A study in the journal Science presents compelling new evidence that neurons in the brain’s memory centre, the hippocampus, continue to form well into late adulthood. The research from Karolinska Institutet provides answers to a fundamental and long-debated question about the human brain’s adaptability.
The hippocampus is a brain region that is essential for learning and memory and involved in emotion regulation. Back in 2013, Jonas Frisén’s research group at Karolinska Institutet showed in a high-profile study that new neurons can form in the hippocampus of adult humans. The researchers then measured carbon-14 levels in DNA from brain tissue, which made it possible to determine when the cells were formed.
Identifying cells of origin
However, the extent and significance of this formation of new neurons (neurogenesis) are still debated. There has been no clear evidence that the cells that precede new neurons, known as neural progenitor cells, actually exist and divide in adult humans.
“We have now been able to identify these cells of origin, which confirms that there is an ongoing formation of neurons in the hippocampus of the adult brain,” says lead researcher Jonas Frisén, professor of stem cell research at the Department of Cell and Molecular Biology.
In the new study, the researchers combined several advanced methods to examine brain tissue from people aged 0 to 78 years from several international biobanks. They used a method called single-nucleus RNA sequencing, which analyses gene activity in individual cell nuclei, and flow cytometry to study cell properties.
By combining this with machine learning, they were able to identify different stages of neuronal development, from stem cells to immature neurons, many of which were in the division phase.
To localise these cells, the researchers used two techniques that show where in the tissue different genes are active: RNAscope and Xenium. These methods confirmed that the newly formed cells were located in a specific area of the hippocampus called the dentate gyrus. This area is important for memory formation, learning and cognitive flexibility.
Hope for new treatments
The results show that the progenitors of adult neurons are similar to those of mice, pigs and monkeys, but that there are some differences in which genes are active. There were also large variations between individuals – some adult humans had many neural progenitor cells, others hardly any at all.
“This gives us an important piece of the puzzle in understanding how the human brain works and changes during life,” explains Jonas Frisén. “Our research may also have implications for the development of regenerative treatments that stimulate neurogenesis in neurodegenerative and psychiatric disorders.”
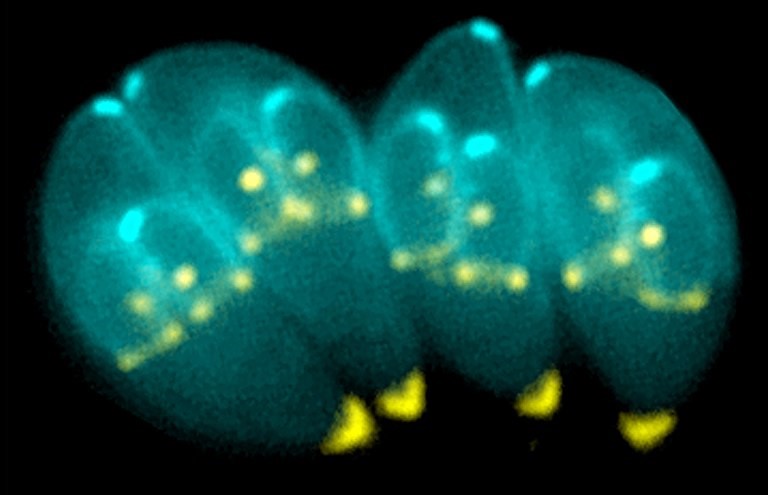
A team of scientists at the University of California, Riverside, explains in a paper published in PLoS Pathogens how the microscopic parasite Toxoplasma gondii can significantly disrupt brain function, even when it infects only a small number of neurons. The team found the parasite interferes with essential communication between brain cells — research that can offer new ways to detect and treat chronic brain infections.
Toxoplasma gondii can infect nearly any warm-blooded animal and prefers to live inside brain cells, forming cysts in neurons that can persist for life. The researchers report that they found infected neurons release fewer extracellular vesicles (EVs) — tiny, membrane-bound packets used by cells to exchange information.
“We found this disruption in EV signalling can interfere with how neurons and glial cells, especially astrocytes, maintain a healthy brain environment,” said Emma H. Wilson, a professor of biomedical sciences in the UC Riverside School of Medicine who led the research team. “Even a handful of infected neurons can shift the brain’s neurochemical balance. This suggests that communication between neurons and supporting glial cells is not only critical, but also vulnerable to hijacking by parasites.”
