Researchers at Monash University have identified a new way of mapping ‘phosphenes’ – the visual perception of the bright flashes we see when no light is entering the eye – to improve the outcome of surgery for patients receiving a cortical visual prosthesis.
Cortical visual prostheses are devices implanted onto the brain with the aim of restoring sight by directly stimulating the area responsible for vision, the visual cortex, bypassing damage to the retina of the eye or the optic nerve. Phosphenes, apparent flashes and patterns of lights, were described by the ancient Greeks and can be elicited by pressure, injury, disease, certain medications or direct electrical stimulation.
A typical prosthesis consists of an array of fine electrodes, each of which is designed to trigger a phosphene. Given the limited number of electrodes, understanding how electrodes can best be placed to generate useful perceived images becomes critical.
Published in the Journal of Neural Engineering, the study presents a more realistic simulation for cortical prosthetic vision.
As part of this researchers from the Department of Electrical and Computer Systems Engineering at Monash University, led by Associate Professor Yan Tat Wong, are honing in on the ideal distribution of phosphenes.
“Phosphenes are likely to be distributed unevenly in an individual’s visual field, and differences in the surface of the brain also affect how surgeons place implants, which together result in a phosphene map unique to each patient,” Associate Professor Wong said.
The study used a retinotopy dataset based on magnetic resonance imaging (MRI) scans, consulting with a neurosurgeon about realistic electrode implantation sites in different individuals, and applying a clustering algorithm to determine the most suitable regions to present stimuli.
Sighted participants recruited for the study were asked to test and verify the phosphene maps based on visual acuity and object recognition.
“We’re proposing a new process that incorporates our simulation paradigm into surgical planning to help optimise the implantation of a cortical prosthesis,” Associate Professor Wong said.
The process would begin with an MRI scan to plot the recipient’s brain surface in the area of the visual cortex. Potential implant locations would then be identified, and the simulation developed in the Monash research would be used to plot phosphene maps.
“We can use the metrics we computed to find practical implant locations that are more likely to give us a usable phosphene map, and we can verify those options through psychophysics tests on sighted participants using a virtual reality headset,” Associate Professor Wong said.
“We believe this is the first approach that realistically simulates the visual experience of cortical prosthetic vision.”
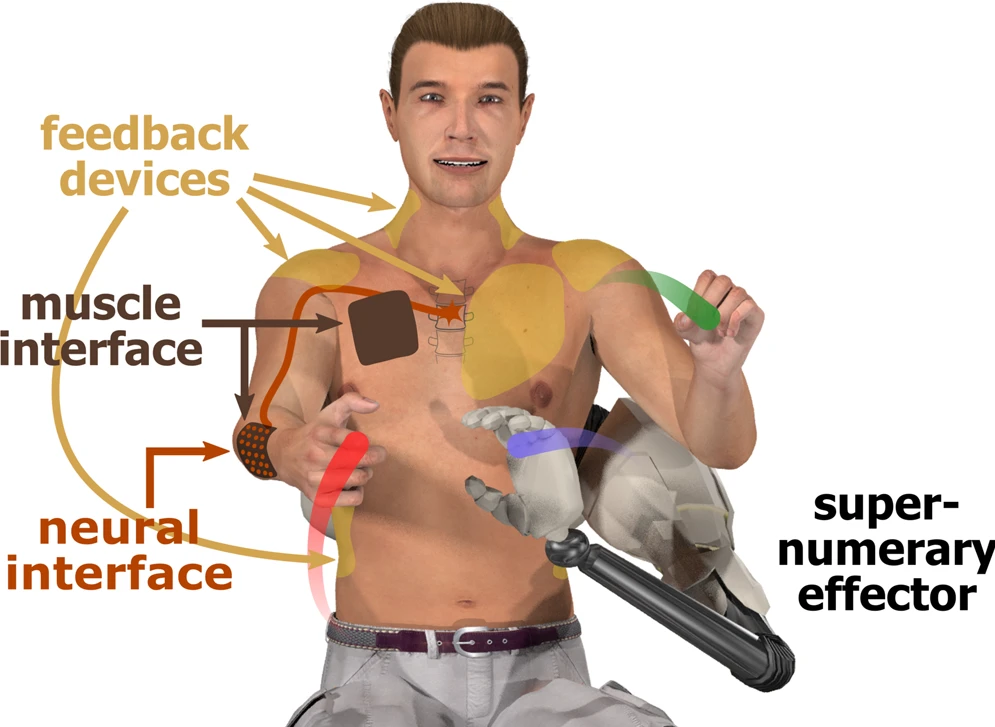
Interfaces for DoF augmentation (figure by Tobias Pistohl). From Eden at al., Nature Communications. 2022
Busy doctors and nurses may have often found themselves wishing they had an extra arm to help with a patient or help with a difficult suture. Researchers around the world are developing supernumerary robotic arms to help workers achieve certain tasks unaided, or with less strain – but how long would it take to master learning an additional limb? The answer is: not long at all. One hour’s worth of training is enough for people to carry out a task with their ‘third arm’ as effectively as with a partner, according to the results of a new study published in IEEE Open Journal of Engineering in Medicine and Biology.
