The award was based on strides made by ASASA towards improving the quality of life of people living with AxSpa, as well as training done to build awareness in the medical fraternity around AxSpA in the country. With 36 posters entered into the awards by organisations across the globe, ASASA came out tops.
When asked about the award, van Dam said, “This was a real honour to represent South Africa at PARE. 2022 is also the first year that an African country was invited to attend PARE. Winning this award sheds light on our country and our unique problems. The delay to diagnosis of 10.8 years is just unacceptable. The access to the correct medication in both the private and public sector is also not sufficient for a debilitating, progressive disease that can lead to disability if left untreated.”
ASASA estimates that there are approximately 160 000 people suffering from the AxSpA in South Africa, with many of these sufferers undiagnosed. ASASA has made significant strides this year in the training of over 100 General Practitioners and over 250 optometrists around AxSpA diagnosis and the effects it can have on other parts of the body, like the eyes. In addition, ASASA, along with other partners, assisted in gathering data from South African respondents in the first ever live patient survey, called the International Map of Axial Spondyloarthritis (IMAS) survey, which is run by the Axial Spondyloarthritis International Federation that surveys people diagnosed with AxSpA and assesses the impact and burden that AxSpA has on the lives of patients, from their perspective.
Van Dam concluded, “There is still a lot we can do in South Africa and ASASA is busy growing its team of volunteers to help to build awareness around AxSpA in the country. We aim to continue to build support structures for patients in the country, as well as continually working with the medical fraternity, assisting with early diagnosis and access to treatment.”
Haemophilia A, the most common severe form of haemophilia, affects almost exclusively males and can usually be with factor VII injections, but not for all sufferers, as the immune system may treat the factor as an intruder. New research has uncovered an important immune mechanism that targets B cells, which is crucial in making the the therapy effective. The study is published online in the Journal of Clinical Investigation.
Haemophilia A patients have a defect in factor VIII, a protein key for clotting. Most patients therefore receive an intravenous injection of the functional clotting factor every few days as treatment. But frequently, and especially at the start of treatment, the immune system recognises the injected agent as foreign to the body and attacks it. This is the most serious complication of haemophilia treatment because factor VIII can then no longer work.
In these cases, immune tolerance therapy, which was also developed at the University Hospital Bonn (UKB) more than 40 years ago, often helps. This involves regularly injecting the haemophilia sufferers with a high dose of factor VIII over several months, letting the immune system learn to tolerate it. The underlying immune mechanisms are unknown. “However, this doesn’t always work,” explains Prof Dr Johannes Oldenburg at the UKB. “In about 30 percent of patients, tolerance induction does not lead to success. So your body’s own defences continue to attack and destroy the factor VIII protein, which means that factor VIII cannot be used for treatment. We wanted to know the reason for this.”
To this end, the team looked at two cell types in the immune system, B cells and regulatory T cells. B cells recognise foreign molecules in the body and produce antibodies against them, which switch off the function of the molecule. For factor VIII, this means that it is no longer effective in haemophilia treatment.
Brake in the immune system
Regulatory T cells moderate the strength and duration of the immune response. The researchers have now found a new type of Treg cell that can act specifically against certain B cells rather than the overall immune response. “We were able to show that immunotolerance therapy results in the generation of regulatory T cells that exclusively induce B cells against factor VIII to commit suicide,” says Dr Janine Becker-Gotot of the Institute of Molecular Medicine and Experimental Immunology (IMMEI) at UKB. “These T cells have a sensor that allows them to recognise and attach to the corresponding B cells. In addition, they have the ability to push the self-destruct button on the surface of B cells.”
This button is a molecule called PD-1 which, on activation, leads to apoptosis. Every active B cell has this button. “Our experiments enabled us for the first time to detect regulatory T cells that can activate this self-destruct button only in very specific B cells, in order to specifically prevent unwanted immune responses,” explains IMMEI Director Prof Dr Christian Kurts.
The more PD-1 buttons the B cells against factor VIII carry on their surface, the easier it is for them to be driven to suicide by immune tolerance therapy. “The amount of PD-1 varies from person to person,” Becker-Gotot explains. “If it’s very low to begin with, there’s a good chance that many inhibitor-producing B cells will survive and continue to neutralise the injected factor VIII.”
