A breakthrough study, published in Science Translational Medicine, features a biomedical engineering innovation with the potential to transform trauma care and surgical practices. The multidisciplinary, multi-university scientific research team developing platelet-like particles that integrate into the body’s clotting pathways to stop haemorrhage.
Addressing a longstanding gap in surgical and trauma care, this advancement holds potential for patient implementation. Patients experiencing acute trauma often require platelet transfusions to manage bleeding; storage constraints restrict their utility in prehospital scenarios. Synthetic platelet-like particles (PLPs) offer a potential alternative for promptly addressing uncontrolled bleeding.
The team has engineered platelet-like particles capable of traveling through the bloodstream and then homing to the site of tissue damage, where they augment the clotting process and then support subsequent wound healing. The approach addresses an unmet clinical need in trauma care and surgical practice. Research team member Andrew Lyon, Founding Dean and Professor of Chapman University’s Fowler School of Engineering, stress the importance of this breakthrough.
“This work represents a pivotal moment in biomedical engineering, showcasing the tangible translational potential of Platelet-Like Particles,” remarked Lyon. “This remarkable collaborative effort has led to a solution that not only addresses critical clinical needs but also suggests a paradigm shift in treatment modalities.”
The study’s comprehensive approach involved rigorous testing in larger animal models of traumatic injury and illustrated that the intervention is extremely well tolerated across a range of models.
Ashley Brown, corresponding author on the study and an associate professor in the joint biomedical engineering program at North Carolina State University and the University of North Carolina at Chapel Hill, said, “In the mouse and pig models, healing rates were comparable in animals that received platelet transfusions and synthetic platelet transfusions and both groups fared better than animals that did not receive either transfusion.”
One of the study’s most significant findings is that these particles can be excreted renally, presenting a breakthrough in elimination pathways associated with injectable, synthetic biomaterials. The remarkable safety profile demonstrated in the study makes it safe and effective in trauma and surgical interventions. This advancement could potentially lead to improved medical treatments and outcomes for patients undergoing such procedures.
Lyon noted, “Given the success of our research and the effectiveness of the synthetic platelets, the team is pushing forward on a path aimed at eventually seeing clinical implementation of this technology.”
The device represents a huge leap ahead guide neurosurgeonswith visualised brain activity
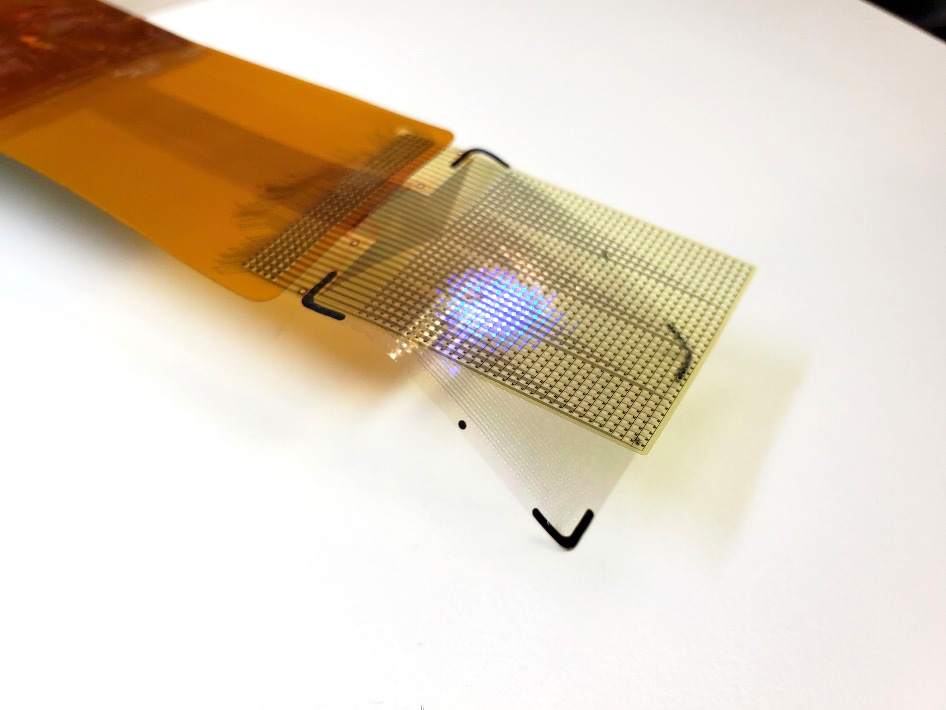
The device’s LEDs can light up in several colors. This allows surgeons to see which areas they need to operate on. It allows them to track brain states during surgery, including the onset of epileptic seizures. Credit: UCSF
A thin film that combines an electrode grid and LEDs can both track and produce a visual representation of the brain’s activity in real-time during surgery-a huge improvement over the current state of the art. The device is designed to provide neurosurgeons visual information about a patient’s brain to monitor brain states during surgical interventions to remove brain lesions including tumours and epileptic tissue.
