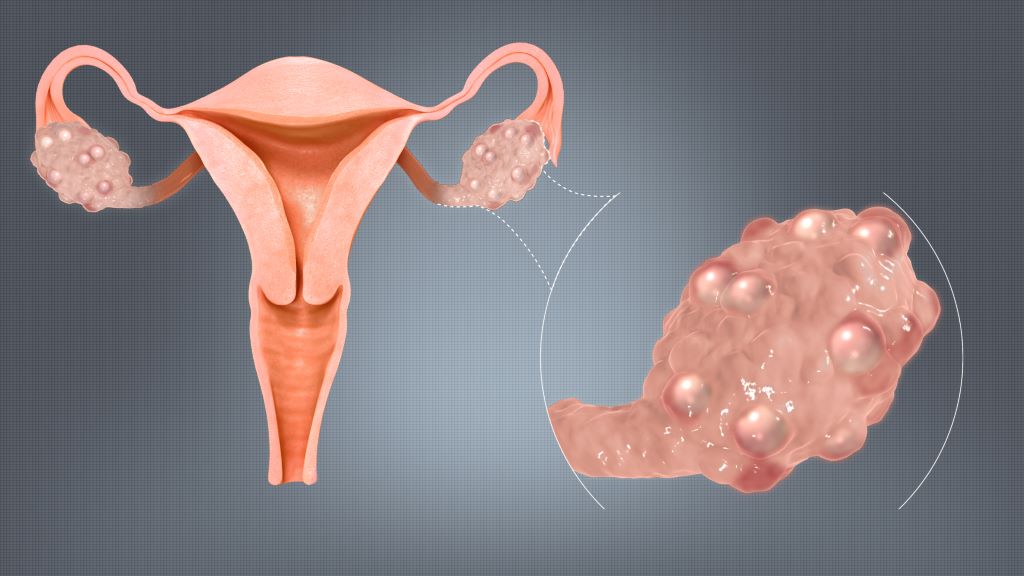
Polycystic ovaries. Credit: Scientific Animations Wiki CC4.0
For decades, women diagnosed with Polycystic Ovary Syndrome (PCOS) have often been told that the condition centres on cysts forming on the ovaries. In reality, many women who meet the diagnostic criteria never develop ovarian cysts at all, which means that the name has long created confusion for both patients and clinicians alike.
In May 2026, global health experts formally introduced Polyendocrine Metabolic Ovarian Syndrome (PMOS) as the updated terminology for this condition, which reflects the growing scientific consensus that it involves multiple hormonal and metabolic systems, not only the ovaries.
The change follows more than a decade of international consultation among endocrinologists, researchers and patient groups. The goal is to align the name of the condition with what research has increasingly shown about how it works in the body.
“Up to 70% of PCOS cases remain undiagnosed due to gaps in awareness, recognition and care, leaving many women navigating years of unexplained symptoms,” says Dr Themba Hadebe, Clinical Executive at Bonitas Medical Fund. “The new terminology recognises that this is a complex endocrine and metabolic disorder that affects several systems in the body.”
A name change to pay attention to
For years, the label Polycystic Ovary Syndrome suggested that ovarian cysts were the defining feature of the condition. Yet the small follicles seen on ultrasound scans are not true cysts, and they are not present in every patient.
Doctors diagnose the condition using a combination of symptom monitoring that may include irregular ovulation, elevated androgen levels and characteristic ovarian changes on ultrasound. This broader clinical picture often sits uneasily with the name itself.
“The terminology shaped how people understood the condition,” says Hadebe. “When patients heard ‘polycystic ovaries’, many assumed the problem was limited to reproductive health. In practice, the condition affects hormones, metabolism and long-term health risk.”
Women living with the syndrome frequently experience a wider set of health concerns. Hormonal imbalances can lead to acne, excess facial or body hair and irregular ovulation. The condition can also influence mood and mental wellbeing.
