New Northwestern Medicine study provides answers and drug targets
Photo by Natanael Melchor on Unsplash
More than 50% of lung-transplant recipients experience a rejection of their new lung within five years of receiving it, yet the reason why this is such a prevalent complication has remained a medical mystery.
Now, a new Northwestern Medicine study has found that, following transplant and in chronic disease states, abnormal cells emerge and “conversations” between them drives the development of lung damage and transplant rejection.
These findings not only help answer why rejection occurs, but they also have spurred immediate exploration of new drugs to treat transplant rejection and other lung-scarring diseases.
“Chronic lung-transplant rejection has been a ‘black box.’ We knew it happened but did not exactly know why,” said corresponding author Dr Ankit Bharat, professor of thoracic surgery at Northwestern University Feinberg School of Medicine and executive director of the Northwestern Medicine Canning Thoracic Institute. “Our study provides the first comprehensive cellular and molecular roadmap of the disease.”
The study was published in JCI Insight.
Leading cause of death after the first year of transplantation
Surgeons perform approximately 3000 to 3500 lung transplants each year in the U.S., and more than 69 000 have been performed worldwide to date. Chronic lung allograft dysfunction (CLAD), which encompasses several manifestations of chronic lung rejection, remains the leading cause of death after the first year of transplantation. There currently are no effective treatments for CLAD once it develops, leaving patients with only one option: re-transplantation.
In the new study, after evaluating almost 1.6 million cells, scientists distinguished between abnormal cells from the donor lung versus cells from the recipient’s own immune system. They discovered the donor-derived structural cells and recipient’s immune cells talk to each other in harmful ways that perpetuate lung damage. The findings could lead to new drug targets and provide insights that could help patients with various lung-scarring diseases, not just transplant recipients.
Comparing rejection to other scarring lung diseases
The scientists discovered a rogue cell type (KRT17 and KRT5 cells) that drives lung scarring across multiple diseases, including idiopathic pulmonary fibrosis, interstitial lung disease, COPD, COVID-19 lung damage and transplant rejection. By integrating data from this array of scarring lung diseases, the scientists created the first comprehensive reference map showing which molecular features are shared across conditions and which are unique to each disease.
“By comparing chronic rejection to other scarring lung diseases, we identified both shared and unique features,” said Bharat, who also is a member of the Robert H. Lurie Comprehensive Cancer Center of Northwestern University. “This means treatments developed for one condition might help others. The benefits extend far beyond transplant patients.”
The scientists also identified previously unrecognised cell populations in rejected lungs. These include “exhausted” T cells that remain activated but dysfunctional, and “super-activated” macrophages that promote inflammation and scarring.
Lastly, the scientists developed new computational methods to analyse data from multiple studies together, overcoming technical barriers that previously prevented this kind of comprehensive analysis, Bharat said.
New drug targets identified
The scientists pinpointed specific genes and signaling pathways (like PDGF, GDF15 and TWEAK) that drive scarring, which allows them to identify potential targets for new drugs, Bharat said. Some existing medications, such as nintedanib, and pirfenidone, which are approved (in the US) for other lung diseases, might be repurposed for transplant rejection, he said.
“The findings have immediate translational potential,” Bharat said. “We’re already exploring therapeutic strategies based on these discoveries.”
Broad impact on pulmonary fibrosis
While addressing CLAD was the main focus of the paper, this research has major implications for understanding and treating all forms of pulmonary fibrosis, Bharat said.
“The molecular pathways and cell types we identified are relevant to conditions affecting hundreds of thousands of patients with various lung-scarring diseases, not just transplant recipients,” Bharat said. “This work essentially provides a ‘Rosetta Stone’ for understanding lung scarring regardless of the initial trigger.”
Cancer is one of the fastest-growing health challenges in South Africa, with over 100 000 new cases diagnosed annually, according to the National Cancer Registry. While most conversations focus on the physical and emotional impact, the financial strain of the disease often goes unspoken.
According to the South African Medical Journal, treatment costs for cancer can exceed R1 million per year, particularly when advanced therapies and prolonged care are required. This leaves many families facing difficult decisions that extend far beyond the hospital ward. With medical aid often falling short and with only 16% of South Africans covered by medical schemes, as reported by the Council for Medical Schemes the financial burden of cancer can be as devastating as the diagnosis itself.
“Medical aid alone often isn’t enough to cover the full cost of treatment, especially when it comes to critical illnesses like cancer,” says Matthew Green, Product Portfolio Manager at FNB Life. “We’ve seen firsthand how having the right insurance can make a real difference.”
The true impact of cancer is often measured in rands and cents: savings depleted, debt accumulated, and households forced to sacrifice essentials to pay for treatment. Myths about affordability and a lack of awareness mean that too many people enter this battle unprepared. The result is a financial shock that can be as devastating as the diagnosis itself. Beyond the direct medical expenses, families often face a range of additional costs from transport to and from treatment centres, specialised nutrition, home modifications, and caregiving support, to lost income due to time off work. Critical illness cover is designed to help bridge these financial gaps, providing a lump-sum payout that can be used not only for treatment, but also for these broader, often overlooked expenses that impact the entire household.
“Against this backdrop, insurers are under growing pressure to offer support that reflects the lived realities of ordinary South Africans. FNB Insure is among those stepping in to help close the gap – focusing on making financial protection more accessible, flexible, and relevant to everyday needs,” says Green.