Each LED in the device represents the activity of a few thousand neurons. In a series of proof-of-concept experiments in rodents and large non-primate mammals, researchers showed that the device can effectively track and display neural activity in the brain corresponding to different areas of the body. In this case, the LEDs developed by the team light up red in the areas that need to be removed by the surgeon. Surrounding areas that control critical functions and should be avoided show up in green.
The study also showed that the device can visualise the onset and map the propagation of an epileptic seizure on the surface of the brain. This would allow physicians to isolate the ‘nodes’ of the brain that are involved in epilepsy. It also would allow physicians to deliver necessary treatment by removing tissue or by using electrical pulses to stimulate the brain.
“Neurosurgeons could see and stop a seizure before it spreads, view what brain areas are involved in different cognitive processes, and visualise the functional extent of tumour spread. This work will provide a powerful tool for the difficult task of removing a tumour from the most sensitive brain areas,” said Daniel Cleary, one of the study’s coauthors, a neurosurgeon and assistant professor at Oregon Health and Science University.
The device was conceived and developed by a team of engineers and physicians from University of California San Diego and Massachusetts General Hospital (MGH) and was led by Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at UC San Diego.
Protecting critical brain functions
During brain surgery, physicians need to map brain function to define which areas of the organ control critical functions and can’t be removed. Currently, neurosurgeons work with a team of electrophysiologists during the procedure. But that team and their monitoring equipment are located in a different part of the operating room.
Brain areas that need to be protected and those that need to be operated on are either marked by electrophysiologists on a paper that is brought to the surgeon or communicated verbally to the surgeon, who then places sterile papers on the brain surface to mark these regions.
“Both are inefficient ways of communicating critical information during a procedure, and could impact its outcomes,” said Dr Angelique Paulk of MGH, who is a co-author and co-inventor of the technology.
In addition, the electrodes currently used to monitor brain activity during surgery do not produce detailed fine grained data. So surgeons need to keep a buffer zone, known as resection margin, of 5 to 7mm around the area they are removing inside the brain.
This means that they might leave some harmful tissue in. The new device provides a level of detail that would shrink this buffer zone to less than 1mm.
“We invented the brain microdisplay to display with precision critical cortical boundaries and to guide neurosurgery in a cost-effective device that simplifies and reduces the time of brain mapping procedures,” said Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at the UC San Diego Jacobs School of Engineering.
Researchers installed the LEDs on top of another innovation from the Dayeh lab, the platinum nanorod electrode grid (PtNRGrid). Using the PtNRGrids since 2019, Dayeh’s team pioneered human brain and spinal cord mapping with thousands of channels to monitor brain neural activity.
They reported early safety and effectiveness results in a series of articles in Science Translational Medicine in 2022 in tens of human subjects.
(New sensor grids record human brain signals with record breaking resolution and Microelectrode array can enable safer spinal cord surgery) — ahead of Neuralink and other companies in this space.
The PtNRGrid also includes perforations, which enable physicians to insert probes to stimulate the brain with electrical signals, both for mapping and for therapy.
How it’s made
The display uses gallium nitride-based micro-LEDs, bright enough to be seen under surgical lights. The two models built measures 5mm or 32mm on a side, with 1024 or 2048 LEDs. They capture brain activity at 20 000 samples a second, enabling .
“This enables precise and real-time displays of cortical dynamics during critical surgical interventions,” said Youngbin Tchoe, the first author and co-inventor, formerly a postdoc in the Dayeh group at UC San Diego and now an assistant professor at Ulsan National Institute of Science and Technology.
In addition to the LEDs, the device includes acquisition and control electronics as well as software drivers to analyse and project cortical activity directly from the surface of the brain.
