South Africa, March 6, 2025 –The Africa Centres for Disease Control and Prevention (Africa CDC) and Illumina (NASDAQ: ILMN), a global leader in sequencing technology, strengthen their collaboration to advance the Africa Pathogen Genomics Initiative (Africa PGI).
The renewed commitment builds on existing efforts over the last 4 years to address COVID-19 and other infectious disease outbreaks, as well as tackle emerging public health threats and endemic diseases like tuberculosis, malaria, and cholera.
Together, both organisations are focused on broadening access to next-generation sequencing (NGS) tools and expertise and enhancing public health surveillance and laboratory networks across Africa.
“Africa CDC is pleased to continue its collaboration with Illumina and other partners to enhance Africa’s capacity to detect and respond to emerging health threats. Genomics is transforming disease surveillance, and this collaboration will help integrate next-generation sequencing into routine public health systems. Our goal remains clear – by the end of 2025, all 55 National Public Health Institutes (NPHIs) will have operational NGS capacity to better protect Africa’s health.” said H.E. Dr. Jean Kaseya, Director-General, Africa CDC.
Since the inception of this collaboration in March 2021, Illumina has provided significant contributions, including next-generation sequencing (NGS) platforms, reagents, and training support. As a part of this association, additional sequencing instruments and reagents will be provided to around 25 countries.
“At Illumina, we are driven by the power of genomics to positively impact the world and are deeply committed to improving global health. By expanding access to cutting-edge sequencing technologies, we are helping to create a future where every country can rapidly detect and respond to health threats. Our association with Africa CDC brings us closer to a world where genomics is integrated into routine public health surveillance – enabling faster, more effective responses to disease outbreaks and ultimately saving lives.” said Belinda Ngongo, Director Global Health, Illumina.
Launched in October 2020, Africa PGI is a flagship initiative of Africa CDC designed to enhance public health surveillance systems across the continent. The program focuses on integrating pathogen genomics and bioinformatics into routine public health efforts, allowing for rapid responses to infectious disease threats, enhanced control and prevention, and the development of more effective diagnostics, treatments, and vaccines. This work will further Africa PGI’s vision of building a resilient, integrated, proactive, and sustainable molecular diagnostic, genomic surveillance, and epidemiology ecosystem across Africa.
An expanded clinical trial that tested a ground-breaking, experimental stem cell treatment for blinding cornea injuries found the treatment was feasible and safe in 14 patients who were treated and followed for 18 months, and there was a high proportion of complete or partial success. The results of this new phase 1/2 trial are published in Nature Communications.
The treatment, called cultivated autologous limbal epithelial cells (CALEC), was developed at Mass Eye and Ear, a member of the Mass General Brigham healthcare system. The innovative procedure consists of removing stem cells from a healthy eye with a biopsy, expanding them into a cellular tissue graft in a novel manufacturing process that takes two to three weeks, and then surgically transplanting the graft into the eye with a damaged cornea.
“Our first trial in four patients showed that CALEC was safe and the treatment was possible,” said principal investigator Ula Jurkunas, MD, associate director of the Cornea Service at Mass Eye and Ear and professor of Ophthalmology at Harvard Medical School. “Now we have this new data supporting that CALEC is more than 90% effective at restoring the cornea’s surface, which makes a meaningful difference in individuals with cornea damage that was considered untreatable.”
Researchersshowed CALEC completely restored the cornea in 50% of participants at their 3-month visit and that rate of complete success increased to 79% and 77% at their 12- and 18-month visits, respectively.
With two participants meeting the definition of partial success at 12 and 18 months, the overall success of CALEC was 93% and 92% at 12 and 18 months. Three participants received a second CALEC transplant, one of whom reached complete success by the study end visit. An additional analysis of CALEC’s impact on vision showed varying levels of improvement of visual acuity in all 14 CALEC patients.
CALEC displayed a high safety profile, with no serious events occurring in either the donor or recipient eyes. One adverse event, a bacterial infection, occurred in one participant, eight months after the transplant due to chronic contact lens use. Other adverse events were minor and resolved quickly following the procedures.
CALEC remains an experimental procedure and is currently not offered at Mass Eye and Ear or any U.S. hospital, and additional studies will be needed before the treatment is submitted for federal approval.
The cornea is the clear, outermost layer of the eye. It’s outer border, the limbus, contains a large volume of healthy stem cells called limbal epithelial cells, which maintain the eye’s smooth surface. When a person suffers a cornea injury, such as a chemical burn, infection or other trauma, it can deplete the limbal epithelial cells, which can never regenerate. The resulting limbal stem cell deficiency renders the eye with a permanently damaged surface where it can’t undergo a corneal transplant, the current standard of care for vision rehabilitation. People with these injuries often experience persistent pain and visual difficulties.
