If a picture is worth a thousand words, how much is a graph worth? For doctors trying to determine whether a patient’s blood pressure is within normal range, the answer may depend on the type of graph they’re looking at.
A new study from the University of Missouri highlights how different graph formats can affect clinical decision-making. Because blood pressure fluctuates moment to moment, day to day, it can be tricky for doctors to accurately assess it.
“Sometimes a patient’s blood pressure is high at the doctor’s office but normal at home, a condition called white coat hypertension,” said Victoria Shaffer, a psychology professor in the College of Arts and Science and lead author of the study published in the Journal of General Internal Medicine. “There are some estimates that 10% to 20% of the high blood pressure that gets diagnosed in the clinic is actually controlled – it’s just white coat hypertension – and if you take those same people’s blood pressure at home, it is really controlled.”
In the study, Shaffer and the team showed 57 doctors how a hypothetical patient’s blood pressure data would change over time using two different types of graphs. One raw graph showed the actual numbers, which displayed peaks and valleys, while the other graph was a new visual tool they created: a smoothed graph that averages out fluctuations in data.
When the blood pressure of the patient was under control but had a lot of fluctuation, the doctors were more likely to accurately assess the patient’s health using the new smoothed graph compared to the raw graph.
“Raw data can be visually noisy and hard to interpret because it is easy to get distracted by outliers in the data,” Shaffer said. “At the end of the day, patients and their doctors just want to know if blood pressure is under control, and this new smoothed graph can be an additional tool to make it easier and faster for busy doctors to accurately assess that.”
This proof-of-concept study is the foundation for Shaffer’s ongoing research with Richelle Koopman, a professor in the School of Medicine, which includes working with Vanderbilt University and Oregon Health & Science University to determine whether the new smoothed graph can one day be shown to patients taking their own blood pressure at home. The research team is working to get the technology integrated with HIPAA-compliant electronic health records that patients and their care team have access to.
This could alleviate pressure on the health care system by potentially reducing the need for in-person visits when blood pressure is under control, reducing the risk for false positives that may lead to over-treatment.
“There are some people who are being over-treated with unnecessary blood pressure medication that can make them dizzy and lower their heart rate,” Shaffer said. “This is particularly risky for older adults who are more at risk for falling. Hopefully, this work can help identify those who are being over-treated.”
The findings were not particularly surprising to Shaffer.
“As a psychologist, I know that, as humans, we have these biases that underlie a lot of our judgments and decisions,” Shaffer said. “We tend to be visually drawn to extreme cases and perceive extreme cases as threats. It’s hard to ignore, whether you’re a patient or a provider. We are all humans.”
Given the increasing popularity of health informatics and smart wearable devices that track vital signs, the smoothed graphs could one day be applied to interpreting other health metrics.
“We have access to all this data now like never before, but how do we make use of it in a meaningful way, so we are not constantly overwhelming people?” Shaffer said. “With better visualisation tools, we can give people better context for their health information and help them take action when needed.”
As a healthcare professional, you’re used to taking care of the health of your patients. But what about the health of your practice? If you’re not sure, that’s understandable – after all, doctors and practice managers have enough on their plate without worrying about finding opportunities for more revenue. Luckily, there’s a new, easy to use tool from a provider with a strong track record of developing actionable, real-world solutions for the South African market.
A control room for your practice
“Think of the new Engage Mx report as the control room for your practice,” says Dr Benji Ozynski, who developed the platform in partnership with Altron HealthTech. “With Engage Mx, everything you need to know about your practice is in one place with one easy to use interface.”
“Engage Mx on Elixir Live has been in the market for a couple of years and already proven popular with doctors eager to embrace the advantages of data-driven healthcare,” says Ntombizanele Gxamza, Head of Product Strategy at Altron HealthTech. “The new Engage Mx report functionality on the platform brings data about the financial health of the practice and most importantly the health of a practice’s population of patients to a patient-centred approach. At a glance, the report makes it possible to see a range of statistics, presented in the form of easy to read graphics. It can be accessed on any device, making it convenient for even the busiest doctor.”