Approximately 10–30% of people in the United States are infected with Toxoplasma gondii, often without knowing it. The parasite is typically contracted through undercooked meat or exposure to cat feces. Although the immune system typically keeps the infection in check, the parasite can lie dormant in the brain for decades. In individuals with weakened immunity, it can reactivate and cause serious illness.
Current diagnostic tools can only detect whether someone has been exposed to Toxoplasma gondii by identifying antibodies. The tools cannot confirm whether the parasite is still present in the brain or how it may be affecting brain function.
“Our research opens the door to using EVs as biomarkers, which can be isolated from blood,” Wilson said.
The study was conducted using mouse models and human cells in a laboratory setting.
Wilson explained that in healthy mouse brains astrocytes regulate neurotransmitters like glutamate, ensuring that neurons do not become overexcited. But when neurons infected with Toxoplasma gondii stop sending the right EV signals, this regulation breaks down. The result is elevated glutamate levels, which can lead to seizures, neural damage, or altered brain connectivity.
“The parasite may play a larger role in neurological and behavioural conditions than we previously thought,” she said.
Wilson’s research team is now working to analyse samples from human blood banks to look for EVs linked to Toxoplasma gondii brain infection. The team also hopes to better understand how glial cells detect and respond to parasite proteins — insights that could one day lead to new therapies or even vaccines.
“Our brains have built-in defences that may recognise and respond to neurons infected by Toxoplasma gondii,” Wilson said. “If we can learn how to support or enhance that process, we may be able to better protect people, especially the most vulnerable.”
Despite its potential impact, Toxoplasma gondii is often misunderstood, Wilson added.
“There’s no need to avoid someone who is infected; most people live their entire lives without symptoms,” she said. “Pregnant individuals should be cautious as the parasite can cause serious birth defects if contracted for the first time during pregnancy. The most effective prevention is proper food handling and hygiene. Cook meat thoroughly, wash vegetables, and always wash your hands after handling cat litter, especially from young cats, which are more likely to shed the parasite.”
A drug commonly used to treat type 2 diabetes may reduce excess fluid in the brains of patients with hydrocephalus, which could help treat the disease less invasively than current treatments, according to a Northwestern Medicine study published in theJournal of Clinical Investigation.
Normal pressure hydrocephalus occurs when excess cerebrospinal fluid builds up inside the skull and puts pressure on the brain. The cause of the condition is elusive and affects up to three percent of individuals over the age of 65, with symptoms including cognitive decline, difficulty walking and bladder problems.
Patients are typically treated with permanent ventriculoperitoneal shunts, which are surgically implanted in the front or back of the skull and are connected to a valve that diverts excess cerebrospinal fluid away from the brain and into the abdomen where it is absorbed. The procedure has been shown to dramatically improve mobility, bladder control and cognitive functioning in patients with hydrocephalus, according to senior study author Stephen Magill, MD, PhD.
“It’s a great procedure because it’s one of the few things you can do that actually reverses these symptoms,” said Magill, who is assistant professor of Neurological Surgery.
There is, however, no pharmacological treatment currently approved to treat hydrocephalus. Additionally, nearly 20% of patients with normal pressure hydrocephalus also have type 2 diabetes and take sodium/glucose cotransporter 2 (SGLT2) inhibitors to manage their blood sugar, cardiovascular and kidney function, and weight loss.
Magill recently observed a reduction in the brain ventricle size in a patient with hydrocephalus who had a ventriculoperitoneal shunt surgically implanted and then began taking SGLT2 inhibitors to treat their type 2 diabetes. This phenomenon prompted Magill to further investigate the impact of SGLT2 inhibitors on ventricular size in patients with hydrocephalus.
“The medication inhibits a receptor found in the kidneys, which is where it works for diabetes. However, that receptor is also expressed in the choroid plexus, which is the structure in the brain that secretes the spinal fluid. Although this was known from animal studies, the clinical aspects of this biology have not been fully appreciated,” Magill said.
In the current study, three patients with hydrocephalus underwent CT scans both before and after surgery for ventriculoperitoneal shunts. After surgery, each patient began taking SGLT2 inhibitors for a medical indication and then underwent additional CT scans.