This need led Jurkunas as a junior scientist and Dana, director of the Cornea Service at Mass Eye and Ear, to explore a new approach for regenerating limbal epithelial cells. Nearly two decades later, following preclinical studies and collaborations with researchers at Dana-Farber and Boston Children’s, it was possible to consistently manufacture CALEC grafts that met stringent quality criteria needed for human transplantation.
As an autologous therapy, one limitation of this approach is that it is necessary for the patient to have only one involved eye so a biopsy can be performed to get starting material from the unaffected normal eye.
“Our future hope is to set up an allogeneic manufacturing process starting with limbal stem cells from a normal cadaveric donor eye,” said Ritz “This will hopefully expand the use of this approach and make it possible to treat patients who have damage to both eyes.”
By Mthobisi Kgathi, Business Development Manager – Health & Retail Solutions, BCX
South Africa’s pharmacy sector is at a crossroads, navigating regulatory pressures, patient expectations, and the rapid shift to digital healthcare. While innovation promises efficiency and improved patient outcomes, stability remains critical—without it, even the most advanced technologies can fail.
Pharmacies are a cornerstone of South Africa’s healthcare system, providing essential medicines and bridging the gap between doctors and patients. As the industry embraces digitalisation, it must balance progress with reliability, accuracy, and compliance.
Challenges Facing Community Pharmacies
Community pharmacies operate in a competitive environment where operational reliability and strict regulatory adherence are non-negotiable. Key challenges include:
Regulatory Compliance: The South African Pharmacy Council (SAPC) enforces stringent rules on record-keeping, patient confidentiality, and dispensing protocols. Non-compliance risks fines, reputational damage, or closure.
Workforce Strain: Pharmacists face mounting workloads, managing high prescription volumes while maintaining care standards. Digital tools must ease their burden, not add to it.
Cybersecurity Risks: With sensitive patient data stored digitally, pharmacies are prime targets for cyberattacks. Breaches can lead to legal and financial repercussions.
Evolving Patient Expectations: Patients now demand more than just medication—they want advisory services, chronic disease management, and digital conveniences like e-prescriptions and tele-pharmacy.
These factors underscore the need for cutting-edge yet resilient technology that enhances operations without disrupting care.
A Day in the Life of a Pharmacist
Maria, a pharmacist in Cape Town, exemplifies the balancing act required in modern pharmacies. Her day begins early, managing prescriptions and patient queries. Her pharmacy recently adopted an AI-powered system to streamline stock management, predict patient needs, and track prescriptions.
While the technology improves efficiency, Maria feels the pressure of ensuring it doesn’t compromise accuracy. A system alert about a potential drug interaction highlights how technology can be a vital ally in safeguarding patient health. Yet, Maria knows her community values her expertise and judgement above all.
For pharmacies like Maria’s, successful digitalisation means integrating technology seamlessly into daily operations—enhancing efficiency, improving patient care, and maintaining trust.
Why Stability is Crucial in Digital Transformation
Digital transformation is essential but must be approached cautiously. Unstable or poorly integrated systems can lead to errors, downtime, and non-compliance. Stability ensures that innovation supports, rather than disrupts, core pharmacy functions.
For South African pharmacies, stability means:
Consistent Performance: Systems must function reliably to avoid disruptions in dispensing and patient care.
Regulatory Alignment: Digital solutions must keep pace with compliance requirements to prevent legal issues.
Interoperability: Pharmacy systems should integrate smoothly with healthcare providers, insurers, and supply chains.
Data Security: Protecting sensitive patient information is paramount, requiring robust cybersecurity measures.
The Role of Technology Providers
Technology providers must prioritise stability alongside innovation. Their goal should be to create scalable, compliant solutions that enhance pharmacy operations without compromising reliability.
Pharmacy management systems have already improved stock control, reporting, and dispensing accuracy. The next phase involves incorporating predictive analytics, AI-driven efficiencies, and cloud-based solutions—all while ensuring uninterrupted service.
Take Unisolv, a widely used software in South African pharmacies. Known for its reliability, its upcoming modernisation aims to maintain operational continuity while introducing new functionalities. This approach balances innovation with the familiarity and dependability pharmacy staff rely on.
Beyond Unisolv, BCX is expanding its pharmacy solutions portfolio, focusing on workflow automation, data security, and patient engagement. From AI-driven prescription analysis to cloud-based compliance tracking, BCX is shaping the future of pharmacy technology with stability at its core.
Strategic Considerations for the Future
To ensure sustainable digital transformation, South African pharmacies must adopt a long-term, strategic approach:
Phased Rollouts: Gradual implementation minimises disruption and allows teams to adapt.
Comprehensive Training: Staff must be equipped to maximise the potential of new systems.
Vendor Partnerships: Technology providers should act as long-term partners, not just suppliers.
Data-Driven Insights: Analytics can optimise stock levels, predict demand, and personalise patient care.
