This illustration depicts a 3D computer-generated image of a group of Gram-positive, Streptococcus pneumoniae bacteria. The artistic recreation was based upon scanning electron microscopic (SEM) imagery. Credit: CDC on Unsplash
In a recent multicentre prospective study conducted at three hospitals in Tennessee and Georgia, including Vanderbilt University Medical Center, researchers at VUMC found a substantial burden of hospitalisations for community-acquired pneumonia (CAP) among adults.
Community-acquired pneumonia refers to a case of the disease contracted without prior exposure to a health care setting, otherwise known as hospital-acquired pneumonia (HAP).
The study, published in JAMA Network Open, included data from 2018 to 2022 and used a novel serotype-specific urinary test that can identify infections caused by 30 different Streptococcus pneumoniae serotypes. A serotype refers to a distinct strain of microorganism, such as bacteria.
An important aspect of the study was the identification of noninvasive pneumococcal infections, said Carlos Grijalva, MD, MPH, professor of Health Policy and Biomedical Informatics and the study’s lead author.
“Standard clinical diagnostic methods such as bacterial cultures of blood are helpful for identifying invasive cases of pneumococcal disease, but the majority of pneumococcal pneumonias are thought to be noninvasive,” Grijalva added. “Using a novel and more sensitive urinary antigen detection method allowed us to identify a number of pneumococcal infections that may have otherwise passed unrecognised.”
Based on current population estimates, some 114 800 U.S. adults may be hospitalised for pneumococcal pneumonia each year, a figure made up in large part by older adults. And according to the study’s findings, each year sees approximately 340 hospitalisations for community-acquired pneumonia per 100 000 adults, approximately 14% of which had evidence of Streptococcus pneumoniae infection.
“Our study results show that Streptococcus pneumoniae remains an important cause of severe community-acquired pneumonia,” said Wesley Self, MD, MPH, professor of Emergency Medicine, Senior Vice President for Clinical Research and the paper’s senior author.
Many of the serotypes identified by pneumococcal detections corresponded with those covered by a recently licensed adult-specific pneumococcal conjugate vaccine, V116, which includes 21 serotypes but was not commercially available during the study period.
“Vaccines with coverage of additional pneumococcal serotypes could be quite beneficial in lessening the burden of severe pneumonia on the U.S. population, especially among older adults,” added Self, who holds the Directorship in Emergency Care Research.
For decades, medical professionals debated whether a common antiviral medication used to treat flu in children caused neuropsychiatric events or if the infection itself was the culprit.
Now researchers at Monroe Carell Jr. Children’s Hospital at Vanderbilt have debunked a long-standing theory about oseltamivir, known as Tamiflu.
According to the study, published in JAMA Neurology, oseltamivir treatment during flu episodes was associated with a reduced risk of serious neuropsychiatric events, such as seizures, altered mental status and hallucination.
“Our findings demonstrated what many pediatricians have long suspected, that the flu, not the flu treatment, is associated with neuropsychiatric events,” said principal investigator James Antoon, MD, PhD, MPH, assistant professor of Pediatrics in the Division of Pediatric Hospital Medicine at Monroe Carell. “In fact, oseltamivir treatment seems to prevent neuropsychiatric events rather than cause them.”
Key points:
Influenza itself was associated with an increase in neuropsychiatric events compared to children with no influenza, regardless of oseltamivir use.
Among children with influenza, those treated with oseltamivir had about 50% reduction in neuropsychiatric events.
Among children without influenza, those who were treated with oseltamivir prophylactically had the same rate of events as the baseline group with no influenza.
“Taken together, these three findings do not support the theory that oseltamivir increases the risk of neuropsychiatric events,” said Antoon. “It’s the influenza.”
The team reviewed the de-identified data from a cohort of children and adolescents ages 5-17 who were enrolled in Tennessee Medicaid between July 1, 2016, and June 30, 2020.
During the four-year period, 692 295 children, with a median age of 11 years, were included in the study cohort. During follow-up, study children experienced 1230 serious neuropsychiatric events (898 neurologic and 332 psychiatric).
The clinical outcomes definition included both neurologic (seizures, encephalitis, altered mental status, ataxia/movement disorders, vision changes, dizziness, headache, sleeping disorders) and psychiatric (suicidal or self-harm behaviours, mood disorders, psychosis/hallucination) events.