From analyzing these scans, Magill’s team discovered that all three patients showed a reduction in ventricle size as well as structural changes in their brains after starting SGLT2 therapy. One patient demonstrated dramatic ventricle size reduction due to ventricular collapse and required a shunt valve adjustment to reduce cerebrospinal fluid drainage.
“It’s a really interesting clinical observation because it raises the possibility that these medications could be used to treat normal pressure hydrocephalus in the future, which would normally require surgery,” Magill said.
Magill said the findings have sparked a new line of research in studying how SGLT2 inhibitors could help prevent hydrocephalus, adding that his team is now studying SGLT2 knockout mouse models to better understand the drug’s impact on ventricular size.
Their findings could ultimately inform new therapeutic strategies for treating normal pressure hydrocephalus as well as post-traumatic hydrocephalus, or the buildup of cerebrospinal fluid after traumatic brain injury, according to Magill.
“This sparks a new line of research on how normal pressured hydrocephalus develops, what causes it, how this protein works in creating and secreting spinal fluid, and has direct translational implications,” Magill said. “There’s a whole new avenue of potentially treating this disease that might save a patient from having surgery, and there’s always risks with surgery. It will also evolve our understanding of how these drugs work.”
Researchers at Karolinska Institutet and Lund University have identified a new treatment strategy for neuroblastoma, an aggressive form of childhood cancer. By combining two antioxidant enzyme inhibitors, they have converted cancer cells in mice into healthy nerve cells. The study is published in the journal Proceedings of the National Academy of Sciences (PNAS).
Neuroblastoma is a type of childhood cancer that affects the nervous system and is the leading cause of cancer-related death in young children. Some patients have a good prognosis, but those with metastatic tumours often cannot be cured despite modern combinations of surgery, radiation, chemotherapy and immunotherapy.
“The children who survive often have lifelong cognitive difficulties due to the harsh treatment, so there is a great need for new forms of therapies for children with neuroblastoma,” says Marie Arsenian Henriksson, professor at the Department of Microbiology, Tumour and Cell Biology at Karolinska Institutet.
Transform cancer cells
Differentiation therapy is a treatment method used in neuroblastoma that aims to transform cancer cells into more mature and healthy cells. The problem with the current retinoic acid differentiation therapy is that many patients do not respond to treatment, and about half develop resistance.
In collaboration with researchers at Lund University, Marie Arsenian Henriksson’s research team has shown that inhibition of two specific enzymes, PRDX6 and GSTP1, could be an alternative to retinoic acid treatment.
Mature into healthy neurons
Neuroblastoma is characterised by high oxidative stress due to the active metabolism in the cancer cells. Tumours are therefore dependent on antioxidant enzymes such as PRDX6 and GSTP1 to manage the stress and avoid cell death. High levels of these enzymes are associated with a poorer prognosis.
“When we inhibit these enzymes in cell cultures as well as in mouse models, some of the tumour cells die while others mature into active, healthy neurons, impairing tumour growth,” says Judit Liaño-Pons, researcher at the Department of Microbiology, Tumour and Cell Biology.
Needs to be tested in children
In the next step, the treatment will need to be tested in a clinical trial to investigate its safety and efficacy in children. One of the inhibitors has received orphan drug designation from the US Food and Drug Administration for the treatment of a different diagnosis in adults, making it a particularly promising drug candidate, according to the scientists.
Many survivors of cardiogenic shock showed evidence of new cognitive impairment after leaving the hospital, according to a study led by UT Southwestern Medical Center researchers. The findings, published in the Journal of the American College of Cardiology, highlight a need to screen survivors and provide referrals to neuropsychology experts, the authors said.
“Our study demonstrated that nearly two-thirds of cardiogenic shock survivors experienced cognitive impairment within three months of hospital discharge, underscoring a critical but overlooked aspect of recovery,” said senior investigator James de Lemos, MD, Professor of Internal Medicine and Chief of the Division of Cardiology at UT Southwestern. “The findings are important for developing interventions that focus not only on improving survival but also on preventing or mitigating the functional consequences of cardiogenic shock, including cognitive decline.”