The Way Forward
As community pharmacies play a vital role in accessible healthcare, technological advancements must empower rather than disrupt their services. Stability is the foundation of this evolution, ensuring that innovations are seamlessly integrated without jeopardising reliability.
Technology providers must focus on creating solutions that are secure, practical, and sustainable. Success will not only be defined by what is new but also by what remains trusted and indispensable.
By embedding resilience into digital strategies, South African pharmacies can confidently embrace the future—leveraging technology to enhance care while safeguarding the principles of trust, accuracy, and compliance. Stability ensures that pharmacies can continue serving their communities effectively, even as they adopt new tools to meet evolving demands.
In the end, the balance between innovation and stability will determine the success of digital transformation in South Africa’s pharmacy sector.
A new USC Leonard Davis School of Gerontology study suggests greater exposure to extreme heat may accelerate biological aging in older adults, raising new concerns about how climate change and heat waves could affect long-term health and aging at the molecular level.
People in neighbourhoods that experience more days of high heat show greater biological aging on average than residents of cooler regions, said Jennifer Ailshire, senior author of the study, which appears in Science Advances. Ailshire is professor of gerontology and sociology at the USC Leonard Davis School.
Biological age is a measure of how well the body functions at the molecular, cellular, and system levels, as opposed to chronological age based on one’s birthdate; having a biological age greater than one’s chronological age is associated with higher risk for disease and mortality. While exposure to extreme heat has itself long been associated with negative health outcomes, including increased risk of death, heat’s link to biological aging has been unclear.
Measuring epigenetic changes
Ailshire and her coauthor Eunyoung Choi, USC Leonard Davis PhD in Gerontology alumna and postdoctoral scholar, examined how biological age changed in more than 3600 Health and Retirement Study (HRS) participants aged 56 and older from throughout the U.S. Blood samples taken at various time points during the six-year study period were analysed for epigenetic changes, or changes in the way individual genes are turned “off” or “on” by a process called DNA methylation.
The researchers used mathematical tools called epigenetic clocks to analyse methylation patterns and estimate biological ages at each time point. They then compared participants’ changes in biological age to their location’s heat index history and number of heat days reported by the National Weather Service from 2010 to 2016.
The National Weather Service Heat Index Chart categorises heat index values into three levels based on the potential risk of adverse health effects. The “Caution” level includes heat index values ranging from 80°F (27°C) to 90°F (32°C), the “Extreme Caution” level includes values between 90°F (32°C) and 103°F (34°C), and the “Danger” level includes values between 103°F (34°C) and 124°F (51°C). Days in all three levels were included as heat days in the study.
The analysis revealed a significant correlation between neighbourhoods with more days of extreme heat and individuals experiencing greater increases in biological age, Choi said. This correlation persisted even after controlling for socioeconomic and other demographic differences, as well as lifestyle factors such as physical activity, alcohol consumption and smoking, she added.
“Participants living in areas where heat days, as defined as Extreme Caution or higher levels (32°C), occur half the year, such as Phoenix, Arizona, experienced up to 14 months of additional biological aging compared to those living in areas with fewer than 10 heat days per year,” she said. “Even after controlling for several factors, we found this association. Just because you live in an area with more heat days, you’re aging faster biologically.”
All three epigenetic clocks employed in the study – PCPhenoAge, PCGrimAge, and DunedinPACE – revealed this association when analysing epigenetic aging over a 1- to 6-year period. PCPhenoAge also showed the association after short (7 days) and medium (30-60 days) periods of time, indicating that heat-related epigenetic changes could happen relatively quickly, and some of them may accumulate over time.
Climate implications for communities
Older adults are particularly vulnerable to the effects of high heat, Ailshire said. She noted that the study used heat index, rather than just air temperature, to take relative humidity into account as they analyzed results.
“It’s really about the combination of heat and humidity, particularly for older adults, because older adults don’t sweat the same way. We start to lose our ability to have the skin-cooling effect that comes from that evaporation of sweat,” she explained. “If you’re in a high humidity place, you don’t get as much of that cooling effect. You have to look at your area’s temperature and your humidity to really understand what your risk might be.”
The next steps for the researchers will be to determine what other factors might make someone more vulnerable to heat-related biological aging and how it might connect to clinical outcomes. In the meantime, the study results could also prompt policymakers, architects, and others to keep heat mitigation and age-friendly features in mind as they update cities’ infrastructure, from placing sidewalks and building bus stops with shade in mind to planting more trees and increasing urban green space, Ailshire said.
“If everywhere is getting warmer and the population is aging, and these people are vulnerable, then we need to get really a lot smarter about these mitigation strategies,” she said.