A new study by researchers at Queen Mary University of London, Imperial College London and The University of Melbourne has found that people can learn to use supernumerary robotic arms as effectively as working with a partner in just one hour of training.
The study investigated the potential of supernumerary robotic arms to help people perform tasks that require more than two hands. The idea of human augmentation with additional artificial limbs has long been a staple of science fiction.
Demonstrating performing a suture with an assistant robotic arm.
“Many tasks in daily life, such as opening a door while carrying a big package, require more than two hands,” said Dr Ekaterina Ivanova, lead author of the study from Queen Mary University of London. “Supernumerary robotic arms have been proposed as a way to allow people to do these tasks more easily, but until now, it was not clear how easy they would be to use.”
The study involved 24 participants who were asked to perform a variety of tasks with a supernumerary robotic arm. The participants were either given one hour of training in how to use the arm, or they were asked to work with a partner.
The results showed that the participants who had received training on the supernumerary arm performed the tasks just as well as the participants who were working with a partner. This suggests that supernumerary robotic arms can be a viable alternative to working with a partner, and that they can be learned to use effectively in a relatively short amount of time.
“Our findings are promising for the development of supernumerary robotic arms,” said Dr Ivanova. “They suggest that these arms could be used to help people with a variety of tasks, such as surgery, industrial work, or rehabilitation.”
Researchers have developed a non-invasive method for mapping the human auditory pathway, which could potentially be used as a tool to help clinicians decide the best surgical strategy for patients with profound hearing loss. The findings, published online in the journal eLife, highlight the importance of early interventions to give patients the ability to hear and understand speech, so that their auditory-language network can develop properly and their long-term outcomes are improved.
Sensorineural hearing loss (SNHL) occurs when the sensitive hair cells inside the cochlea are damaged, or when there is damage to the auditory nerve which transmits sound to the brain. A person with profound hearing loss is typically unable to hear any sounds, or at best, only very loud sounds. Congenital SNHL has increased in prevalence over the past two decades, from 1.09 to 1.7 cases per 1000 live births.
The sound of speech is carried through the brain by nerve fibres in regions known as the auditory pathway, and are processed in a region called the language network. In cases of congenital SNHL, the lack of speech inputs reaching the language network may hinder its proper development, leading to poorer spoken language skills.
Currently, the primary treatments for profound SNHL are cochlear and auditory brainstem implantation, where a device is used to stimulate the peripheral cochlea or the central cochlear nucleus, respectively. Both techniques can partially restore hearing in patients, but their language development outcomes can vary. This is especially true for patients with inner ear malformations (IEM) or cochlear nerve deficiencies (CND), which contribute to 15-39% of congenital SNHL cases.
“Where SNHL is caused by CNDs and/or IEMs, there is a great deal of uncertainty around the best method of treatment. This is due to the difficulty of assessing the condition of the cochlear nerve and distinguishing between certain types of IEM, both of which impact surgical decision making,” says senior authors Hao Wu, a professor and Chief Physician specialising in Otolaryngology at Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, China. Wu also serves as the Hospital Administrator and the Clinical and Academic Lead for the department. “We therefore need a more effective method for mapping the auditory pathway and diving deeper into how IEMs and CNDs affect the development of the auditory-language network.”
In their study, professor Wu’s team investigated the auditory and language pathways in 23 children under the age of six. They included 10 children with normal hearing, and 13 with profound SNHL. In the latter group, seven children had received cochlear implantations, two had received auditory brainstem implantations, and four were candidates for auditory brainstem implantations.