Cardiogenic shock results from heart failure, heart attack, or complications following cardiac surgery, and is characterised by a sudden drop in heart pumping ability. It results in acute hypoperfusion and hypoxia of the organs and has historically resulted in high mortality.
With advances in treatment during the past two decades, up to 70% of patients suffering from cardiogenic shock can now survive. But there is limited understanding of survivors’ recovery and quality of life after they leave the hospital.
“Our study is the first to systematically examine the cognitive outcomes of cardiogenic shock survivors, evaluating how cognition impacts patients’ ability to return to daily activities,” said Eric Hall, M.D., a clinical fellow in the Division of Cardiology who was the study leader and first author. “We found that cardiogenic shock is associated with cognitive impairment, which is an under-recognized consequence strongly linked to patients’ overall quality of life.”
UTSW researchers conducted the study by enrolling 141 patients who had survived cardiogenic shock before being discharged. To establish a baseline, family members completed a questionnaire, the AD8 survey, about the patients’ cognitive function before hospitalisation.
Before discharge, each patient completed the Montreal Cognitive Assessment-Blind (bMoCA) to screen for signs of cognitive impairment. Three months after discharge, patients repeated the assessments, allowing researchers to track changes in thinking ability and daily functioning over time.
Among patients with no sign of cognitive impairment before admission, 65% were found to have new impairment at discharge, and 53% continued to show impairment at their three-month follow-up. UTSW researchers emphasized that these findings should inform the development of comprehensive survivorship programs including screening protocols to identify impairments patients face and rehabilitation programs to help them recover from those challenges.
“We hope to use this study as a foundation to develop targeted rehabilitation strategies that connect patients with neuropsychology experts and improve long-term recovery in cardiogenic shock survivors,” Dr de Lemos said.
Heals spinal cord injuries with the help of electricity. Researchers have developed an ultra-thin implant that can be placed directly on the spinal cord. The implant delivers a carefully controlled electrical current across the injured area. In a recent study, researchers were able to observe how the electrical field treatment led to improved recovery in rats with spinal cord injuries, and that the animals regained movement and sensation. Please note that the image shows a newer model of the implant used in the study. Photo and illustration: University of Auckland
Researchers at Chalmers University of Technology in Sweden and the University of Auckland in New Zealand have developed a groundbreaking bioelectric implant that restores movement in rats after injuries to the spinal cord.
This breakthrough, published in Nature Communications, offers new hope for an effective treatment for humans suffering from loss of sensation and function due to spinal cord injury.
Electricity stimulated nerve fibres to reconnect
Before birth, and to a lesser extent afterwards, naturally occurring electric fields play a vital role in early nervous system development, encouraging and guiding the growth of nerve fibres along the spinal cord. Scientists are now harnessing this same electrical guidance system in the lab.
“We developed an ultra-thin implant designed to sit directly on the spinal cord, precisely positioned over the injury site in rats,” says Bruce Harland, senior research fellow, University of Auckland, and one of the lead researchers of the study.
The device delivers a carefully controlled electrical current across the injury site.
“The aim is to stimulate healing so people can recover functions lost through spinal cord injury,” says Professor Darren Svirskis, University of Auckland, Maria Asplund, Professor of bioelectronics at Chalmers University of Technology.
She is, together with Darren Svirskis, University of Auckland,
In the study, researchers observed how electrical field treatment improved the recovery of locomotion and sensation in rats with spinal cord injury. The findings offer renewed hope for individuals experiencing loss of function and sensation due to spinal cord injuries.
“Long-term, the goal is to transform this technology into a medical device that could benefit people living with life-changing spinal-cord injuries,” says Maria Asplund.
The study presents the first use of a thin implant that delivers stimulation in direct contact with the spinal cord, marking a groundbreaking advancement in the precision of spinal cord stimulation.
“This study offers an exciting proof of concept showing that electric field treatment can support recovery after spinal cord injury,” says doctoral student Lukas Matter, Chalmers University of Technology, the other lead researcher alongside Harland.
Improved mobility after four weeks
Unlike humans, rats have a greater capacity for spontaneous recovery after spinal cord injury, which allowed researchers to compare natural healing with healing supported by electrical stimulation.