A new study led by researchers at Mass General Brigham suggests a nasal spray developed to target neuroinflammation could one day be an effective treatment for traumatic brain injury (TBI). By studying the effects of the nasal anti-CD3 in a mouse model of TBI, researchers found the spray could reduce damage to the central nervous system and behavioural deficits, suggesting a potential therapeutic approach for TBI and other acute forms of brain injury. The results are published in Nature Neuroscience.
“Traumatic brain injury is a leading cause of death and disability – including cognitive decline – and chronic inflammation is one of the key reasons,” said lead author Saef Izzy, MD, FNCS, FAAN, a neurologist and head of the Immunology of Brain Injury Program at Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system. “Currently, there is no treatment to prevent the long-term effects of traumatic brain injury.”
The study examines the monoclonal antibody Foralumab, made by Tiziana, which has been tested in clinical trials for patients with multiple sclerosis, Alzheimer’s disease, and other conditions.
“This opens up a whole new area of research and treatment in traumatic brain injury, something that’s almost impossible to treat,” said senior author Howard Weiner, MD, co-director of the Ann Romney Center for Neurologic Diseases at Brigham and Women’s Hospital. “It also means this could work in intracerebral hemorrhage and other stroke patients with brain injury.”
Multiple experiments were done in mouse models with moderate-to-severe traumatic brain injury to explore the communication between regulatory cells induced by the nasal treatment and the microglial immune cells in the brain. Over time, researchers were able to identify how they modulate immune response.
“Modulating the neuroinflammatory response correlated with improved neurological outcomes, including less anxiety, cognitive decline, and improved motor skills,” Izzy said.
In addition to assessing the effects of the treatment, the research team was able to learn about immune response over time and compare the immune responses and effects of TBI in the mice.
The next step in the research is to translate the findings from preclinical models to human patients.
“Our patients with traumatic brain injury still don’t have an effective therapeutic to improve their outcomes, so this is a very promising and exciting time to move forward with something that’s backed up with solid science and get it to patients’ bedsides,” said Izzy.
Once in the clinical setting, Weiner said the hope is this treatment could be used on a variety of traumatic brain injury patients, including football players with repetitive concussions.
“We envision giving a nasal spray right there on the sidelines,” said Weiner. “It isn’t something we can do yet, but we see the potential.”
Scientists have uncovered the mechanism behind how aspirin could reduce the metastasis of some cancers by stimulating the immune system.
In the study published in Nature, the scientists say that discovering the mechanism will support ongoing clinical trials, and could lead to the targeted use of aspirin to prevent the spread of susceptible types of cancer and the development of more effective drugs to prevent cancer metastasis.
The scientists caution that aspirin can have serious side effects and that trials are underway to establish safety and efficacy.
A reduction in the spread of some cancers
Studies of people with cancer have previously observed that those taking daily low-dose aspirin have a reduction in the spread of some cancers, such as breast, bowel, and prostate cancers, leading to ongoing clinical trials. However, until now it wasn’t known exactly how aspirin could prevent metastases.
In this study, led by researchers at the University of Cambridge, the scientists say their discovery of how aspirin reduces cancer metastasis was serendipitous.
They were investigating the process of metastasis, because, while cancer starts out in one location, 90% of cancer deaths occur when cancer spreads to other parts of the body.
Lung cancer metastasis. Credit: National Cancer Institute
The scientists wanted to better understand how the immune system responds to metastasis. This is because when individual cancer cells break away from their originating tumour and spread to another part of the body, they are particularly vulnerable to immune attack.
An effect on cancer metastasis
The immune system can recognise and kill these lone cancer cells more effectively than cancer cells within larger originating tumours, which have often developed an environment that suppresses the immune system.
The researchers previously screened 810 genes in mice and found 15 that had an effect on cancer metastasis. In particular, they found that mice lacking a gene that produces a protein called ARHGEF1 had less metastasis of various primary cancers to the lungs and liver.
The researchers determined that ARHGEF1 suppresses T cells, which can recognise and kill metastatic cancer cells.
To find a suitable drug, the scientists traced signals in the cell to determine that ARHGEF1 is switched on when T cells are exposed to a clotting factor called thromboxane A2 (TXA2).
This was an unexpected revelation for the scientists, because TXA2 is already well-known and linked to how aspirin works.
Reduces the production of TXA2
TXA2 is produced by platelets; aspirin reduces the production of TXA2, leading to the anti-clotting effects, which underlies its ability to prevent heart attacks and strokes.
This new research found that aspirin prevents cancers from spreading by decreasing TXA2 and releasing T cells from suppression. They used a mouse model of melanoma to show that in mice given aspirin, the frequency of metastases was reduced compared to control mice, and this was dependent on releasing T cells from suppression by TXA2.
Despite advances in cancer treatment, many patients with early stage cancers receive treatments, such as surgical removal of the tumour, which have the potential to be curative, but later relapse due to the eventual growth of micrometastases – cancer cells that have seeded other parts of the body but remain in a latent state.