Rather than positioning insurance cover as a luxury, the emphasis is on practical tools that help households navigate the rising costs of treatment and the economic strain that often follows a serious diagnosis. Whether it’s support during hospital stays, assistance with unexpected medical shortfalls, or a payout that enables immediate action after a diagnosis, the goal is to empower customers to focus on recovery – not financial survival.
This is evident from our customer feedback, where individuals have shared how timely access to cover helped them act quickly, avoid financial delays, and prioritise their health during some of life’s most difficult moments. “And its stories like this underline the importance of early financial planning and the role of accessible insurance in giving families space to focus on recovery rather than financial survival,” says Green.
With October marking Breast Cancer Awareness Month and November bringing the spotlight on men’s health through initiatives like Movember, FNB Insure is adding its voice to the broader call for awareness. “The message is clear: cancer doesn’t only affect health; it reshapes every aspect of life. Building resilience means preparing not just medically, but financially too,” concludes Green.
Research reveals Alzheimer’s disease-like DNA damage, hints at immune involvement
Photo by Hermes Rivera on Unsplash
Chronic traumatic encephalopathy (CTE), a neurodegenerative disease diagnosed after death, most often athletes of contact sports and military personnel, is not just caused by repeated head impact but also linked to DNA damage similar to that seen in Alzheimer’s disease, according to a new study led by researchers at Harvard Medical School, Boston Children’s Hospital, Mass General Brigham, and Boston University.
CTE is known to share characteristics with Alzheimer’s disease, namely the buildup of abnormal tau protein in the brain. CTE has also been associated with the development of dementia. The new research, published October 30 in Science, highlights the commonalities between CTE and Alzheimer’s at the genetic level and raises hopes that future treatments could target both diseases.
The findings also support recent work from study co-authors Jonathan Cherry and Ann McKee at Boston University in suggesting that immune system responses could help explain why only some people with repeated head impact go on to develop CTE.
“Our results suggest that CTE develops through some process in addition to head trauma,” said co-senior author Christopher A. Walsh, Professor of Pediatrics and Neurology and chief of the Division of Genetics and Genomics at Boston Children’s. “We suspect it involves immune activation in a way similar to Alzheimer’s disease, happening years after trauma.”
A new approach to studying CTE
The team used two types of single-cell genomic sequencing to identify somatic genetic mutations – non-inherited changes in DNA. This marked the first time scientists took such an approach to studying CTE.
Studying postmortem brain tissue samples, the researchers analysed hundreds of neurons from the prefrontal cortex of 15 individuals diagnosed with CTE after death and 4 individuals with repeated head impact but without CTE and compared them with 19 neurotypical controls and 7 individuals with Alzheimer’s.
The team found that neurons from individuals with postmortem CTE diagnoses had specific abnormal patterns of somatic genome damage that closely resemble those seen in Alzheimer’s. Individuals displaying signs of repeated head impact without postmortem CTE diagnoses didn’t have these changes.
“One of the most significant aspects of our work is the introduction of a new, single-cell genome approach to CTE,” said co-senior author Michael Miller, HMS assistant professor of pathology at Brigham and Women’s Hospital. “Our study provides further evidence that CTE is a bona fide neurodegenerative disease defined by its unique neuropathological features.”
The researchers also observed that the CTE brain samples showed signs of damage equivalent to more than 100 years of excess aging.
Clues to CTE’s origins
Repeated head impact most often occurs during contact sports such as American football, hockey, and rugby or during military service. CTE has been found postmortem in the brains of teenagers and young adults playing amateur sports as well as in older professional athletes.
Recent research in Nature from Cherry and McKee found that repeated head impact causes brain damage in young people even before tau deposition or symptoms indicative of CTE arise. That study also indicated that repeated head trauma induces immune activation in athletes’ brains, said Walsh, who is also an investigator of the Howard Hughes Medical Institute.
The October 30 paper adds to this growing evidence base by linking CTE with Alzheimer’s, which involves inflammation in microglial cells in the brain, despite the diseases’ differing risk factors, Walsh said.
The NHI Act is facing a slew of legal challenges from multiple organisations. For this special series, Spotlight combed through court papers, and spoke with legal experts to pin down what specific arguments litigants are betting on. In part one, we focused on the claim that the scheme is unaffordable and therefore unreasonable. Here, in part two, we discuss the argument that the NHI will unjustifiably compromise people’s right to access healthcare services.
Since the National Health Insurance (NHI) Act was signed into law by President Cyril Ramaphosa in May 2024, eight different groups have challenged it in court, with some filing multiple applications.
One core argument which appears in different ways across many of these submissions is that under the NHI, people will have access to fewer health services, or simply a reduced quality of care, than what they currently have.
If this was true then the NHI could be in violation of Section 27 of the country’s Constitution, according to which government has to do what it can to achieve the “progressive realisation” of the right to healthcare services (along with the right to food, water and social security). Courts have often interpreted this to mean that the government not only has to take active steps to advance people’s access to healthcare, but also that it should avoid doing things that might limit their existing rights.
Sasha Stevenson, who heads the public interest law clinic SECTION27, explained that the Constitution uses the phrase “progressive realisation” because of a “recognition that not everything can be perfect straight away, so the government needs to take steps to move toward full realisation of certain socioeconomic rights”. She added: “What that means logically is that you can’t move backwards.”
