Scientists identify a positive molecular feedback loop which could explain stroke-induced memory loss.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
In learning, neurons communicate with each other, and the connections between them getting stronger with repetition. This is known as long-term potentiation or LTP.
Another type of LTP occurs when the brain is deprived of oxygen temporarily – anoxia-induced long-term potentiation or aLTP. aLTP blocks the former process, thereby impairing learning and memory. Therefore, some scientists think that aLTP might be involved in memory problems seen in conditions like stroke.
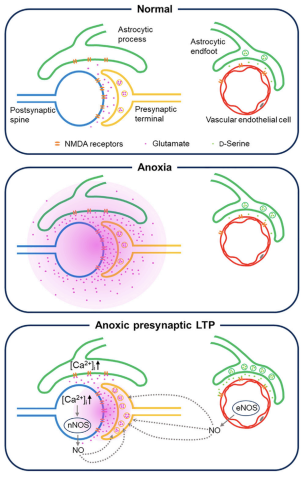
Researchers at the Okinawa Institute of Science and Technology (OIST) and their collaborators have studied the aLTP process in detail. They found that maintaining aLTP requires the amino acid glutamate, which triggers nitric oxide (NO) production in both neurons and brain blood vessels. This process forms a positive glutamate-NO-glutamate feedback loop. Their study, published in iScience, indicates that the continuous presence of aLTP could potentially hinder the brain’s memory strengthening processes and explain the memory loss observed in certain patients after experiencing a stroke.
The brain’s response to low oxygen
When there is a lack of oxygen in the brain, the neurotransmitter glutamate is released from neurons in large amounts. This increased glutamate causes the production of NO. NO produced in neurons and brain blood vessels boosts glutamate release from neurons during aLTP. This glutamate-NO-glutamate loop continues even after the brain gets enough oxygen.
“We wanted to know how oxygen depletion affects the brain and how these changes occur,” stated Dr Han-Ying Wang, a researcher in the former Cellular and Molecular Synaptic Function Unit at OIST and lead author of the study,. “It’s been known that nitric oxide is involved in releasing glutamate in the brain when there is a shortage of oxygen, but the mechanism was unclear.”
During a stroke, when the brain is deprived of oxygen, amnesia – the loss of recent memories – can be one of the symptoms. Investigating the effects of oxygen deficiency on the brain is important because of the potential medicinal benefits. “If we can work out what’s going wrong in those neurons when they have no oxygen, it may point in the direction of how to treat stroke patients,” Dr Patrick Stoney, a scientist in OIST’s Sensory and Behavioral Neuroscience Unit, explained.
Brain tissues from mice were placed in a saline solution, mimicking the natural environment in the living brain. Normally, this solution is oxygenated to meet the high oxygen demands of brain tissue. However, replacing the oxygen with nitrogen allowed the researchers to deprive the cells of oxygen for precise lengths of time.
The tissues were then examined under a microscope and electrodes were placed on them to record electrical activity of the individual cells. The cells were stimulated in a way that mimics how they would be stimulated in living mice.
Stopping memory and learning activity
The aLTP process is activated when the brain is temporarily deprived of oxygen and glutamate levels increase. If aLTP is maintained for an extended period, this hijacks the normal functioning of the memory strengthening process (LTP), resulting in memory loss. Blocking nitric oxide (NO) synthesis or the molecular pathways that boost glutamate release eventually stops aLTP. Credit: Wang et al., 2024
The scientists found that maintaining aLTP requires NO production in both neurons and in blood vessels in the brain. Collaborating scientists from OIST’s Optical Neuroimaging Unit showed that in addition to neurons and blood vessels, aLTP requires the activity of astrocytes, another type of brain cell. Astrocytes connect and support communication between neurons and blood vessels.
“Long-term maintenance of aLTP requires continuous synthesis of nitric oxide. NO synthesis is self-sustaining, supported by the NO-glutamate loop, but blocking molecular steps for NO-synthesis or those that trigger glutamate release eventually disrupt the loop and stop aLTP,” Prof. Tomoyuki Takahashi, leader of the former Cellular and Molecular Synaptic Function Unit at OIST, explained.
Notably, the cellular processes that support aLTP are shared by those involved in memory strengthening and learning (LTP). When aLTP is present, it hijacks molecular activities required for LTP and removing aLTP can rescue these memory enhancing mechanisms. This suggests that long-lasting aLTP may obstruct memory formation, possibly explaining why some patients have memory loss after a short stroke.