“The brain iEEG-microdisplay can impressively both record the activity of the brain to a very fine degree and display this activity for a neurosurgeon to use in the course of surgery. We hope that this device will ultimately lead to better clinical outcomes for patients with its ability to both reveal and communicate the detailed activity of the underlying brain during surgery,” said study coauthor Jimmy Yang, a neurosurgeon and assistant professor at The Ohio State University.
Next steps
Dayeh’s team is working to build a microdisplay that will include 100 000 LEDs, with a resolution equivalent to that of a smartphone screen – for a fraction of the cost of a high-end smartphone. Each LED in those displays would reflect the activity of a few hundred neurons.
These brain microdisplays would also include a foldable portion. This would allow surgeons to operate within the foldable portion and monitor the impact of the procedure as the other, unfolded portion of the microdisplay shows the status of the brain in real time.
Researchers are also working on one limitation of the study – the close proximity of the LED sensors and the PtNRGrids led to a slight interference and noise in the data.
The team plans to build customised hardware to change the frequency of the pulses that turn on the LEDs to make it easier to screen out that signal, which is not relevant to the brain’s electrical activity.
A common practice of shoulder surgeons may be impairing the success of rotator cuff surgery, a new study from orthopaedic scientists and biomedical engineers at Columbia University suggests.
During the surgery, surgeons often remove the bursa, a cushion-like tissue, while repairing torn tendons in the shoulder joint – but the study, which is published in Science Translational Medicine, suggests that the small tissue in fact plays a role in helping the shoulder heal.
“It is common to remove the bursa during shoulder surgery, even for the simple purpose of visualising the rotator cuff,” says Stavros Thomopoulos, PhD, the study’s senior author and the Robert E. Carroll and Jane Chace Carroll Laboratories Professor of Orthopaedic Surgery at Columbia University Vagelos College of Physicians and Surgeons.
“But we really don’t know the role of the bursa in rotator cuff disease, so we don’t know the full implications of removing it,” Thomopoulos says. “Our findings in an animal model indicate that surgeons should not remove the bursa without carefully considering the consequences.”
The challenge of rotator cuff surgery
Most damage to tendons in the rotator cuff comes from wear and tear that accumulates over years of repetitive motions. Among people over 65, about half have experienced a rotator cuff tear, which can make simple daily tasks like combing one’s hair difficult and painful.
More than 500 000 rotator cuff surgeries are performed each year in the US to repair these injuries, restore range of motion, and alleviate pain, but failure is common – ranging from one in five surgeries in young patients to as high as 94% in elderly patients with large tears.
Rotator cuff repairs usually fail because of poor healing between tendon and bone where the tendon is reattached to the bone.
Bursa: friend or foe?
The bursa is a thin, fluid-filled sac originally thought to protect the tendons by providing a cushion between the tendons and adjacent bones.
The bursa often becomes inflamed, sometimes concurrently, when underlying tendons are injured, and surgeons often remove the tissue because they suspect it is a source of shoulder inflammation and pain. But recent studies suggest the tissue may be playing other biological roles besides mechanical cushioning, including promoting healing of injuries to the tendons in the shoulder.
To explore the role of the bursa in rotator cuff disease, Thomopoulos and graduate student Brittany Marshall examined rats with repaired rotator cuff injuries, with and without bursa removal.
Bursa removal impairs uninjured tendons
After the rats underwent repair of a rotator cuff injury, the researchers measured the mechanical properties of the repaired tendon and an adjacent undamaged tendon, the quality of the underlying bone, and changes to protein and gene expression.
The researchers found that the presence of the bursa protected the undamaged tendon by maintaining its mechanical properties and protected the bone by maintaining its morphometry. When the bursa was removed, strength of the undamaged tendon deteriorated and the bone quality deteriorated.
“The loss of mechanical integrity in the uninjured tendon in the absence of the bursa was striking,” Thomopoulos says. Uninjured tendons in the shoulder frequently degenerate over time after the initial injury, and “the animal data imply that retaining the bursa may prevent or delay progression of this pathology.”
In the damaged tendon, the researchers found that the bursa promoted an inflammatory response and activated wound healing genes, but no changes were seen in the mechanical properties of the repaired tendon two months after the repair. It’s possible that differences in mechanical properties would be detected after a longer healing period, Thomopoulos says, something that the research team is currently investigating.