There is however some wiggle room, said Stevenson. This is because the Constitution only expects the government to take “reasonable” steps that are “within its available resources”, she said.
Thus, if the government was cash-strapped and able to show that it simply couldn’t afford to maintain its current levels of health expenditure without seriously compromising other core rights, then it may be able to take steps backward without violating the Constitution. Stevenson argued that, at its core, the key idea is simply that the state must fully justify what it is doing.
To show that the NHI Act violates Section 27 of the Constitution, litigants will need to prove that it not only limits people’s right to healthcare, but that the government hasn’t provided good enough reasons for why it is doing this.
But why are litigants arguing that the NHI would limit people’s right to healthcare in the first place? Let’s start with medical scheme members.
Cutting out medical schemes
Section 33 of the NHI Act states that once the scheme is fully implemented, medical schemes will only be allowed to cover top-up health services that aren’t covered by the NHI. In addition, the Act requires “mandatory prepayment”, meaning people will have to pay to be covered by the NHI, whether or not they want to join.
Thus, unless someone was able to afford both the mandatory prepayment for the NHI, and complimentary cover from their medical schemes, they would have to switch to relying solely on the NHI for their medical coverage.
This is an issue for the Board of Healthcare Funders (BHF), which represents the medical insurance industry, and was one of the first groups to challenge the NHI in court.
“When you look at what medical scheme members are entitled to now versus to what they’re entitled to under an NHI scheme, it’s a regressive process,” Neil Kirby, who heads the healthcare and life science practice area at Werksmans Attorneys, which represents BHF, told Spotlight.
“You probably would be entitled to less under an NHI scheme than you would under the current regime,” he said.
Of course, at present we don’t yet know exactly what health services the NHI will cover, as the package of benefits has not yet been detailed. It thus may be difficult for courts to assess this claim.
When asked about this, Kirby said: “The current assessment by various economic experts is that if one were to price the value of the current basket of prescribed minimum benefits [the services which medical schemes have to cover]… and spread that cost over the entire population covered by NHI, the NHI would be entirely unaffordable.”
As a result, he said: “There would have to be some degree of compromise in respect of the benefits to be provided under NHI in order for the state to afford to purchase those benefits”. In other words, they’d need to offer less than what medical schemes currently cover.
In response to this, the National Health Department’s NHI lead, Dr Nicholas Crisp, denied that people’s coverage would be compromised under the NHI. In a conversation with Spotlight, he argued that the NHI would not need to incur the same total payment obligations as medical schemes in order to cover a comprehensive package of health services. This is given that it could purchase services more efficiently, he said.
ANC President Cyril Ramaphosa, with Minister of Health, Dr Joe Phaahla and his deputy Dr Sibongiseni Dhlomo, during the signing into law of the National Health Insurance Bill. (Photo: @MYANC/Twitter)
Crisp justified this on several grounds. One is that private health providers are currently accused of overservicing clients, which he argues could be rectified under the NHI.
For instance, Crisp pointed to the Competition Commission’s Health Market Inquiry report, which found that private health facilities are reimbursed for each consultation, operation or other service that they provide. The report found that this “creates an incentive for providers to over-service patients, to over-invest in generously remunerated services, and under-invest in poorly remunerated services [even if they have a positive impact on patient outcomes]”.
Under the NHI scheme, a different reimbursement model would be used to cover health providers both at private and public health facilities. For instance, in the primary healthcare sector, the NHI would rely on capitation. This means that health providers would be provided a fixed fee for each patient, rather than for each individual service, removing the incentive to overservice, and thus overcharge.
Crisp also argued that the government is able to procure medicines and other health services at lower prices than the private sector partly by buying in bulk. Additionally, he noted that billions of rands are reportedly lost in fraud, waste and abuse within the private health sector, due for instance to fraudulent medical claims.
According to Crisp, the NHI fund would be able to save on all of these unnecessary costs.
Pushing back on this view, Professor Alex van den Heever, from the Wits school of governance, told Spotlight that there was no reason to think the state could purchase cover more efficiently than the private medical schemes.
In the public sector, he said that “whether you have a [national] monopoly like Eskom, or a public monopoly in a province like the Gauteng Department of Health, they hardly spend their money efficiently”. Van den Heever added: “For Tembisa hospital to lose R2 billion and not get a cent back in terms of actual products is an indication of the risk.”
He was referring to a damning report by the Special Investigating Unit which confirmed large-scale looting to the tune of around R2 billion meant for patient care at Tembisa Hospital in Gauteng’s East Rand. Their investigation zoomed in on nine criminal syndicates, with three of them pocketing nearly R1.7 billion. The SIU found that R122 million in kickbacks were paid to at least 15 current and former health department officials.
“So you have to have some real evidence that [the state would] be able to procure services more efficiently, and there’s no evidence. All the historical evidence suggests they’d do worse,” Van den Heever said.
Does the state have good reasons?
If litigants are able to show that the NHI was regressive for people on medical schemes in the sense that it diminished their rights, the courts might still decide that the government had provided a good enough justification for why these limitations are reasonable.
But according to Van den Heever, the government has thus far categorically failed to do this.
“From the green paper to the white paper to the [NHI] bill, there is not a single technical document that provides a clear rationale for Section 33 [the restriction on medical schemes],” said Van den Heever. Overall, the very question about what specific problems the NHI is trying to solve and how it would do this remain elusive.