“The 2024-2025 influenza season highlighted the severity of influenza-associated neurologic complications, with many centres reporting increased frequency and severity of neurologic events during the most recent season,” said Antoon. “It is important for patients and families to know the true risk-benefit profile of flu treatments, such as oseltamivir, that are recommended by the American Academy of Pediatrics.”
“These flu treatments are safe and effective, especially when used early in the course of clinical disease,” added senior author Carlos Grijalva, MD, MPH, professor of Health Policy and Biomedical Informatics at Vanderbilt University Medical Center.
Investigators hope the findings will provide reassurance to both caregivers and medical professionals about the safety of oseltamivir and its role in preventing flu-associated complications.
A UK trial involving 16 500 mechanically ventilated intensive care unit (ICU) patients found no 90-day survival benefit for conservative supplemental oxygen over usual oxygen therapy. Nevertheless, the study, published in JAMA, did demonstrate the accuracy and cost-effectiveness of conducting a large trial with a simple intervention.
Oxygen is one of the most commonly administered treatments to patients in ICUs, but liberal oxygen therapy to avoid the risks of hypoxaemia may lead to harm, so finding the right level could optimise outcomes. Trials to date have shown mixed results.
For COVID patients admitted to the ICU with severe hypoxaemia, survival without life support was extended with conservative oxygen therapy. In a paediatric ICU study, conservative oxygen therapy resulted in a reduction in a composite of organ support at 30 days or death. A meta-analysis of 13 trials showed no differences between liberal and conservative oxygen therapy.
Even with just a small difference in survival benefit, with tens of millions of patients mechanically ventilated in the ICU would still mean significant numbers of lives saved. Other tests of new drugs and procedures in the ICU are hampered by high cost, as Seitz et al. noted in an accompanying editorial, so this sort of trial comparing two approaches to a common therapy is much more affordable.
The UK Intensive Care Unit Randomised Trial Comparing Two Approaches to Oxygen Therapy (UK-ROX) trial was initiated to determine if there was a difference between conservative and usual oxygen therapy.
The trial randomised 16 500 patients across 97 ICUs in the UK to either conservative oxygen therapy or usual oxygen therapy, in adults receiving mechanical ventilation and supplemental oxygen in the ICU. The primary outcome was mortality at 90 days. Conservative oxygen therapy targeted a peripheral oxygen saturation (Spo2) of 90% (range, 88%-92%), while usual oxygen therapy was at the discretion of the treating clinician.
Patients were early in mechanical ventilation (median, 5 hours), were severely ill (median predicted mortality risk, 35%), had a range of critical illnesses (eg, > 5000 patients with sepsis and > 1500 patients with hypoxic-ischaemic encephalopathy) and with significant hypoxaemia (eg, > 11 000 patients with a Pao2:Fio2 ratio, consistent with acute respiratory distress syndrome). Obtaining informed consent from the patients was, of course, largely not feasible, so this requirement was waived for the study.
Exposure to supplemental oxygen was 29% lower for those in the conservative oxygen therapy group compared with the usual oxygen therapy group. Of the patients randomised to conservative oxygen therapy, 35.4% died by 90 days compared with 34.9% of patients receiving usual oxygen therapy.
No differences were seen for secondary outcomes, including ICU stay, days free of life support and mortality at various time points. No interactions for confirmed or suspected COVID, ethnicity or other illnesses were observed.
Post hoc analysis showed weak evidence of increased harm from conservative oxygen therapy among the first 10 patients in each site but no difference for the random enhanced data collection sample compared with standard data collection.
Seitz et al. pointed out that the high level of adherence to the conservative target resulted in a mean oxygen saturation of 93.3%, versus 95.1% for usual care. The differences in oxygen saturation (1.9%) and Fio2 (0.04) between the trial groups in UK-ROX were about half the magnitude of some prior trials, due to not aiming for widely separated targets, and usual care varies considerably depending on location and clinical considerations.
Therefore, the researchers concluded that the findings do not support an approach of reducing oxygen exposure by targeting an Spo2 of 90% in mechanically ventilated adults receiving oxygen in the ICU. They suggest that future research may involve using AI to determine specific situations where conservative or liberal oxygen therapy may have beneficial outcomes.