“Overall, what we’re seeing is a beneficial role of the bursa for rotator cuff health, in contrast with the historical view that the inflamed bursa is detrimental,” says Thomopoulos.
The researchers documented similar changes to cells and proteins in bursa samples from patients who underwent surgery to repair rotator cuff injuries, suggesting comparable processes may occur in people.
The bursa as a drug delivery depot
If the bursa is not removed, the tissue could be used to deliver drugs to the repaired tendon to improve healing.
Thomopoulos and Marshall explored this possibility by injecting corticosteroid microspheres into the bursa of their rat model after tendon injury. Steroids are often used to treat musculoskeletal injuries and reduce inflammation.
“The treatment results are somewhat preliminary and require additional timepoints and mechanical characterisation before we can draw strong conclusions,” Thomopoulos says, “but our initial data supports the idea that the bursa can be therapeutically targeted to improve rotator cuff healing.”
With technology developed at UC Riverside, scientists can, for the first time, make high resolution images of the human spinal cord during surgery. The advancement could help bring real relief to millions suffering chronic back pain.
The technology, known as fUSI or functional ultrasound imaging, not only enables clinicians to see the spinal cord, but also enables them to map the cord’s response to various treatments in real time. A paper published today in the journal Neuron details how fUSI worked for six people undergoing electrical stimulation for chronic back pain treatment.
“The fUSI scanner is freely mobile across various settings and eliminates the requirement for the extensive infrastructure associated with classical neuroimaging techniques, such as functional magnetic resonance imaging (fMRI),” said Vasileios Christopoulos, assistant professor of bioengineering at UCR who helped develop the technology. “Additionally, it offers ten times the sensitivity for detecting neuroactivation compared to fMRI.”
Until now, it has been difficult to evaluate whether a back pain treatment is working since patients are under general anaesthesia, unable provide verbal feedback on their pain levels during treatment. “With ultrasound, we can monitor blood flow changes in the spinal cord induced by the electrical stimulation. This can be an indication that the treatment is working,” Christopoulos said.
The spinal cord is an “unfriendly area” for traditional imaging techniques due to significant motion artifacts, such as heart pulsation and breathing. “These movements introduce unwanted noise into the signal, making the spinal cord an unfavorable target for traditional neuroimaging techniques,” Christopoulos said.
By contrast, fUSI is less sensitive to motion artifacts, using echoes from red blood cells in the area of interest to generate a clear image. “It’s like submarine sonar, which uses sound to navigate and detect objects underwater,” Christopoulos said. “Based on the strength and speed of the echo, they can learn a lot about the objects nearby.”
Christopoulos partnered with the USC Neurorestoration Center at Keck Hospital to test the technology on six patients with chronic low back pain. These patients were already scheduled for the last-ditch pain surgery, as no other treatments, including drugs, had helped to ease their suffering. For this surgery, clinicians stimulated the spinal cord with electrodes, in the hopes that the voltage would alleviate the patient’s discomfort and improve their quality of life.
“If you bump your hand, instinctively, you rub it. Rubbing increases blood flow, stimulates sensory nerves, and sends a signal to your brain that masks the pain,” Christopoulos said. “We believe spinal cord stimulation may work the same way, but we needed a way to view the activation of the spinal cord induced by the stimulation.”
The Neuron paper details how fUSI can detect blood flow changes at unprecedented levels of less than 1mm/s. For comparison, fMRI is only able to detect changes of 2cm/s.
“We have big arteries and smaller branches, the capillaries. They are extremely thin, penetrating your brain and spinal cord, and bringing oxygen places so they can survive,” Christopoulos said. “With fUSI, we can measure these tiny but critical changes in blood flow.”
Generally, this type of surgery has a 50% success rate, which Christopoulos hopes will be dramatically increased with improved monitoring of the blood flow changes. “We needed to know how fast the blood is flowing, how strong, and how long it takes for blood flow to get back to baseline after spinal stimulation. Now, we will have these answers,” Christopoulos said.
Moving forward, the researchers are also hoping to show that fUSI can help optimise treatments for patients who have lost bladder control due to spinal cord injury or age. “We may be able to modulate the spinal cord neurons to improve bladder control,” Christopoulos said.
“With less risk of damage than older methods, fUSI will enable more effective pain treatments that are optimised for individual patients,” Christopoulos said. “It is a very exciting development.”