Prof Takahashi emphasised that the formation of a positive feedback loop formed between glutamate and NO when the brain is temporarily deprived of oxygen is an important finding. It explains long-lasting aLTP and may offer a solution for memory loss caused by a lack of oxygen.
Research by West Virginia University has demonstrated that American Heart Association and American Stroke Association guidelines are effective at speeding up hospitals’ response times for stroke treatment and can be mastered even by members of ‘ad hoc‘ medical teams that assemble rapidly on the fly.
When a stroke patient arrives at an emergency room, specialists from across hospital departments – emergency medical services, neurologists, pharmacists, physicians, nurses, radiologists and technicians – rush to coordinate a team response. AHA and ASA guidelines put specific limits on how much time can optimally elapse between the onset of ischaemic stroke, in which blood flow to the brain is blocked, and subsequent events like arrival at the hospital and delivery of an infusion.
But experts have questioned whether the communication of those best practices helps medical teams that assemble temporarily and whose members don’t typically collaborate. In a Journal of Operations Management article, WVU associate professor Bernardo Quiroga and coauthors answer that question using data about more than 8000 patients who received stroke care at a large hospital between 2009 and 2017.
“‘Time is brain’ for stroke victims,” Quiroga explained. “Blocked blood flow to the brain kills almost two million neurons a minute, so your life or ability to walk or talk hinges on how quickly multiple professionals coordinate to restore blood flow. If you’re lucky, you’re treated within the first hour of symptom onset. Better yet, you receive a shot of Tissue Plasminogen Activator, which dissolves clots. TPA works better the earlier it’s given and usually isn’t effective after 4.5 hours.”
In 2010, the AHA and ASA launched Target: Stroke, a program that identifies stroke care best practices and standardises each step in the process. Participating hospitals reduced median treatment times from 79 minutes in 2009 to 51 minutes in 2017, but it wasn’t clear if that improvement was driven by adherence to best practices or by clinicians learning through repetition as they handled more stroke cases.
To figure that out, the researchers investigated whether repeated ‘learning by doing’ decreased the hospital’s stroke care time. Then, they evaluated whether deliberate, ‘induced’ learning and implementation of AHA/ASA best practices decreased the time further.
Learning through repetition worked. The more strokes the hospital treated, the faster it responded. For each doubling of cumulative stroke alerts, ‘door-to-needle time’ – the time to get patients from the hospital door to a TPA infusion – decreased by 10.2%.
Best practices also worked. Specifically, the researchers examined two best practices: the Helsinki Model protocol, which directs that EMS staff keep stroke patients on the stretcher for transport to the CT room rather than transferring them to ER beds; and the Rapid Administration of TPA protocol, which requires the pharmacist to be in the CT room with TPA before completion of the CT scan. Those protocols significantly reduced the hospital’s door-to-needle time beyond improvements from repetition-based learning.
According to Quiroga’s coauthor and former PhD student Brandon Lee, that matters because it demonstrates the efficacy of best practices and shows ad hoc teams learning guidelines and implementing them long-term.
However, Lee emphasised the importance of the presence of the hospital’s stroke advisory committee, which set targets, evaluated stroke teams’ performances and gave feedback.
Without similar “countermeasures to organisational forgetting,” Quiroga acknowledged that best practices aren’t always sustainable, especially on ad hoc teams.
“In the case of the best practice indicated by the Helsinki Model, compliance is difficult because the hospital needs to coordinate with multiple independent EMS systems. Some EMS providers may be reluctant to commit resources to extended time in the CT room, and EMS staff turnover may lead to forgetting,” Quiroga said.
Lee added, “Overall, because ad hoc teams are fluid, information sharing is harder. And when a group of people don’t know each other well, group learning slows. But although ad hoc teams learn more slowly, we determined they still learn.”
The research also assessed whether neurologists’ abilities to meet time goals were affected by their recent experiences treating prior stroke patients.
“As team leaders, neurologists can have an outsized influence on performance,” Quiroga said. “Because other members of the ad hoc team aren’t familiar with each other, they lean on their leader.”
But data showed stroke teams improving response times regardless of how many stroke cases the neurologist had treated individually or what the neurologist’s recent success rate was. Quiroga said that’s good news.