Test to show in whom immunotolerance therapy is useful
Interestingly, B cells also produce more PD-1 once they come into contact with regulatory T cells. “We can now test how strong this reaction is,” the researcher says. “If PD-1 levels go up shortly after starting immune tolerance therapy and then stay up, that’s a clear sign that the treatment is going to be successful.” The team is currently developing a blood test that can be used to detect whether or not immune tolerance therapy is working in patients during the prolonged treatment.
“Our findings have great basic scientific value,” explains Prof Kurts. “And not just for haemophilia, but also for other congenital disorders where missing proteins are replaced therapeutically. In the long term, they could also be used to develop new treatments.”
Since 11 October 2022, the National Institute for Communicable Diseases (NICD) seven measles cases have been detected in Greater Sekhukhune District in Limpopo province within 30 days, as of 21 October.
Infected individuals ranged from 9 months to 24 years. One child was fully vaccinated for measles, with two measles doses given in 2019. One child was unvaccinated, and the other five measles cases had unknown vaccination history. One measles case was hospitalised while one other had a complication that led to pneumonia.
District and provincial health officials have started a public health response. This includes enhanced surveillance for measles, contact tracing, screening for suspected cases using a case definition followed by collection of blood and throat swabs for measles diagnostic testing, and reviewing medical records to pick up missed cases. Vaccinations are underway for those exposed to suspected or confirmed cases.
The measles immunisation coverage data for the Greater Sekhukhune district showed a decrease of 87% to 64% for measles dose 1 and 86% to 60% for measles dose 2 from 2017 to 2022. This is below the 95% coverage needed to achieve herd immunity. A survey is being done to validate the vaccination data provided to the province and investigate factors that might be contributing to the measles outbreak. Community awareness and health promotion by healthcare workers is continuing in the district to inform the public about the spread of measles and interventions to prevent disease. Measles vaccination has been initiated for children under 15 years to increase the measles immunity in the community and to prevent further spread of measles.
Clinicians should continue to be on the alert for measles cases, especially in Limpopo Province, as large measles outbreaks are occurring in sub-Saharan Africa, including in neighbouring countries.
Signs and Symptoms
Measles is a highly contagious disease caused by a virus of the paromyxovirus family. Patients with measles present with fever and a rash. The rash looks like small, red, flat spots over the body. The rash does not form blisters, nor is it itchy or painful. Other signs include cough, conjunctivitis and coryza. Complications of measles can include diarrhoea, dehydration, encephalitis, blindness and death. Other measles complications are pneumonia, scarring of the cornea (kerato-conjunctivitis), and rarely encephalitis. Complications are more serious in very young children (under 2 years) or who are malnourished.
Clinicians and caregivers should check children’s road-to-health booklets to ensure measles vaccinations are up to date. Suspected measles cases should be notified on the NMC system. Click here to access the Case Notification form
Researchers in the American Journal of Epidemiology report that wastewater surveillance of diseases that infect humans should work in most cases. But more research is needed to apply the science for public health benefit, the research team concluded.
Led by epidemiologist David Larsen from Syracuse University, the team’s work published examined all peer-reviewed scientific articles of wastewater surveillance published through July 2020. The team identified a variety of pathogens that can be found in wastewater, including almost all infectious diseases that the World Health Organization has classified as a Public Health Emergency of International Concern (PHEIC) such as Ebola virus and Zika virus.
But despite this positive finding, few studies relate what is found in the wastewater to public health and the amount of disease that is circulating.
“Testing the wastewater is only one component of this powerful science,” said Dr Larsen, an associate professor of public health at Syracuse University. “Understanding the results and implications for public health is just as challenging. We need interdisciplinary teams working together to maximise the benefit of wastewater-based epidemiology.”
Wastewater-based epidemiology is the science of taking what is found in wastewater and using that information to understand population-level health trends. Most of the articles reviewed looked at what they could find in the wastewater and omitted the second step of relating the findings to other measures of population-level health, such as numbers of cases, test positivity, or hospitalisations.