The human auditory pathway is difficult to investigate non-invasively due to its delicate and intricate subcortical structures located deep within the brain. To navigate this, the team developed a new methodology to reconstruct the pathway. First, they segmented the subcortical auditory structures using track density imaging, which are reconstructed from a specific type of MRI scan and provide much greater detail and information on the structural connectivity of the brain. This allowed them to delineate the cochlear nucleus and the superior olivary complex of the auditory pathway. They then tracked the auditory and language pathways using a neuroimaging technique called probabilistic tractography, which uses the information from an MRI scan to provide the most likely view of structural brain connectivity. Next, the team assessed the density and cross-section of the nerve fibres in the auditory and language pathways.
This combined methodology allowed them to investigate three key areas to inform surgical decision making: the condition of the nerve fibres in the auditory-language network of children with profound SNHL; the potential impact of IEMs and CNDs on the development of the network before surgical intervention; and the relationship between the pre-implant structural development of the network and the auditory-language outcomes following implantation.
The team’s observations revealed a lower nerve fibre density in children with profound SNHL, in comparison to those with normal hearing. This reduction was most pronounced in two regions of the inferior central auditory pathway, as well as the left language pathway.
In addition, the findings revealed that the language pathway is more sensitive than the central auditory system to IEMs and/or CNDs, implying that the structural development of the language pathway is more negatively impacted by the condition of the peripheral auditory structure. However, the authors caution that further study is required to validate this finding. As it is more difficult to image the central auditory pathway than the language pathway, this difference could have arisen due to the limitations of current neuroimaging technologies.
The authors say the study is also limited by a relatively small cohort of patients and an incomplete genetic dataset, so more studies with a more diverse patient population will also be needed. But with further validation, they add that the methodology could be used more widely for informing decisions in treating profound SNHL.
Cedars-Sinai investigators have shown that redo transcatheter aortic valve replacement (TAVR) procedures are both safe and effective when compared with situations in which patients with similar risk profiles undergo the same procedure for the first time.
The novel findings, which appear in The Lancet,are significant because recent randomised clinical trials have shown that TAVR is a meaningful treatment option for both younger and lower-risk surgical patients.
“We now know that redo TAVR with balloon-expandable valves may be a reasonable treatment for failed TAVR procedures in select patients,” said Raj Makkar, MD, Cedars-Sinai’s vice president of Cardiovascular Innovation and Intervention and the study’s senior author. “This is increasingly important, as the patients treated with TAVR are younger than they were a decade ago, meaning they will likely need a repeat procedure at some point in their lifetime.”
At both the 30-day post-procedure mark and at one year, Makkar’s team found no difference between redo TAVR or first-time TAVR in terms of death or stroke rates.
“Our findings also suggest that redo TAVR was associated with a significant improvement in quality of life,” said Makkar, who is also the associate director of the Smidt Heart Institute at Cedars-Sinai, director of the Interventional Cardiology Division in the Department of Cardiology, and the Stephen R. Corday, MD, Chair in Interventional Cardiology.
Transcatheter aortic valve replacement is a procedure that replaces a diseased aortic valve with a man-made valve. The procedure is now the standard treatment for patients with symptomatic severe aortic valve stenosis (narrowing of the artery).
The research team accessed a national database of all consecutive patients undergoing commercial TAVR in the US. Among the 350 591 patients who underwent TAVR between November 2011 and December 2022, 1320 individuals required redo procedures. The patients who underwent a repeat procedure had a mean age of 78 years old. About 58% were male and 42% female.
“Fixing damaged valves is something in which we excel at the Smidt Heart Institute,” said Eduardo Marbán, MD, PhD, professor and executive director of the Smidt Heart Institute. “Our finding that TAVR can be redone safely is yet another step in establishing this as the default technology for aortic valve disease.”
Interventionalists in the Smidt Heart Institute at Cedars-Sinai have successfully completed more than 6000 minimally invasive transcatheter aortic valve replacements to date, with more than 650 performed in fiscal year 2022.
Scientists at UC San Francisco are working on a new approach to treating kidney failure that could one day free people from needing dialysis or a transplant and the associated immunosuppressive drugs.
The technology, described in Nature Communications, shows for the first time that kidney cells, housed in an implantable device called a bioreactor, can survive inside the body of a pig and mimic several important kidney functions. The device can work quietly in the background, like a pacemaker, and does not trigger the recipient’s immune system to go on the attack.
Eventually, scientists plan to fill the bioreactor with different kidney cells that perform vital functions like balancing the body’s fluids and releasing hormones to regulate blood pressure, then pair it with a device that filters waste from the blood.