“The implication is that learning and sustaining best practices ensures an even quality of care for patients, regardless of individual neurologists’ experience levels.”
The over-the-counter supplement nicotinamide riboside, a form of vitamin B3, increased the walking endurance of patients with peripheral artery disease, a chronic leg condition for which there are few effective treatments.
In a preliminary, randomised, double-blind clinical trial led by Northwestern University and University of Florida scientists, patients who took nicotinamide riboside daily for six months increased their timed walking distance by more than 17.3m, compared to a placebo group. As expected, walking speed declined in the placebo group, because peripheral artery disease causes progressive declines in walking performance.
“This is a signal that nicotinamide riboside could help these patients,” said Christiaan Leeuwenburgh, PhD, a UF professor of physiology and aging and senior author of the clinical trial report. “We are hoping to conduct a larger follow-up trial to verify our findings.”
Along with other researchers, Leeuwenburgh, whose research specialises in anti-aging treatments, collaborated with Mary M. McDermott, MD, a physician and professor of medicine at Northwestern University and an expert in peripheral artery disease.
The scientists recruited 90 people with an average age of 71 who had peripheral artery disease, or PAD, to test the effects of nicotinamide riboside. The supplement is increasingly popular as an anti-aging treatment (sales exceeded $60 million in 2022 in the US alone) but there has been scant evidence of any benefit in healthy people. Nicotinamide riboside is a precursor for the essential compound NAD, which plays roles in the body related to energy generation, improved blood flow and DNA repair.
Because PAD is associated with problems generating energy within muscle cells, McDermott and Leeuwenburgh thought that nicotinamide riboside, by improving energy generation, could help improve walking in people with the disease.
And indeed that’s what they found. Participants taking the supplement walked an average of 7m more in a six-minute walking test after six months, while those taking a placebo walked 10.3m less. Those who took at least 75% of the pills they were supposed to take performed even better, adding more than 30m to their walking distance, compared to people who took a placebo.
(The researchers also tested if resveratrol, a compound best known for being in red wine, could boost the effects of nicotinamide riboside; they found no additional benefits.)
PAD affects more than 8.5 million Americans over the age of 40. Caused by the buildup of fatty deposits in arteries, and associated with diabetes and smoking, the disease reduces blood flow to the limbs, especially the legs. Walking often becomes painful, and the disease typically causes declines in walking ability over time. Supervised walking exercise is first line therapy for PAD, but most people with the condition do not have access to supervised exercise.
In addition to a larger trial focused on patients suffering from PAD, Leeuwenburgh hopes to test the effects of nicotinamide riboside on walking performance in healthy older adults.
“We need to test it on a healthy older population before we recommend healthy people take it,” he said.
One of the biggest stories in HIV in the last year was that a class of medicines called statins could help reduce cardiovascular disease in people living with the virus. In response, treatment guidelines in the United States were quickly updated, but the picture is more complicated in South Africa. Spotlight’s Elri Voigt explores why the case for widespread use of statins by people living with HIV is less compelling in South Africa than in some other countries.
People living with HIV, provided they are stable on antiretroviral therapy, are affected by the same diseases as those who don’t have HIV, including cardiovascular disease, says Professor Mpiko Ntsekhe, head of Cardiology at Groote Schuur Hospital in Cape Town.
The key difference, he says, is that although both groups of people get the same spectrum of diseases, people living with HIV get those diseases more frequently and earlier. One way to think about this, he explains, is to imagine twins who are identical in every way except one is living with HIV. The twin living with HIV is more likely to get cardiovascular disease than the other twin.
And these differences can be substantial. Current evidence shows that people living with HIV have a twofold increased risk of developing cardiovascular disease compared to people not living with HIV, says Professor Hans Strijdom. He is the Head of the Division of Medical Physiology and Deputy Director of the Centre for Cardio-Metabolic Research in Africa (CARMA) at Stellenbosch University. The cardiovascular risk attributable to HIV, Strijdom adds, is now believed to be equivalent to that posed by traditional risk factors such as smoking. This prompted an editorial in 2018 in one of the top cardiovascular journals, Circulation, advocating for HIV to be recognised as a major cardiovascular risk factor.