After four weeks, animals that received daily electric field treatment showed improved movement compared with those who did not. Throughout the 12-week study, they responded more quickly to gentle touch.
“This indicates that the treatment supported recovery of both movement and sensation,” Harland says.
“Just as importantly, our analysis confirmed that the treatment did not cause inflammation or other damage to the spinal cord, demonstrating that it was not only effective but also safe,” Svirskis says.
The next step is to explore how different doses, including the strength, frequency, and duration of the treatment, affect recovery, to discover the most effective recipe for spinal-cord repair.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
Patients with atrial fibrillation who have experienced a stroke would benefit greatly from earlier treatment than is currently recommended in UK guidelines, finds a new study led by UCL researchers.
The results of the CATALYST study, published in The Lancet, included data from four randomised trials with a total of 5441 patients across the UK, Switzerland, Sweden and the United States, who had all experienced a recent stroke (between 2017-2024) due to a blocked artery and atrial fibrillation (irregular heartbeat).
Patients had either started medication early (within four days of their stroke) or later (after five days or more).
The researchers found that starting direct oral anticoagulants (DOACs, which thin the blood to prevent it from clotting as quickly) within four days of having a stroke was safe, with no increase in bleeding into the brain. Additionally, early initiation of treatment significantly reduced the risk of another stroke due to bleeding or artery blockage by 30% compared to those who started treatment later.
People with atrial fibrillation who have had a stroke have an increased risk of having another stroke, but this risk can be reduced by taking anticoagulants.
Anticoagulants come with the rare but dangerous side effect of bleeding into the brain, and there is a lack of evidence about when is best to start taking them after a stroke. Current UK guidelines are varied, suggesting that those who have had a moderate or severe stroke should wait at least five days before starting blood-thinning treatments.
To tackle this question, the researchers investigated the impact of early compared to delayed anticoagulant treatment.
Chief Investigator, Professor David Werring (UCL Queen Square Institute of Neurology) said: “Our new study supports the early initiation of DOACs in clinical practice, offering better protection against further strokes for a wide range of patients.”
The researchers now hope that their findings will influence clinical guidelines and improve outcomes for stroke patients worldwide.
First author and main statistician, Dr Hakim-Moulay Dehbi (UCL Comprehensive Clinical Trials Unit), said: “By systematically combining the data from four clinical trials, we have identified with increased confidence, compared to the individual trials, that early DOAC initiation is effective.”
The CATALYST study builds on findings from the British Heart Foundation funded OPTIMAS study – where the UCL-led research team analysed 3621 patients with atrial fibrillation who had had a stroke between 2019 and 2024, across 100 UK hospitals.
Half of the participants began anticoagulant treatment within four days of their stroke (early), and the other half started treatment seven to 14 days after having a stroke (delayed). Patients were followed up after 90 days to assess several outcomes including whether they went on to have another stroke and whether they experienced bleeding in the brain.
Both the early and late groups experienced a similar number of recurrent strokes. Early treatment was found to be effective and did not increase the risk of a bleed into the brain.
Professor Nick Freemantle, Senior Investigator and Director of the UCL Comprehensive Clinical Trials Unit (CCTU) that co-ordinated the OPTIMAS trial, said: “The benefits of early initiation of blood-thinning treatment are clear: patients receive the definitive and effective long-term stroke prevention therapy promptly, rather than waiting. This approach ensures that crucial treatments are not delayed or missed, particularly for patients who are discharged from the hospital.”
Study limitations
The timing for starting blood-thinning medication was based on previous trial designs (such as OPTIMAS), which may not cover all possible scenarios. Additionally, not all participants were randomised to the same timing groups, so some data was excluded. Lastly, the study didn’t include many patients with very severe strokes, so the findings might not apply to those cases.
A diabetes medication that lowers brain fluid pressure has cut monthly migraine days by more than half, according to a new study presented at the European Academy of Neurology (EAN) Congress 2025
A diabetes medication that lowers brain fluid pressure has cut monthly migraine days by more than half, according to a new study presented at the European Academy of Neurology (EAN) Congress 2025.1
Researchers at the Headache Centre of the University of Naples “Federico II” gave the glucagon-like peptide-1 (GLP-1) receptor agonist liraglutide to 26 adults with obesity and chronic migraine (defined as ≥ 15 headache days per month). Patients reported an average of 11 fewer headache days per month, while disability scores on the Migraine Disability Assessment Test dropped by 35 points, indicating a clinically meaningful improvement in work, study, and social functioning.