The aim is to produce a human-scale device to improve on dialysis, which keeps people alive after their kidneys fail but is a poor substitute for having a real working organ. In the US, more than 500 000 require dialysis several times a week. Many seek kidney transplants, but there are not enough donors, and only about 20 000 people receive them each year. An implantable kidney would be a boon.
This is a key step forward is for The Kidney Project, which is jointly headed by UCSF’s Shuvo Roy, PhD (technical director) and Vanderbilt University Medical Center’s William H. Fissell, MD (medical director).
“We are focused on safely replicating the key functions of a kidney,” said Roy, a bioengineering professor in the UCSF School of Pharmacy. “The bioartificial kidney will make treatment for kidney disease more effective and also much more tolerable and comfortable.”
Inspired by nature, honed by science
Roy and his colleagues engineered the bioreactor to connect directly to blood vessels and veins, allowing the passage of nutrients and oxygen, much like a transplanted kidney would. Silicon membranes keep the kidney cells inside the bioreactor safe from attack by the recipient’s immune cells.
The team used a proximal tubule cell, which regulates water, as a test case. Co-author H. David Humes, MD, from the University of Michigan, had previously used these cells to help dialysis patients in the intensive care unit with life-saving results.
No immunosuppression needed
The team tracked the renal cells and the recipient animals for seven days after transplantation and both did well. The next step will be month-long trials, as required for by the U.S. Food and Drug Administration (FDA), first in animals and eventually in humans.
“We needed to prove that a functional bioreactor will not require immunosuppressant drugs, and we did,” Roy said. “We had no complications and can now iterate up, reaching for the whole panel of kidney functions at the human scale.”
A first-in-human trial of deep brain stimulation (DBS) for post-stroke rehabilitation patients has shown that using DBS to target the dentate nucleus – which regulates fine-control of voluntary movements, cognition, language, and sensory functions in the brain – is safe and feasible.
The EDEN trial (Electrical Stimulation of the Dentate Nucleus for Upper Extremity Hemiparesis Due to Ischemic Stroke) also shows that the majority of participants (9 of 12) demonstrated improvements in both motor impairment and function. Importantly, the study found that participants with at least minimal preservation of distal motor function at enrolment showed gains that almost tripled their initial scores.
Published in Nature Medicine, these findings build on more than a decade of preclinical work led by principal investigators Andre Machado, MD, PhD, and Kenneth Baker, PhD, at Cleveland Clinic.
“These are reassuring for patients as the participants in the study had been disabled for more than a year and, in some cases, three years after stroke. This gives us a potential opportunity for much needed improvements in rehabilitation in the chronic phases of stroke recovery,” said Dr Machado, patented the DBS method in stroke recovery. “The quality-of-life implications for study participants who responded to therapy have been significant.”
“We saw patients in the study regain levels of function and independence they did not have before enrolling in the research,” Dr Machado said. “This was a smaller study and we look forward to expanding as we have begun the next phase.”
The completed EDEN trial enrolled 12 individuals with chronic, moderate-to-severe hemiparesis of the upper extremity as a result of a unilateral middle cerebral artery stroke 12-to-36 months prior. There were no major complications throughout the study. Nine of the 12 participants improved to a degree that is considered meaningful in stroke rehabilitation.
Study participant Gert-Jan Oskam walking with the brain-spine interface. Credit: Swiss Federal Institute of Technology in Lausanne
A 40 year-old man, Gert-Jan Oskam, has regained the ability to walk independently after being paralysed from a spinal cord injury with the use of a new brain-spine interface. The ‘digital bridging’ technology, developed at the Swiss Federal Institute of Technology in Lausanne and described in Nature, consists of implants and a computer to translate brain signals of the intention to move into stimulations that move the legs accordingly..
This BSI system could be calibrated in minutes, and remained stable for one year, including use at home. The BSI enabled the participant to exert natural control over the movements of his legs to stand, walk, climb stairs and even traverse complex terrains.
In addition to the digital bridging, neurorehabilitation supported by the BSI improved neurological recovery. The participant regained the ability to walk with crutches overground even when the BSI was switched off. This digital bridge establishes a framework to restore natural control of movement after paralysis.
The system consists of a pair cortical of sensors, each an array with 64 electrodes housed in 5cm-diameter titanium discs. These discs are implanted snugly in the skull to pick up brain activity. They transmit the data wirelessly to a personalised headset, which also provides power for the sensors. The headset then sends the data to a portable processing unit (which may be carried in a backpack). Using specialised software, it uses this brain signal data to generates real-time predictions of motor intentions. These decoded intentions are translated into stimulation commands and sent on to another implant, a paddle array of 16 electrodes implanted next to the spinal cord, delivering current to the targeted dorsal root entry zones.