He explains that people living with HIV who are stable on treatment are living longer, making them susceptible to the normal risk posed by older age. They also have “modifiable risk factors, in other words lifestyle risk factors”, like a higher smoking and alcohol use incidence, as well as increasing rates of being overweight and obesity. Strijdom says that living with HIV, even when someone is stable on treatment, causes low-grade inflammation, which over time increases a person’s risk for cardiovascular disease. “That all in combination are the current theories [of] why we think that they have a bigger risk of cardiovascular disease,” he says.
Important study findings
Arguably, the biggest news from last year’s International AIDS Society (IAS) Conference in Australia was findings from a study on heart disease in people living with HIV. The trial, called REPRIEVE, showed that a class of cholesterol-busting drugs called statins can prevent a lot of cardiovascular disease events in people living with HIV whose cardiovascular disease (CVD) risk score meets a certain threshold. Spotlight previously reported on these findings, which showed that compared to placebo, daily treatment with 4mg oral pitavastatin – a specific statin – led to a 35% reduction in major adverse cardiovascular events (MACE) in people living with HIV classified to be at risk of cardiovascular disease.
When the findings were presented at the IAS conference, the study’s principal investigator, Dr Steven Grinspoon, said that while the researchers still have to assess more of the data collected to get a clearer picture of things, like the mechanisms driving cardiovascular disease across regions and conduct additional sub-group analyses, the study has already shown that using pitavastatin can save lives.
These sub-group analyses were discussed in greater detail at the Conference on Retroviruses and Opportunistic Infections (CROI) held in Denver in March this year. For the most part, the use of pitavastatin in the manner prescribed by REPRIEVE was considered a huge success, and the United States has since changed its guidelines to include the use of statins in the primary prevention of atherosclerotic cardiovascular disease.
Why it is different in South Africa
However, for low-and-middle-income countries like South Africa, the case for pitavastatin might not be as clear-cut. In fact, a panel discussion at CROI was dedicated to exploring the implications of the REPRIEVE findings for such countries.
Ntsekhe, who was a speaker on the CROI panel, tells Spotlight that data from REPRIEVE’s sub-group analyses reveal there was a striking difference in event rates – which in the case of the study are MACE in those who were getting the placebo – by country income status. He explains that as predicted in high-income countries, the event rates were high, while in low-and-middle income countries – particularly in Sub-Saharan Africa – event rates were very low.
He says one of the reasons for the difference in event rates was that the screening tool used in REPRIEVE worked well to identify those people living with HIV who might benefit from pitavastatin in high-income countries like the United States, but it did not work well in Sub-Saharan Africa.
This means using pitavastatin as part of a primary prevention strategy is a much more effective intervention in high-income countries than in low-and-middle income countries like in Sub-Saharan Africa because the cardiovascular disease profile is so different.
Ntsekhe explains the term cardiovascular disease itself is broad and all-encompassing and there are many forms, including valve disease, heart muscle disease, and vascular disease. The dominant form of cardiovascular disease in the high-income countries (which he refers to as the Global North) is known as atherosclerotic cardiovascular disease, which is characterised by a build-up of fatty deposits and plaque in the arteries.
In Sub-Saharan Africa though, Ntsekhe says “atherosclerotic cardiovascular disease is but one of many forms of cardiovascular disease”, taking the fourth or fifth place in the ranking of types of major heart disease.
Research conducted in high-income countries don’t always take differences in disease burden into account, according to Ntsekhe. This means that interventions researched in high-income countries and shown to be effective in that context won’t necessarily work as well in low-and-middle income countries like South Africa.
Strijdom concurs that while results from REPRIEVE in the global context were a game-changer, the findings are not easily transferable to South Africa’s context because pitavastatin is mainly aimed at reducing “bad cholesterol” and coronary artery disease (also called atherosclerosis).
‘Taking money away’
During the panel discussion at CROI, Ntsekhe asked whether Sub-Saharan Africa could justify taking money away from other health programmes that work in order to invest in pitavastatin.
“I said basically what should be a priority for us is a) finding tools that can better identify those at risk and b) continuing to focus on what our local data suggests are the priority areas,” Ntsekhe says.
“If your entire prevention strategy is aimed at atherosclerotic cardiovascular disease, but it isn’t the dominant cause of disease [in your country], you’re going to be treating a whole host of people to try and tackle this thing that affects very few in a sense,” he says.