Most immunotherapies are developed to treat patients with established metastatic cancer, but when cancer first spreads there’s a unique therapeutic window of opportunity when cancer cells are particularly vulnerable to immune attack.
We hope that therapies that target this window of vulnerability will have tremendous scope in preventing recurrence in patients with early cancer at risk of recurrence.
More accessible globally
Dr Jie Yang, who carried out the research, at the University of Cambridge, said:
It was a Eureka moment when we found TXA2 was the molecular signal that activates this suppressive effect on T cells.
Before this, we had not been aware of the implication of our findings in understanding the anti-metastatic activity of aspirin. It was an entirely unexpected finding which sent us down quite a different path of enquiry than we had anticipated.
Aspirin, or other drugs that could target this pathway, have the potential to be less expensive than antibody-based therapies, and therefore more accessible globally.
In the future, the researchers plan to help the translation of their work into potential clinical practice by collaborating with Professor Ruth Langley, of the MRC Clinical Trials Unit at University College London, who is leading the Add-Aspirin clinical trial, to find out if aspirin can stop or delay early stage cancers from coming back.
Caution on aspirin use
Professor Langley, who was not involved in this study, commented:
This is an important discovery. It will enable us to interpret the results of ongoing clinical trials and work out who is most likely to benefit from aspirin after a cancer diagnosis.
In a small proportion of people, aspirin can cause serious side-effects, including bleeding or stomach ulcers. Therefore, it is important to understand which people with cancer are likely to benefit and always talk to your doctor before starting aspirin.
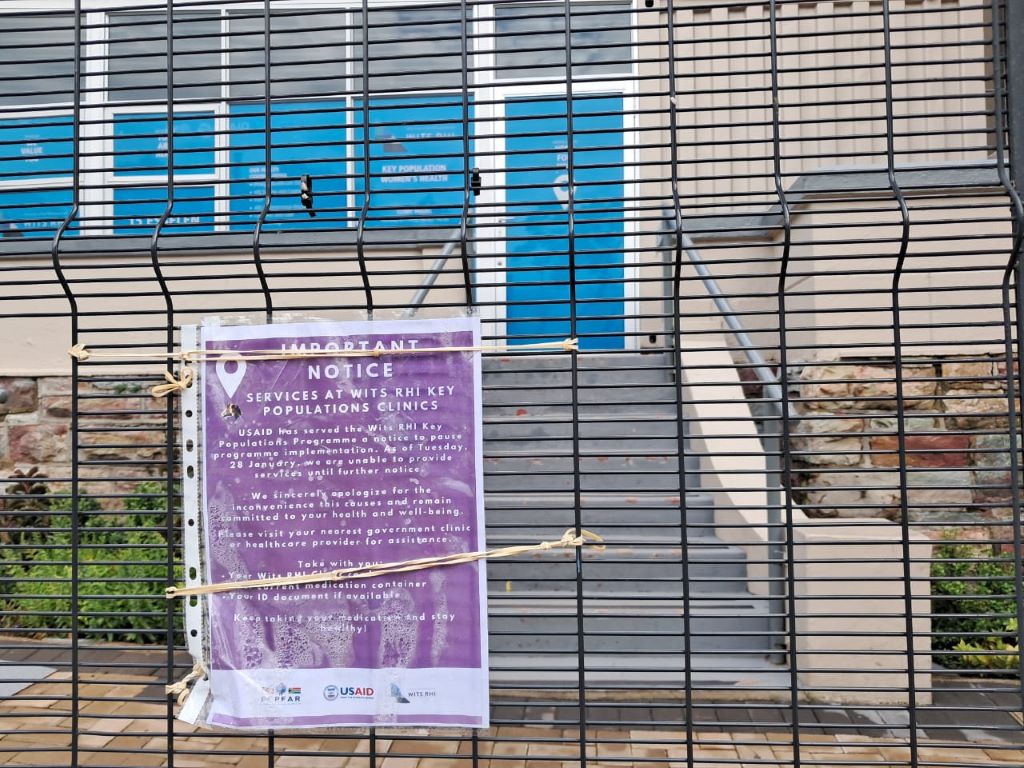
South Africa faces its worst health crisis in 20 years. Worse than COVID, and one that will overshadow diabetes as a major killer, while pouring petrol on a dwindling TB fire. But it is preventable if our government steps up urgently.
Nearly eight-million people have HIV in South Africa; they need life-long antiretroviral medicines to stay healthy.
The near-total removal of US government funding last week, a programme called PEPFAR, will see every important measure of the HIV programme worsen, including hospitalisations, new infections in adults and children, and death. Unless government meaningfully steps in to continue funding the network of highly efficient organisations that currently fill key gaps in national care, an epidemic that was tantalisingly close to coming under control will again be out of our reach. Millions of people in South Africa will become infected with HIV and hundreds of thousands more will die in the next ten years. 2025 will end much more like 2004, when we started our HIV treatment programme.