GLP-1 agonists have gained recent widespread attention, reshaping treatment approaches for several diseases, including diabetes and cardiovascular disease.2 In the treatment of type 2 diabetes, liraglutide helps lower blood sugar levels and reduce body weight by suppressing appetite and reducing energy intake.3,4,5
Importantly, while participants’ body-mass index declined slightly (from 34.01 to 33.65), this change was not statistically significant. An analysis of covariance confirmed that BMI reduction had no effect on headache frequency, strengthening the hypothesis that pressure modulation, not weight loss, drives the benefit.
“Most patients felt better within the first two weeks and reported quality of life improved significantly”, said lead researcher Dr Simone Braca. “The benefit lasted for the full three-month observation period, even though weight loss was modest and statistically non-significant.”
Patients were screened to exclude papilledema (optic disc swelling resulting from increased intracranial pressure) and sixth nerve palsy, ruling out idiopathic intracranial hypertension (IIH) as a confounding factor. Growing evidence closely links subtle increases in intracranial pressure to migraine attacks.6 GLP-1-receptor agonists such as liraglutide reduce cerebrospinal fluid secretion and have already proved effective in treating IIH.7 Therefore, building on these observations, Dr Braca and colleagues hypothesised that exploiting the same mechanism of action might ultimately dampen cortical and trigeminal sensitisation that underlie migraine.
“We think that, by modulating cerebrospinal fluid pressure and reducing intracranial venous sinuses compression, these drugs produce a decrease in the release of calcitonin gene-related peptide (CGRP), a key migraine-promoting peptide”, Dr Braca explained. “That would pose intracranial pressure control as a brand-new, pharmacologically targetable pathway.”
Mild gastrointestinal side effects (mainly nausea and constipation) occurred in 38% of participants but did not lead to treatment discontinuation.
Following this exploratory 12-week pilot study, a randomised, double-blind trial with direct or indirect intracranial pressure measurement is now being planned by the same research team in Naples, led by professor Roberto De Simone. “We also want to determine whether other GLP-1 drugs can deliver the same relief, possibly with even fewer gastrointestinal side effects”, Dr Braca noted.
If confirmed, GLP-1-receptor agonists could offer a new treatment option for the estimated one in seven people worldwide who live with migraine,8 particularly those who do not respond to current preventives. Given liraglutide’s established use in type 2 diabetes and obesity, it may represent a promising case of drug repurposing in neurology.
References
Braca S., Russo C. et al.GLP-1R Agonists for the Treatment of Migraine: A Pilot Prospective Observational Study. Abstract A-25-13975. Presented at the 11th EAN Congress (Helsinki, Finland).
Zheng, Z., Zong, Y., Ma, Y. et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Sig Transduct Target Ther9, 234 (2024).
Lin, C. H. et al. An evaluation of liraglutide including its efficacy and safety for the treatment of obesity. Expert Opin. Pharmacother.21, 275–285 (2020).
Moon, S. et al. Efficacy and safety of the new appetite suppressant, liraglutide: A meta-analysis of randomized controlled trials. Endocrinol. Metab. (Seoul.)36, 647–660 (2021).
Jacobsen, L. V., Flint, A., Olsen, A. K. & Ingwersen, S. H. Liraglutide in type 2 diabetes mellitus: clinical pharmacokinetics and pharmacodynamics. Clin. Pharmacokinet.55, 657–672 (2016).
De Simone R, Sansone M, Russo C, Miele A, Stornaiuolo A, Braca S. The putative role of trigemino-vascular system in brain perfusion homeostasis and the significance of the migraine attack. Neurol Sci. 2022 Sep;43(9):5665-5672. doi: 10.1007/s10072-022-06200-x. Epub 2022 Jul 8. PMID: 35802218; PMCID: PMC9385793.
Mitchell J.L., Lyons H.S., Walker J.K. et al. (2023). The effect of GLP-1RA exenatide on idiopathic intracranial hypertension: a randomised clinical trial. Brain. 146(5):1821-1830.