“It was not anything about REPRIEVE, it was a wonderful study, the hypothesis was tested, and it was shown to be correct, the intervention we know works,” Ntsekhe says. “It really then comes down to regional areas to think very carefully about how best they’re going to get their biggest bang for their buck,” he says. “We have to carefully consider the local context, local burden, we have set local health priorities, and weigh benefit and cost before we adopt new interventions or recommendations.”
SA’s cardiovascular disease burden
While Strijdom says we don’t have great data, he points to a large systematic review and meta-analysis published in 2018 in Circulation, which estimates that around 15% of the total cardiovascular disease burden in South Africa is attributable to HIV. “It’s probably higher than that. I would say that probably about one in five people with heart disease have heart disease because of HIV in South Africa,” he says, adding “that figure is probably only going to increase”.
Because of this, he says, there is a need for proper and clear primary healthcare guidelines specifically aimed at managing cardiovascular disease in people living with HIV, which we don’t currently have.
Strijdom says what we have at the moment since the rollout of the 2019 National ART Clinical Guidelines is very basic guidelines. This involves screening someone who has just been diagnosed with HIV by taking their blood pressure, and testing urine for glucose and proteins, and an assessment of their general cardiovascular disease risk by taking their medical and family history. These guidelines, according to Strijdom, only make provision for routine screening at baseline, but screening guidelines at follow-up visits are insufficient.
“I am, however, aware of the fact that there is progress especially from the integrated chronic disease management model which is currently being piloted in South Africa – and hopefully with that will come much more definitive and universal guidelines,” he says. “The bottom line is that South Africa, in its public health [sector] especially, really very quickly needs to come up with very clear and more comprehensive guidelines to actively manage cardiovascular disease risk in people with HIV.”
Need for annual screening
Strijdom suggest that to improve screening for cardiovascular disease risk in people living with HIV, there needs to be annual screening of people’s weight, their measure of body fat based on height and weight, waist circumference, blood pressure, cholesterol and triglyceride levels as well as testing urine samples for kidney function. There also needs to be a thorough family and medical history conducted for each patient.
“It’s not really a very expensive or very exhaustive list of stuff that you have to do. Unless of course they have specific symptoms and signs that leads you in a specific direction that you then have to perhaps do an ECG [a test used to evaluate the functioning of the heart] or cardiac imaging but that is usually determined by what you get from their history and clinical examination,” he says.
Ntsekhe says public health strategies to combat the growing burden of non-communicable diseases (NCDs), including cardiovascular disease, in South Africa must be strengthened. These include screening and prevention tools like checking a patient’s blood pressure and blood glucose, advising against smoking and alcohol as well as promoting health lifestyle choices like exercise and weight loss. These interventions should be offered to everyone, regardless of whether they are living with HIV or not, he says.
“The thing about NCDs and cardiovascular disease, for the most part, they are diseases of lifestyle and behaviour. So, when you talk prevention, it’s not always about drug prevention,” he says. “It’s more about intensification of those [interventions] that are already in the public domain, are very effective, and cost very little. Many of the public health and primary healthcare guidelines do advise local ministries, local health authorities on what should be happening.”
In terms of public education, Stritjdom says people need to be aware that there is something like high blood pressure. “If people are aware they will come to the clinic and will say please measure my blood pressure,” he says.
“Our health system is understandably focused on infectious diseases, but if we are not careful, we will then be totally unprepared to tackle the epidemic that will have replaced it. Namely, cancer, heart disease, stroke, obesity, diabetes, and it will totally overwhelm our public healthcare system,” he says.
Cleveland Clinic researchers found higher amounts of the sugar alcohol xylitol are associated with increased risk of cardiovascular events like heart attack and stroke. They confirmed the association in a large-scale patient analysis, preclinical research models and a clinical intervention study, published in the European Heart Journal.
Xylitol is a common sugar substitute used in sugar-free candy, gums, baked goods and oral products like toothpaste. Over the past decade, the use of sugar substitutes, including sugar alcohols and artificial sweeteners, has increased significantly in processed foods that are promoted as healthy alternatives.
The team, led by Stanley Hazen, MD, PhD, had also previously revealed a similar link between erythritol and cardiovascular risk last year. Xylitol is not as prevalent as erythritol in keto or sugar-free food products in the US but is common in other countries.
“This study again shows the immediate need for investigating sugar alcohols and artificial sweeteners, especially as they continue to be recommended in combatting conditions like obesity or diabetes,” said Dr Hazen. “It does not mean throw out your toothpaste if it has xylitol in it, but we should be aware that consumption of a product containing high levels could increase the risk of blood clot related events.”