Neurosurgical implantation procedure
Oskam had sustained an incomplete cervical (C5/C6) spinal cord injury during a biking accident 10 years previously. He had already participated in a neurological recovery programme, the STIMO trial, which had used neurostimulation to get him to the stage where he could walk with the aid of a front-wheel walker. The neurorehabilitation from the trial also enabled him to use his hip flexors and lift his legs against gravity, but recovery had plateaued for the three years prior to his participation in the present study.
For the BSI to function, the researchers needed to locate neural features related to the intention to move the legs. To pinpoint the cortical regions associated with the intention to move, they used CT scans and magnetoencephalography. Taking into account anatomical restraints, they then decided on the positions of the implants.
Under general anaesthesia, surgeons performed a bicoronal incision of the scalp to allow two circular-shaped craniotomies over the planned locations of the left and right hemispheres. They then replaced the bone flaps with the two implantable recording devices, before closing the scalp.
The paddle lead had already been emplaced over the dorsal root entry zones of the lumbar spinal cord during the STIMO clinical trial. Its optimal positioning was identified using high-resolution structural imaging of the spine, and its final position was decided during the surgery based on electrophysiological recordings. The implantable pulse generator was inserted subcutaneously in the abdomen. Oskam was able to return home 24 hours after each procedure.
Elon Musk’s company Neuralink had finally received approval for human testing of its brain-computer interface (BCI). After initially rejecting the application, the US Food and Drug Administration finally gave the company the go-ahead on Thursday.
Neuralink, which aims to develop an implant that would allow humans to interface directly with computers as well as enabling medical applications such as controlling prostheses. Last year, the company showed off a monkey that was able to play the simple video game Pong on a monitor using its mind.
Neuralink is by no means the first company to try to achieve these goals. Many other institutions have made advances over the past decades, but the field is a difficult one and progress is slow. In its previous rejection, the FDA cited concerns such as the devices using lithium for their batteries, migration of the wires inside the brain and the difficulty of extracting the devices without harming brain tissue.
The company’s use of animals to develop the technology has infuriated activists, but this is a standard practice in development of BCI technology. Last year, whistleblowers accused the company of killing 1500 animals since its inception.
In a guidance document, the FDA says that, “The field of implanted BCI devices is progressing rapidly from fundamental neuroscience discoveries to translational applications and market access. Implanted BCI devices have the potential to bring benefit to people with severe disabilities by increasing their ability to interact with their environment, and consequently, providing new independence in daily life.”
China is also aggressively pursuing the development of BCIs as part of their ‘China Brain Project’, as discussed in the journal Neuron. It has a significant advantage as it has a large population of macaques to draw on, along with fewer ethical concerns and policies expediting biotech research.
Researchers report recreating a sense of temperature for amputees, by heating or cooling a part of their residual limb. The results of their tests are published in Science.
Researchers Silvestro Micera and Solaiman Shokur have been keen on incorporating new sensory feedback into prosthetic limbs for providing more realistic touch to amputees, and their latest study focuses on temperature. They stumbled upon a discovery about temperature feedback that far exceeds their expectations.
“When I touch the stump with my hand, I feel tingling in my missing hand, my phantom hand. But feeling the temperature variation is a different thing, something important… something beautiful,” says Francesca Rossi.
Rossi is an amputee from Bologna, Italy. She recently participated in a study to test the effects of temperature feedback directly to the skin on her residual arm. She is one of 17 patients to have felt her phantom, missing hand, change in temperature thanks to new EPFL technology. More importantly, she reports feeling reconnected to her missing hand.
“Temperature feedback is a nice sensation because you feel the limb, the phantom limb, entirely. It does not feel phantom anymore because your limb is back,” Rossi continues.
Placing a hot or cold object on the forearm of an intact individual, will result in that person feeling the temperature where it was placed. But in amputees, that temperature sensation on the residual arm may be felt in the phantom, missing hand.
By providing temperature feedback non-invasively, via thermal electrodes (aka thermodes) placed against the skin on the residual arm, amputees like Rossi report feeling temperature in their phantom limb. They can feel if an object is hot or cold, and can tell if they are touching copper, plastic or glass. In a collaboration between EPFL, Sant’Anna School of Advanced Studies (SSSA) and Centro Protesi Inail, the technology was successfully tested in 17 out of 27 patients.
