From genetics to stress myths, researchers reveal what really drives greying and the breakthroughs pointing to natural colour restoration
Photo by Ravi Patel on Unsplash
Grey hair is more than a cosmetic concern – it drives a booming industry, influences how people are perceived, and can affect confidence. Globally, the hair colour market was valued at nearly USD 28 billion in 2025, with over half of purchases linked specifically to concealing greys. In South Africa, spending on hair colourants is projected to grow from roughly USD 172 million in 2021 to over USD 228 million by 2028, highlighting the demand for solutions that go beyond temporary cover-ups.
By age 50, roughly 50-70% of adults have visible grey hair, while premature greying can appear in some as early as the 20s. The psychological weight is clear: studies indicate grey hair can make people appear 20-30% older, influencing workplace perception, social interactions, and self-esteem. Studies show faces with grey hair are consistently perceived as more subdued than the same faces without greys, confirming that hair colour alone can shape social impressions.
“Many popular beliefs about greying hair are misleading,” says Dr Kashmal Kalan, Medical Director at Alvi Armani. “Stress does not turn hair grey overnight, plucking one strand won’t trigger several more, and no supplement or home remedy has been proven to restore pigment reliably. The reality is far more biological – genetics and pigment cell behaviour are the keys we are finally beginning to understand.”
At the heart of greying are melanocyte stem cells (McSCs) within hair follicles. In youth, these cells migrate and maintain melanin production, the pigment responsible for hair colour. With age, many become inactive or “trapped,” interrupting pigment delivery and causing grey strands. In mouse models, freeing these cells restored pigment production in roughly half of cases – a major step toward therapies that could reawaken natural colour without dyes.
Emerging research aims to tackle the root cause rather than just the appearance of grey hair. Scientists are exploring topical agents that target dormant pigment cells, metabolic modulators that influence follicle behaviour, and activation therapies designed to revive pigment production. These innovations could allow hair to regain its natural shade – not just cover it – while supporting overall follicle health.
“We are witnessing science that was once purely theoretical become reality,” says Dr Sunaina Paima, aesthetic and hair-restoration physician at Alvi Armani Johannesburg. “For patients, this could mean seeing grey strands regain their original shade naturally – a moment the hair science world has long dreamed of. The potential impact on confidence and self-esteem is enormous, because this isn’t just about covering colour, it’s about restoring it at a biological level.”
While most pigment-restoring therapies remain in development, advances in genetics, dermatology, and biotechnology are converging at unprecedented speed. “For decades, grey hair was seen as an irreversible hallmark of ageing,” adds Dr Kalan. “Today, that assumption is being seriously challenged. We’re on the brink of options that rejuvenate hair from the inside out, not just cosmetically.”
These breakthroughs signal a new era in hair science: ageing hair may no longer be inevitable or purely cosmetic, but a biological process that can be understood, guided, and ultimately restored.
An analysis led by Mass General Brigham investigators found slower aging in older adults after two years of a daily multivitamin, with greater benefits for those who began the trial with accelerated biological age.
‘Biological age’, age on a cellular level, can differ from chronological age. Using data from a large randomised clinical trial of older adults, researchers at Mass General Brigham evaluated the effects of taking a daily multivitamin over the course of two years on five measures of biological ageing and found a slowing equivalent to about four months of ageing. The benefits were increased in those who were biologically older than their actual age at the start of the trial. Their results are published in Nature Medicine.
“There is a lot of interest today in identifying ways to not just live longer, but to live better,” said senior author Howard Sesso, ScD, MPH, associate director of the Division of Preventive Medicine in the Mass General Brigham Department of Medicine. “It was exciting to see the benefits of a multivitamin linked with markers of biological ageing. This study opens the door to learning more about accessible, safe interventions that contribute to healthier, higher-quality ageing.”
Epigenetic clocks estimate biological ageing based specific sites in our DNA that regulate gene expression (known as DNA methylation) and change naturally as we get older, helping track mortality and the pace of ageing. This study, which uses data from the well-established COcoa Supplement Multivitamins Outcomes Study (COSMOS), analysed DNA methylation data from blood samples of 958 randomly selected healthy participants with an average chronological age of 70.