When using the new Engage Mx report, healthcare professionals can see:
Revenue by week
Number of patients seen, compared month by month and year by year
Busiest days, months, and seasons
Patient profiles by age group
Gaps in care by age group
Trends in types of conditions being treated
Using this kind of information, doctors are able to build up a clear picture of the health of their practice, and where there could be opportunities for improvement. In just one pilot project with a GP with a busy practice, the Engage Mx report uncovered over R400 000 lost due to missed patient health reviews. The doctor was able to see which age groups were most likely to need intervention – and prevention – before health problems became more serious.
Better health for patients, healthcare professionals and practices
The report helps healthcare professionals answer a range of questions such as:
When is the best time for me to take leave?
What kind of services could I add to the practice offering?
Are there growing patient needs that my practice could be fulfilling?
Where and how can I innovate my offering?
How do I grow my practice sustainably?
What kind of resources am I going to need in order to grow?
When and how should I be communicating with my patients?
Could my practice benefit from running marketing campaigns?
Because the data is so clearly visualised and easily accessible, busy healthcare providers don’t need to take hours out of their professional or personal time to make sense of the numbers.
Ultimately, the beauty of the new tool is that better health outcomes for patients can also improve the financial health of the practice – and also the time and administrative burden on doctors, because it can help reduce the hours currently spent on doing these tasks manually. Adds Dr Ozynski: “Doctors who’ve already used the Engage Mx report have told me that it makes it easier to plan their leave, for example, or look for new opportunities to expand services, while making their patients feel valued.”
Data-driven healthcare is perhaps the most exciting global trend in healthcare today. Practical, user-friendly tools like Engage Mx make it possible for South African doctors to take what they do best – bring the human touch to healthcare, while enabling them to future-proof their practices in an increasingly complex clinical and regulatory environment. A financially healthy practice is a sustainable practice, and that’s good for everyone.
Patients with spastic paraplegia type 15 develop movement disorders during adolescence that may ultimately require the use of a wheelchair. In the early stages of this rare hereditary disease the brain appears to play a major role by over-activating the immune system, as shown by a recent study published in the Journal of Experimental Medicine. The study was led by researchers at the University of Bonn and the German Center for Neurodegenerative Diseases (DZNE). These findings could also be relevant for Alzheimer’s disease and other neurodegenerative conditions.
Spastic paraplegia type 15 is characterised by the progressive loss of neurons in the central nervous system that are responsible for controlling movement. Initial symptoms typically appear in late childhood, manifesting first in the legs in the form of uncontrollable twitching and paralysis. “What exactly causes these neurons to die is still not fully understood,” explains Professor Elvira Mass from the LIMES Institute at the University of Bonn. “In this study, we investigated the potential role of the immune system in this process.”
Professor Mass and Dr. Marc Beyer from the DZNE, together with Professor Ralf Stumm from University Hospital Jena, served as the study’s lead investigators, bringing together extensive experience to study this rare hereditary disease. The condition is triggered by a defect in the so-called SPG15 gene, which contains instructions for building a protein. But due to that defect, the protein cannot be produced.
Severe inflammation preceding the onset of cell damage
In their experiments the researchers used mice that shared the same genetic defect. “There was existing evidence that inflammatory processes in the brain play a role in development of the disease,” Dr Beyer explains, “So we studied microglia, which are the immune cells of the brain, and also whether immune cells in bone marrow are additionally involved in the inflammatory response.”
White blood cells form in bone marrow and can reach the brain via the bloodstream. Microglia, on the other hand, have already migrated to the brain during embryonic development. The researchers succeeded in specifically labelling the cells derived from bone marrow with a fluorescent dye. “This makes them distinguishable from microglia under a microscope,” Mass elaborates. “This allowed us to study the interaction between these two cell populations at the individual cell level.”
Analyses show that the microglia cells undergo dramatic changes in very early stages of the disease, long before any neuronal damage is identifiable. The cells are thereby altered into “disease-associated microglia.” These release messenger substances which, among other things, call for the help of cytotoxic “killer” T cells from the bone marrow that destroy other cells. The two cell types communicate with each other via signaling molecules, and their interplay drives the inflammatory process.