A neurosurgeon alleged during his employment tribunal that a “gang culture” exists within the neurosurgery department of an NHS hospital already beset by claims of a toxic culture and investigations into negligence.
As reported by the BBC, Dr Mansoor Foroughi was dismissed from University Hospitals Sussex in 2022 for misconduct. At a separate employment tribunal, Krish Singh, the former clinical director for general surgery, claimed that rota changes reduced the number of “safe” consultants, putting patients at risk.
Four whistleblowers had also told the BBC of a “Mafia-like” culture, where patients had died unnecessarily and others “maimed”. These new allegations came to light as the BBC and The Times fought a nine-month court battle to have the employment tribunal documents unsealed.
Dr Foroughi alleges that one colleague was signed off to do complex spinal procedures despite lacking training, another performed procedures with a “disproportionate” mortality rate, and yet another took on private work while on call to the NHS – a serious breach of conduct.
University Hospital Sussex encompasses several hospitals, which includes Royal Sussex Country Hospital, which has been the source of many complaints, and a history of poor service delivery, which was put into special measures between 2016 and 2019.
At least 105 cases of alleged medical negligence from failings at the hospital’s neurosurgery and general surgery departments are being investigated by police. According to court documents, there was “serious dysfunctionality in the neurosurgery department” with “stark divisions between colleagues”.
An investigation by the Royal College of Surgeons found that “a culture of fear” existed in the hospital’s surgery department, and that senior staff were “dismissive and disrespectful”. Two staff were allegedly assaulted.
In a statement, the trust said: “The trust will vigorously contest these claims at the Employment Tribunals, which we are keen take place at the earliest opportunity so they can be examined properly and fairly.
“Dismissing anyone, or removing someone from a leadership role, is an absolute last resort and we would always seek to avoid this outcome if possible.
“In both of these cases, due process was followed, and we are confident we did the right things, in the right way, for the benefit of our patients, their care and safety.”
Withdrawing aspirin one month after percutaneous coronary intervention (PCI) in high-risk heart patients and keeping them on ticagrelor alone safely improves outcomes and reduces major bleeding by more than half when compared to patients taking aspirin and ticagrelor combined (also known as dual antiplatelet therapy or DAPT), which is the current standard of care.
These are the results from the ULTIMATE-DAPT study announced during a late-breaking trial presentation at the American College of Cardiology Scientific Sessions on Sunday, April 7, and published in The Lancet.
This is the first and only trial to test high-risk patients with recent or threatened heart attack (acute coronary artery syndromes, or ACS) taking ticagrelor with a placebo starting one month after PCI, and compare them with ACS patients taking ticagrelor with aspirin over the same period. The significant findings could change the current guidelines for standard of care worldwide.
“Our study has demonstrated that withdrawing aspirin in patients with recent ACS one month after PCI is beneficial by reducing major and minor bleeding through one year by more than 50 percent. Moreover, there was no increase in adverse ischaemic events, meaning continuing aspirin was causing harm without providing any benefit,” says Gregg W. Stone, MD, the study co-chair of ULTIMATE-DAPT, who presented the trial results.
“It is my belief that it’s time to change the guidelines and standard clinical practice such that we no longer treat most ACS patients with dual antiplatelet therapy beyond one month after a successful PCI procedure. Treating these high-risk patients with a single potent platelet inhibitor such as ticagrelor will improve prognosis,” adds Dr Stone.
The study analysed 3400 patients with ACS at 58 centres in four countries between August 2019 and October 2022. All of the patients had undergone PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow. The patients were stable one month after PCI and were on ticagrelor and aspirin. Researchers randomised the patients after one month, withdrawing aspirin in 1700 patients and putting them on ticagrelor and a placebo, while leaving the other 1700 patients on ticagrelor and aspirin. All patients were evaluated between 1 and 12 months after the procedure.
During the study period, 35 patients in the ticagrelor-placebo group had a major or minor bleeding event, compared to 78 patients in the ticagrelor-aspirin group, meaning that the incidence of overall bleeding incidents was reduced by 55 percent by withdrawing aspirin. The study also analysed major adverse cardiac and cerebrovascular events including death, heart attack, stroke, bypass graft surgery, or repeat PCI. These events occurred in 61 patients in the ticagrelor-placebo group compared to 63 patients in the ticagrelor-aspirin group, and were not statistically significant – further demonstrating that removing aspirin did no harm and improved outcomes.