The study participants were randomised to take a daily cocoa extract and multivitamin; daily cocoa extract and placebo; placebo and multivitamin; or placebos only. Samples were analysed for changes in five epigenetic clocks from the start of the trial and at the end of the first and second years. Compared to the placebo only group, people in the multivitamin group had slowing in all five epigenetic clocks, including statistically significant slowing seen in the two clocks that are predictive of mortality. The changes equated to about four months less biological ageing over the course of two years. Additionally, people who were biologically older than their actual age at the start of the trial benefited the most.
“We plan to do follow-up research to determine if the slowing of biological ageing – observed through these five epigenetic clocks, and additional or new ones – persists after the trial ends,” said co-author and collaborator Yanbin Dong, MD, PhD, director of Georgia Prention Institute, Medical College of Georgia at Augusta Univeristy.
Further studies are also needed to determine how improvements in biological aging may explain reductions in clinical outcomes. The COSMOS team plans to investigate how the effects of a daily multivitamin on biological aging may extend to different outcomes they have seen evidence of benefits for, such as improvements in cognition and reductions in cancer and cataracts.
“A lot of people take a multivitamin without necessarily knowing any benefits from taking it, so the more we can learn about its potential health benefits, the better,” said Sesso. “Within COSMOS, we are fortunate and excited to build upon a rich resource of biomarker data to test how two interventions may improve biological aging and reduce age-related clinical outcomes.”
Ageing in later life is often portrayed as a steady slide toward physical and cognitive decline. But a new study by scientists at Yale University suggests an alternate narrative – that older individuals can and do improve over time and their mindset toward ageing plays a major part in their success.
Analysing more than a decade of data from a large, nationally representative study of older Americans, lead author Becca R. Levy, a professor of social and behavioural sciences at the Yale School of Public Health (YSPH), found that nearly half of adults aged 65 and older showed measurable improvement in cognitive function, physical function, or both, over time.
The improvements were not limited to a small group of exceptional individuals and, notably, were linked to a powerful but often overlooked factor: how people think about ageing itself.
“Many people equate ageing with an inevitable and continuous loss of physical and cognitive abilities,” said Levy, an international expert on psychosocial determinants of ageing health. “What we found is that improvement in later life is not rare, it’s common, and it should be included in our understanding of the ageing process.”
The findings are published in the journal Geriatrics.
For the study, the researchers followed more than 11 000 participants in the Health and Retirement Study, a federally supported longitudinal survey of older Americans. The research team tracked changes in cognition using a global performance assessment, and physical function using walking speed — often described by geriatricians as a “vital sign” because of its strong links to disability, hospitalisation, and mortality.
Over a follow-up period of up to 12 years, 45% of participants improved in at least one of the two domains, according to the study. About 32% improved cognitively, 28% improved physically, and many experienced gains that exceeded thresholds considered clinically meaningful. When participants whose cognitive scores remained stable over that period (rather than declining) were included, more than half defied the stereotype of inevitable deterioration in cognition.
“What’s striking is that these gains disappear when you only look at averages,” said Levy, author of the book “Breaking the Age Code: How Your Beliefs About Aging Determine How Long & How Well You Live.” “If you average everyone together, you see decline. But when you look at individual trajectories, you uncover a very different story. A meaningful percentage of the older participants that we studied got better.”
The authors also examined potential reasons for why some people improve and some do not. They hypothesized that an important factor could be participants’ baseline age beliefs — or, specifically, whether they had assimilated more positive or more negative views about ageing by the start of the study. In support of this hypothesis, they found that those with more positive age beliefs were significantly more likely to show improvements in both cognition and walking speed, even after accounting for factors such as age, sex, education, chronic disease, depression, and length of follow-up.
The findings build on Levy’s stereotype embodiment theory, which posits that age stereotypes absorbed from culture – through a range of domains including social media and advertisements – eventually become self-relevant and biologically consequential. Levy’s prior studies have found negative age beliefs predict poorer memory, slower walking speed, higher cardiovascular risk, and biomarkers associated with Alzheimer’s disease.
The current study shows that those who have assimilated more positive age beliefs often show improvement, Levy said.
“Our findings suggest there is often a reserve capacity for improvement in later life,” she said. “And because age beliefs are modifiable, this opens the door to interventions at both the individual and societal level.”
The improvements were not limited to people who started out with impairments. Even among participants who had normal cognitive or physical function at baseline, a substantial proportion improved over time. That challenges the assumption that later-life gains reflect only people getting better after being sick or rebounding from earlier setbacks, the authors said.