In this new study, researchers identified that high levels of circulating xylitol were associated with an elevated three-year risk of cardiovascular events in an analysis of more than 3000 patients in the US and Europe. A third of patients with the highest amount of xylitol in their plasma were more likely to experience a cardiovascular event. To confirm the findings, the research team conducted pre-clinical testing and found that xylitol caused platelets to clot and heightened the risk of thrombosis. Researchers also tracked platelet activity from people who ingested a xylitol-sweetened drink versus a glucose-sweetened drink and found that every measure of clotting ability significantly increased immediately following ingestion of xylitol but not glucose.
The authors note that further studies assessing the long-term cardiovascular safety of xylitol are warranted. The research had several limitations, including that clinical observation studies demonstrate association and not causation.
Blocking a protein known as CDK7 could prevent heart damage associated with the commonly used cancer chemo drug doxorubicin, according to a study led by scientists at Washington State University. Importantly, the researchers also found that inhibiting CDK7 could help enhance the drug’s cancer-killing capability.
Based on an animal model, the study findings could provide a foundation for future treatment strategies to reduce chemotherapy-related heart toxicity and increase treatment effectiveness. This could ultimately help increase the lifespan of people with cancer. Heart damage related to chemotherapy treatment can surface decades after treatment and can result in heart attacks, heart failure, cardiomyopathy and other types of heart disease.
Published in the journal Cardiovascular Research, the WSU study focused on doxorubicin, a chemotherapy drug used to treat breast cancer, lymphoma, leukaemia and other cancers. Capable of killing a wide range of cancer cells, doxorubicin and other similar chemotherapy medications are known to be toxic to the heart. Despite this toxicity, the drug still sees a lot of use.
“Doxorubicin remains the mainstay treatment for certain cancer types for which targeted therapies or other better treatments are not available,” said senior study author Zhaokang Cheng, an associate professor in the WSU College of Pharmacy and Pharmaceutical Sciences.
Cheng has been working to unravel the underlying mechanisms of doxorubicin-induced heart toxicity to make the use of doxorubicin safer for patients who rely on the drug. This new study builds on findings from earlier research that showed that doxorubicin activates a protein known as CDK2. That protein then activates another known as FOXO1, which causes heart cells to die. Cheng’s team collaborated with WSU cancer biology researcher Boyang (Jason) Wu to take a closer look at CDK7, a protein that helps fuel cell growth and has been shown to play a role in the development of cancer.
The researchers found that CDK7 activated CDK2, which set off the chain of molecular signals that eventually led to heart cell death. They also showed that mice that lacked the CDK7 gene were protected from doxorubicin-induced heart toxicity. Next, they used a CDK7 inhibitor drug known as THZ1 to block the protein’s activity and examine the impact on heart health and cancer growth. A similar inhibitor is currently being tested as an anticancer drug in clinical trials, but its effect on the heart is still not clear.
“We are the first to study the effect of THZ1 on the heart and on tumor growth in the same model,” said study first author Jingrui Chen, a WSU research associate. “And what we found is that this CDK7 inhibitor drug can increase heart function and at the same time inhibit tumour growth.”
Though more research is needed, the researchers said their findings suggest that combining doxorubicin and THZ1 could help prevent heart damage and increase the effectiveness of chemotherapy treatment.
The researchers’ next step is to test the effect of THZ1 on heart damage and cancer growth in younger mice and follow them longer. This would more closely mimic long-term doxorubicin-induced heart toxicity seen in childhood cancer survivors. They also plan to look at other proteins that may somehow be involved in the signaling pathway that underlies doxorubicin-related heart damage.
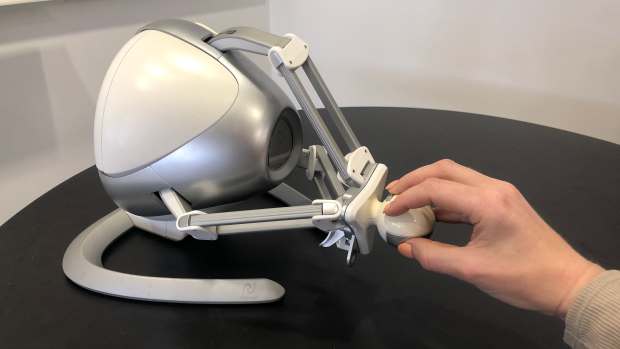
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller.