New therapeutic possibilities
“Our data suggest that the early stages of the disease are driven not by the loss of motor neurons but rather by the severe, early immune response,” Mass relates, “and that finding implies new therapeutic possibilities. Immune suppression drugs could potentially help slow progression of the disease.”
Inflammatory processes in the brain play an important role in Alzheimer’s and other neurodegenerative diseases. Spastic paraplegia is caused by entirely different conditions than dementia, but a very similar disruption of the immune system could be involved in dementia.
Researchers have developed a new therapy that can be injected intravenously right after a heart attack to promote healing and prevent heart failure. The therapy both prompts the immune system to encourage tissue repair and promotes survival of heart muscle cells after a heart attack. Researchers tested the therapy in rats and showed that it is effective up to five weeks after injection.
The research team, led by bioengineers at the University of California San Diego and chemists at Northwestern University, published their findings in Advanced Materials.
“Preventing heart failure after a heart attack is still a major unmet clinical need,” said Karen Christman, one of the study’s corresponding authors and a professor of bioengineering at UC San Diego. “The goal of this therapy is to intervene very soon after someone suffers a heart attack to keep them from ultimately going into heart failure.”
Side by side comparison of heart muscle cells with and without treatment. Damage to the cells is shown in blue. On the left, tissue has been injected with saline and the damaged area is considerably larger. On the right, the issue was treated with the PLP platform and the damaged area is significantly smaller.
The therapy could have broader applications, said Nathan Gianneschi, the paper’s other corresponding author and a professor in the Department of Chemistry at Northwestern.
“This therapeutic platform has tremendous potential for several diseases, including everything from macular degeneration to multiple sclerosis and kidney disease,” Gianneschi said.
The platform aims to block the interaction of two key proteins that intervene in the body’s response to stress and inflammation. When the protein Nrf2 is activated, cells resist the degradation brought on by inflammation. But KEAP1 binds with Nrf2 to degrade it in turn. After a heart attack, this process of degradation has to be stopped so that tissues can health better.
The protein-like polymer, or PLP, platform is made from a polymer that mimics Nrf2. Once injected intravenously, it finds KEAP1 and binds to it, preventing it from binding to the actual Nrf2 protein and degrading it.
Researchers injected rat models after a heart attack with either the PLP platform or a saline solution. The team was blinded to which animals received the polymer or saline. After five weeks, the rodents underwent MRIs while sedated. The animals injected with the polymer showed better cardiac function and significantly more healing in their heart muscle tissue. Other tests also showed that genes that promote healing of tissues were expressed more.
Researchers describe the study as a proof of concept. Before moving on to tests in larger mammals, they want to optimize the design and dosage, and conduct further analysis.
“Proteins are the molecular machines that drive all essential cellular function, and dysregulated intracellular protein-protein interactions are the cause of many human diseases,” Gianneschi said. “Existing drug modalities are either unable to penetrate cells or cannot effectively engage these large disease target domains. We are looking at these challenges through a new lens.”
The therapy method was developed by Gianneschi, while he was a faculty member at UC San Diego, where he is now an adjunct faculty. He continued working on the technology at Northwestern.
In a new study, National Institutes of Health (NIH) researchers found that altered B cell function in children with mitochondrial disorders led to a weaker and less diverse antibody response to viral infections. The study, published in Frontiers in Immunology, was led by researchers at the National Human Genome Research Institute (NHGRI), who analysed the gene activities of immune cells in children with mitochondrial disorders and found that B cells, which produce antibodies to fight viral infections, are less able to survive cellular stress.
“Our work is one of the first examples to study how B cells are affected in mitochondrial disease by looking at human patients,” said Eliza Gordon-Lipkin, MD, assistant research physician in NHGRI’s Metabolism, Infection and Immunity Section and co-first author of the paper.
Mitochondria are important components of nearly every cell in the body because they convert food and oxygen into energy. Genomic variants in more than 350 genes have been linked to mitochondrial disorders with varied symptoms depending on which cells are affected.
“For children with mitochondrial disorders, infections can be life threatening or they can worsen the progression of their disorder,” said Peter McGuire, MBBCh, NHGRI investigator, head of the Metabolism, Infection and Immunity Section and senior author of the study. “We wanted to understand how immune cells differ in these patients and how that influences their response to infections.”