The authors hope their findings will reverse the popular perception that continuous decline is inevitable and encourage policy makers to increase their support for preventive care, rehabilitation, and other health-promoting programs for older persons that draw on their potential resilience.
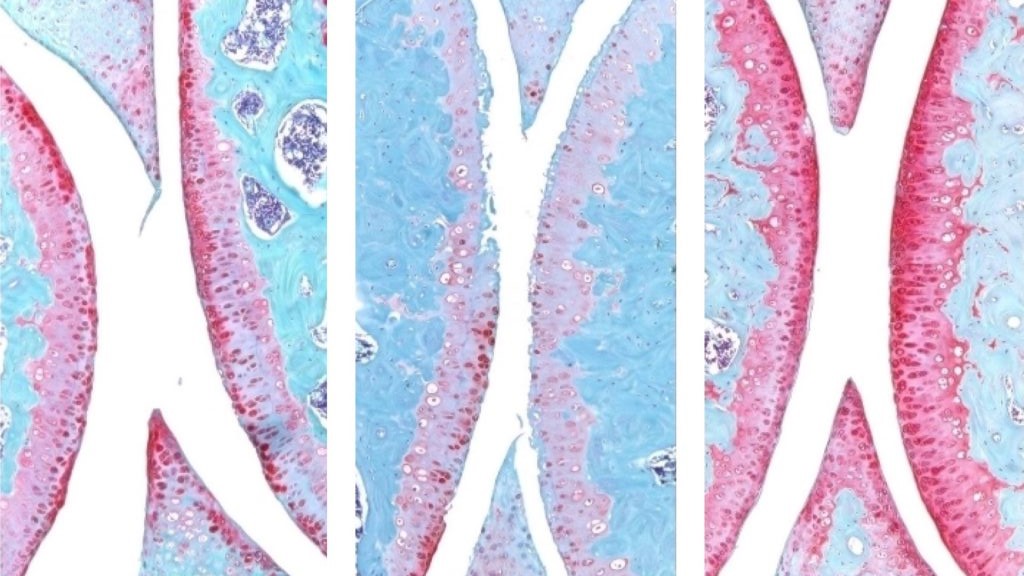
The knee joint of a young mouse (left), aged mouse (middle) and treated aged mouse (right). The red indicates cartilage. Credit: Nidhi Bhutani
An injection that blocks the activity of a protein involved in ageing reverses naturally occurring cartilage loss in the knee joints of old mice, a Stanford Medicine-led study has found. The treatment also prevented the development of arthritis after knee injuries mirroring the ACL tears often experienced by athletes or recreational exercisers. An oral version of the treatment is already in clinical trials with the goal of treating age-related muscle weakness.
Samples of human tissue from knee replacement surgeries – which include both the extracellular scaffolding, or matrix, in the joint as well as cartilage-generating chondrocyte cells – also responded to the treatment by making new, functional cartilage.
The study results suggest it may be possible to regenerate cartilage lost to ageing or arthritis with an oral drug or local injection, rendering knee and hip replacement unnecessary.
The treatment directly targets the cause of osteoarthritis, a disease for which no drug can slow down or reverse its progress; the primary treatments for osteoarthritis are pain control and surgical replacement of the affected joints.
The protein, 15-PGDH – termed a gerozyme due to its increase in prevalence as the body ages – is a master regulator of ageing. Gerozymes, identified by the same researchers in 2023, also drive the loss of tissue function. They are a major force behind age-related loss of muscle strength in mice. Blocking the function of 15-PGDH with a small molecule results in an increase in old animals’ muscle mass and endurance. Conversely, expressing15-PGDH in young mice causes their muscles to shrink and weaken. The gerozyme has also been implicated in the regeneration of bone, nerve and blood cells.
In each of these tissues, regeneration is due to increases in the proliferation and specialisation of tissue-specific stem cells. However, chondrocytes change their patterns of gene expression to assume a more youthful state without the involvement of stem cells.
“This is a new way of regenerating adult tissue, and it has significant clinical promise for treating arthritis due to ageing or injury,” said Helen Blau, PhD, professor of microbiology and immunology. “We were looking for stem cells, but they are clearly not involved. It’s very exciting.”
“Millions of people suffer from joint pain and swelling as they age,” Bhutani said. “It is a huge unmet medical need. Until now, there has been no drug that directly treats the cause of cartilage loss. But this gerozyme inhibitor causes a dramatic regeneration of cartilage beyond that reported in response to any other drug or intervention.”