References:
Martin DS, Gould DW, Shahid T, et al. Conservative Oxygen Therapy in Mechanically Ventilated Critically Ill Adult Patients: The UK-ROX Randomized Clinical Trial. JAMA. 2025;334(5):398–408. doi:10.1001/jama.2025.9663
Seitz KP, Casey JD, Semler MW. Patient, Treatment, Outcome—Large Simple Trials of Common Therapies. JAMA. 2025;334(5):395–397. doi:10.1001/jama.2025.9657
Trained immunity – a process being explored in vaccine and therapy development to boost immune defences – appears to be counterproductive in certain contexts, researchers at McGill University and the Research Institute of the McGill University Health Centre (The Institute) have found.
Trained immunity is when the body’s first line of defence remembers past threats and becomes more reactive, responding more strongly to future infections even if they are different, by changing immune cells’ behaviour.
In an earlier study, the researchers had determined beta-glucan, a molecule found in the cell walls of fungi like yeast and mushrooms, can reduce lung damage during influenza infection. That study had focused on beta-glucan’s impact on neutrophils.
However, in a new study, published in the journal eLife, the team found exposure to beta-glucan can reprogram alveolar macrophages in a way that worsens lung damage during severe inflammation caused by viral or bacterial products. These cells help keep the lungs clean by clearing out dust, debris and pathogens.
“To date, most trained immunity research has focused on circulating immune cells that arise from the bone marrow,” said lead author Renaud Prével, a postdoctoral fellow at the Meakins-Christie Laboratories at The Institute. “We wanted to explore whether beta-glucan could induce trained immunity in alveolar macrophages, and whether that might be helpful or harmful.”
The researchers exposed mice to beta-glucan, which is known to trigger trained immunity and is found in some health supplements. A week later, the mice were exposed to signals that mimic severe viral or bacterial infections with sepsis-like phenotype. Using high-resolution microCT scans and fluid analysis, they found that mice given beta-glucan developed significantly more severe lung damage compared to the untreated control group.
To confirm the immune cells were causing the damage, researchers removed them from the mice, and the inflammation went away. When they put trained alveolar macrophages into other mice, the inflammation came back. The cells showed signs of immune training, but surprisingly, this didn’t happen through the usual immune pathways. It needed signals from infections and help from other immune cells.
“Our study shows that immune memory in the lungs is more dynamic than previously thought,” said senior author Maziar Divangahi, Professor of Medicine at McGill and Associate Director of the Meakins-Christie Laboratories. “This could help explain why some individuals develop more severe lung inflammation, especially in settings like sepsis.”
Genetic analysis of the early pandemic virus shows key adaptations to humans.
Creative artwork featuring colourised 3D prints of influenza virus (surface glycoprotein hemagglutinin is blue and neuraminidase is orange; the viral membrane is a darker orange). Note: Not to scale. Credit: NIAID
Researchers from the universities of Basel and Zurich have used a historical specimen from UZH’s Medical Collection to decode the genome of the virus responsible for the 1918-1920 influenza pandemic in Switzerland. The genetic material of the virus reveals that it had already developed key adaptations to humans at the outset of what became the deadliest influenza pandemic in history.
New viral epidemics pose a major challenge to public health and society. Understanding how viruses evolve and learning from past pandemics are crucial for developing targeted countermeasures. The so-called Spanish flu of 1918-1920 was one of the most devastating pandemics in history, claiming some 20 to 100 million lives worldwide. And yet, until now, little has been known about how that influenza virus mutated and adapted over the course of the pandemic.
More than 100-year-old flu virus sequenced
An international research team led by Verena Schünemann, a paleogeneticist and professor of archaeological science at the University of Basel (formerly at the University of Zurich) has now reconstructed the first Swiss genome of the influenza virus responsible for the pandemic of 1918-1920. For their study, the researchers used a more than 100-year-old virus taken from a formalin-fixed wet specimen sample in the Medical Collection of the Institute of Evolutionary Medicine at UZH. The virus came from an 18-year-old patient from Zurich who had died during the first wave of the pandemic in Switzerland and underwent autopsy in July 1918.
Three key adaptations in Swiss virus genome
“This is the first time we’ve had access to an influenza genome from the 1918-1920 pandemic in Switzerland. It opens up new insights into the dynamics of how the virus adapted in Europe at the start of the pandemic,” says last author Verena Schünemann. By comparing the Swiss genome with the few influenza virus genomes previously published from Germany and North America, the researchers were able to show that the Swiss strain already carried three key adaptations to humans that would persist in the virus population until the end of the pandemic.