Around 1 in 5000 people worldwide have a mitochondrial disorder. Examples of mitochondrial disorders are Leigh’s syndrome, which primarily affects the nervous system, and Kearns-Sayre syndrome, which primarily affects the eyes and heart.
While mitochondrial disorders are known to affect organs such as the heart, liver, and brain, less is known how they affect the immune system.
Using a genomic technique called single-cell RNA sequencing, which analyzes gene activity in different cell types, researchers studied immune cells found in blood. These cells include different types of white blood cells that help the body fight infections. During stressful conditions, these cells produce a microRNA called mir4485. MicroRNAs are small strings of RNA that help control when and where genes are turned on and off. mir4485 controls cellular pathways that help cells survive.
“We think that B cells in these patients undergo cellular stress when they turn into plasma cells and produce antibodies, and these B cells then try to survive by producing the microRNA to cope,” said Dr. McGuire. “But the B cells are too fragile due to their limited energy, so they are unable to survive the stressful conditions.”
Researchers used a technique called VirScan to look at all past viral infections, assess how well the immune system fought those infections and see the effects of B cells and plasma cells on antibody production. With a weaker antibody response, the immune systems in children with mitochondrial disorders are less able to recognize and neutralize invading viruses and clear infections.
Researchers aim to use the results of this study to guide future treatment of patients with mitochondrial disorders, noting that more translational studies are needed in this research area.
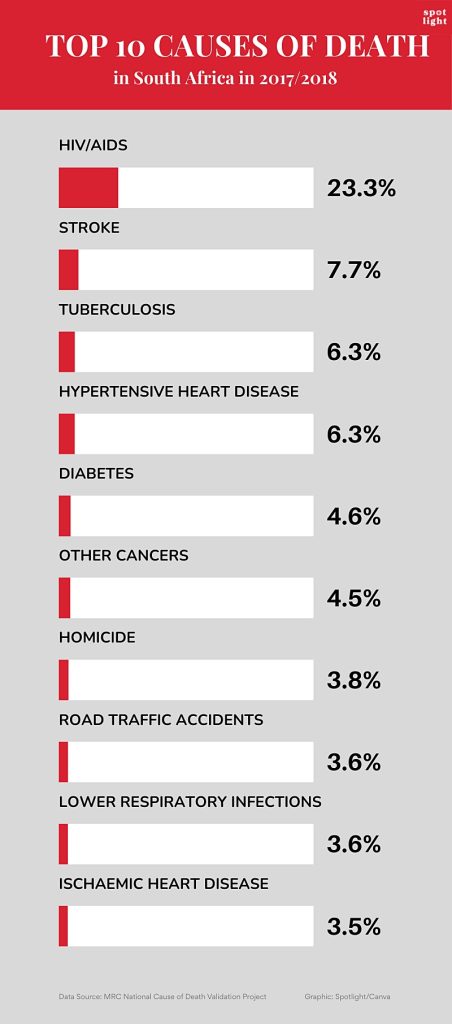
It is widely acknowledged among health and demographic experts that relying solely on what is written on death certificates does not paint an accurate picture of what people in South Africa are actually dying of. Now, an SAMRC study has provided evidence that the undercounting of deaths due to HIV might be even greater than previously thought.
Many in health circles were surprised by a recent South African Medical Research Council (SAMRC) study that found that 23% of deaths in a nationally representative sample drawn from 2017/2018 were due to HIV. By comparison, Stats SA data for roughly the same period puts the figure at only 5.7%.
That Stats SA’s HIV mortality figures differs from other sources is not new and not in itself surprising. This is because Stats SA reports a relatively straight-forward count of what is written on death certificates – where it is known HIV is often not indicated, even if it is the underlying cause of death. By contrast, the new SAMRC study looked at autopsy reports, death certificates, medical records, and interviews with next of kin to come up with its much higher estimate.
The thing that did come as a surprise, is just how much higher the SAMRC figures were than anticipated. Previously, the real number of HIV deaths were thought to be around double the Stats SA number, rather than four times as much. For example, according to Thembisa, the leading model of HIV in South Africa and the basis for UNAIDS’s estimates for the country, around 12% of deaths in the country in 2018 were due to HIV.