He added that one public health professor had submitted court papers in support of NHI which argued that the existence of the private health sector undermines the public sector, for instance by hoarding doctors and specialists. Yet according to Van den Heever, “no technical report has ever been produced” which provides evidence for that claim.
Additionally, he noted that doctor shortages at public facilities are evidently not driven by private sector hoarding but by financial constraints emanating from mismanagement and corruption. This prevents public hospitals from hiring people who are available for work. (Previous Spotlight reporting has also suggested that the shortage of doctors in the public sector is driven by a lack of funding, rather than a lack of doctors.)
Similarly, the Hospital Association of South Africa (HASA) argued in court papers that the NHI Act’s restrictions on medical schemes serves “no rational, reasonable or economic purpose”.
The association also argued that there are no examples of health systems that impose these restrictions, aside from a few provinces in Canada, and thus Section 33 of the NHI Act is clearly “not a requirement for a successful national health system aimed at [universal health coverage]”.
Defending the restriction on medical schemes, Crisp said that if two different streams of health financing are allowed to continue, then so will inequity. He also stated that single-payer health systems funded by the state are not unusual, even if their exact form differs across countries.
Limiting the rights of public sector users
In addition to the arguments that the NHI Act will unjustly restrict the rights of medical scheme members, some have also argued that it will be regressive for public sector users.
One organisation making this argument is the Treatment Action Campaign (TAC). It has applied to be a friend of the court in the dispute between the South African Medical Association (SAMA) and the government. The TAC argued that the governance provisions within the NHI are so weak that they threaten the entire health system, including for those relying on government health facilities.
Stevenson, whose organisation SECTION27 is represents the TAC, said that checks and balances within the governance of the NHI fund are deficient, leaving it vulnerable to corruption and mismanagement.
Van den Heever, who is serving as an expert in the SAMA case, seconded this concern. He also said that the NHI ultimately centralises the management and purchasing of healthcare services under national institutions. This introduces inefficiencies that will compromise patient care at government facilities, he argued.
“Healthcare is [a sector] where the purchasing and management [should be] decentralised,” he said, largely because different communities have different health needs.
Even in the United Kingdom, said Van den Heever, the responsibility for the National Health Service, which provides the majority of medical services, is devolved across England, Wales, Scotland and northern Ireland, with semi-autonomous trusts, boards and hospitals in each country having a major say in operational decisions.
Van den Heever argued that not only would the centralisation of health under NHI be highly undesirable, but the actual transition to this system from one in which provinces are responsible for healthcare would be enormously disruptive, impacting patient care.
Asylum seekers compromised by NHI
An additional argument concerns the rights of asylum seekers and undocumented people, a central concern for SAMA and the TAC.
Stevenson explained that under our current system, all people, including asylum seekers and undocumented migrants, have the right to free primary healthcare services in the public sector. Just like ordinary citizens, asylum seekers also have the right to access public hospitals on a means-tested basis (meaning your level of subsidisation is determined by what you can afford).
In addition, pregnant and lactating women, as well as children under six, are entitled to all services regardless of documentation status, and the government is compelled to screen, test and treat anyone with HIV.
Under the NHI Act, all of these rights are compromised for asylum seekers and undocumented migrants. This is because Section 4 of the NHI Act states that these groups are only covered for emergency care and for services related to notifiable conditions. The country’s list of notifiable conditions includes diseases like cholera and pulmonary TB, but excludes HIV, diabetes and many other common diseases.
Stevenson argued that this not only compromises the rights of individual asylum seekers, but makes for terrible public health policy.
“It essentially means dropping part of our population off the HIV programme,” she said.
“It would also mean we’re waiting more and more for emergencies, because people can access care [at the point of emergency] but not at a primary healthcare level. So you can’t go and get yourself checked for diabetes… But when your foot is gangrenous [a symptom of untreated diabetes] and needs amputation then you’re in an emergency situation.”
Overall, the Act in its current form constitutes a clear regression for asylum seekers, said Stevenson, and the government has provided no comprehensive justification for why it is excluding this group. If the government wanted to justify the exclusion of migrants on the basis that it is too costly to cover them under the NHI then they “have to show the numbers”, Stevenson said.
Thus far, they haven’t done so.
“There has been no assessment of the so-called burden of migrants in the health sector, let alone how many people fit into which category or how much money is spent on services for people,” said Stevenson, “Instead, there has just been this persistent scapegoating, and these broad statements about the burden.”
Court documents submitted by SAMA have made similar allegations.
“There is no reliable study which shows the extension of the NHI to foreigners will have a significant effect on the affordability of the NHI,” it argued, noting that in fact the converse may be true, as the contributions of foreigners to the economy may outweigh the costs of providing them healthcare.
Asked about this, Crisp said that they were aware of the issue, and that while it was a complicated matter, the state would ultimately have to ensure healthcare for all people, in line with its domestic laws and international agreements.
Disclosure: SECTION27 is mentioned in this article. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council and subject to the South African Press Code.
An international panel of leading experts on women’s mental health is recommending that postpartum psychosis be recognised as a distinct category of mental illness and classified accordingly within standardised medical coding systems.
The recommendation, published in Biological Psychiatry, follows a comprehensive review of the scientific literature on the illness.