There are three main types of cartilage in the human body. One, elastic cartilage, is soft and flexible and forms structures like the outer ear. A second, fibrocartilage, is dense and tough, absorbing shock in areas such as between the spinal vertebrae. The third, hyaline cartilage, is smooth and glossy, providing a low-friction surface for lubrication and flexibility in joints like the ankles, hips, shoulders and parts of the knee. Hyaline cartilage, also known as articular cartilage, is the cartilage most commonly affected by osteoarthritis.
Osteoarthritis occurs when a joint is stressed by ageing, injury or obesity. The chondrocytes begin to release pro-inflammatory molecules and to break down collagen, which is the primary structural protein of cartilage. When collagen is lost, the cartilage thins and softens; the accompanying inflammation causes the joint swelling and pain that are hallmarks of the disease. Under normal circumstances, articular cartilage rarely regenerates. Although some populations of putative stem or progenitor cells capable of generating cartilage have been identified in bone, attempts to identify similar populations of cells in the articular cartilage have been unsuccessful.
Previous research from Blau’s lab has shown that a molecule called prostaglandin E2 is essential to muscle stem cell function. 15-PGDH degrades prostaglandin E2. Inhibiting 15-PGDH activity, or increasing levels of prostaglandin E2, supports the regeneration of damaged muscle, nerve, bone, colon, liver and blood cells in young mice.
Blau, Bhutani and their colleagues wondered if 15-PGDH might also play a role in ageing cartilage and joints. They wanted to find out if a similar pathway contributes to cartilage loss from ageing or in response to injury. When they compared the amount of 15-PGDH in the knee cartilage in young versus old mice, they saw that, as in other tissues, levels of the gerozyme increased about two-fold with age.
They next experimented with injecting old animals with a small molecule drug that inhibits 15-PGDH activity – first into the abdomen, which affects the entire body, then directly into the joint. In each case, the knee cartilage, which was markedly thinner and less functional in older animals as compared with younger mice, thickened across the joint surface. Further experiments confirmed that the chondrocytes in the joint were generating hyaline, or articular, cartilage, rather than less-functional fibrocartilage.
“Cartilage regeneration to such an extent in aged mice took us by surprise,” Bhutani said. “The effect was remarkable.”
Addressing ACL tears
Similar results were observed in animals with knee injuries like the ACL tears that frequently occur in people participating in sports such as soccer, basketball and skiing that require sudden pivoting, stopping or jumping. While the tears can be surgically repaired, about 50% of people develop osteoarthritis in the injured joint within about 15 years.
The researchers found that a series of injections twice a week for four weeks of the gerozyme inhibitor after injury dramatically reduced the chance that osteoarthritis develops in the mice. Animals treated with a control drug had levels of 15-PGDH that were twice as high as in their uninjured peers, and they developed osteoarthritis within four weeks.
The animals treated with the gerozyme inhibitor also moved more typically and put more weight on the paw of the affected leg than did untreated animals.
“Interestingly, prostaglandin E2 has been implicated in inflammation and pain,” Blau said. “But this research shows that, at normal biological levels, small increases in prostaglandin E2 can promote regeneration.”
A closer investigation of the chondrocytes in the joints of old mice and young mice showed that old chondrocytes expressed more detrimental genes involved in inflammation and the conversion of hyaline cartilage to unwanted bone, and fewer genes involved in cartilage development.
The researchers were also able to pinpoint subcategories of old chondrocytes that change their patterns of gene expression after treatment. One, which expresses 15-PGDH and genes involved in cartilage degradation, decreased in prevalence from 8% to 3% after treatment. Another, which does not express 15-PGDH but does express genes involved in the production of fibrocartilage, also decreased in prevalence: from 16% to 8% after treatment. A third population, which does not make 15-PGDH and which expresses genes involved in hyaline cartilage formation and the maintenance of the extracellular matrix necessary for its function, increased in prevalence after treatment from 22% to 42%. The findings indicate an overall shift in gene expression after treatment to a more youthful cartilage composition – without the involvement of stem or progenitor cells.
Finally, the researchers studied human cartilage tissue removed from patients with osteoarthritis undergoing total knee replacements. Tissue treated with the 15-PGDH inhibitor for one week exhibited lower levels of 15-PGDH-expressing chondrocytes and lowered cartilage degradation and fibrocartilage genes than control tissue and began to regenerate articular cartilage.