“Patients often arrive in consulting rooms with a range of symptoms that appear unrelated,” says Hadebe. “When you step back and view the condition as a broader endocrine disorder, those symptoms begin to make sense.”
One of the strongest drivers of the renaming is the role of metabolism in the condition. Research shows that many women living with the syndrome experience insulin resistance, where the body’s cells respond poorly to insulin and struggle to regulate blood sugar effectively. This metabolic disruption can contribute to weight gain and increase the risk of developing Type 2 Diabetes and cardiovascular disease later in life.
The importance of early diagnosis
Despite how common the condition is, many women spend years searching for answers before receiving a diagnosis, with updated NICE guidelines for PMOS aimed at standardising diagnostic pathways expected to be released towards the end of 2026. Symptoms such as irregular periods, persistent acne, excess hair growth or unexplained weight gain are often dismissed as routine hormonal fluctuations.
Delayed diagnosis can carry long-term consequences. Without proper management, metabolic complications may develop gradually over time. “Early detection allows clinicians to manage the condition more effectively and reduce future health risks,” says Hadebe. “Women who notice persistent hormonal or menstrual changes should seek medical advice so that underlying causes can be assessed.”
Addressing stigma and misunderstanding
The name change also addresses the emotional impact many women describe when navigating the condition. Patients frequently report that their symptoms were minimised or attributed to stress, weight or lifestyle factors before they received an explanation.
Language plays a powerful role in shaping how conditions are understood. A name that reflects the complexity of the syndrome helps validate the experiences of those living with it.
“Renaming the condition does not change the biology,” says Hadebe. “However, updating the name to better reflect current scientific understanding will improve awareness, support earlier diagnosis, enhance quality of care, drive greater consistency in research, and ultimately improve the overall patient experience.”
As awareness grows, experts hope the shift to Polyendocrine Metabolic Ovarian Syndrome, or PMOS, will encourage earlier recognition of symptoms and more holistic care for women affected by the condition.
Meningitis is rare in newborns but often life-threatening and can cause serious and lasting damage, including developmental problems. Now, researchers from ETH Zurich and the University of Basel have developed an approach that seeks to prevent transmission to newborns. The research is published in Nature Communications.
Although meningitis is thankfully rare in newborns as a whole, it is more common in premature babies, affecting one in every 500 such infants in industrialised economies and likely more in developing countries. One of the leading pathogens responsible for these meningitis cases is the K1 form of the E. coli bacterium. In the adult intestine: in one in three healthy adults, E. coli K1 is part of the intestinal flora. As a silent cohabitant, the bacterium causes no problems in this environment. It is kept in check by other bacteria and a functioning immune system.
However, if the pathogen is carried by an expectant mother, it can be transmitted to the child during birth and enter its intestine. In premature babies whose immune systems are still weak, the pathogen can enter the bloodstream and migrate to the brain, where it causes severe inflammation.
First weaken the pathogen, then fight it
Researchers led by Emma Slack, Professor of Mucosal Immunology at ETH Zurich, and Médéric Diard, Professor of Infection Biology at the Biozentrum of the University of Basel, want to stop transmission from happening in the first place. Their idea is to eliminate the pathogen in pregnant women who carry it in their intestine – but that’s easier said than done.
A year ago, the two researchers from Zurich and Basel had already jointly developed a concept for eradicating other pathogens living in the intestine (as ETH News reported). Back then, they used a combination therapy with two components: an oral vaccination that weakens the pathogenic bacterium, followed by a dose of harmless microbes that compete with the weakened pathogen for food, starve it out, and ultimately supersede it. In experiments on mice, the researchers demonstrated that this approach can eliminate certain salmonellas and E. coli strains in the intestine.
So tough that three components are needed
However, the K1 form of E. coli is a formidable opponent: unlike other E. coli bacteria, it is protected by a slippery outer layer. This prevents the antibodies generated by the oral vaccination from attacking the bacterium.