Postpartum psychosis is an acute and severe psychiatric illness that sets in within weeks after delivery. Most women with postpartum psychosis experience severe mood symptoms, including mania, mixed episodes, or depression with psychotic features. Impaired cognition, irritability, and agitation are also common.
The condition is considered a psychiatric emergency and, in most cases, requires hospitalisation of the mother. If left untreated, postpartum psychosis is associated with high risks of suicide and infanticide. However, if it is detected and treated in time, patients respond well to treatment and most women return to their previous functioning.
Despite being one of the most distinct clinical phenotypes in psychiatry, postpartum psychosis is not recognized in the Diagnostic and Statistical Manual (DSM-5) or the International Classification of Disease (ICD), which are used to code diseases and medical conditions for treatment and billing purposes.
The panel, in close collaboration with patient advocacy organisations and key interested partners, recommended classifying postpartum psychosis as a distinct category within the bipolar disorders chapter of the DSM and ICD.
“Postpartum psychosis is the most severe perinatal mental health problem, and yet one that is often misdiagnosed and mismanaged, with severe consequences for women, and their children and families. A proper nosological classification of this disorder is an essential step towards its correct identification and treatment”.Professor Paola Dazzan, Professor of Neurobiology of Psychosis, Vice Dean (International) at King’s IoPPN and a member of the research panel
Due to the risks to the patient and the infant, the rapid escalation of severity, and its severe and sudden course, it is imperative that postpartum psychosis is recognized, diagnosed, and treated as early as possible. To facilitate such care, the panel recommends DSM-5 and ICD-10 include the following criteria for a diagnosis of postpartum psychosis:
The onset of at least one of the following states within 12 weeks of childbirth, lasting at least one week and present most of the day, nearly every day, or any duration if hospitalisation is necessary:
Mania/mixed state
Delusions
Hallucinations
Disorganised speech or formal thought disorder
Disorganised, confusional, or catatonic behaviour
Depression with psychotic features
The episode is associated with an unequivocal change in functioning that is uncharacteristic of the postpartum period.
The disturbance in mood and the change in functioning are observable by others.
The episode is sufficiently severe enough to cause marked impairment in social functioning and in the care of the baby or to necessitate hospitalization to prevent harm to the patient, baby, or others.
“We have been working with the American Psychiatric Association and the DSM steering committee since 2020 to find a solution that will facilitate diagnostic accuracy and the provision of timely and evidence-based treatment to improve the quality of treatment and outcomes for women with postpartum psychosis and to prevent the tragic outcomes of suicide and infanticide. We are committed to continue this work,” concludes Dr Veerle Bergink, Director of the Women’s Mental Health Center at Mount Sinai and first author of the paper.
Imagine knowing in your 20s or 30s that you carry a gene which will cause your mind and body to slowly unravel. Huntington’s disease is inherited, relentless and fatal, and there is no cure. Families live with the certainty of decline stretching across generations.
Now, a new treatment is being widely reported as a breakthrough.
Last week, gene therapy company uniQure announced that a one-time brain infusion appeared to slow the disease in a small clinical study.
If confirmed, this would not only be a landmark for Huntington’s disease but potentially the first time a gene therapy has shown promise in any adult-onset neurodegenerative disorder.
But the results, which were announced in a press release, are early, unreviewed and based on external comparisons. So, while these findings offer families hope after decades of failure, we need to remain cautious.
Symptoms usually start in mid-life. They include involuntary movements, depression, irritability and progressive decline in thinking and memory. People lose the ability to work, manage money, live independently and eventually care for themselves. Most die ten to 20 years after onset.
The disease is caused by an expanded stretch of certain DNA repeats (CAG) in the huntingtin gene. The number of repeats strongly influences when symptoms begin, with longer expansions usually linked to earlier onset.
Looking for a treatment
The gene that causes Huntington’s disease was identified in 1993, 32 years ago. Soon afterwards, mouse studies showed that switching off the mutant huntingtin protein even after symptoms had begun could reverse signs and improve behaviour.
This suggested lowering the toxic protein might slow or even partly reverse the disease. Yet for three decades, every attempt to develop a therapy for people has failed to show convincing clinical benefit. Trials of huntingtin-lowering drugs and other approaches did not slow progression.
What is the new treatment?
The one-time gene therapy, called AMT-130, involves brain surgery guided by MRI. Surgeons infuse an engineered virus directly into the caudate and putamen brain regions, which are heavily affected in Huntington’s.
The virus carries a short genetic “microRNA” designed to reduce production of the affected huntingtin protein.
By delivering it straight into the brain, the treatment bypasses the blood–brain barrier. This natural wall usually prevents medicines from entering the central nervous system. That barrier helps explain why so many brain-targeted drugs have failed.
What did they find?
Some 29 patients received treatment, with 12 in each group (one low-dose, and one high-dose) followed for three years. According to uniQure, those given the higher dose declined much slower than expected.
The study compared how much participants’ movement, thinking and daily function declined, compared to a matched external group from a global Huntington’s registry (meaning they weren’t part of the study). The company claimed those given the higher dose had a 75% slowing in their decline.
On a functional scale focused on independence, the company reported a 60% slowing in decline for the higher dose group.
Other tests of movement and thinking also favoured treatment. Nerve-cell damage in spinal fluid was lower for study participants than would be expected for untreated patients.