Steiner T.J., Stovner L.J., Jensen, R. et al. (2020). Migraine remains second among the world’s causes of disability. The Journal of Headache and Pain. 21:137.
A medical team at Erasmus University Medical Center in the Netherlands uses the new imaging probe with a Quest camera to get a better view of cancerous tumors during non-brain cancer surgery. Photo courtesy of Erasmus University Medical Center
In a significant leap forward for successful cancer surgery, researchers at the University of Missouri and collaborators have developed a new imaging probe to help surgeons more accurately identify and remove aggressive tumours during operations.
The tool is expected to be a critical advancement in the fight against glioblastoma, one of the most difficult-to-treat brain cancers. In the future, it is intended to be expanded for image-guided surgery of various other solid tumours.
Described in a new study in Nature Publishing Group Imaging, the innovation works by pairing a fluorescent dye with a fatty acid molecule that cancer cells readily absorb. When introduced into the body, the compound is taken up by tumour cells, causing them to glow under near-infrared light, revealing cancer that might otherwise remain hidden.
Glioblastoma is considered surgically incurable because the tumour doesn’t stay in one place – it spreads and invades healthy brain tissue in a diffuse, microscopic way. This makes it impossible to remove completely without risking serious damage to brain function.
“Surgery remains one of the primary treatments for many cancers,” Elena Goun, associate professor of chemistry in the College of Arts and Science and one of the lead authors of the study, said. “In breast or prostate cancer, surgeons can often remove the tumour along with surrounding tissue. In brain cancer, that’s simply not possible. You must preserve healthy brain tissue. But if even a few cancer cells are left behind, the disease will return.”
That dilemma is especially acute with glioblastoma, which doesn’t form a neatly contained mass. Instead, it sends out microscopic extensions — finger-like projections that blend into healthy brain tissue and are invisible to the naked eye.
Because of this, surgeons must walk a fine line: removing as much tumour as possible while avoiding harm to vital brain areas. The more thoroughly the tumour is removed, the more effective follow-up treatments like radiation and chemotherapy tend to be.
The new small-molecule probe, known as FA-ICG, is engineered to solve that problem. It links a natural long-chain fatty acid (FA) to indocyanine green (ICG), an FDA-approved near-infrared dye widely used in surgical imaging. This fatty acid-based approach means the probe is highly selective: glioblastoma cells, which thrive on fatty acids, absorb it more than normal brain cells. That makes the cancer stand out more clearly.
The result is a tool that takes advantage of cancer’s altered metabolism to highlight tumour cells from within.
“Surgeons would view a monitor during surgery showing where the probe is lighting up,” Goun explained. “If they still see fluorescent signals, it means cancer is still present and more tissue needs to be removed. When the light disappears, they would know they’ve cleared the area.”
In the operating room, surgeons already use a variety of tools to guide tumour removal – including microscopes, ultrasound and fluorescent dyes. Of those, fluorescent dyes are particularly useful because they make otherwise invisible tumour cells light up under special lighting.
Right now, the only approved imaging dye for glioblastoma surgery is 5-ALA, which fluoresces under blue light. But 5-ALA comes with major limitations: The operating room must be darkened in order to see it, tissue penetration is shallow and the fluorescent signal is often weak and non-specific.
It also comes with side effects, including photosensitivity, meaning patients must avoid bright light exposure after surgery due to the risk of skin and eye damage.
That’s where the FA-ICG probe shines – both literally and functionally.
Compared to 5-ALA, FA-ICG is brighter, works under normal surgical lighting, and offers real-time visualisation under the microscope – no need to turn the lights off mid-surgery. This saves time and makes procedures more efficient. The signal-to-background ratio is also higher, meaning it’s easier to distinguish tumour tissue from healthy brain.
The FA-ICG probe is not only easier to see, it’s also easier to use. Its longer half-life allows more flexibility in scheduling surgeries, and the logistics of administration are simpler than with current probes.
“The upside of fluorescence-guided surgery is that you can make little remnants much more visible using the light emitting properties of these tumour cells when you give them a dye,” said Rutger Balvers, a neurosurgeon at Erasmus University Medical Center in the Netherlands, who is expected to lead human clinical trials of the probe. “And we think that the upside of FA-ICG compared to what we have now is that it’s more select in targeting tumour cells. The visual properties of the probe are better than what we’ve used before.”