Wastewater-based epidemiology of COVID has enjoyed substantial availability of clinical COVID data, and results from wastewater surveillance are more easily understood in terms of COVID transmission. However, the research team determined that more work is needed to be done for other pathogens, including monkeypox and polio, to increase the utility of wastewater surveillance to benefit public health.
Systemic sclerosis, or scleroderma that affects the skin and internal organs, is one of the rarest autoimmune diseases, affecting roughly 100 000 people in the US, mostly women. It has the highest mortality rate among rheumatic diseases.
There are no licensed treatments available for this subset of scleroderma patients, and rheumatology researchers are constantly searching for opportunities to use resources and technology that have proven beneficial in treating other autoimmune and rheumatic diseases.
In a new study published in JCI Insight, researchers found that tofacitinib, a drug approved for rheumatoid arthritis, was well tolerated among patients with early systemic sclerosis, and discovered the drug primarily affected the protein, interferon, both in fibroblasts and keratinocytes cells.
Dinesh Khanna MBBS., MSc, director of the Michigan Medicine Scleroderma Program, explained: “We wanted to understand first, if there was any clinical benefit of tofacitinib to patients, but we were also asking, what are the differences in the cells of healthy skin versus systemic sclerosis cells…how does the drug work?”
The study sample size consisted of 15 patients with early diffuse cutaneous systemic sclerosis — patients with skin hardening and issues with organs. Of the total participants, 10 patients received 5mg of tofacitinib twice a day, and the remaining received placebo in a double-blind randomised placebo-controlled trial.
Over the course of the 24-week trial period, researchers found no patients who exhibited severe adverse effects at or before the trial ended. Measures included the modified Rodnan skin score (mRSS).
These results showed that the average mRSS score and other measures improved over the course of the trial. In addition, patients on placebo went on open label tofacitinib after 24 weeks and there was ongoing improvement during the next 24 weeks, indicating improvement in the measure.
“We are delighted to find that the drug is safe to use and can possibly be repurposed for systemic sclerosis treatment,” said Khanna, “but what made this study innovative was the use of single cell technology.”
Participants in the study had a skin biopsy at the start of the trial and then again six weeks after they received tofacitinib or placebo. Then, clinicians used the relatively new technology — single cell RNA sequencing — to watch the mechanism of tofacitinib at work in the trial participants’ skin cells.
“This work highlights the ability of single-cell RNA-sequencing to determine how disease states are maintained and how various cell populations in the skin, both fibroblasts, skin cells, and immune cells communicate, providing unparallelled power to address disease mechanisms, and how drugs, like tofacitinib, work in a disease where they have not previously been used,” said Johann Gudjonsson MD, PhD, professor of dermatology and a collaborator on this study.
Along with discovering how tofacitinib inhibits fibroblasts and keratinocytes, researchers found that the drug had minimal effect on T cells.
“Because we found that the drug was working on one part (the mechanism of fibroblasts and keratinocytes), we are now considering if we can combine tofacitinib with another drug with complementary mechanism in action, in order to treat early systemic sclerosis without causing toxicity,” explained Khanna.
To understand more about the drug, researchers will need to conduct a more robust study and trial to see if their recent discoveries hold true.
“From this combined effort between Michigan Medicine and University of Pittsburgh, we know that the drug is safe, and we know that the technology (RNA sequencing) is feasible, now we can start to utilise the technology and find out what type of therapies we can mix and match that will add benefit to patients,” Khanna said.
A 3D map of the islets in the human pancreas. Source: Wikimedia
A meta-analysis of molecular studies found a strong link between enterovirus infection and type 1 diabetes. Across 48 abstracts on the topic, people with type 1 diabetes were nearly eight times more likely to have an enterovirus infection than those with normal pancreatic function, according to a presentation at the European Association for the Study of Diabetes (EASD) meeting.
For this review, researchers examined 56 studies using molecular methods to identify enterovirus infection by looking for viral nucleic acid or protein in a human clinical sample.