“The mechanism is quite striking and really shifted our perspective about how tissue regeneration can occur,” Bhutani said. “It’s clear that a large pool of already existing cells in cartilage are changing their gene expression patterns. And by targeting these cells for regeneration, we may have an opportunity to have a bigger overall impact clinically.”
Blau added, “Phase 1 clinical trials of a 15-PGDH inhibitor for muscle weakness have shown that it is safe and active in healthy volunteers. Our hope is that a similar trial will be launched soon to test its effect in cartilage regeneration. We are very excited about this potential breakthrough. Imagine regrowing existing cartilage and avoiding joint replacement.”
Photo by Kampus Production: https://www.pexels.com/photo/man-in-blue-and-black-crew-neck-shirt-8638036/
A new study has shown how muscle stem cells protect themselves from loss in old age: as we age, muscles lose their ability to regenerate quickly, due to increased production of the protein NDRG1 in muscle stem cells. Prof Dr Julia von Maltzahn from the BTU Cottbus-Senftenberg, who has spent many years researching muscle regeneration during ageing as a group leader at the Leibniz Institute on Aging – Fritz Lipmann Institute (FLI), has published a commentary on this article, as these new findings will change the way we look at changes in stem cells during ageing.
Muscle stem cells are essential for repairing our skeletal muscles. In young people, they respond very quickly to injuries, dividing and helping to rapidly replace damaged muscle tissue. However, these cells change with age, and muscles regenerate much more slowly – this has been known for some time.
A study on “Cellular survivorship bias as a mechanistic driver of muscle stem cell aging” by Jengmin Kang et al. from Stanford University School of Medicine, USA, now published in the journal Science, reveals for the first time an important mechanism behind the changes in muscle stem cells during aging. In aging muscle stem cells in mice, the protein NDRG1 is produced in increased amounts, which slows down their activation after injuries but at the same time increases their survivability. This balance of delayed activity during regeneration and increased resistance explains a fundamental trade-off in the aging process of muscle regeneration – and provides a new cellular mechanism behind the observed loss of function of aging cells.
Prof Dr Julia von Maltzahn classifies the new findings by Kang et al. against the background of relevant work on changes in muscle stem cells associated with aging as follows.
“The study shows that muscle stem cells develop a kind of protective mechanism during the aging process that leads to the survival of a subpopulation of stem cells. It is therefore important to look at the aging process and not the final stage.”
Study finds genetic contribution to human lifespan is about 50% – more than double previous estimates
Photo by Matteo Vistocco on Unsplash
What determines how long we live – and to what extent is our lifespan shaped by our genes? Surprisingly, scientists believed for decades that the heritability of human lifespan was relatively low compared to other human traits, standing at just 20 to 25%; some recent large-scale studies even placed it below 10%. Now, a new study from the Weizmann Institute of Science, published in Science, presents an entirely different picture. According to the findings, genetics accounts for about 50% of variation in human lifespan – twice as much, or more, than previously thought.
The study was led by Ben Shenhar from the lab of Prof Uri Alon of Weizmann’s Molecular Cell Biology Department.
“For many years, lifespan was attributed mainly to non-genetic factors, fuelling scepticism about genetic determinants of longevity”
Using mathematical models and analyses of three large twin databases from Sweden and Denmark – including, for the first time in this context, a dataset of twins who were raised apart – the researchers showed that earlier heritability estimates were masked by high levels of extrinsic mortality, such as deaths caused by accidents, infections and environmental hazards. Filtering out such extrinsic factors was impossible in historic datasets because they provided no information about the cause of death. To compensate for this limitation, the researchers developed an innovative framework that included mathematical simulation of virtual twins to separate deaths due to biological ageing from those caused by extrinsic factors. The new results are consistent with the heritability of other complex human traits and with findings from animal models.
Science Numbers
Up to age 80, the risk of dying from dementia shows a heritability of about 70% – far higher than that of cancer or heart disease.
The results have far-reaching implications for ageing research and public health. “For many years, human lifespan was thought to be shaped almost entirely by non-genetic factors, which led to considerable scepticism about the role of genetics in ageing and about the feasibility of identifying genetic determinants of longevity,” says Shenhar. “By contrast, if heritability is high, as we have shown, this creates an incentive to search for gene variants that extend lifespan, in order to understand the biology of ageing and, potentially, to address it therapeutically.”
Super agers were 68% less likely to harbour the gene nobody wants, APOE-ε4, compared to individuals with AD dementia in the same 80+ age group.