The team of researchers led by Slack and Diard therefore extended its previous two-pronged approach with a third component known as bacteriophages (or simply phages). These are viruses that specifically infect and kill bacteria.
However, the bacteria can make changes to themselves in order to evade the danger posed by these viruses. The phages attack the bacteria by docking to the protective layer, and the bacteria seek to prevent this by undergoing a sort of rapid evolution in which this layer is disposed of. Rapid in this case means that, since the bacteria are so numerous and multiply so quickly, they need fewer than 24 hours to adapt.
“This is essentially a resistance mechanism that the bacteria deploy against the phages,” says Slack. “We use this mechanism to our advantage: the antibodies formed by the oral vaccination are effective against K1 bacteria that no longer have their protective coating.”
Most young animals protected
The project involved searching for effective strains of phages. Scientists generally find phages in places that are home to lots of bacteria: nutrient-rich bodies of water, the intestinal flora or, very often, waste water and waste water treatment plants. When it comes to the phages used in this study, the researchers from the Biozentrum in Basel found what they were looking for in waste water samples from the treatment plant of the Lucerne conurbation. From such a sample, their lab work successfully isolated several phages that are particularly effective at attacking the bacterium E. coli K1.
In experiments with pregnant mice, which the researchers had previously infected with pathogenic E. coli K1, they were able to demonstrate the effectiveness of their triple-pronged treatment. The researchers first gave the mice phages that forced the bacteria to cast off their protective shell. Second, they administered an oral vaccination that produced antibodies in the intestine in order to weaken the bacteria. Third, they gave them a harmless probiotic bacterium that could compete against the weakened bacteria and occupy their ecological niche in the intestine.
In a control experiment in which the researchers did not treat the mothers, E. coli K1 was transmitted to 83% of young animals at birth. By contrast, the triple-pronged treatment significantly reduced the level of E. coli K1 in the mothers’ intestines, such that the pathogen was only transmitted to 23% of the young animals. The remaining offspring were protected.
Works even when antibiotics fail
The researchers are now keen to continue with their approach in order to develop a treatment for humans. In a world in which effective antibiotics are becoming increasingly scarce, we need new therapeutic approaches, says Slack. “Bacteria such as E. coli K1 are difficult to tackle. Our approach is potentially the only one that can be used to fight this pathogen and others without antibiotics.”
Not only can E. coli K1 cause cases of meningitis in newborns, which today must be treated with antibiotics in a race against time. It is also one of the most frequent causes of cystitis and pyelitis – infections that can also lead to serious cases of sepsis.
The ETH professor doesn’t perceive any major obstacles to developing an effective treatment for humans: “Oral vaccinations, probiotics and even phages are all already used in medicine,” she says. It will also be possible, she adds, to pack all three components into a single capsule that people can simply swallow.
Moreover, the scientists are planning projects in which they want to use the same approach to tackle bacteria other than E. coli K1, including multi-resistant pathogens, against which many antibiotics are no longer effective.
Hepatitis C virus. The hepatitis B virus has significant differences compared to the C virus, including differences in the protein envelope and DNA versus hep C’s RNA genome. Credit: Scientific Animations CC4.0
In an editorial published in the New England Journal of Medicine, University of Michigan Health hepatologist Anna S. Lok, MD, hails newly announced results of the B-Well clinical trials as “a major step toward a functional cure for hepatitis B virus infection.”
The results, published concurrently in NEJM, report that 20% and 19% of patients in two duplicate clinical trials achieved a functional cure for their chronic hepatitis B infections following 24 weeks of bepirovirsen (versus 0% of the placebo groups).
The lead and corresponding author of the trial results is Jinlin Hou, M.D., Chairman and Professor of the Hepatology Unit and Department of Infectious Diseases, Southern Medical University in Guangzhou, China.
The University of Michigan Health did not participate in these clinical trials.