“Accurate mortality data are essential for informed public health policies and targeted interventions; however, this study highlights critical gaps in our cause-of-death data, particularly in the underreporting of HIV/AIDS and suicides,” says Professor Debbie Bradshaw, study co-author and Chief Specialist Scientist at the SAMRC Burden of Disease Research Unit, in a media statement. (The study also found substantial under-reporting of suicide on death certificates.)
Multiple data sources
The study was conducted in three phases, examining deaths that were registered in 27 randomly selected health sub-districts between 1 September 2017 and 13 April 2018.
In addition to the examination of autopsy reports, death certificates, and medical records, trained fieldworkers interviewed next of kin to conduct verbal autopsies using a World Health Organization (WHO) questionnaire that had been translated into the country’s nine official languages.
Based on these various sources of data, the cause of each death was categorised into one or more of 44 categories and then compared to the cause of death indicated on the person’s death certificate. (The process for ensuring accuracy, including a review shared by a team of 49 medical doctors, is described in detail in this report.)
The researchers collected data for over 26 000 deaths, although not all types of data were available for each death. Medical records were available for over 17 600 cases, forensic pathology (autopsy) records for 5 700, and about 5 400 verbal autopsies were conducted. In the end, “to save costs”, not all medical records were reviewed.
Overall, for just over 15 000 deaths, the researchers could link and compare their assessment of why a person died to what was written on death certificates.
‘Poor agreement’
The researchers found that “there was poor agreement between the underlying cause of death obtained from the study and the official cause of death data”. The cause of death was the same in only 37% of cases. In addition to the under-reporting of HIV, the researchers also identified “severe under-reporting” of suicide as a cause of death.
A strong link between TB and HIV was observed, with TB responsible for 46% of deaths among people with HIV and 63% of TB deaths occurring in individuals with HIV. Together, these two diseases accounted for almost 30% of deaths.
Some question marks
As noted earlier, the new numbers are substantially higher than estimates from the highly respected Thembisa model. According to their data only 12% of deaths from mid-2017 to mid-2018 were due to HIV-related causes, with a further 9% of deaths occurring in persons with HIV but due to other causes.
Dr Pam Groenewald, a co-author of the new study and also with the SAMRC, describes Thembisa as “an excellent source”. She tells Spotlight they had a long discussion with the Thembisa researchers, “but we weren’t able to fully explain the differences”.
The study authors cite several factors that might contribute to a higher proportion of HIV deaths in their study. Firstly, the weighted national causes of death validation sample aimed to represent the registered deaths in the country, and it was known that deaths in rural areas and child deaths were under-represented. Secondly, deaths that occurred in private sector hospitals were not represented. Groenewald says the HIV-linked deaths in private hospitals are “definitely lower”, but doubts they would have had a significant impact on their findings.
One thing in favour of the study numbers is the fact that the cases they identified with HIV/AIDS as the underlying cause of death were independently reviewed by clinicians. As Groenewald points out, they looked at medical records of people admitted to and who died in hospital, including CD4 cell counts and HIV viral loads. The suggestion is that if someone had a very low CD4 count and a very high HIV viral load at the time of death, then it is very likely HIV played a role in their death, unless of course they died of a clearly non-associated cause like injuries from a car accident.
On the other hand, it might be argued that since HIV is very widely tested for in South Africa, it is more likely to appear on medical records than other less tested for diseases.
Another interesting wrinkle is that the proportion of deaths from HIV/AIDS from this study was higher than anticipated based on observed declines in adult mortality. It is widely accepted that the decline in adult mortality and the increase in life-expectancy over the last two decades was driven by antiretroviral therapy keeping more people with HIV alive. While the new findings do not challenge this narrative, it does suggest the effect may be less pronounced than previously thought.
What to do?
The researchers suggest their study has immediate implications for the country’s response to HIV and TB.
“The study recommends strengthening case finding, follow-up, prevention, and treatment for HIV, AIDS and TB to reduce mortality rates, and underlines the importance of government’s rapid response to counter the recent abrupt withdrawal of Pepfar funding,” Bradshaw comments in the media release.