For recovering stroke survivors, getting intensive, frequent rehabilitation therapy to help restore fine motor skills can be challenging and expensive.
Now, researchers at NYU Tandon School of Engineering are developing a new technology that could allow stroke patients to undergo rehabilitation exercises at home by tracking their wrist movements through a simple setup: a smartphone strapped to the forearm and a low-cost gaming controller called the Novint Falcon.
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller. But it cannot directly measure the angle of the user’s wrist, which is essential data for therapists providing remote rehabilitation.
“Patients would strap their phone to their forearm and manipulate this robot,” said Maurizio Porfiri, NYU Tandon Institute Professor and director of its Center for Urban Science + Progress (CUSP), who is the paper’s senior author. “Data from the phone’s inertial sensors can then be combined with the robot’s measurements through machine learning to infer the patient’s wrist angle.”
The researchers collected data from a healthy subject performing tasks with the Falcon while wearing motion sensors on the forearm and hand to capture the true wrist angle. They then trained an algorithm to predict the wrist angles based on the sensor data and Falcon controller movements.
The resulting algorithm could predict wrist angles with over 90% accuracy, a promising initial step toward enabling remote therapy with real-time feedback in the absence of an in-person therapist.
“This technology could allow patients to undergo rehabilitation exercises at home while providing detailed data to therapists remotely assessing their progress,” Roni Barak Ventura, the paper’s lead author who was an NYU Tandon postdoctoral fellow at the time of the study. “It’s a low-cost, user-friendly approach to increasing access to crucial post-stroke care.”
The researchers plan to further refine the algorithm using data from more subjects. Ultimately, they hope the system could help stroke survivors stick to intensive rehab regimens from the comfort of their homes.
This study adds to NYU Tandon’s body of work that aims to improve stroke recovery. In 2022, Researchers from NYU Tandon began collaborating with the FDA to design a regulatory science tool based on biomarkers to objectively assess the efficacy of rehabilitation devices for post-stroke motor recovery and guide their optimal usage. A study from earlier this year unveiled advances in technology that uses implanted brain electrodes to recreate the speaking voice of someone who has lost speech ability, which can be an outcome from stroke.
Inflammatory bowel disease (IBD) is associated with a slightly increased risk of heart failure up to 20 years after diagnosis, according to a comprehensive registry study from Karolinska Institutet published in the European Heart Journal.
The researchers analysed the risk of heart failure in over 80 000 patients with inflammatory bowel disease, that is, Crohn’s disease, ulcerative colitis or unclassified IBD, compared with 400 000 people from the general population, as part of the ESPRESSO study.
The results show that people with IBD have a 19% increased risk of developing heart failure up to 20 years after diagnosis. This corresponds to one extra heart failure case per 130 IBD patients in those 20 years, and the risk increase was seen regardless of the type of IBD. The highest risk of heart failure was seen in older patients, people with lower education and people with pre-existing cardiovascular-related disease at IBD diagnosis.
Contribute to new guidelines
“Both healthcare providers and patients should be aware of this increased risk, and it’s important that cardiovascular health is properly monitored,” says the study’s first author Jiangwei Sun, researcher at the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet. “We hope the results will raise the awareness of health workers as to the increased risk of heart failure in individuals with IBD and contribute to new guidelines for cardiovascular disease management in IBD patients.”
Comparing siblings with and without ABD, the risk increase was slightly lower, 10%, suggesting that genetics and early environmental factors shared within families may play a role.
“We don’t know if there is a causal relationship, but we will continue to explore genetic factors and the role of IBD medications and disease activities on the risk of heart failure,” says the study’s senior author Professor Jonas F. Ludvigsson from the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet.
Cerebrovascular accidents, or strokes, are the most common cause of aphasia, a speech disorder of cerebral origin. People with aphasia have a reduced ability to understand or produce speech or written language. An estimated 40% of people who have had a stroke have aphasia. As many as half of them experience aphasia symptoms even a year after the original attack.
Researchers at the University of Helsinki previously found that sung music helps in the language recovery of patients affected by strokes. Now, the researchers have uncovered the reason for the rehabilitative effect of singing. The recently completed study was published in the eNeuro journal.
