New Expanding Pill for Weight Loss Reduces Hunger Cravings
An innovative new pill could soon offer a new and affordable weight management treatment, following a successful clinical trial involving University of Bristol researchers and supported by the National Institute for Health and Care Research (NIHR). The results are published in the journal Obesity.
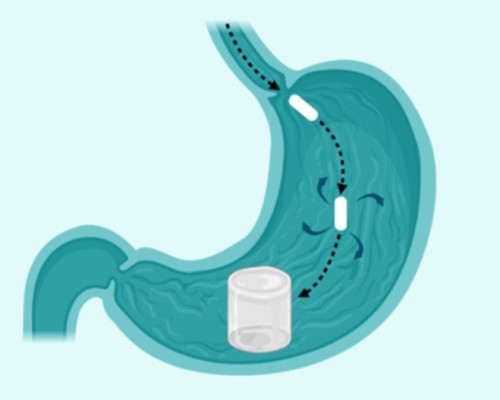
Sirona by Oxford Medical Products is a hydrogel-based pill that is designed to aid weight loss by reducing hunger. After it is swallowed, the pill expands in the stomach, leading to faster satiety. This helps individuals to eat less without needing strong medications or injections.
Thirty-nine participants in Southampton took part at the NIHR Southampton Clinical Research Facility.
In the trial, funded by Innovate UK, participants lost up to 13.5% of their body weight in just six months. On average, people with class 1 obesity (BMI 30-35) lost 6.4% of their body weight.
Participants also ate on average 400 fewer calories per day compared to those taking a placebo. For context, recent Government-led research suggests that even a 216-calorie daily reduction could cut the UK’s obesity rate in half.
The trial was led by chief investigator Professor James Byrne in the NIHR Southampton Biomedical Research Centre.
Mr Byrne, a consultant surgeon at University Hospital Southampton, said: “Obesity is a chronic and often progressive disease. With obesity rates continuing to rise, these results are an important step towards providing a different treatment option.
“This trial demonstrated Sirona could be a safe, affordable, and non-pharmacological treatment to support long-term weight management.”
Sirona will be accessible to anyone with a BMI 25-40, which means Sirona is particularly well-suited to help two key patient types. Firstly, for patients with an overweight BMI (25–30), allowing them to proactively manage their weight and to avoid progressing into obesity and the serious health problems it can bring. Secondly, it is suitable for use as an ‘off-ramp’ for GLP-1 users looking to come off treatment but prevent weight regain, which often occurs once GLP-1 medication ceases.
GLP-1 medications have become very popular for weight loss, with around 1.5 million users in the UK. However, a significant proportion of users pay out of pocket and prices have recently doubled in the UK for some doses of Mounjaro.
Camilla Easter, CEO of Oxford Medical Products, added: “GLP-1 medications perform an important role in helping those with a BMI in the obese range to lose weight and reduce weight-related health risks. There is, however, a real opportunity for a new style of treatment to work in a complementary way to GLP-1s, in a format that is significantly less expensive, and with better tolerability and therefore more accessible for the majority.
“Sirona has demonstrated amazing results during testing with UK hospitals, which have now been externally peer-reviewed. Next, we are setting sights on commercial UK release plans, targeting 2027 to make Sirona available.”
Sirona is a dual-polymer hydrogel pill. That means it’s made from two types of safe materials that expand in the stomach. It doesn’t use drugs or chemicals to change how your body works.
The pill was well tolerated during the 24-week study. There were no serious adverse events. Participants lost up to 13.5% of their body weight in just 24 weeks, and individuals with class 1 obesity (BMI 30-35) lost 6.4% of their body weight on average.
Importantly, no serious adverse events were reported during the trial. Sirona was well tolerated (95 percent of patients adhered to the dosing regimen at 12 weeks) and demonstrated a fantastic safety and side effect profile. This makes Sirona appropriate for patients who have struggled with adverse side effects when using GLP-1 medications.
OMP is planning a pivotal study in the UK and USA to further assess the effectiveness of Sirona and confirm these results. The novel weight loss treatment will aim for a 2027 UK commercial launch.
Source: University of Bristol