Two of these mutations made the virus more resistant to an antiviral component in the human immune system – an important barrier against the transmissions of avian-like flu viruses from animals to humans. The third mutation concerned a protein in the virus’s membrane that improved its ability to bind to receptors in human cells, making the virus more resilient and more infectious.
New genome-sequencing method
Unlike adenoviruses, which cause common colds and are made up of stable DNA, influenza viruses carry their genetic information in the form of RNA, which degrades much faster. “Ancient RNA is only preserved over long periods under very specific conditions. That’s why we developed a new method to improve our ability to recover ancient RNA fragments from such specimens,” says Christian Urban, the study’s first author from UZH. This new method can now be used to reconstruct further genomes of ancient RNA viruses and enables researchers to verify the authenticity of the recovered RNA fragments.
Invaluable archives
For their study, the researchers worked hand in hand with UZH’s Medical Collection and the Berlin Museum of Medical History of the Charité University Hospital. “Medical collections are an invaluable archive for reconstructing ancient RNA virus genomes. However, the potential of these specimens remains underused,” says Frank Rühli, co-author of the study and head of the Institute of Evolutionary Medicine at UZH.
The researchers believe the results of their study will prove particularly important when it comes to tackling future pandemics. “A better understanding of the dynamics of how viruses adapt to humans during a pandemic over a long period of time enables us to develop models for future pandemics,” Verena Schünemann says. “Thanks to our interdisciplinary approach that combines historico-epidemiological and genetic transmission patterns, we can establish an evidence-based foundation for calculations,” adds Kaspar Staub, co-author from UZH. This will require further reconstructions of virus genomes as well as in-depth analyses that include longer intervals.
A new handheld tuberculosis testing device by Tulane University is the size of a credit card, requires no electricity and significantly improves detection of the disease in those with HIV. (Vincent Postle/Tulane University)
Current tuberculosis infection tests struggle to detect the disease in those with HIV. A common co-infection, HIV can hide TB from traditional tests by eliminating the immune cells relied upon to sound the alarm.
While more than 90% of the 2 billion TB cases worldwide are latent – symptom-free and not contagious – the weakening of the immune system in those with HIV can allow latent TB to turn active, increasing the potential for new infections to spread and often resulting in fatal outcomes. Tuberculosis is the leading cause of death among those with HIV worldwide.
Now, Tulane University researchers have developed a new handheld TB test that significantly improves detection in people with HIV, according to a new study in Nature Biomedical Engineering. Powered by a beetle-inspired chemical reaction, the device requires no electricity and addresses a critical gap in TB infection detection that has long hobbled efforts to eliminate the world’s deadliest infectious disease.
“The goal was to develop a TB test that could be taken anywhere and provide quicker, more accurate results for anybody.”
Tony Hu, PhD
Dubbed the ASTRA (Antigen-Specific T-cell Response Assay), the credit card-sized device requires only a drop of blood to provide same day diagnoses without need for a laboratory or trained staff. When tested against the traditional IGRA blood test (Interferon-Gamma Release Assay), the ASTRA detected TB in HIV-infected individuals with 87% specificity compared to IGRA’s 60%, while also outperforming in detection of TB without HIV co-infection.
“The goal was to develop a TB test that could be taken anywhere and provide quicker, more accurate results for anybody,” said senior author Tony Hu, PhD, Chair in Biotechnology Innovation at Tulane University and director of the Tulane Center for Cellular & Molecular Diagnostics. “Current tests such as the IGRA are cost-prohibitive or require access to facilities that resource-limited communities don’t have. If we are going to eliminate TB, we have to diagnose and treat as many infection cases as possible.”
Added Bo Ning, lead author and assistant professor of biochemistry at Tulane University School of Medicine: “If your community has an immunocompromised population, someone may have latent TB. This can help block the spread of TB and ensure that no one slips through the cracks.”
To create a test that would not be stymied by HIV, the researchers identified two new biomarkers that could detect TB without relying on the immune cells susceptible to the virus.
After adding a drop of blood to the device, it must incubate for 4 hours to allow a preloaded reagent to stimulate a response from the immune cells. The reagent acts as a “wanted poster” asking if they’ve seen tuberculosis bacteria before.
To avoid the use of electricity, the researchers looked to an unlikely source for inspiration: the bombardier beetle. When threatened, these large insects combine two chemicals, and the resulting reaction produces a forceful spray. Similarly, two chemicals in the ASTRA are combined to propel the sample across a chip for final analysis and diagnosis.