People with islet autoimmunity were twice as likely to have had an enterovirus infection at any point in time, based on data from 18 studies.
Subgroup analysis of people who were diagnosed with the enterovirus within the past month found 16.22-fold higher odds of recent-onset type 1 diabetes, based upon 28 studies.
“This is very recent onset type 1 diabetes, and that was the highest risk group that we detected,” reported Sonia Isaacs, PhD candidate, of University of New South Wales in Australia, during a press conference.
Looking more closely at other subgroup criteria revealed associations.
First, those who had any islet autoimmunity and eventually progressed to full-blown type 1 diabetes were over five times more likely to have an enterovirus infection than controls; this was a higher risk than those who had islet autoimmunity and never progressed to type 1 diabetes. When it came to timing, only infections at the time of or after islet autoimmunity seroconversion carried higher risk (OR 5.1), whereas the increased risk wasn’t significant for infections prior to seroconversion.
Isaacs noted that those with a familial risk of type 1 diabetes (ie in a first-degree relative) also had a much higher risk for an enterovirus infection (OR 9.8), higher than the subgroup recruited for having a high-risk HLA gene. Those who had the high-risk HLA gene and a familiar risk of type 1 diabetes had 141.1-times higher odds of prior enterovirus infection.
Having several enterovirus infections was also linked with a doubled chance of islet autoimmunity.
Specific type of enterovirus linked to risk of type 1 diabetes included:
Enterovirus A: OR 3.7
Enterovirus B: OR 12.7
Enterovirus C: OR 13.8
“This is where the coxsackieviruses come from,” Isaacs pointed out. “Coxsackievirus B1 and B4 stood out.”
Isaacs suggested the possibility of enterovirus vaccinations and antivirals as a prevention strategy for type 1 diabetes.
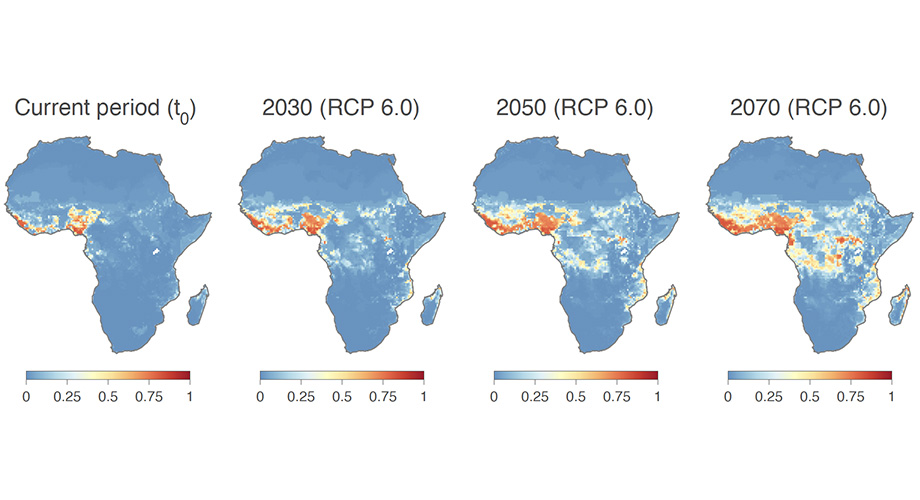
Pictured are projections of the ecological niche suitability for Lassa virus based on climate models and other data. Credit: Scripps Research and University of Brussels
Analysing decades of environmental data associated with Lassa virus outbreaks, researchers projected that areas hospitable to Lassa virus spread may extend from West Africa into Central and East Africa in the next several decades. With this expansion and expected African population growth, the human population living in the areas where the virus should theoretically be able to circulate may rise by more than 600 million.
“Our analysis shows how climate, land use, and population changes in the next 50 years could dramatically increase the risk of Lassa fever in Africa,” says first author Raphaëlle Klitting, PhD, a postdoctoral researcher at Scripps Research during the study, which is published in Nature Communications.