But more broadly, the findings put the spotlight on major problems in the country’s death certification systems.
“Our findings highlight the need for improved record quality and adherence to testing guidelines within the medical community. Poor record keeping included incomplete documentation of clinical findings and results,” the study authors write.
“A lot of doctors’ report HIV as ‘retroviral disease’, for example, and it’s not coded as HIV,” Groenewald explains to Spotlight.
Urging doctors to record the actual underlying cause of death when writing up death certificates, she also called for improved training in death certification at medical schools.
Doctors’ reluctance to report HIV on death certificates likely has various reasons, including stigma related to HIV and the fact that some medical insurance policies used to exclude HIV, though policies now treat HIV like any other chronic condition.
Overall, Groenewald says, we need to step back and probe the rationale of compiling underlying cause of death statistics.
“The public health aim of the medical certificate of cause of death, (MCCD), is to prevent premature deaths. We therefore need to record the cascade of events or causal sequence of medical conditions leading to death and target our interventions at the underlying cause of death. The coding rules focus on the underlying cause of death, (UCOD), to compile the mortality statistics,” she says.
Groenewald stresses that the law requires doctors to provide accurate information on death causation. The Health Professions Council of SA’s ethical rules also recognised that a statute requiring disclosure about a deceased person’s health must be complied with and is not considered unethical. Contrary to common physician misconception, Groenewald says all this combined to show “it is completely ethical to disclose on a death certificate that a person has died from an AIDS related illness”.
In the meantime, routine mortality data from Stats SA should clearly be taken with a pinch of salt. As Groenewald points out, vital registration data should not be accepted at face value but should be interrogated and cross-checked with other data sources to get coherent and consistent estimates that fit within an envelope of all causes of mortality.
A misfolded protein facilitates reliable diagnosis even in the early stages of Parkinson’s disease in body fluids.
Source: CC0
Parkinson’s disease is a neurodegenerative disorder that is usually diagnosed in its late stage on the basis of clinical symptoms, mainly motor disorders. By this point, however, the brain is already severely and irreparably damaged. Moreover, diagnosis is difficult and often incorrect because the disease takes many forms and symptoms overlap with other disorders.
Researchers from the PRODI Center for Protein Diagnostics at Ruhr University Bochum, Germany, and the biotech company betaSENSE have now discovered a biomarker in cerebrospinal fluid (CSF) that facilitates a reliable diagnosis at an early stage and can shed light on the progression of the disease and the effect of a therapy. They report their findings in the journal EMBO Molecular Medicine.
Parkinson’s disease – an unstoppable condition
Parkinson’s disease is characterised by the loss of dopaminergic nerve cells in the brain, typically leading to increasing motor impairments as the symptoms progress. Dopamine supplements can compensate for the loss and temporarily alleviate the symptoms. The misfolding of the key protein alpha-synuclein (αSyn) from α-helical structures to β-sheet-rich structures plays a crucial role in the development of Parkinson’s disease. “These misfoldings make the protein sticky, leading to the formation of larger complexes, so-called oligomers. The oligomers then produce long fibrillar filaments and cause the aggregation of these filaments into macroscopically large Lewy bodies in the brain,” explains Professor Klaus Gerwert, founding and managing director at PRODI and CEO of betaSENSE.
Advanced platform technology
In two independent clinical cohorts with a total of 134 participants, the Bochum-based researchers showed that, with a sensitivity and specificity of well over 90%, this misfolding of αSyn in body fluids is a viable biomarker for the diagnosis of Parkinson’s disease. The research was conducted using cerebrospinal fluid samples from patients at the Parkinson’s centres in Bochum (St. Josef Hospital, Professor Lars Tönges, Professor Ralf Gold) and Kassel (Paracelsus-Elena-Klinik, Dr. Sandrina Weber, Professor Brit Mollenhauer). The measurements were carried out using the patented iRS (immuno-infrared sensor) technology from betaSENSE GmbH.
betaSENSE has already successfully implemented the iRS technology for diagnosing Alzheimer’s disease. In this case, it was shown that the misfolding of the biomarker Aβ can indicate the risk of Alzheimer’s dementia at a later stage with high accuracy up to 17 years before clinical diagnosis. “We have now transferred this approach to Parkinson’s for the misfolding of αSyn,” stresses Klaus Gerwert.