The new device delivers results in about 4 hours, compared to the IGRA, which takes 24 hours, and a common TB skin test, which can take between two and three days for a diagnosis.
The ASTRA’s performance was validated using samples collected from a cohort in Eswatini, a country with high TB incidence and the highest reported HIV prevalence (27.3%) worldwide.
Increasing testing accuracy, access and speed is even more vital as TB resistance to drugs grows more robust, Hu said.
“The sooner you have a diagnosis, the sooner you can begin the process of determining proper treatment,” Hu said. “TB is the No. 1 pathogen HIV patients worry about globally. If treatment is available, we should be working to kill these bacteria, latent or not.”
Biological drugs have improved the lives of many people with severe asthma. However, a new study from Karolinska Institutet shows that some immune cells with high inflammatory potential are not completely eradicated after treatment.
Biological drugs have become an important tool in the treatment of severe asthma.
“They help most patients to keep their symptoms under control, but exactly how these drugs affect the immune system has so far remained unknown,” says Valentyna Yasinska, consultant in pulmonary medicine at Karolinska University Hospital and doctoral student at Karolinska Institutet’s Department of Medicine in Huddinge.
Increased in blood
In a new study published in the scientific journal Allergy, researchers at Karolinska Institutet have explored what happens to the immune cells of patients being treated with biologics. By analysing blood samples from 40 patients before and during treatment, they found that instead of disappearing during treatment, certain types of immune cell – which play a key part in asthma inflammation – actually increased.
“This suggests that biologics might not attack the root of the problem, no matter how much they help asthma patients during treatment,” says Jenny Mjösberg, professor of tissue immunology at Karolinska Institutet’s Department of Medicine in Huddinge. “Continued treatment might be necessary to keep the disease under control.”
Surprising finding
The study is based on data from patients with severe asthma sourced from the BIOCROSS study. The researchers used advanced methods such as flow cytometry and single-cell sequencing to determine the properties and function of the immune cells.
“We were surprised to find that blood levels of inflammatory cells increased rather than decreased,” says Lorenz Wirth, doctoral student at the same department at Karolinska Institutet. “This could explain why inflammation of the airways often returns when the treatment is tapered or discontinued. It is important that we understand the long-term immunological effects of these drugs.”
Relatively new drugs
Little is still known about the long-term effects of biologics like mepolizumab and dupilumab since they are relatively new, having been prescribed to asthmatics for less than ten years.
The next stage of the study will be to analyse samples from patients with a long treatment history and to study lung tissue to see how the immune cells are affected in the airways.
Cells taken from the lungs of people with chronic obstructive pulmonary disease (COPD) have a larger accumulation of soot-like carbon deposits compared to cells taken from smokers without COPD, according to a study published in ERJ Open Research. Carbon can enter the lungs via cigarette smoke, diesel exhaust and polluted air.
The cells, called alveolar macrophages, normally protect the body by engulfing any particles or bacteria that reach the lungs. But, in their new study, researchers found that when these cells are exposed to carbon they grow larger and encourage inflammation.
The research was led by Dr James Baker and Dr Simon Lea from the University of Manchester, UK. Dr Baker said: “COPD is a complex disease that has a number of environmental and genetic risk factors. One factor is exposure to carbon from smoking or breathing polluted air.
“We wanted to study what happens in the lungs of COPD patients when this carbon builds up in alveolar macrophage cells, as this may influence the cells’ ability to protect the lungs.”
The researchers used samples of lung tissue from surgery for suspected lung cancer. They studied samples (that did not contain any cancer cells) from 28 people who had COPD and 15 people who were smokers but did not have COPD.
Looking specifically at alveolar macrophage cells under a microscope, the researchers measured the sizes of the cells and the amount of carbon accumulated in the cells.
They found that the average amount of carbon was more than three times greater in alveolar macrophage cells from COPD patients compared to smokers. Cells containing carbon were consistently larger than cells with no visible carbon.
Patients with larger deposits of carbon in their alveolar macrophages had worse lung function, according to a measure called FEV1%, which quantifies how much and how forcefully patients can breathe out.
When the researchers exposed macrophages to carbon particles in the lab, they saw the cells become much larger and found that they were producing higher levels of proteins that lead to inflammation.