The most common treatment for chronic hepatitis B infection, nucleoside or nucleotide analogue (NA) therapy, can successfully suppress hepatitis B virus replication – reducing the risk of cirrhosis and cancer – but is rarely curative, and most patients will relapse if treatment is discontinued before hepatitis B surface antigen loss.
In 2016, Lok led the first meeting among the US Food and Drug Administration, European Medicine Agency, American Association for the Study of Liver Diseases, European Association for the Study of the Liver, and experts in academia and industry to discuss definition and paths towards a cure for hepatitis B.
This group of experts recommended that functional cure of hepatitis B should be defined as undetectable hepatitis B surface antigen and hepatitis B virus DNA at least 24 weeks after completing a finite course of treatment. During the past 10 years, many clinical trials testing different combinations of antiviral and immunomodulatory agents have been evaluated but only one phase 3 trial has been completed so far.
In these latest phase 3 clinical trials, 24% of the patients taking bepirovirsen were able to discontinue NA therapy, compared to zero patients in the placebo groups, and none of the patients who discontinued NA therapy including a few who failed to achieve functional cure had clinical relapse.
Although these trials were conducted in highly selected patients and the results may not be generalizable to other patients with chronic hepatitis B — and side effects were more common among the patients who received bepirovirsen — they are encouraging and represent a major step towards a cure for hepatitis B. Lok hopes the results of these trials will encourage testing of other combinations that are safe and can lead to higher rates of functional cure in broader patient populations.
A renowned researcher into the natural history and treatment of hepatitis B, Lok co-authored every edition of the American Association for the Study of the Liver Diseases Guidelines on hepatitis B since 2001 and the first World Health Organization guideline on the condition in 2015.
Earlier this month, she was the senior author on a review of the current state of global hepatitis B virus prevention and treatment, published in JAMA.
The study, published in Jama Open Network, found naloxone administration during resuscitation by emergency medical service (EMS) personnel was associated with improved outcomes in patients with suspected OA-OHCA.
“This study provides important real-world evidence that naloxone may offer benefit even after cardiac arrest has occurred.”
David Dillon, study author
What the data shows
For this retrospective cohort study (looking back at existing patient records), researchers collected data from the California Resuscitation Outcomes Consortium between 2021 and 2022. In total, 3811 patients with suspected OHCA were treated by EMS.
Researchers found that people who received naloxone, a medication better known for reversing opioid overdoses, had higher rates of survival from the time they were treated by EMS to the time they were discharged from the hospital. The patients also benefitted from return of spontaneous circulation (ROSC) and favourable neurological outcomes compared to those who did not receive the drug.
The key findings included:
Survival to hospital discharge was higher among those receiving naloxone (8.1%) compared to those who did not (4.4%).
Naloxone use was associated with a 2.8% absolute increase in survival, after accounting for patient and clinical factors.
People treated with naloxone had improved neurologic outcomes (+3.2%) and ROSC (+3.3%).
Benefits were even greater among those with EMS-suspected drug-related cardiac arrest, with survival improvements approaching 8–9%.
The study also found that the association between naloxone and improved outcomes was weakened in certain situations – particularly among patients who required epinephrine during resuscitation. This suggests that timing, patient condition or resuscitation complexity may influence effectiveness.
Addressing a critical gap
Opioid overdose deaths in the United States have surged over the past two decades, contributing to a growing number of cardiac arrests outside the hospital. While naloxone is widely used to reverse opioid overdoses, its role during cardiac arrest has remained unclear and is identified by the American Heart Association as a key evidence gap.
“This study provides important real-world evidence that naloxone may offer benefit even after cardiac arrest has occurred,” said David Dillon, assistant professor of emergency medicine at UC Davis Health and one of the study’s authors. “While these findings are promising, randomised controlled trials are needed to determine whether naloxone directly improves survival in opioid-associated cardiac arrest.”
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
The combination of a vaccine and a drug, which both harness the immune system to attack cancer cells, has proven successful in cutting the risk of skin cancer recurrence by 49% , a new study shows. This reduction, which was calculated five years after patients had their tumours surgically removed, remains unchanged.