Photo by Ravi Patel on Unsplash
A comparatively large study reported Jan. 16 in Alzheimer’s & Dementia, The Journal of the Alzheimer’s Association, led by researchers at Vanderbilt Health, measures the frequency ofAPOE-ε4 and APOE-ε2 in so-called super agers — people ages 80 or older whose cognitive function is comparable to people 20 or 30 years younger.
The gene variant posing the greatest genetic risk of late-onset Alzheimer’s disease (AD) is called APOE-ε4. A different variant of the same gene, APOE-ε2, is thought to confer protection against AD.
Super agers were 68% less likely to harbour the gene nobody wants, APOE-ε4, compared to individuals with AD dementia in the same 80+ age group.
Most notably, super agers were 19% less likely to harbour APOE-ε4 than were cognitively normal participants in the same age group.
“This was our most striking finding – although all adults who reach the age of 80 without receiving a diagnosis of clinical dementia exhibit exceptional aging, our study suggests that the super-ager phenotype can be used to identify a particularly exceptional group of oldest-old adults with a reduced genetic risk for Alzheimer’s disease,” said Leslie Gaynor, PhD, assistant professor of Medicine in the Division of Geriatric Medicine, who led the study with Alaina Durant, BS, statistical genetic analyst in the Vanderbilt Memory and Alzheimer’s Center.
Super agers were also found for the first time to have higher frequency of the variant you’d want, APOE-ε2: They were 28% more likely to carry APOE-ε2 than were cognitively normal controls ages 80+, and 103% more likely to carry the variant than were participants with AD dementia age 80 or older.
The observational study, which includes the largest sample of super agers to date, uses data from the Alzheimer’s Disease Sequencing Project Phenotype Harmonization Consortium, led by another member of the study team, Timothy Hohman, PhD, professor of Neurology. The study included 18,080 participants from eight national aging cohorts.
Super-ager status was defined in part as people ages 80+ whose memory performance was above the average scored among cognitively normal participants ages 50 to 64. The study included multiple race/ethnicity groups, including 1412 non-Hispanic white super agers, 211 non-Hispanic Black super agers, 8829 participants with AD dementia, and 7,628 cognitively normal controls. APOE-ε4 frequency worldwide is 13.7%; in the study it was 43.9%.
“With interest in super agers growing,” Gaynor said, “our findings notably encourage the view that the super-ager phenotype will prove useful in the continued search for mechanisms conferring resilience to AD.
“This is by far the largest study to date to identify differences in APOE-ε4 allele frequency based on super-ager status, and the first study to find a relationship between APOE-ε2 allele frequency and super-ager status. We would expect these findings to lend continued interest to questions of how these variants may influence development of clinical dementia due to Alzheimer’s disease, as well as to the super-ager phenotype more generally.”
Using data from the nationally representative US Health and Retirement Study, researchers examined how shingles vaccination affected several aspects of biological aging in more than 3800 study participants who were age 70 and older in 2016. Even when controlling for other sociodemographic and health variables, those who received the shingles vaccine showed slower overall biological aging on average in comparison to unvaccinated individuals.
Shingles, also called herpes zoster, is a painful, blistering skin rash caused by the reactivation of the chickenpox virus, or varicella zoster. Anyone who has had chickenpox is at risk for shingles; while shingles can occur at younger ages, risk is higher for those 50 and older and immunocompromised individuals. Vaccination, which has generally only been provided to older people, offers protection from shingles as well as a lower chance of postherpetic neuralgia, or long-term pain after a shingles infection.
While vaccines are designed to protect against acute infection, recent research has highlighted a possible connection between adult vaccines, including those for shingles and influenza, and lower risks of dementia and other neurodegenerative disorders, said Research Associate Professor of Gerontology Jung Ki Kim, the study’s first author.
“This study adds to emerging evidence that vaccines could play a role in promoting healthy aging by modulating biological systems beyond infection prevention,” she said.
Measuring the body, not the calendar
Unlike chronological aging, biological aging refers to how the body is changing over time, including how well organs and systems are working. Two people who are both 65 years old may look very different inside: one may have the biological profile of someone younger, while another may show signs of aging earlier.