Lassa virus is a zoonotic pathogen found in the Natal multimammate rat (Mastomys natalensis), most likely transmitted to humans via its droppings. While an estimated 80% of infections are mild or asymptomatic, the remaining cases are more severe, with signs and symptoms that can include haemorrhaging from the mouth and gut, hypotension, and potentially permanent hearing loss. Mortality rate in hospitalised patients can be up to 80%.
An estimated several hundred thousand infections occur each year, chiefly in Nigeria and several other West African countries. So far there is no approved vaccine or highly effective drug treatment.
Although the primary animal reservoir for Lassa virus is known, the virus spreads in only a subset of the areas where the animal is found. Thus, it is possible that environmental factors also help determine whether and where significant viral transmission can occur. In the study, the researchers developed an ‘ecological niche’ model of Lassa virus transmission, using environmental data at sites of known spread.
Combining the model with projections of climate and land-use changes in Africa in the next several decades, as well as the known range of the Natal multimammate rat, the researchers estimated the areas of Africa that could support Lassa virus transmission currently, and in the years 2030, 2050, and 2070. The projected current areas corresponded well to known endemic areas in West Africa, but the estimates for future decades suggested a vast expansion within and beyond West Africa.
“We found that several regions will likely become ecologically suitable for virus spread in Central Africa, including in Cameroon and the Democratic Republic of the Congo, and even in East Africa, in Uganda,” Klitting said.
Currently Africa’s population is undergoing rapid growth; the researchers therefore considered projections of this population growth for the areas of current and potential future Lassa virus circulation. They found that the number of people potentially exposed to the virus could increase from about 92 million today to 453 million by 2050, and 700 million by 2070 – an increase of over 600%.
More hopefully, the researchers examined the dynamics of the spread of Lassa virus using data on sequenced viral genomes sampled at various locations in West Africa and found that virus dispersal appeared to be slow. They concluded that, unless transmission dynamics change drastically in the new location where the virus circulates, the virus’s spread into new ecologically suitable areas in the coming decades may also be slow.
The authors say that the findings should inform African public health policies, for example, by encouraging officials to add Lassa virus to lists of viruses under epidemiologic surveillance in parts of Central and East Africa.
“With the ongoing climate change and increasing impact of human activities on the environment, further comprehensive studies of the ecology and spread of zoonotic and vector-borne diseases are needed to anticipate possible future changes in their distribution as well as their impact on public health,” said senior author Simon Dellicour, PhD, of the University of Brussels.
Scanning electron micrograph of Lassa virus budding off a Vero cell. Image credit: National Institute of Allergy and Infectious Diseases, NIH
Scientists have found that viruses lurking inside cells may be on the ‘watch’ for information from their environment to choose when to multiply and burst out. The work, published in Frontiers in Microbiology, has implications for antiviral drug development.
A virus’s ability to sense its environment, including elements produced by its host, adds “another layer of complexity to the viral-host interaction,” said senior author Ivan Erill, professor of biological sciences. Currently, viruses use that ability to their benefit. But in the future, he says, “we could exploit it to their detriment.”
Not a coincidence
The new study focused on bacteriophages, viruses which infect bacteria – also known as ‘phages.’ The phages in the study can only infect their hosts when the bacterial cells have special appendages, called pili and flagella, that help the bacteria move and mate. The bacteria produce a protein called CtrA that controls when they generate these appendages. The new paper shows that many appendage-dependent phages have patterns in their DNA where the CtrA protein can attach, called binding sites. A phage having a binding site for a protein produced by its host is unusual, explained Prof Erill.
Even more surprising, Erill and the paper’s first author Elia Mascolo, a PhD student in Erill’s lab, found through detailed genomic analysis that these binding sites were not unique to a single phage, or even a single group of phages. Many different types of phages had CtrA binding sites – but they all needed their hosts to have pili and/or flagella to infect them. It couldn’t be a coincidence, they decided.
The ability to monitor CtrA levels “has been invented multiple times throughout evolution by different phages that infect different bacteria,” Prof Erill said. This convergent evolution indicates that the trait is useful.