Led by researchers at NYU Langone Health and its Perlmutter Cancer Center, the study tested the vaccine, called intismeran, in combination with the mainstay immunotherapy pembrolizumab (Keytruda) in 107 patients who had been randomly chosen after melanoma surgery to determine whether the combination therapy prevented their cancer from recurring. Intismeran is a personalized immunotherapy strategy that is developed with information from a patient’s individual tumour. These results were compared with those from a randomly selected group of 50 melanoma patients who had only received pembrolizumab postoperatively, a current standard of care.
Results of the phase 2b trial, known formally as KEYNOTE-942, are being presented at the 2026 annual meeting of the American Society of Clinical Oncology on June 1 in Chicago and simultaneously published in the society’s Journal of Clinical Oncology.
After five years of follow-up, 68.8% of patients who took the combination therapy remained cancer-free, while 49.1% of the patients in the pembrolizumab-alone group had no signs of cancer. This means that adding intismeran to pembrolizumab reduced the risk for recurrence or death by 49%. The combination therapy also reduced the risk of distant metastasis by 59%. Overall survival, meaning no death from cancer or any other cause, was 92.2%for the vaccine with immunotherapy group, while for the immunotherapy-alone group it was 71.3%.
“Our study offers strong evidence to melanoma patients that intismeran vaccine therapy, when used in combination with immunotherapy, can demonstrably reduce their risk of having their cancer return and improve clinical outcomes,” said study senior investigator Janice Mehnert, MD, a professor in the Department of Medicine at NYU Grossman School of Medicine.
“Our findings also serve as encouragement to cancer researchers globally that mRNA vaccines like intismeran could work well in combination with immunotherapy for other cancers whose high rates of mutations have proven difficult to target,” said Dr Mehnert, who also serves as director of the melanoma medical oncology program and associate director of clinical research at Perlmutter Cancer Center.
The study results highlight the role of T cells, which are capable of attacking viruses as well as cancers. To spare normal cells, the immune system uses checkpoint molecules on T cell surfaces to “turn off” their attack against viruses when they clear the infection. The body may recognide tumours as abnormal, but cancer cells hijack checkpoints to turn off and evade immune responses. Immunotherapies like pembrolizumab seek to block checkpoints, specifically the PD-1 protein receptor, making cancer cells more “visible” and vulnerable again to immune cells.
Immunotherapies, including PD-1 inhibitors like pembrolizumab, have become the mainstay for treating melanoma, although they do not work for all patients, because melanoma cells, known for their ability to evade the immune system, can become resistant to immunotherapy. For this reason, researchers have looked at adding vaccines.
The vaccine intismeran is based on messenger RNA, a chemical cousin of DNA that provides cells with instructions for making proteins. Intismeran and other mRNA cancer vaccines are meant to teach the immune system to recognize cancer cells as different from normal cells. In designing a vaccine against melanoma, researchers attempted to trigger an immune response to specific abnormal proteins, called neoantigens, made by cancer cells.
Because the study volunteers all had their tumours removed, researchers were able to analyse their cells for 34 neoantigens that were specific to each melanoma and create a personalised vaccine for each patient. As a result, T cells specific to the neoantigen proteins encoded by the mRNA were produced. Those T cells could then attack any melanoma cells trying to grow or spread.
Dr. Mehnert said that a phase 3, multicenter trial is already underway to determine if intismeran helps as a first-line therapy in combination with pembrolizumab for melanoma. Already, the vaccine is being tested to see if it also works to prevent recurrence of lung and other cancers.
For the KEYNOTE-942 trial, patients were enrolled at cancer centers in Australia and the United States from 2019 to 2021. All were men and women who had had surgery to remove their melanoma tumors. Seven patients in each treatment group died during follow-up, most from cancer. Side effects were considered manageable and included fatigue, pain at injection sites, and chills.