Dr Lea said: “As we compared cells from COPD patients with cells from smokers, we can see that this build-up of carbon is not a direct result of cigarette smoking. Instead, we show alveolar macrophages in COPD patients contain more carbon and are inherently different in terms of their form and function compared to those in smokers.
“Our research raises an interesting question as to the cause of the increased levels of carbon in COPD patients’ macrophages. It could be that people with COPD are less able to clear the carbon they breathe in. It could also be that people exposed to more particulate matter are accumulating this carbon and developing COPD as a result.
“In future, it would be interesting to study how this carbon builds up and how lung cells respond over a longer period of time.”
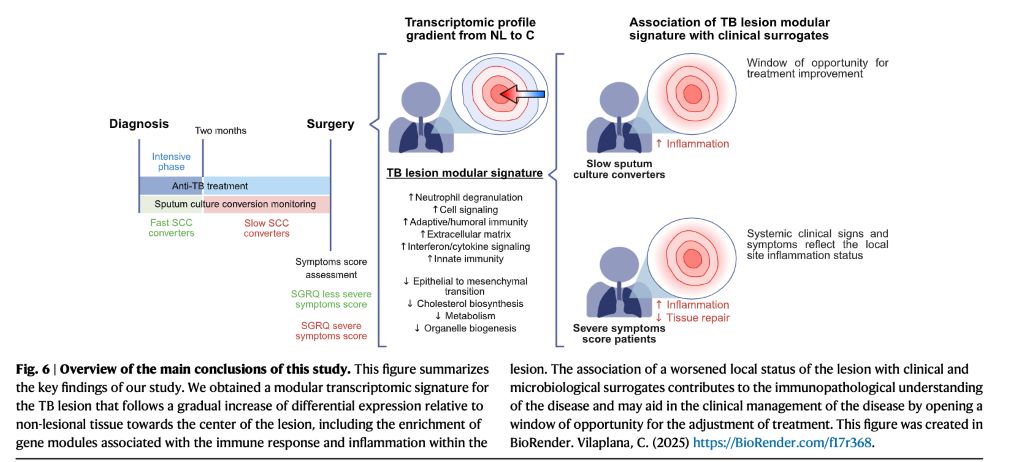
A study in Nature Communications reveals, for the first time, how the transcriptomic profile of human tuberculosis lung lesions is correlated with clinical data from the same patients. The work could potentially lead to improved prognosis by using personalised strategies.
Dr Cristina Vilaplana led researchers from the Experimental Tuberculosis Unit (UTE) at the Germans Trias i Pujol Research Institute (IGTP) and the Germans Trias i Pujol University Hospital.
The study applied RNAseq techniques to 44 fresh tissue samples from lesional and adjacent lung areas of patients with drug-sensitive and multidrug-resistant tuberculosis who underwent therapeutic surgery. The results show a clear separation between lesional and non-lesional tissue, with high expression of pro-inflammatory genes in the lesions.
Weighted gene co-expression network analysis (WGCNA) identified 17 differential transcriptomic modules and revealed a gradient of immune response elements depending on their location within the lesion.
Although lesion transcriptomics has been studied previously, this is the first work to associate these molecular profiles with clinical indicators from the same patients.
“Individuals with more severe forms of the disease present more inflamed lesions, while patients with better clinical outcomes show profiles compatible with tissue repair phases,” explains Dr Vilaplana.
The researchers used two clinical surrogates: a validated respiratory quality of life questionnaire (SGRQ) and sputum culture conversion.
“We confirmed that when a patient says they feel unwell, it is also reflected at the molecular level: their lesions show a stronger inflammatory response,” adds Vilaplana.
Furthermore, patients who take longer to achieve sputum culture conversion, a factor previously linked to worse prognosis, also show higher immune activation at the lesion site.
“These data open the door to personalised strategies: If after two months the patient hasn’t cleared the bacillus, we may need to adapt the treatment to modulate the inflammatory response and avoid a worse clinical outcome,” she concludes.
Johannesburg, 26 May 2025: Despite national guidelines and access to essential medicines, severe asthma remains under-recognised and inconsistently managed within South Africa’s healthcare system. It is therefore critical to address ongoing patient challenges, particularly regarding access to diagnostic tools, limited use of phenotyping, and the imperative to align clinical practice with international best practice recommendations.