Michael Chicoine is a neurosurgeon at MU Health Care and chair of Mizzou’s School of Medicine’s Department of Neurosurgery. While he’s not directly involved in the research, Chicoine understands the potential benefits firsthand.
Currently, he said, MRIs are the gold standard for imaging tumours; however, they’re expensive and time-consuming, especially when required during an operation.
“This fluorescent metabolically linked tool gives you real-time imaging,” he said. “We could merge techniques, using the probe during surgery and saving the MRI for a sort of final exam. It’s definitely an exciting advancement.”
Researchers are also excited about other uses for the probe, including for other types of cancers and for use during follow-up treatments.
“After radiation or chemotherapy, it becomes very difficult to distinguish between scar tissue and active tumor,” Chicoine said. “This probe could give us a definitive answer – helping doctors know whether to continue treatment or adjust it, or consider another surgery. Eliminating the current uncertainty would be really helpful.”
Another promising use of the probe could be in photodynamic therapy either during or after surgery. Since the dye also has light-activated properties that can kill cancer cells, researchers are exploring whether it could double as a treatment tool, not just a diagnostic one.
Clinical trials for use in glioblastoma cases are expected to start in Europe, with strong interest already growing among neurosurgical teams.
The upcoming Phase 1 trial will focus on how patients tolerate the probe, whether there are any side effects at an effective dose and how its performance compares to existing tools. Ultimately, the goal is to make brain tumour surgery safer, helping surgeons remove all cancerous tissues while preserving as much healthy brain tissue as possible.
If results are positive, future studies could expand the use of FA-ICG beyond brain tumours to other cancers with high fatty acid metabolism, such as pancreatic cancer,according to fellow corresponding author Laura Mezzanotte from the Erasmus’ Department of Radiology and Nuclear Medicine.
While scientists have long known that different senses activate different parts of the brain, a new Yale-led study indicates that multiple senses all stimulate a critical region deep in the brain that controls consciousness.
The study, published in the journal NeuroImage, sheds new light on how sensory perception works in the brain and may fuel the development of therapies to treat disorders involving attention, arousal, and consciousness.
In the study, a research team led by Yale’s Aya Khalaf focused on the workings of subcortical arousal systems, brain structure networks that play a crucial role in regulating sleep-wake states. Previous studies on patients with disorders of consciousness, such as coma or epilepsy, have confirmed the influence of these systems on states of consciousness.
But prior research has been largely limited to tracking individual senses. For the new study, researchers asked if stimuli from multiple senses share the same subcortical arousal networks. They also looked at how shifts in a subject’s attention might affect these networks.
For the study, researchers analysed fMRI (functional magnetic resonance imaging) datasets collected from 1,561 healthy adult participants as they performed 11 different tasks using four senses: vision, audition, taste, and touch.
They made two important discoveries: that sensory input does make use of shared subcortical systems and, more surprisingly, that all input, regardless of which sense delivered the signal, stimulates activity in two deep brain regions, the midbrain reticular formation and the central thalamus, when a subject is sharply focused on the senses.
The key to stimulating the critical central brain regions, they found, were the sudden shifts in attention demanded by the tasks.
“We were expecting to find activity on shared networks, but when we saw all the senses light up the same central brain regions while a test subject was focusing, it was really astonishing,” said Khalaf, a postdoctoral associate in neurology at Yale School of Medicine and lead author of the study.
The discovery highlighted how key these central brain regions are in regulating not only disorders of consciousness, but also conditions that impact attention and focus, such as attention deficit hyperactivity disorder. This finding could lead to better targeted medications and brain stimulation techniques for patients.
“This has also given us insights into how things work normally in the brain,” said senior author Hal Blumenfeld, the Mark Loughridge and Michele Williams Professor of Neurology who is also a professor in neuroscience and neurosurgery and director of the Yale Clinical Neuroscience Imaging Center. “It’s really a step forward in our understanding of awareness and consciousness.”
Looking across senses, this is the first time researchers have seen a result like this, said Khalaf, who is also part of Blumenfeld’s lab.
“It tells us how important this brain region is and what it could mean in efforts to restore consciousness,” she said.