“Of particular importance is that phantom thermal sensations are perceived by the patient as similar to the thermal sensations experienced by their intact hand,” explains Shokur, EPFL senior scientist neuroengineer who co-led the study.
Towards realistic bionic touch
The projection of temperature sensations into the phantom limb has led to the development of new bionic technology, one that equips prosthetics with non-invasive temperature feedback that allows amputees to discern what they’re touching.
“Temperature feedback is essential for relaying information that goes beyond touch, it leads to feelings of affection. We are social beings and warmth is an important part of that,” says Micera, Bertarelli Foundation Chair in Translational Neuroengineering, professor at EPFL and SSSA who also co-led the study. “For the first time, after many years of research in my laboratory showing that touch and position information can be successfully delivered, we envisage the possibility of restoring all of the rich sensations that one’s natural hand can provide.”
Temperature feedback, from well-being to prosthetics
Metaphysiks has been developing neuro-haptic technology, MetaTouch, which connects the body with digital worlds. MetaTouch combines touch and temperature feedback to augment physical products for well-being.
“This breakthrough highlights the power of haptics to improve medical conditions and enhance the quality of life for people with disabilities,” says Simon Gallo, Co-founder and Head of Technology at Metaphysiks.
The EPFL neuroengineers borrowed MetaTouch that provides thermal feedback directly to a user’s skin. With this device, they discovered the thermal phantom sensations and subsequently tested it in 27 amputees.
The Minitouch prototype and tests
For the study, Shokur and Micera developed the MiniTouch, a device that provides thermal feedback and specifically built for integration into wearable devices like prosthetics. The MiniTouch consists of a thin, wearable sensor that can be placed over an amputee’s prosthetic finger. The finger sensor detects thermal information about the object being touched, more specifically, the object’s heat conductivity. If the object is metallic, it will naturally conduct more heat or cold than, for instance, a plastic one. A thermode, one that is in contact with the skin on the amputee’s residual arm, heats up or cools down, relaying the temperature profile of the object being touched by the finger sensor.
“When we presented the possibility to get back temperature sensation on the phantom limb or the possibility to feel the contact with different materials, we obtained a lot of positive feedback. And eventually, we were able to recruit more than 25 volunteers in less than two years,” says Federico Morosato who was responsible for organizing the clinical aspect of the trials at Centro Protesi Inail.
The scientists found that small areas of skin on the residual arm project to specific parts of the phantom hand, like the thumb, or the tip of an index finger. As expected, they discovered that the mapping of temperature sensations between the residual arm and the entire projected phantom one is unique to each patient.
Bionic prosthetics for repairing the human body
Almost a decade ago, Micera and colleagues provided real-time sensory feedback about objects being grasped. They went on to improve touch resolution by providing feedback about an object’s texture and position information in a reliable way. Moreover, they discovered that amputees begin to embody their prosthetic hand if provided with sensory feedback directly into their intact nervous system. The added sensation of temperature feedback is yet another step towards building bionic prosthetics for repairing the human body. Fine-tuning temperature sensations and integrating these into a wearable device that can be mapped out to each patient are part of the next steps.
Combat-related injuries to bone are common in military personnel and can lead to pain and disability. Results from a new study in the Journal of Bone and Mineral Research suggest that amputations for such injuries may negatively affect bone mass.
Traumatic amputation from combat injuries has the potential to lead to osteoporosis through not only systemic inflammation and hormonal changes but also altered loading. Although a documented long-term complication of lower limb amputation is osteoporosis, this is often observed in older less active subjects with comorbidities, thus it is unknown whether this is secondary to systemic changes or changes to the loading environment.
In the study of 575 male adult UK military personnel with combat-related traumatic injuries and 562 without such injuries, veterans who sustained traumatic amputations often had low bone density in the hip region. Changes in bone health appeared to be mechanically driven rather than systemic and were only evident in those with lower limb amputations.
“We hope these results will drive further research into ways to reverse bone mineral density changes,” said co-author Group Captain Alex Bennett, Defence Professor of Rehabilitation, Defence Medical Rehabilitation Centre. “We need to investigate the role of prosthetics and exercise in reversing bone mineral density loss to reduce the longer-term risk of hip fracture. Because systemic treatments like bisphosphonates are not indicated in this young population with bone mineral density loss, it is important to understand other ways to reduce their hip fracture risk.”