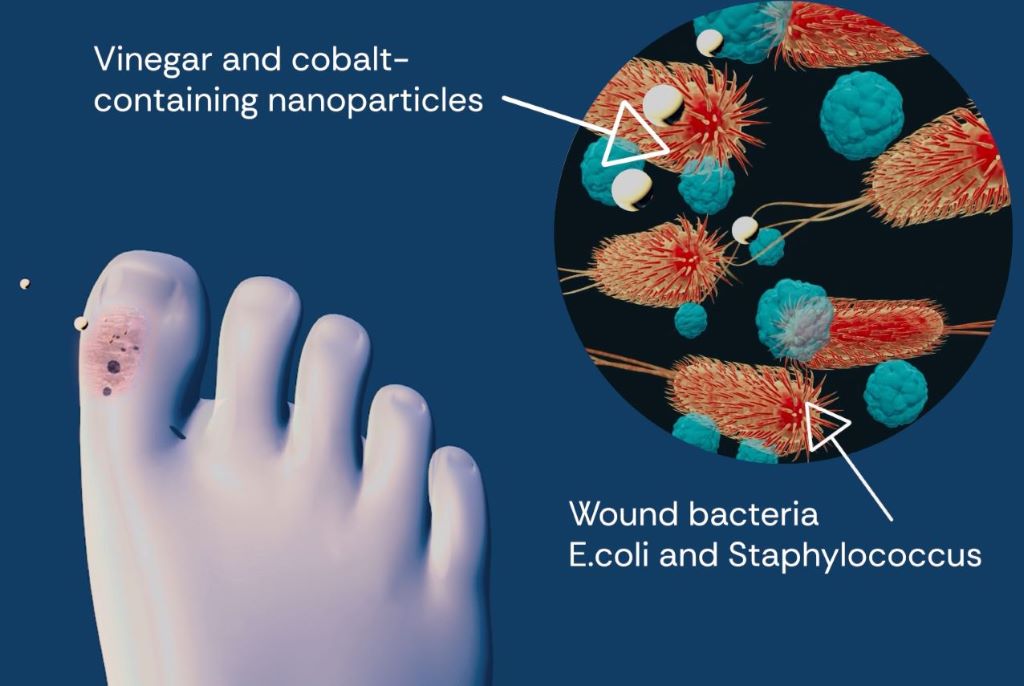
A new study suggests adding microscopic particles to vinegar can make them more effective against dangerous bacterial infections, with hopes the combination could help combat antibiotic resistance.
The research, led by researchers at QIMR Berghofer, Flinders University and the University of Bergen in Norway, has resulted in the ability to boost the natural bacterial killing qualities of vinegar by adding antimicrobial nanoparticles made from carbon and cobalt.
Wounds that do not heal are often caused by bacterial infections and are particularly dangerous for the elderly and people with diabetes, cancer and other conditions.
Acetic acid (more commonly known as vinegar) has been used for centuries as a disinfectant, but it is only effective against a small number of bacteria, and it does not kill the most dangerous types.
The findings have been published in the international journal ACS Nano.
Flinders University and QIMR Berghofer molecular biologists Dr Adam Truskewycz and Professor Nils Halberg found these particles could kill several dangerous bacterial species, and their activity was enhanced when added to a weak vinegar solution.
As part of the study, Dr Truskewycz and Professor Halberg added cobalt-containing carbon quantum dot nanoparticles to weak acetic acid (vinegar) to create a potent antimicrobial treatment.
They used this mixture against several pathogenic species, including the drug-resistant Staphylococcus aureus, Escherichia coli (E. coli) and Enterococcus faecalis.
Dr Truskewycz says the acidic environment from the vinegar made bacterial cells swell and take up the nanoparticle treatment.
“Once exposed, the nanoparticles appear to attack dangerous bacteria from both inside the bacterial cell and also on its surface, causing them to burst. Importantly, this approach is non-toxic to human cells and was shown to remove bacterial infections from mice wounds without affecting healing,” he says.
The anti-bacterial boost in vinegar found in the study could potentially be an important contribution towards the ongoing battle against the rising antimicrobial resistance levels worldwide, with an estimated 4.5 million deaths associated with a direct infectious disease.
Professor Halberg adds this study shows how nanoparticles could be used to increase the effectiveness of traditional bacterial treatments.
“Combination treatments such as the ones highlighted in this study may help to curb antimicrobial resistance. Given this issue can kill up to 5 million people each year, it’s vital we look to find new ways of killing pathogens like viruses, bacteria and fungi or parasites,” he says.