Why should we be cautious?
These findings are an early snapshot of results reported by the company, not yet peer-reviewed. The study compared treated patients to an external matched control group, not people randomised to placebo at the same time. This design can introduce bias. The numbers are also small – only 12 patients at the three-year mark – so we can’t draw solid conclusions.
The company reports the therapy was generally well tolerated, with no new serious adverse events related to the drug since late 2022. Most problems were related to the neurosurgical infusion itself, and resolved. But in a disease that already causes such severe symptoms, it is often hard to know what counts as a side effect.
The company uniQure has said it plans to seek regulatory approval in 2026 on the basis of this dataset.
Regulators will face difficult decisions: whether to allow access sooner before all the questions and uncertainties are addressed – based on the needs of a community with no effective options – and wait for further data while people are being treated, or to insist on larger trials that confirm results before approval.
What does it mean?
If upheld, these results represent the first convincing signs that a gene-targeted therapy can slow Huntington’s disease. They may also be the first evidence of benefit from a gene therapy in any adult-onset neurodegenerative disorder. That would be a milestone after decades of failure.
But these results do not prove success. Only larger, longer and fully peer-reviewed studies will show whether this treatment truly changes lives. Even if approved, a complex neurosurgical gene therapy may not be easily accessible to all patients.
The company has said the drug’s price would be similar to other gene therapies – which can cost over A$3 million per patient – and will have the added cost of brain surgery.
The takeaway
For families who carry this gene, the hope is profound. But caution is just as important.
We may be witnessing the first credible step toward slowing an inherited adult-onset neurodegenerative disease, or just an early signal that may not hold up.
Ultimately, only time and rigorous science will show whether this treatment delivers the benefits so urgently needed.
An analysis in the Journal of the American Geriatrics Society reveals that older inpatients admitted to physicians who prescribe higher amounts of first-generation antihistamines face an elevated risk of delirium while in the hospital.
First-generation antihistamines, such as diphenhydramine, are among the leading causes of medication-related harms in older adults, and although these medications are indicated for histamine-related conditions such as hives and anaphylaxis, they may be prescribed inappropriately.
When investigators analysed data on 328 140 patients aged 65 years and older who were admitted by 755 attending physicians to 17 hospitals in Ontario, Canada in 2015–2022, they found that the overall prevalence of delirium was 34.8%. Patients admitted to physicians who more commonly prescribed first-generation antihistamines had 41% increased odds of experiencing delirium compared with patients admitted to physicians who rarely prescribed first-generation antihistamines.
“We hope our study raises awareness among hospitalists that sedating antihistamines can be harmful, and should be prescribed with caution,” said corresponding author Aaron M. Drucker, MD, of the University of Toronto and Women’s College Hospital.
Botulinum injection around neuromas may also be effective for other forms of pain
Photo by Raghavendra V Konkathi on Unsplash
Botulinum toxin injections provided greater short-term relief for phantom limb pain than standard medical and surgical care among Ukrainian war amputees, reports a new study led by Northwestern Medicine and Ukrainian physicians.
The study, which involved 160 amputees treated at two hospitals in western Ukraine between 2022 and 2024, could ultimately benefit millions worldwide, according to the research team.
Post-amputation pain affects most amputees. The condition limits prosthetic use, mobility and quality of life. In the US, more than 2 million people live with limb loss. In Ukraine, it is estimated that over 100 000 soldiers and civilians have lost limbs since Russia’s full-scale invasion, which began in 2022.
“Botulinum toxin injected into painful stumps of residual limbs and around neuromas was on some outcome measures more effective than comprehensive medical and surgical treatment at one month post-treatment,” said senior study author Dr Steven P. Cohen, a professor of anaesthesiology and the vice chair of research and pain medicine at Northwestern University Feinberg School of Medicine.
Dr. Steven Cohen is a retired U.S. Army colonel who traveled to Ukraine to collaborate with local doctors.
“Our results show that botulinum toxin potentially could be a powerful short-term tool for treating post-amputation pain when used alongside comprehensive medical and surgical care,” said co-author Dr. Roman Smolynets, an anesthesiologist and intensive care specialist at Multidisciplinary Clinical Hospital of Emergency and Intensive Care in Lviv, Ukraine.
“It could be another step toward helping amputees live with less pain and more dignity. But always as an additional point to comprehensive medical and surgical care, not as a monotherapy.”
All study participants were amputees treated at the First Medical Union of Lviv or Ivano-Frankivsk Regional Hospital. About one-fifth received botulinum toxin injections around painful nerve endings, called neuromas, in addition to standard medical and physical therapy. The other participants received comprehensive medical and surgical treatment, which included surgical revision, nerve blocks, physical and psychological therapy, medications and other interventional procedures.
The research team assessed pain levels at the start of treatment and after one and three months, focusing separately on phantom limb pain (pain in the missing limb) and residual limb pain (pain at the stump site).
At one month, the botulinum toxin group experienced an average reduction of four points in phantom limb pain on a 10-point scale, compared with just one point among patients in the comparison group. Also at one month, 69% of patients who received botulinum toxin achieved a meaningful improvement (defined as at least a 30% drop in pain) in phantom limb pain, versus only 43% in the other patient group.
However, the results shifted at three months: Patients who received comprehensive care showed more durable pain relief than the botulinum toxin group, consistent with previous research showing that botulinum toxin’s pain-relieving effects typically last about three months.