“It was previously believed that discontinuing dual antiplatelet therapy within one year after PCI in patients with ACS would increase the risk of heart attack and other ischaemic complications, but the present study shows that is not the case, with contemporary drug-eluting stents now used in all PCI procedures. Discontinuing aspirin in patients with a recent or threatened heart attack who are stable one month after PCI is safe and, by decreasing serious bleeding, improves outcomes,” Dr Stone adds. “This study extends the results of prior work that showed similar results but without the quality of using a placebo, which eliminates bias from the study.”
By HualinXMN – Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=133759262
New research from Cedars-Sinai found that glucagon-like peptide-1 receptor agonists (GLP-1RAs) are associated with an increased risk of aspiration pneumonia following endoscopy. The large, population-based study is published in the leading peer-reviewed journal Gastroenterology.
One way the new obesity medications work is by slowing digestion, so people feel full longer, causing them to eat less.
This also means that food sits in the stomach longer. As a result, the stomach may not empty completely during the usual duration of fasting that is recommended ahead of a surgical procedure to decrease risk of aspiration, explained the study’s corresponding author, Ali Rezaie, MD, medical director of the GI Motility Program and director of bioinformatics at the MAST Program at Cedars-Sinai.
“Aspiration during or after endoscopy can be devastating,” Rezaie said.
“If significant, it can lead to respiratory failure, ICU admission and even death. Even mild cases may require close monitoring, respiratory support and medications including antibiotics. It is important we take all possible precautions to prevent aspiration from occurring.”
The study analysed data from nearly 1 million de-identified U.S. patients who underwent upper or lower endoscopy procedures between January 2018 and December 2020.
Patients who were prescribed GLP-1RA medications had a 33% higher chance of experiencing aspiration pneumonia than those who did not take these medications before the procedure.
This comparison also considered other variables that could influence the outcome to ensure a fair comparison between the two groups.
“When we apply this risk to the more than 20 million endoscopies that are performed in the U.S. each year, there may actually be a large number of cases where aspiration could be avoided if the patient safely stops their GLP-1RA medication in advance,” Rezaie said.
“The results of this study could change clinical practice,” said Yee Hui Yeo, MD, first author of the study and a clinical fellow in the Karsh Division of Gastroenterology and Hepatology at Cedars-Sinai. “Patients taking these medications who are scheduled to undergo a procedure should communicate with their healthcare team well in advance to avoid unnecessary and unwanted complications.”
The two most common obesity surgeries, gastric bypass and gastric sleeve, have few short-term complications and show no significant differences, according to study findings published in the journal JAMA Network Open. These are the first results of a multicentre randomised controlled trial comparing obesity surgeries conducted by the University of Gothenburg.
Patients undergoing obesity surgery will normally have a BMI of at least 40, or 35 if they also have other serious medical conditions related to obesity.
The most common procedures are gastric bypass, where a large part of the stomach and part of the small intestine are bypassed, and gastric sleeve, where a large part of the stomach is surgically removed.
The aim of the current study was to compare the short-term risks of the different procedures.
The study is the largest of its kind. 1735 adult patients planned for surgery in Norway and Sweden between 2015 and 2022 agreed to participate, and they were randomly assigned to either gastric bypass or gastric sleeve.
Relatively few complications
Surgical time was longer for gastric bypass, averaging 68 minutes compared to 47 minutes for gastric sleeve, but hospitalisation after surgery was one day regardless of method.
The follow-ups also gave equivalent results for the two methods.
At 30 days after surgery, both groups had relatively few complications such as haemorrhage, leakage, blood clots and infections.
No deaths occurred during the follow-up period of a total of 90 days.
“For both surgical procedures, the risk of complications is very low, especially from an international perspective, and there is no statistically significant or clinically relevant difference between the groups,” says Suzanne Hedberg, first author of the study.
Many stakeholders and many opinions
“Many people have had surgery, or are on waiting lists for surgery, and there are lots of discussions and opinions about the different methods. What the study shows is that patients and doctors can now choose their surgical method without considering short-term surgical risks,” she says.
Suzanne Hedberg defended her thesis in surgery at Sahlgrenska Academy, University of Gothenburg in April 2023, and is a consultant at Sahlgrenska University Hospital.