Timing is everything
Another wrinkle in the story: The first phage in which the research team identified CtrA binding sites infects a particular group of bacteria called Caulobacterales. Caulobacterales are an especially well-studied group of bacteria, because they exist in two forms: a free-swimming ‘swarmer’ form which has pili/flagella, and a ‘stalked’ form that attaches to a surface and lacks those appendages. In these bacteria, CtrA also regulates the cell cycle, determining whether a cell will divide evenly into two more of the same cell type, or divide asymmetrically to produce one swarmer and one stalk cell.
Because the phages can only infect swarmer cells, it’s in their best interest only to burst out of their host when there are many swarmer cells available to infect. Generally, Caulobacterales live in nutrient-poor environments, and they are very spread out. “But when they find a good pocket of microhabitat, they become stalked cells and proliferate,” Prof Erill said, eventually producing large quantities of swarmer cells.
“We hypothesise the phages are monitoring CtrA levels, which go up and down during the life cycle of the cells, to figure out when the swarmer cell is becoming a stalk cell and becoming a factory of swarmers,” Prof Erill said, “and at that point, they burst the cell, because there are going to be many swarmers nearby to infect.”
Listening in
Unfortunately, the method to prove this hypothesis is labour-intensive and extremely difficult, so that wasn’t part of this latest paper — although Erill and colleagues hope to tackle that question in the future. However, the research team sees no other plausible explanation for the proliferation of CtrA binding sites on so many different phages, all of which require pili/flagella to infect their hosts. Even more interesting, they note, are the implications for viruses that infect humans.
“Everything that we know about phages, every single evolutionary strategy they have developed, has been shown to translate to viruses that infect plants and animals,” he said. “It’s almost a given. So if phages are listening in on their hosts, the viruses that affect humans are bound to be doing the same.”
There are a few other documented examples of phages monitoring their environment in interesting ways, but none include so many different phages employing the same strategy against so many bacterial hosts.
Prof Erill predicts that more examples of this will be found, and his lab is already discovering more.
New therapeutic avenues
The key takeaway from this research is that “the virus is using cellular intel to make decisions,” Erill says, “and if it’s happening in bacteria, it’s almost certainly happening in plants and animals, because if it’s an evolutionary strategy that makes sense, evolution will discover it and exploit it.”
For example, to optimize its strategy for survival and replication, an animal virus might want to know what kind of tissue it is in, or how robust the host’s immune response is to its infection. While it might be unsettling to think about all the information viruses could gather and possibly use to make us sicker, these discoveries also open up avenues for new therapies.
“If you are developing an antiviral drug, and you know the virus is listening in on a particular signal, then maybe you can fool the virus,” Erill said. “We are just starting to realise how actively viruses have eyes on us – how they are monitoring what’s going on around them and making decisions based on that. “It’s fascinating.”
People who wear reusable contact lenses are nearly four times as likely as those wearing daily disposables to develop a rare sight-threatening eye infection, Acanthamoeba keratitis (AK), according to new research. The study, published in Ophthalmology, identifies multiple factors that increase the risk of AK, including reusing lenses or wearing them overnight or in the shower.
AK is a type of microbial keratitis – a condition that results in inflammation of the cornea.
Eye infection from Acanthamoeba. Credit: CDC
Lead author, Professor John Dart (UCL Institute of Ophthalmology and Moorfields Eye Hospital NHS Foundation Trust) said: “In recent years we have seen an increase of Acanthamoeba keratitis in the UK and Europe, and while the infection is still rare, it is preventable and warrants a public health response.
“Contact lenses are generally very safe but are associated with a small risk of microbial keratitis, most commonly caused by bacteria, and which is the only sight threatening complication of their use. Given that an estimated 300 million people across the globe wear contact lenses, it is important that people know how to minimise their risks for developing keratitis.”
Contact lens use is now the leading cause of microbial keratitis in patients with otherwise healthy eyes in countries in the global north. While sight loss resulting from microbial keratitis is uncommon, Acanthamoeba, is one of the most severe causes and is responsible for about half of those contact lens users who develop sight loss after keratitis. Avoidable risks are associated with 90% of AK cases. The infection remains rare, affecting fewer than 1 in 20 000 contact lens wearers per year in the UK.