A novel way to inject botulinum toxin
While botulinum toxin injections, a non-surgical treatment that alleviates pain by blocking nerve signals, are most commonly known for their use in cosmetic procedures, they are also an established tool to treat chronic pain.
In the study, the substance was injected in a novel way. The research team used ultrasound guidance to inject botulinum toxin directly around painful nerve endings and surrounding soft tissues, rather than into muscle or skin. This targeted “peri-neuromal” approach, the scientists believe, may explain the strong short-term reduction in pain by quieting nerve activity and local inflammation. Previous studies have shown botulinum toxin to be effective for neuropathic pain, but none injected it around painful nerves.
The new findings suggest that botulinum toxin injections near nerves may also help relieve other types of nerve pain, such as shingles-related pain, carpal tunnel syndrome and pain following surgeries like mastectomy or thoracotomy.
Friendship with a Ukrainian anaesthesiologist
Cohen, who traveled to Ukraine in 2024 to help launch the study, is a retired U.S. Army colonel who served four overseas tours in support of military operations; his son currently serves with the infantry.
In Ukraine, he partnered with Smolynets, who has treated thousands of soldiers and civilians injured in the war by working in the country’s largest trauma and emergency center, and Dr. Nadiya Segin, who is pioneering the use of Botulinum toxin and nerve stimulation to treat war injuries.
Smolynets will visit Chicago the week of Oct. 19 with a Ukrainian delegation for an observership program, spending time with Cohen at his pain medicine clinic and at a Shirley Ryan AbilityLab in downtown Chicago. The two physicians, now close friends, are available for interviews during that week.
More research in Ukraine
Cohen and his colleagues stress the need for larger, randomized trials to confirm their findings, refine patient selection and optimize botulinum toxin dosing. Future research should also explore whether repeat botulinum toxin injections over time could produce sustained benefits for post-amputation pain, as they appear to do for migraine treatment.
Cohen and Smolynets, who published another study in February about using hydrodissection for post-amputation pain in Ukraine, are also researching more novel war treatments in Ukraine, at Walter Reed, and Northwestern, for traumatic brain injury and PTSD. These studies are underway.
“As a retired colonel and the father of an infantry soldier who could be deployed in future conflicts and suffered from traumatic brain injury while at the U.S. Military Academy, this research carries special personal meaning for me,” Cohen said.
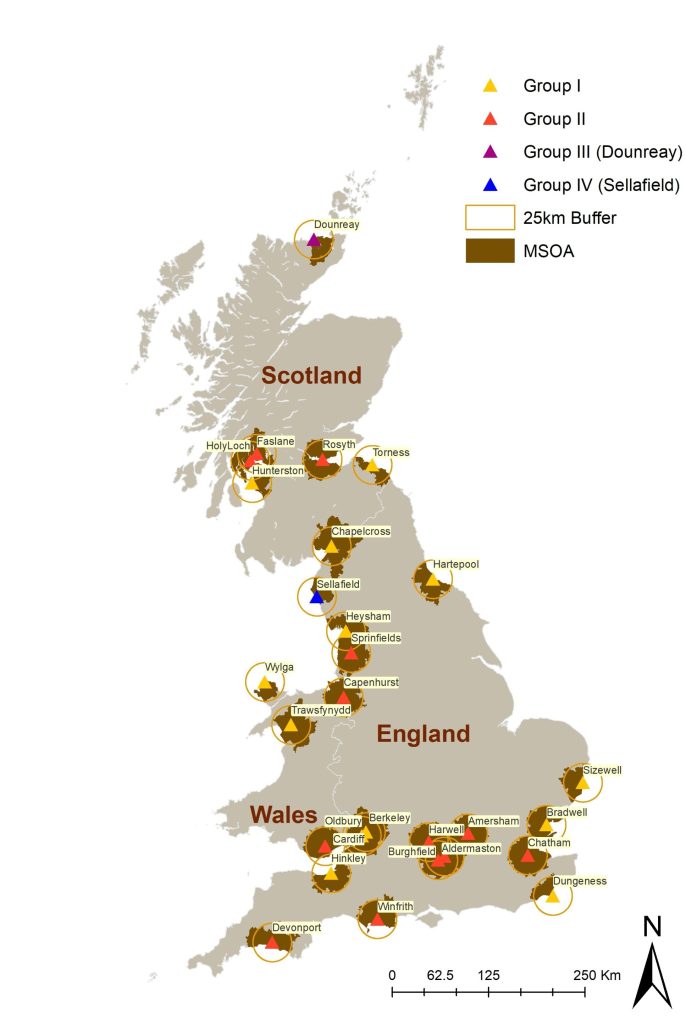
Children living near nuclear power stations in the UK are not at increased risk of childhood cancers, according to a new analysis.
The research was led by scientists at Imperial College London and University of Bristol and commissioned by the UK Committee on the Medical Aspects of Radiation in the Environment (COMARE). The results, published in International Journal of Epidemiology, found no evidence of increased risk of childhood cancers among children living near 28 nuclear installations between 1995 and 2016.
Researchers analysed cancer incidence data for nearly 50 000 cases of childhood leukaemia, non-Hodgkin’s lymphoma (LNHL), central nervous system (CNS) tumours, and other solid tumours in children aged 0–14 years.