The study, included in her thesis, is the first publication with results from BEST (Bypass Equipoise Sleeve Trial), a Scandinavian registry-based randomised controlled multicentre study comparing the two methods of obesity surgery.
The main outcome of the trial which analyses the risk of complications and weight progression over 5 years, is expected to be completed in 2028.
“For the ongoing studies, we are off to a good start with equivalent groups, laying a good foundation for further comparisons of more long-term results,” concludes Suzanne Hedberg.
Including patients as partners for making decisions about their medical treatments is an important aspect of patient-centred care. A new study from England examined choices that patients with breast cancer make when considering where to have surgery for their condition and assessed how policies that offer such choices might affect inequalities in the health care system. The findings are published in CANCER.
For the study, investigators analysed data from the National Health Service (NHS), the publicly funded health care system in the United Kingdom that offers patients with cancer the opportunity to select any hospital providing cancer treatment, and identified all women diagnosed with breast cancer from 2016 to 2018 who had breast-conserving surgery or a mastectomy.
Records showed that 22 622 of 69,153 patients undergoing breast-conserving surgery (32.7%) and 7179 of 23 536 patients undergoing mastectomy (30.5%) bypassed their nearest hospital to receive surgery farther away from home. Women who were younger, without additional medical conditions, of white ethnic background, or lived in rural areas were more likely to travel to more distant hospitals.
Patients were more likely to be treated at hospitals classified as specialist breast reconstruction centres even if they personally were not undergoing breast reconstruction after surgery. Patients who had a mastectomy and immediate breast reconstruction were more likely to travel to hospitals that had surgeons with a strong media reputation for breast cancer surgery, and patients were less likely to travel to hospitals with shorter surgical waiting times. Patients did not seem to make choices based on hospitals’ research activity, quality rating, breast re-operation rates (to remove additional cancer cells that were missed), or status as a multidisciplinary cancer centre (where patients can receive all their care at one location).
The investigators noted that this separation – elderly patients, those with comorbidities, and those from ethnic minority backgrounds receiving care at their local hospital, while others travel to other hospitals and specialist centres – could further drive inequalities in access to quality care.
“As marginalized groups already face barriers to high-quality care, it is important for policy makers to consider measures that mitigate against the risks of increasing inequalities in access and outcomes, by for example providing free transport, accommodation, or even protection against loss of income,” said co-author Lu Han, PhD, of the London School of Hygiene & Tropical Medicine. “Moreover, patients prefer to access information on the quality of breast cancer care of the hospitals in their region at the start of the management pathway when a diagnosis is sought. Such information should be easy to understand and presented in a format that can support the trade-offs that patients have to make.”
Young people who have had surgery for obesity do not improve their mental health despite significant and permanent weight loss. At the same time, bariatric surgery also increases the risk of early alcohol problems. This is according to the largest long-term study of young people who have undergone bariatric surgery, the results of which were published in Lancet Child and Adolescent Health.
The researchers studied mental health problems – before and after surgery – among all young people in Sweden who underwent bariatric surgery between 2007 and 2017. The study was conducted using register data, which enabled the scope of the study and facilitated comparisons with other groups in society.
The study recruited 1554 adolescents (< 21 years) with severe obesity underwent bariatric surgery between 2007 and 2017, 1169 (75%) of whom were female. At time of surgery, the mean age was 19·0 years [SD 1·0], and the mean BMI was 43·7 kg/m2 (SD 5·5). They were matched with 15 540 adolescents from the general population.
It was found that young people who underwent surgery were more likely to have received treatment and medication for mental health problems already five years before the surgery.
“Although mental illness generally increases between the ages of 15 and 21, for this group the need for treatment increased faster than for young people in general”, says Kajsa Järvholm, Associate Professor of Psychology at Lund University.
Unfortunately, this pattern continued even after obesity surgery; the young people who had the surgery continued to have a greater need for mental health treatment than their peers.
“Obesity surgery has very positive effects on weight, blood sugar and blood pressure control, but when it comes to mental health, it does not get better or worse after bariatric surgery”, says Martin Neovius, Professor of Clinical Epidemiology at Karolinska Institutet.
Additional findings from the new study include an increase in dependency diagnoses, particularly on alcohol, in the surgical group, both in comparison to pre-surgery and to young people in general.
The study is the largest long-term study in the world of young people who have had obesity surgery.