Development of Parkinson’s drugs
In addition to diagnostic applications, the technology can also help to develop new active substances and prove their efficacy in clinical trials.
Researchers at Aston University have called for more advice to be given to young people about preventing dry eye disease, after a study carried out in conjunction with Oslo University Hospital and Sørlandet Hospital Trust in Norway found that 90% of participants had at least one sign of the condition in their eyes.
Dry eye disease occurs when the eyes do not make enough tears, or make poor-quality tears without sufficient lipid or mucus levels which leads to poor tear film stability and rapid evaporation. Sufferers may have gritty feeling eyes, itching or stinging in the eyes, red eyes, sensitivity to light and blurry vision. There are several risk factors for dry eye disease, including stress and wearing contact lenses. It is also more prevalent in females. In the 18-25 age group, a major risk factor is screen use.
The research, following 50 18-25-year-olds over time, was led by Dr Rachel Casemore at Aston University School of Optometry and is the first of its kind. It was published in The Ocular Surface. The researchers looked for symptoms of dry eye disease in the participants, studied lifestyle factors, and followed up with participants one year on to find out if there had been any progression of the condition.
The initial study showed that 56% of participants had dry eye disease, while 90% had at least one symptom of the condition. Around half of the participants in the study had lost at least 25% of a type of gland in the eye called the meibomian gland. These glands produce the outer lipid layer of the eye’s tear film, which is responsible for preventing evaporation of tears, and therefore keeps the tear film stable and the eye moist. One year on, the researchers found that there had been significant progression of dry eye disease in the study participants.
Additionally, the researchers found correlation found between how long the study group used screens and signs of dryness on the eye surface. The average screen use of participants was eight hours per day.
The researchers concluded that the evidence of dry eye disease symptoms and progression in the young adults in their study shows the need for early detection of potential signs, and the identification of those who may go on to develop dry eye disease. These individuals can then be advised on managing the condition before progression.
The progression and development of dry eye disease can be slowed by various methods. Dr Casemore says that the simplest ways are to take regular screen breaks, to carry out blink exercises to ensure the release of oils from the meibomian glands and to keep hydrated. A healthy, balanced diet, including sources of omega-3 fatty acids, such as oily fish, is also important, as is regular sleep patterns.
Dr Casemore suggests that those with irregular sleep patterns, such as those caused by sleep disorders or anxiety, should seek advice. People who wear contact lenses need to ensure they get regular check-ups to ensure optimum fitting, and that they adhere to their replacement schedule, wearing time schedule, cleaning regimes and safety advice, such as no sleeping, showering or swimming in contact lenses.
Dr Casemore said:
“It is concerning to note the increasing prevalence of dry eye disease signs and symptoms in young adults, which has been referred to as a ‘lifestyle epidemic’ by some researchers. Eye care practitioners are well placed to identify the clinical indicators of dry eye disease and counsel young adults around modifiable risk factors, such as screen use habits, sleeping habits, contact lens use, diet, blinking patterns, and management of stress levels.
“Our future research aims to continue investigation of the potential tear and meibomian gland oil biomarkers which were identified during the study and further explore the effect of diet on dry eye disease development.”
Pancreatic cancer. Credit: Scientific Animations CC BY-SA 4.0
Pancreatic cysts are fluid-filled sacs that can form in the pancreas. Some remain benign, while others have the potential to develop into pancreatic cancer. A recent study, which followed 257 patients in Japan for an average of five years, showed that the presence or absence of invasive nodules in pancreatic cysts is key to assessing whether these cysts are benign or cancerous.
The findings, published in the journal Annals of Surgery, may help patients diagnosed with a high risk of pancreatic cancer to avoid unnecessary surgery.
Pancreatic cancer is one of the most life-threatening and rapidly growing cancers. Pancreatic cysts, known as pancreatic intraductal papillary mucinous neoplasms (IPMNs), are gaining attention as one of the precursors of the cancer that can be identified by radiological imaging. In this context, patients diagnosed with pancreatic cysts are referred for further evaluation, and if they meet the criteria for being at particularly high risk of developing cancer, called high-risk stigmata, they are often recommended for surgery.