The Severe Asthma Index 2025 found that South Africa scored below the global average in four out of five domains, revealing persistent gaps in policy coordination, equitable access, diagnostic capacity, and environmental health.¹ᵃ Of concern is the continued reliance on oral corticosteroids (OCS) without proper assessment or referral, especially where evidence-based, targeted biologics remain inaccessible or unfunded.1b+2a
Understanding asthma in South Africa
South Africa has robust asthma guidelines, but the absence of a national asthma strategy and lack of participation in global severe asthma registries limit insight into outcomes and weaken care coordination. Specialist care and phenotyping are largely confined to urban centres, and national data on hospitalisations and treatment outcomes is scarce. Although reported asthma-related societal costs and disability adjusted life years (DALYs) are relatively low, this likely masks the true burden among patients with severe, underdiagnosed, or poorly controlled disease.¹ᵇ Traditionally, asthma mortality in Southern Africa has been considered as relatively high due in large part to short-acting beta-agonists (SABAs) overuse.3
Environmental factors compound these challenges. High levels of particulate matter (PM2.5) and poor indoor air quality contribute significantly to disease severity, particularly in low-income areas. Meanwhile, access to advanced diagnostics and therapies remains limited. Biologic add-on therapies and fractional exhaled nitric oxide (FeNO) testing are not routinely available in the public sector, leaving most patients dependent on standard treatments with few options for escalation if the disease remains uncontrolled.¹ᵇ
Rethinking corticosteroid use
The Severe Asthma Index 2025 highlights the widespread use of oral corticosteroids (OCS) in South Africa as a persistent pattern that may pose long-term health risks if not carefully managed or replaced by more targeted therapies. While OCS play a critical role in treating acute exacerbations, frequent or prolonged use is linked to serious side effects, including osteoporosis, adrenal suppression, diabetes, and infections.²ᶜ
“There’s growing awareness that long-term OCS use can lead to significant health risks,” says Dwayne Koot, Medical Manager at Sanofi South Africa. “For severe asthma, the shift is towards biologic therapies that specifically target the underlying inflammation, not just the symptoms.1c As a simple regimen (where available), inhaled corticosteroid–formoterol combinations are now recommended as the preferred reliever across all severity levels.3 If high-dose ICS-LABA is needed, its use should be limited to 3 – 6 months, prompting phenotyping and biologic therapy add-on if asthma is not controlled. Low-dose maintenance OCS should only be considered as a last resort if no other options are available.”
Improving diagnosis and referral
Access to diagnostic tools remains uneven across South Africa, particularly in the public sector. Spirometry is not routinely available at primary care level, while FeNO testing, oscillometry, and biomarker analysis are largely limited to research centres or private practices.¹ᵇ
“This makes it difficult to accurately diagnose, phenotype, and manage asthma, potentially leading to suboptimal treatment decisions and poorer patient outcomes,” says Koot.
“There’s an opportunity to enhance the referral pathway to specialists and expand access to advanced diagnostic tools by defining referral criteria and partnering with specialised centres,” Koot says. “Routine phenotyping at GINA step 5, crucial for tailoring treatment plans and identifying suitable candidates for biologic therapies, is currently limited in many healthcare settings. Expanding these capabilities would enable a more personalised approach to asthma management.”3
To help close these gaps, the Severe Asthma Index 2025 recommends piloting basic phenotyping tools such as eosinophil counts at regional hospitals, establishing asthma registries to monitor outcomes and access, and expanding clinician training in severe asthma diagnosis and escalation pathways.¹ᵇ “Better data and better training could transform how we identify and treat severe asthma,” says Koot.
Next steps for clinical practice
Healthcare professionals have a pivotal role to play in strengthening asthma care — from recognising poor control early to ensuring patients access the most appropriate treatment in a timely manner. This includes reassessing those with persistent symptoms, reinforcing correct inhaler technique, referring for further investigation when needed, and considering alternative therapies when conventional options are no longer sufficient.3
South Africa already has many of the essential components in place: national treatment guidelines, access to key medicines, and clinical expertise. The next step is to ensure that patients with severe asthma are consistently identified, supported, and offered the full range of available interventions.
“As the World Asthma Day 2025 theme reminds us, the goal is to ‘Make Inhaled Treatments Accessible for ALL’, because inhaled medications are vital not just for preventing attacks, but for controlling chronic inflammation,” says Koot. “We encourage healthcare practitioners and policy makers to help make appropriate, evidence-based asthma care a reality for every South African asthmatic .”
For more information about asthma management and Sanofi’s commitment to respiratory health, please visit www.sanofi.co.za