Many fail to recognize the danger. Commentators, public health officials, and government spokespeople have downplayed the US financial contributions to the HIV response, suggesting services can be absorbed within current services. The funding cuts amount to approximately 17% of the entire budget for HIV and largely go to salaries for health staff. On the face of it, this indeed seems replaceable. So why are the consequences so deadly?
To understand the impact, one must recognize how US funding has supported HIV care. The money is largely allocated to a network of non-government organisations through a competitive, focused, and rigorously monitored program in four key areas:
Active case finding: The best way to prevent new cases of HIV is find everyone with the disease early on, and get them on treatment. These organisations deploy people in high-risk areas, to test for HIV and screen for TB, and shepherd people who test positive to treatment programmes. People are almost always healthy when they start treatment, and remain healthy, with greatly reduced time to transmit the virus, and much less chance of ever “burdening” the health sector with an opportunistic infection. They are hugely cost-effective.
Tracing people who disappear from care: Patients on antiretrovirals fall out of care for many reasons, ranging from changing their address, to life chaos such as losing their job or mental illness. Or they are simply mixed up in the filing dysfunction within clinics. The US supported programmes helped finding people ‘lost from care’, maintaining systems able to track who has not come back, and how to contact them, often spending considerable time cleaning redundant records as people move between facilities.
Vulnerable population programmes: Services include those for sex workers, LGBTQ+ people, adolescents, people who use drugs, and victims of gender violence. These programs are for people who need tailored services beyond the straightforward HIV care offered in state clinics. They are often discriminated against in routine services and also at significant risk of contracting HIV.
Supporting parts of the health system: This includes technical positions supporting medicine supply lines, laboratories and large information systems, as well as organisations doing advocacy or monitoring the quality of services. All of this keeps the health system ticking over.
In central Johannesburg, where I work, HIV testing services have collapsed. The people who fell out of programmes are not coming back. HIV prevention and TB screening have largely stopped.
Reassurances that state clinics will pick up testing are empty – the staff do not exist, and testing has not resumed. State clinics do not trace people who fall out of care for any illness, let alone for HIV. The data systems maintained by PEPFAR-supported organisations are now gone.
What happens now? The first hard sign that things are failing will be a large drop in the number of people starting treatment, versus what happened in the same month one year ago. The next metric to watch will be hospitalisations for tuberculosis and other infections associated with untreated HIV infection. This will happen towards the end of the year, as immune systems fail. Not long after, death rates will rise. We will see that in death certificates among younger people – the parents and younger adults.
Unfortunately, much of this information will not be available to the health department for at least a year or two, because among the staff laid off in this crisis are the data collectors for the programmes that tracked vital metrics.
The above should come as no surprise, especially to the public health commentators and health department, which is why it is so surprising to hear how certain they are that the PEPFAR programme can easily be absorbed into the state services. The timing of this crisis could not be worse, with huge budget holes in provincial health departments.
Why should this be a priority? After starting the HIV programme in 2004, we spent the next few years muddling through how to deliver antiretrovirals to millions of people in primary care, before we realised we also needed to diagnose them earlier. In 2004, the average CD4 count (a measure of immune strength) at initiation of treatment was about 80 cells/ul, devastatingly low – normal is > 500 cells/ul. A quarter were ill with TB.
This CD4 count average took years to go up, but only by pushing testing into clinic queues, communities, and special services for key populations, not waiting till they were sick. Recently, the average initiation CD4 count was about 400 cells/ul, stopping years of transmission, with most people healthy, and only a small number with TB.
There are many reasons to criticise the relationship between PEPFAR and the health department. It suited both parties to have a symbiotic relationship that meant each got on with their job and ticked their respective output boxes, but neither had to tussle with the messiness of trying to move the PEPFAR deliverables into the health department. As we move forward, learning from these fragilities to plan for the future of the HIV care programme, and for other diseases, will be critical.
Since the suspension of funding, many people have said, “We don’t hear much about HIV anymore”. That is because when the system works well, you don’t hear about it. Some things are far better compared to 2004:
We have a government not in denial about HIV being a problem nor encouraging pseudoscience or crackpots.
Our frontline health workers, in over 3000 clinics, have vast experience initiating and maintaining antiretrovirals.
Antiretrovirals are cheaper, more potent, more durable, and safer.
Treatment protocols are simpler.
New infection rates are way down.
Government delivery systems have improved.
Data systems suggest that the majority of ‘lost’ patients are in care, often simply in another clinic.
A sensible emergency plan would do this:
Fund existing programmes for a limited time, understanding that the level of reach and expertise is impossible for the health department to replicate at short notice.