The article, ‘Cobalt-Doped Carbon Quantum Dots Work Synergistically with Weak Acetic Acid to Eliminate Antimicrobial-Resistant Bacterial Infections’ (2025) by Adam Truskewycz, Benedict Choi, Line Pedersen, Jianhua Han, Melanie MacGregor and Nils Halberg has been published in ACS Nano.
A microneedle patch captures cancer biomarkers in the top-most layer of skin to detect melanoma in animal tissue samples
The newly designed ExoPatch being removed from a sample of mouse skin successfully distinguished melanoma from healthy skin in mice. A gel coating the microneedles picks up cancer indicators from the top-most layer of the skin. Dissolving the gel releases exosomes into a solution, which is then used on a two-lined test strip, similar to an at-home COVID-19 test. Image credit: Jeremy Little, Michigan Engineering.
Melanoma testing could one day be done at home with a skin patch and test strip with two lines, similar to COVID-19 home tests, according to University of Michigan researchers. Developed with funding from the National Institutes of Health, the new silicone patch with star-shaped microneedles, called the ExoPatch, distinguished melanoma from healthy skin in mice.
The patch and test move toward rapid at-home melanoma testing, helping patients catch the most aggressive form of skin cancer early without a biopsy or blood draw.
“The star-shaped needles make puncture easier and less painful, but they are so small that they only go through the top-most layer of the skin, the epidermis, and do not draw blood,” said Sunitha Nagrath, the Dwight F. Benton Professor of Chemical Engineering at U-M and co-corresponding author of the study published in Biosensors and Bioelectronics.
The ExoPatch microneedles, at just 0.6mm long with a width of less than 100 nm (0.0001 mm) at the tip, are coated with a gel that picks up exosomes, tiny packages released by cells, from the interstitial fluid that fills the spaces between cells in the epidermis.
Once thought to be trash ejected from cells for cleanup, exosomes actually contain DNA and RNA fragments that cells use to communicate with each other. Cancer cell exosomes can help tumours spread by preparing tissues to accept tumour cells before arrival, and detecting them can catch cancer earlier than past methods.
The gel that coats the ExoPatch contains a protein called Annexin V that attracts and sticks exosomes to the microneedles’ surface. Once removed from the skin, placing the patch in an acid dissolves the gel, which releases the exosomes into a solution. After dipping a test strip into the solution, two lines form if the sample contains melanoma exosomes, and one line forms for a negative test – the same way an at-home COVID-19 test strip works.
“A fair-skinned person with moles must go to the doctor about every six months to send off a biopsy to see if they’re malignant or benign. With this test, they could instead test at home, get the results right away and follow up with a dermatologist for a positive result,” Nagrath said.
As a first step in the proof-of-concept study, the researchers tested the ExoPatch on a tissue sample of pig skin, which closely resembles human skin in thickness and composition. Using a microscope, they found the microneedles penetrated about 350 to 600nm into the skin. For scale, the epidermis on the human forearm is about 18 300nm thick.
To test whether the ExoPatch could capture melanoma exosomes from skin tissue, the research team tested tissue samples of mouse skin, half from healthy mice and half from mice injected with a fragment of a human melanoma tumour. After a 15-minute application, the ExoPatch was placed under a powerful microscope.
“When looking at microscopy images, I was happy to see how nicely the exosomes adhered to the microneedles and were within the 30 to 150 nanometre size range we expect,” said Scott Smith, U-M doctoral student of chemical engineering and co-lead author of the study.
After confirming the exosomes stuck to the ExoPatch, the researchers dissolved the gel and ran the sample through the test strips. The test successfully distinguished between melanoma and healthy tissues with a 3.5-fold darker line in melanoma samples.
The ExoPatch isolated 11.5 times more exosomal protein from melanoma tissue samples compared to healthy tissue, showing it can specifically target cancerous exosomes.
A pilot study in humans followed by a series of clinical trials will be the next steps to move the technology toward use. Beyond melanoma, the ExoPatch gel coating could be modified to detect exosomes released by other cancers with a solid tumour, including lung, breast, colon, prostate and brain cancer.
“This is the first patch designed to capture disease-specific exosomes from fluid under the skin. The potential applications are huge,” said Nagrath.
Flavoured marijuana vaping is now the most common form of use among American teenagers who vape cannabis, according to new findings from the University of Michigan.
The research, published in the Journal for Adolescent Health, found particularly sharp increases among younger teens between 2021 and 2024. Among eighth graders who vaped marijuana, the percentage using flavoured solutions jumped from 47% in 2021 to 63% in 2024. The trend was similar for older students, with use climbing from 41% to 53% for 10th graders and from 36% to 50% for 12th graders.