They looked at data for communities living within 25 kilometres of installations, including those which have been linked to historical concerns about potential health impacts – such as Sellafield in Cumbria and Dounreay in northern Scotland.
The analysis found no evidence of increased risk of childhood cancers among children living near 28 nuclear installations between 1995 and 2016. (Credit: Davies, B. et al. Int J Epidemiol, 2025)
Using these data and advanced statistical modelling, they found no increased incidence of childhood cancers in these areas compared to national averages.[1] They also found no evidence that cancer risk increased the closer children lived to the nuclear sites.
Dr Bethan Davies, from Imperial’s School of Public Health and lead author of the study, said: “For many years there have been public concerns about the potential health impacts of living near nuclear installations. Our analysis suggests that children living near these sites today are not at increased risk.”
The latest study builds on decades of research following reports in the 1980s of clusters of cancer cases near nuclear facilities in England, Scotland and Germany[2] – following which, the UK Government set up COMARE to advise on the health effects of radiation.
Early investigations confirmed clusters of cases of some cancers near nuclear installations, particularly LNHL.
However, subsequent studies failed to show any direct link between these cases and radiation exposure from nuclear facilities.
In 2016, a COMARE report[3] suggested other potential explanations for these case clusters, including infections introduced due to population mixing in the areas.
The new findings come at a time of renewed interest in nuclear energy as part of the UK’s strategy to meet net-zero carbon targets and the government committing £14.2bn to build a new nuclear power station in Suffolk and develop small modular reactors.
The researchers say that while their study offers reassurance, they support COMARE’s recommendations for ongoing surveillance of cancer incidence near nuclear sites.
The authors acknowledge a number of limitations with their study, including the use of residential address at diagnosis as a proxy for exposure.
They were also unable to account for individual-level risk factors – such as genetic or medical conditions. However, they emphasise that the study’s design and comprehensive data make it one of the most detailed assessments to date.
Dr Davies added: “As the UK government announces a multibillion-pound investment for new nuclear energy infrastructure, our findings should provide reassurance that the historical clusters of childhood cancers reported near sites such as Sellafield and Dounreay are no longer evident.”
Professor Mireille Toledano, Mohn Chair in Population Child Health in Imperial’s School of Public Health, said: “These findings are both timely and important. As the UK and other countries expand their nuclear energy capacity, it’s vital that public health remains a central consideration. It’s reassuring that our study found that the historic case clusters have resolved, but it remains important we continue to monitor public health data around such sites across the UK for any emerging trends of concern.”
The full study, published today in the International Journal of Epidemiology, was supported by funding from the National Institute for Health and Care Research (NIHR), Health Data Research UK (HDRUK) and the UK Medical Research Council (UK Research and Innovation (UKRI)).
The work was also supported by the NIHR Imperial Biomedical Research Centre, a translational research partnership between Imperial College Healthcare NHS Trust and Imperial College London.
–
[1] Researchers obtained national incident cases of cancer diagnosed between 1995 and 2016 in children under 15 years of age from NHS England (formerly Public Health England), Welsh Cancer Intelligence and Surveillance Unit and Health Protection Scotland.
[2] A cluster of cases of leukaemia in children living close to the Sellafield nuclear plant was reported in 1983. An Independent Advisory Group confirmed the cluster and the UK government established COMARE to advise on the health effects of radiation. Subsequent studies identified increased risks of cancers in children and young adults living near Sellafield, Dounreay (Scotland), and Hamburg (Germany) nuclear installations.
[3] Committee on Medical Aspects of Radiation in the Environment (COMARE) – Seventh report (2016) https://assets.publishing.service.gov.uk/media/5a7f70ed40f0b6230268f83c/COMARE_17th_Report.pdf
HealthTech is transforming healthcare through AI, mobile applications, wearable devices, telemedicine, and big data analytics. While these advances offer enormous potential to improve patient outcomes and operational efficiency, they also raise complex legal and regulatory challenges – spanning intellectual property, data privacy, licensing, corporate governance, funding, taxation, and litigation.
Webber Wentzel’s Navigating HealthTech Legal Solutions highlights the firm’s extensive experience in helping innovators, investors, and healthcare providers across Africa address the legal and regulatory complexities of HealthTech. Mapping out the complexities at play across both the technology and the law, this resource brings together Webber Wentzel’s cross-practice teams to give clients a holistic perspective on opportunities, risks, and emerging trends in healthcare innovation.
“Our clients are leading the way in healthcare innovation, and they need legal partners who understand the sector end-to-end,” says Bernadette Versfeld, head of the Consumer sector. “This resource demonstrates how we help businesses navigate regulatory hurdles, adopt new technologies, structure investments effectively, and manage risk, all while enabling growth and innovation.”
Drawing on extensive experience working with healthcare companies, insurers, tech providers, investors, and regulators across Africa, the report provides insights into medical device licensing, HealthTech investment structuring, protecting personal health data, managing litigation risks, and compliance with South Africa’s National Health Insurance Act.
“As part of our ongoing commitment to supporting Africa’s healthcare sector, Webber Wentzel continues to advise on emerging trends, innovative technologies, and regulatory developments. By combining deep sector knowledge with cross-practice expertise, we help clients not just respond to change but shape it, empowering them to navigate the complex intersection of healthcare and technology,” adds Versfeld.