According to the findings, singing, as it were, repairs the structural language network of the brain. The language network processes language and speech in the brain, which has been damaged.
“For the first time, our findings demonstrate that the rehabilitation of patients with aphasia through singing is based on neuroplasticity changes, that is, the plasticity of the brain,” says University Researcher Aleksi Sihvonen from the University of Helsinki.
Singing improves language network pathways
The language network encompasses the cortical regions of the brain involved in the processing of language and speech, as well as the white matter tracts that convey information between the different end points of the cortex.
According to the study results, singing increased the volume of grey matter in the language regions of the left frontal lobe and improved tract connectivity especially in the language network of the left hemisphere, but also in the right hemisphere.
“These positive changes were associated with patients’ improved speech production,” Sihvonen says.
A total of 54 aphasia patients participated in the study, of whom 28 underwent MRI scans at the beginning and end of the study. The researchers investigated the rehabilitative effect of singing with the help of choir singing, music therapy and singing exercises at home.
Singing is a cost-effective treatment
Aphasia has a wide-ranging effect on the functional capacity and quality of life of affected individuals and easily leads to social isolation.
According to Sihvonen, singing can be seen as a cost-effective addition to conventional forms of rehabilitation, or as rehabilitation for mild speech disorders in cases where access to other types of rehabilitation is limited.
“Patients can also sing with their family members, and singing can be organised in healthcare units as a group-based, cost-efficient rehabilitation,” Sihvonen says.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
A new study led by investigators from Brigham and Women’s Hospital has developed a new test by combining blood-based biomarkers with a clinical score to identify patients experiencing large vessel occlusion (LVO) stroke with high accuracy. Their results are published in the journal Stroke: Vascular and Interventional Neurology.
“We have developed a game-changing, accessible tool that could help ensure that more people suffering from stroke are in the right place at the right time to receive critical, life-restoring care,” said senior author Joshua Bernstock, MD, PhD, MPH, a clinical fellow in the Department of Neurosurgery at Brigham and Women’s Hospital.
Most strokes are ischaemic, in which blood flow to the brain is obstructed. LVO strokes are an aggressive type of ischaemic stroke that occurs when an obstruction occurs in a major artery in the brain, causing brain cells to rapidly die off from lack of oxygen. Major medical emergencies, LVO strokes require the swift treatment with mechanical thrombectomy, a surgical procedure that retrieves the blockage.
“Mechanical thrombectomy has allowed people that otherwise would have died or become significantly disabled be completely restored, as if their stroke never happened,” said Bernstock. “The earlier this intervention is enacted, the better the patient’s outcome is going to be. This exciting new technology has the potential to allow more people globally to get this treatment faster.”
The research team previously targeted two specific proteins found in capillary blood, one called glial fibrillary acidic protein (GFAP), which is also associated with brain bleeds and traumatic brain injury, and one called D-dimer. In this study, they demonstrated that the levels of these blood-based biomarkers combined with field assessment stroke triage for emergency destination (FAST-ED) scores could identify LVO ischaemic strokes while ruling out other conditions such as bleeding in the brain. Brain bleeds cause similar symptoms to LVO stroke, making them hard to distinguish from one another in the field, yet treatment for each is vastly different.
In this prospective, observational diagnostic accuracy study, the researchers looked at data from a cohort of 323 patients coded for stroke in Florida between May 2021 and August 2022. They found that combining the levels of the biomarkers GFAP and D-dimer with FAST-ED data less than six hours from the onset of symptoms allowed the test to detect LVO strokes with 93% specificity and 81% sensitivity. Other findings included that the test ruled out all patients with brain bleeds, suggesting that it may also eventually be used to detect intracerebral haemorrhage in the field.
Bernstock’s team also sees promising potential future use of this accessible diagnostic tool in low- and middle-income countries, where advanced imaging is not always available. It might also be useful in assessing patients with traumatic brain injuries. Next, they are carrying out another prospective trial to measure the test’s performance when used in an ambulance. They have also designed an interventional trial that leverages the technology to expedite the triage of stroke patients by having them bypass standard imaging and move directly to intervention.
“In stroke care, time is brain,” Bernstock said. “The sooner a patient is put on the right care pathway, the better they are going to do. Whether that means ruling out bleeds or ruling in something that needs an intervention, being able to do this in a prehospital setting with the technology that we built is going to be truly transformative.