In the new study, Kim and coauthor Eileen Crimmins, USC University Professor and AARP Professor of Gerontology, measured seven aspects of biological aging:
inflammation
innate immunity
adaptive immunity
cardiovascular haemodynamics
neurodegeneration
epigenetic aging (changes in how genes are turned “off” or “on”)
transcriptomic aging (changes in how genes are transcribed into RNA used to create proteins)
The team also used the measures collectively to record a composite biological aging score.
Surprising results beyond shingles prevention
On average, vaccinated individuals had significantly lower inflammation measurements, slower epigenetic and transcriptomic aging, and lower composite biological aging scores. The results provide more insight into the possible mechanisms underlying how immune system health interacts with the aging process.
Chronic, low-level inflammation is a well-known contributor to many age-related conditions, including heart disease, frailty, and cognitive decline. This phenomenon is known as “inflammaging,” Kim said.
“By helping to reduce this background inflammation — possibly by preventing reactivation of the virus that causes shingles, the vaccine may play a role in supporting healthier aging,” she said. “While the exact biological mechanisms remain to be understood, the potential for vaccination to reduce inflammation makes it a promising addition to broader strategies aimed at promoting resilience and slowing age-related decline.”
These potential benefits could also be persistent. When analysing how the time since vaccination affected results, Kim and Crimmins found that participants who received their vaccine four or more years prior to providing their blood sample still exhibited slower epigenetic, transcriptomic and overall biological aging on average versus unvaccinated participants.
“These findings indicate that shingles vaccination influences key domains linked to the aging process,” Crimmins said. “While further research is needed to replicate and extend these findings, especially using longitudinal and experimental designs, our study adds to a growing body of work suggesting that vaccines may play a role in healthy aging strategies beyond solely preventing acute illness.”
Spending too long sitting raises the risk of heart disease and diabetes in people over 60, warns a major global review. Published in the Journal of Physical Activity and Health, the review analysed data from 28 international studies involving 82 000 people aged 60 and older.
It flags strong links between sitting time and worsening markers for chronic disease including high blood sugar, cholesterol, waist size, and blood pressure. And that’s even for people who exercise regularly.
That means — whether watching TV, using a tablet or reading a book — the longer older people sit, the higher their risk of major health problems like heart disease, stroke, and type 2 diabetes.
“This is a link we can’t ignore,” said Dr Daniel Bailey, Reader in Sedentary Behaviour and Health at the Department of Life Sciences, Brunel University of London. “You can meet the weekly exercise target, but if you spend the rest of the day sitting, your health is still at risk.”
In the UK, where more than 12 million people are aged 65 or older, older adults can spend up to 80% of their waking hours sitting down and longer during winter or for people with mobility issues. That means millions may be unknowingly accumulating risks day after day — a concern for families, carers, and health professionals.
One of the most revealing findings was that the harmful effect of sitting for long periods showed up even in otherwise healthy older adults, not just those already diagnosed with illness. Waist measurement, a major predictor of health risk, had the strongest, most consistent link with sitting time.
“We’re seeing these impacts in people who don’t yet feel unwell,” said Dr Bailey. “That means we have a chance to intervene early and protect health before problems start.”
Importantly, the study found limited protective effect from exercise alone. After accounting for how active people were, the damage from long hours of sitting remains.
“The evidence is clear. We urgently need strategies that don’t just encourage exercise, but also help people sit less throughout the day,” said Dr Bailey. “Simple changes make a difference —standing during phone calls, replacing some TV time with gardening or a stroll, or light chores around the house.”
The study by Brunel University of London, the University of Lincoln, Federation University in Australia, and the University of Bedfordshire is the most comprehensive analysis to date linking sedentary behaviour to cardiometabolic risk in later life. As the NHS contends with rising rates of diabetes and heart disease, it spells out to policymakers that keeping moving throughout the day is as vital as structured exercise.
Dr Bailey stressed the shared role of public services, community groups and healthcare professionals to help older people avoid sitting for long stretches: “From GP advice to local councils and charities, there’s a role for everyone in changing the message.”
Empowering Dignified Elder Care Through Compliant, Compassionate Staffing Solutions
Photo by Matthias Zomer on Pexels
For nearly seven decades, The Association for The Aged (Tafta) has been a cornerstone of care for senior persons in Durban and surrounding communities. Its services include assisted living, frail care, home-based care, meal delivery, and essential social work and advocacy programmes, all designed to support the dignity and well-being of older persons.
Delivering this level of care consistently requires the right professional healthcare staff and strong administrative support across Tafta’s multiple facilities.