In AK, ,infection by Acanthamoeba, a cyst-forming microorganism, causes the cornea to become painful and inflamed. The most severely affected patients (a quarter of the total) end up with less than 25% of vision or become blind following the disease and face prolonged treatment. Overall, 25% of people affected require corneal transplants to treat the disease or restore vision.
For the study, the researchers recruited over 200 patients of Moorfields Eye Hospital who completed a survey, including 83 people with AK, and compared them with 122 participants who came to eyecare clinics with other conditions, who acted as a control group.
People who wore reusable soft contact lenses (such as monthlies) had 3.8 times the odds of developing AK, compared to people who wore daily disposable lenses. Showering with lenses increased AK risk by 3.3 times, while wearing lenses overnight increased risk by 3.9 times. Among daily disposable wearers, reusing their lenses increased their infection risk. Having had a recent contact lens check with a health professional reduced the risk.
With further analysis, the researchers estimated that 362% of cases in the UK, and potentially in many other countries, could be prevented if people switched from reusable to daily disposable lenses.
A recent study led by Prof Dart found that AK is increasing in prevalence in the UK. By reviewing incidence data from Moorfields Eye Hospital from 1985 to 2016, he and his team found an increase starting in 2000–2003, when there were eight to 10 cases per year, to between 36 and 65 annual cases at the end of the study period.
First author, Associate Professor Nicole Carnt (UNSW, Sydney, UCL Institute of Ophthalmology and Moorfields Eye Hospital) said: “Previous studies have linked AK to wearing contact lenses in hot tubs, swimming pools or lakes, and here we have added showers to that list, underlining that exposure to any water when wearing lenses should be avoided. Public pools and coastal authorities could help reduce this risk by advising against swimming in contact lenses.”
Prof Dart added: “Contact lens packaging should include information on lens safety and risk avoidance, even as simple as ‘no water’ stickers on each case, particularly given that many people buy their lenses online without speaking to a health professional.
“Basic contact lens hygiene measures can go a long way in avoiding infections, such as by thoroughly washing and drying your hands before putting in your lenses.”
Huge clumps of E. coli (red) infecting diabetic mouse bladder. Photo: Soumitra Mohanty
Lower immunity and recurring infections are common in type 1 and type 2 diabetes. Research has shown that the immune system of people with diabetes has lower levels of the antimicrobial peptide psoriasin, which compromises the urinary bladder’s cell barrier, increasing the risk of urinary tract infection. The study is published in Nature Communications.
One effect of diabetes is that it compromises the innate immune system, leaving many people with increased susceptibility to regular infections, such as urinary tract infections (UTI)s caused by E. coli bacteria. In people with diabetes, these are more likely to lead to general blood poisoning, sepsis, originating in the urinary tract.
An endogenous antibiotic
Karolinska Institutet researchers investigated whether glucose levels in people with diabetes (type 1, type 2, or prediabetes) are linked with psoriasin, an endogenous antibiotic which is a part of the innate immune system.
Using samples of urine, bladder cells and blood serum from patients, the researchers analysed levels of psoriasin and other peptides necessary for ensuring that the bladder mucosa remains intact and protects against infection. The findings were then verified in mice and urinary bladder cells with and without infection.
“We found that high glucose concentrations reduce the levels of the antimicrobial peptide psoriasin, while insulin has no effect,” said Professor Annelie Brauner, who led the study. “People with diabetes have lower levels of psoriasin, which weakens the cells’ protective barrier function and increases the risk of bladder infection.”
Oestrogen therapy reduced bacterial population
Professor Brauner’s research group has previously shown that oestrogen restores the protective function of bladder cells in humans and mice and thereby help to regulate the immune response to a UTI. The researchers therefore tested how oestrogen treatment affects infected cells exposed to high glucose concentrations. They found that the treatment boosted levels of psoriasin and reduced bacterial populations, indicating that the treatment may have an effect also among patients with diabetes.
“We now plan to probe deeper into the underlying mechanisms of infections in individuals with diabetes,” said lead author Soumitra Mohanty. “The ultimate goal is to reduce the risk of infection in this growing patient group.”