Couple this with a plan to make posts more sustainable over the next year or two.
Learn from the PEPFAR programme that rigorously held organisations accountable, so that provinces can similarly be answerable for their HIV metrics.
Ask hard questions why single patient identifiers, and government information systems, that could easily be linked to laboratory, pharmacy and radiology databases, are still not integrated within the public systems, as they are throughout the private health system.
Accept that certain key functions and clinics may best be sited outside of the health department.
This will not save the large and valuable research programmes, which need other help. Much of the rest of Africa needs a Marshall Plan to rescue their entire HIV service, as they are almost totally dependent on US government funding.
But ideas like the above will preserve the current South African HIV response and allow us to imagine interventions that could end the disease as a threat for future generations.
No one disputes we need a move away from donor-assisted health programmes. But the scale and immense urgency of this oncoming emergency needs to be understood. We need a plan and a budget, and fast. Or we will have an overwhelmed hospital system and busy funeral services again.
Professor Francois Venter works for Ezintsha, a policy and research unit at Wits. He has been involved in the HIV programme since 2001, and ran several large PEPFAR programmes till 2012. Venter and his unit do not receive funding from PEPFAR, USAID or CDC. Thank you to several experts for supplying analysis and ideas for the initial draft of the article.
Neuroblastoma is a solid tumour that occurs in children. When high-risk, the disease has a poor prognosis. Decades ago, adding the drug retinoic acid to neuroblastoma treatment increased survival by 10–15%. However, this effect was only evident in post-chemotherapy consolidation after bulky primary tumours had largely been eliminated. Why retinoic acid is effective in this setting but not against primary tumours, has been speculated about for nearly 50 years.
St. Jude Children’s Research Hospital scientists resolved the mystery in a new study, showing retinoic acid uses a novel mechanism to kill metastasised neuroblastoma. The drug “hijacks” a normal developmental pathway to trigger cancer cell death. The findings, which have implications for future combination therapy approaches, appears in Nature Communications.
“We’ve come up with an explanation for a decades-long contradiction about why retinoic acid works in post-chemotherapy consolidation but has little impact on primary neuroblastoma tumours,” said senior co-corresponding author Paul Geeleher, PhD. “Retinoic acid’s activity heavily depends on the cellular microenvironment.”
The cellular microenvironment is the soup of chemicals, proteins and other signals that surround a cell, and which is unique to that part of the body. For example, the bone marrow microenvironment contains signals to grow blood cells and restructure bone. Metastasised neuroblastoma cells often migrate to bone marrow, where the bone morphogenetic protein (BMP) pathway signalling is highly active. The researchers showed that BMP signaling makes neuroblastoma cells much more vulnerable to retinoic acid.
“Unexpectedly, we found that cells expressing genes from the BMP signaling pathway were very sensitive to retinoic acid,” said co-first and co-corresponding author Min Pan, PhD, St. Jude Department of Computational Biology. “However, since the bone marrow microenvironment causes neuroblastoma cells there to have higher BMP activity, it neatly explained why retinoic acid is very effective at treating those cells during consolidation therapy, but not the primary tumours during up-front treatment.”
Hijacking development to drive metastatic neuroblastoma cell death
Using gene editing technology, the scientists uncovered the relationship between BMP signaling and retinoic acid. They assembled a group of neuroblastoma cell lines susceptible to retinoic acid, then cut out genes to find which were responsible for the drug’s activity. Genes in the BMP pathway had the largest effect while providing a plausible explanation for retinoic acid’s varying outcomes in patients.
“We found that, in neuroblastoma, BMP signaling works with retinoic acid signaling in the same way as during development,” said co-first author Yinwen Zhang, PhD, who characterised how transcription factors, the proteins that bind DNA to regulate gene expression, led to different results in highly retinoic acid-sensitive or insensitive neuroblastoma cells. “If there are a lot of BMP-signaling pathway transcription factors already on DNA, then retinoic acid signaling combines with it to promote downstream cell death–related gene expression. This occurs both in normal embryonic development and neuroblastoma cells in certain microenvironments.”
“We are the first to uncover such an example of ‘hijacking’ a normal embryonic developmental process preserved in cancer that we can exploit therapeutically,” Geeleher said. “Now, we can look for similar processes in other diseases to design less toxic and more effective treatment strategies.”
Gut microbes that were thought to feed exclusively on dietary fibre also get fed sugar from our guts, from which they produce short-chain fatty acids that are crucial to many body functions. The Kobe University discovery of this symbiotic relationship also points the way to developing novel therapeutics.
Gut microbes produce many substances that our body needs but cannot produce itself. Among them are short-chain fatty acids that are the primary energy source for the cells lining our guts but have other important roles, too, and that are thought to be produced by bacteria who feed on undigested fibre. However, in a previous study, the Kobe University endocrinologist Ogawa Wataru found that people who take the diabetes drug metformin excrete the sugar glucose to the inside of their guts. He says: “If glucose is indeed excreted into the gut, it is conceivable that this could affect the symbiotic relationship between the gut microbiome and the host.”