The challenge: ensuring compliance and consistency Recruiting and managing trained Caregivers across several care units can be complex, particularly when strict compliance and accreditation standards must be met. Tafta needed a partner who could supply qualified staff while supporting operational efficiency and upholding care standards. Allmed, a specialist medical personnel solutions provider, with proven experience in healthcare staffing and administration, emerged as the ideal solution.
“At the time we were reviewing our contracts, we considered Allmed as one of the service providers to tender,” explains Yoshina Kistensamy, Divisional Manager: Operations of Tafta.
The requirements were clear: the partner needed to ensure all staff were fully compliant and accredited, while also providing responsive after-contract support. Financial flexibility was equally critical, enabling staffing to scale up or down according to operational realities without penalty.
Allmed provides layered support, with trained professionals backed by clinical facilitators, ensuring both quality care and peace of mind for residents’ families. This support is delivered across three key areas:
Strategic staffing: Ensures every facility has adequate, skilled personnel and optimises workforce allocation to meet varying needs.
Compliance oversight: Monitors adherence to healthcare standards, reducing risk and ensuring safe, consistent care practices.
Hands-on engagement: Provides practical support to staff and enhances day-to-day operations.
By combining these three areas, Allmed enables Tafta to operate efficiently while maintaining a strong focus on the quality and dignity of resident care.
The impact: lifting the burden, prioritising care The partnership has given Tafta the space to focus on its core mission: providing compassionate care. By outsourcing much of its care staff, Tafta has transferred complex HR responsibilities, including training coordination, on-site supervision, and disciplinary processes, directly to Allmed.
Allmed provides layered support, with trained professionals backed by clinical facilitators, ensuring both quality care and peace of mind for residents’ families. This support is delivered across three key areas:
Strategic staffing: Ensures every facility has adequate, skilled personnel and optimises workforce allocation to meet varying needs.
Compliance oversight: Monitors adherence to healthcare standards, reducing risk and ensuring safe, consistent care practices.
Hands-on engagement: Provides practical support to staff and enhances day-to-day operations.
By combining these three areas, Allmed enables Tafta to operate efficiently while maintaining a strong focus on the quality and dignity of resident care.
The impact: lifting the burden, prioritising care The partnership has given Tafta the space to focus on its core mission: providing compassionate care. By outsourcing much of its care staff, Tafta has transferred complex HR responsibilities, including training coordination, on-site supervision, and disciplinary processes, directly to Allmed.
“For us, the primary benefit lies in ensuring that our care staff remain fully compliant with all required accreditations and registrations, which supports our commitment to delivering quality care through trained professionals,” says Kistensamy. “In addition, Allmed manages the HR processes, supplementary training, and ongoing supervision for this team, allowing us to focus on expanding and strengthening care and support services for our residents and the broader eThekwini community.”
Allmed’s support goes beyond typical service agreements. They work alongside Tafta’s management and care teams. “Whether it’s a quick phone call, a WhatsApp message, or an on-site visit, Allmed is always available,” Kistensamy adds. “Knowing they are just a message away provides enormous peace of mind.”
Forging a partnership that goes above and beyond Tafta values the partnership for more than staffing consistency. At the organisation’s annual Sports Day for older persons, Allmed has donated essential items, provided an on-site nurse, and actively participated alongside staff and residents. “It’s not just about supplying caregivers – Allmed consistently shows up and supports our programmes,” says Kistensamy.
Allmed also contributes to Tafta’s fundraising and public-relations events, including the International Day of Care and Support, golf days, resident Christmas lunches, and donor gala dinners. Their willingness to engage with staff, residents, and fellow care partners reinforces Tafta’s values and demonstrates that effective healthcare partnerships are built on the seamless alignment of the organisation, its beneficiaries, and its supporters.
Flexible solutions for non-profit needs Agility has been a cornerstone of the Allmed–Tafta partnership. When budget pressures arose, Allmed offered alternative staffing rates without compromising service quality.
“They understand our sector and our challenges, and they work with us to make sure our residents are always cared for,” says Kistensamy. Three elements define the success of this collaboration:
Exceptional customer service: proactive support and responsiveness beyond contractual obligations.
Flexible staffing solutions: ability to scale services up or down based on resident needs and operational realities.
Through this partnership, Tafta can prioritise its core mission: ensuring every resident receives compassionate, dignified care. With Allmed providing expert staffing and compliance support, the organisation can operate smoothly while maintaining high-quality care standards.