However, it was not clear whether all patients who met the criteria would need to undergo surgery. “In fact, among patients who underwent surgery, there were a number of cases where pathological examination results showed that their IPMNs were still benign and had not progressed to cancer,” explained Ryohei Kumano from Nagoya University, the first author of the study. “Pancreatic surgery is a significant burden for patients, so we wanted to find a more accurate way to diagnose whether their IPMNs are benign or cancerous in order to avoid unnecessary surgery.”
A research group consisting of Professor Hiroki Kawashima and Dr Kumano from Nagoya University Graduate School of Medicine, Professor Eizaburo Ohno from Fujita Health University, and their colleagues focused on the presence or absence of invasive nodules in 257 IPMN patients with high-risk stigmata. The researchers evaluated the prognosis of the patients with and without these nodules.
Invasive nodules, solid growths within cysts that have begun to invade surrounding tissues, are difficult to detect with a conventional method that uses a CAT scan. Therefore, the researchers instead used contrast-enhanced endoscopic ultrasound, which is thought to detect invasive nodules more accurately.
To track the prognosis of patients with and without invasive nodules between surgical and non-surgical groups, the researchers followed them for an average of about five years (ranging from 6 months to 24 years, depending on the patient).
The results showed that the presence or absence of invasive nodules had a significant impact on their survival. For patients with invasive nodules, undergoing surgery had a positive effect on improving their survival. On the other hand, most patients without invasive nodules had a favorable outcome even without surgery.
Endoscopic ultrasound (EUS) enables differentiation between non-invasive and invasive nodules within IPMN, providing crucial information for surgical decision making. (Credit: Ryohei Kumano)
In this study, a total of 21 patients who did not have invasive nodules opted for clinical monitoring instead of surgery. Notably, their five-year survival rates were 84.7% for overall survival and 100% for disease-specific survival.
In addition, in patients at higher risk for surgery, such as the elderly, there was little difference in survival rates between patients who underwent surgery and those who did not, if they had no invasive nodules. “Avoiding surgery, especially in such patients, seems to be a reasonable treatment strategy, given the fact that pancreatic surgery is highly invasive, carries a high risk of complications, and requires a long recovery period,” Kumano said.
“We expect that our findings will contribute to future clinical guidelines for IPMNs, leading to more accurate cancer diagnosis and optimised treatment selection.”
Excessive screen time among adolescents negatively impacts multiple aspects of sleep, which in turn increases the risk of depressive symptoms – particularly among girls. That is the conclusion of a new study published in the open-access journal PLOS Global Public Healthby Sebastian Hökby of Karolinska Institutet, Sweden, and colleagues.
Recently, the Swedish Public Health Agency published recommendations that adolescents use no more than two-to-three hours of daily leisure screen time, partly to promote better sleep. Previous studies have suggested associations between screen time, sleep disruptions, and depression in teens. However, sleep problems and depression often coincide, and the direction of these associations has been unclear.
In the new study, researchers tracked 4,810 Swedish students aged 12-16, collecting data on sleep quality and quantity, depressive symptoms, and screen usage at three timepoints over the course of a year.
The researchers found that increased screen time led to deteriorated sleep within three months, impacting both the duration and quality of sleep. Screen time was also found to postpone sleep times towards later hours – disrupting multiple aspects of the human sleep-wake cycle at once. Among boys, screen time had a direct adverse effect on depression after twelve months, while among girls the depressive effect was mediated through sleep disturbances. Sleep could explain about half (38%-57%) of the association between screen time and depression in girls. Boys who spent more time on screens also experienced sleep disruptions, but these were not strongly associated to later depression.
The authors summarize: “In this study, we found that adolescents who reported longer screen times also developed poorer sleep habits over time. In turn, this led to increased depression levels, especially among girls.”
They add: “Our results do suggest that less[…] screen time seems healthier, in line with previous World Health Organization statements…if screen times were somehow reduced, for example through public health policies, our results imply that the high burden of depressive states among young Swedish women, and maybe young men, would likely decrease.”