Ogawa and his team set out to learn more about the details of the glucose excretion and its relationship with the gut microbiota. “We had to develop unprecedented bioimaging methods and establish novel analytical techniques for the products of the gut microbial metabolism,” he says. They used their new methods to not only see where and how much glucose enters the guts, but also used mouse experiments to find out how the sugar is transformed after that. In addition, they also checked how the diabetes drug metformin influences these results both in humans and in mice.
The Kobe University team now published their results in the journal Communications Medicine. They found that, first, glucose is excreted in the jejunum and is transported from there inside the gut to the large intestine and the rectum. “It was surprising to find that even individuals not taking metformin exhibited a certain level of glucose excretion into the intestine. This finding suggests that intestinal glucose excretion is a universal physiological phenomenon in animals, with metformin acting to enhance this process,” Ogawa explains. In both humans and mice, irrespective of whether they were diabetic or not, metformin increased the excretion by a factor of almost four.
And second, on the way down, the glucose gets transformed into short-chain fatty acids. Ogawa says: “The production of short-chain fatty acids from the excreted glucose is a huge discovery. While these compounds are traditionally thought to be produced through the fermentation of indigestible dietary fibres by gut microbiota, this newly identified mechanism highlights a novel symbiotic relationship between the host and its microbiota.”
Ogawa and his team are now conducting further studies with the aim of understanding how metformin and other diabetes drugs affect glucose excretion, the gut microbiome and their metabolic products. He says: “Intestinal glucose excretion represents a previously unrecognised physiological phenomenon. Understanding the underlying molecular mechanisms and how drugs interfere with this process could lead to the development of novel therapeutics aimed at the regulation of gut microbiota and their metabolites.”
Rutgers Health researchers have made discoveries about brown fat that may open a new path to helping people stay physically fit as they age. A team from Rutgers New Jersey Medical School found that mice lacking a specific gene developed an unusually potent form of brown fat tissue that expanded lifespan and increased exercise capacity by roughly 30%. The team is working on a drug that could mimic these effects in humans.
“Exercise capacity diminishes as you get older, and to have a technique that could enhance exercise performance would be very beneficial for healthful aging,” said Stephen Vatner, university professor and director of the Cardiovascular Research Institute in the medical school’s Department of Cell Biology and Molecular Medicine and senior author of the study in Aging Cell. “This mouse model performs exercise better than their normal littermates.”
Unlike white fat, which stores energy, brown fat burns calories and helps regulate body temperature. This study revealed brown fat also plays a crucial role in exercise capacity by improving blood flow to muscles during physical activity.
The genetically modified mice produced unusually high amounts of active brown fat and showed about 30% better exercise performance than normal mice, both in speed and time to exhaustion.
The discovery emerged from broader research into healthy aging. The modified mice, which lack a protein called RGS14, live about 20% longer than normal mice, with females living longer than males – similar to the pattern seen in humans. Even at advanced ages, they maintain a healthier appearance, avoiding the typical signs of aging, such as loss of hair and graying that appear in normal elderly mice. Their brown adipose tissue also protects them from obesity, glucose intolerance, cardiovascular disorders, cancer and Alzheimer’s disease, in addition to reduced exercise tolerance.
To test whether the brown fat – rather than some other result from the missing genes –accounted for the benefits, the researchers transplanted the brown fat to normal mice. They noted that the recipients gained similar benefits within days. Transplants using regular brown fat from normal mice, by contrast, took eight weeks to produce much milder improvements.
The discovery could eventually improve human lifespans – the total time when people enjoy good mental and physical health.
“With all the medical advances, aging and longevity have increased in humans, but unfortunately, healthful aging hasn’t,” Vatner said. “There are a lot of diseases associated with aging – obesity, diabetes, myocardial ischemia, heart failure, cancer – and what we have to do is find new drugs based on models of healthful aging.”
Rather than develop a treatment that addresses aging broadly, which poses regulatory challenges, Vatner said his team plans to test for specific benefits such as improved exercise capacity and metabolism. This approach builds on their previous success in developing a drug based on a different mouse healthful longevity model.
“We’re working with some people to develop this agent, and hopefully, in another year or so, we’ll have a drug that we can test,” Vatner said.
In the meantime, techniques such as deliberate cold exposure can increase brown fat naturally. Studies have found such efforts to produce short-term benefits that range from enhanced immune system function to improved metabolic health, but Vatner said none of the studies have run long enough to find any effect on healthful aging.
He added that most people would prefer to increase brown fat levels by taking pills rather than ice baths and is optimistic about translating the newest finding into an effective medication.