“The findings suggest that these products are gaining traction among youth; in fact, since the pandemic onset in 2020 youth appear to be turning toward these products while reducing their use of all other drugs,” said Richard Miech, principal investigator of the Monitoring the Future study at U-M’s Institute for Social Research.
The overall percentage of marijuana users who chose to vape the drug also grew over the study period. Among eighth graders who had used marijuana in the past 12 months, the percentage who vaped it increased from 48% to 57%. In 10th grade, the number went from 60% to 66%, and among 12th graders, it rose from 58% to 67%.
“Flavoured vaping solutions offer a discreet mode of cannabis use, with flavours apparently enhancing their appeal,” Miech said. “The study results suggest that a growing proportion of youth find the newly available flavours – especially fruit flavours – more attractive than the standard cannabis taste.
“Vaping does not produce the distinctive odor that comes from smoking cannabis, and vaping devices can be quickly concealed if an authority figure appears unexpectedly.”
More addictive?
This increase in those who vaped highlights growing public health concerns about changing patterns of substance use among teens.
“As for health consequences for cannabis use, one of the most potentially serious is addiction,” Miech said. “Should cannabis use become more popular among youth in future years, then a greater number will end up with an addiction that can impair their social and academic life. Many people may not realize that more adolescents meet the criteria for cannabis use disorder than for alcohol use disorder, with 5% affected by cannabis compared to 3% for alcohol.”
These results point to flavored marijuana vaping solutions as a critical area for future research and policy development. The study’s authors suggest that these findings underscore the need for targeted policies, interventions and educational campaigns to address and mitigate this escalating concern among young people.
“Our survey includes questions on both cannabis’s perceived risk and its social acceptability,” Miech said. “Interestingly, perceived risk among adolescents actually increased over the study period from 2021-24, and social acceptability has gone down. That being said, our questions so far have been about cannabis use in general, and not flavoured cannabis solutions, which students may view differently.”
Would restricting flavoured vapes work?
Recent trends in adolescent cannabis vaping raise concerns about the best way to protect youth. Restricting flavors may seem like an easy solution, but it is by no means a guaranteed success, researchers said.
Teens who seek flavored cannabis products could easily shift to unflavored options or return to smoking cannabis in traditional forms. At the same time, adults in states with legal cannabis may resist limits on flavor choices, and industry lobbying could block such policies.
“An alternative approach to restricting supply of cannabis flavours is to restrict demand,” Miech said. “That is, to reduce teens’ interest and willingness to use cannabis, including flavoured vaping solutions. A demand reduction approach has been very effective for cigarettes.”
Evidence from previous studies on cigarette use supports this approach. In 1998, 35% of 12th graders had used cigarettes in the past month. By 2024, that number dropped to 3%. Cigarettes remained legal and available, but broad-based media campaigns, public education and tighter rules on marketing to youth drove the change.
As the complexities of global healthcare evolve, the need for collaborative, values-driven investment in health systems has never been more urgent. Rand Mutual Assurance’s (RMA) recent completion of the Welkom Sub-Acute Rehabilitation Hospital upgrade offers more than a modern facility; it stands as a bold statement of intent on how the private sector can participate responsibly as a vehicle of driving universal healthcare coverage that addresses the disparities in access to quality healthcare.
General health inequities in South Africa are well-documented and mirror the persistent income inequalities of an unequal society. Bridging these inequity gaps demands multilateral thinking that transcends siloed programme implementation and that sees rehabilitation as a core component of the healing journey. RMA’s approach exemplifies how a private occupational healthcare insurer can work hand-in-hand with regulators, multi-disciplinary clinical teams and local stakeholders, to construct a shared vision for rehabilitation and wellness.
Hospital upgrade
Established in 2016 to provide basic wound care for injured workers and assisted living for disabled ex-miners (RMA pensioners), the Welkom Sub-Acute Hospital has undergone a major upgrade. It now features:
• Specialist wound management and vocational rehabilitationunits
• Assisted living units for ex-workers injured and/or disabled in the line of duty
• A multidisciplinary clinical team of occupational therapists, physiotherapists, sessional medical officers and urologists• 24-hour nursing support and dedicated case management, and
• An in-house orthotics and prosthetics centre developed via a joint venture.
These enhancements speak to RMA’s core values of serving with care and compassion and its aspirations of being a pioneering social insurer. Patients benefit from seamless care journeys that prioritise functional recovery and long-term wellness. More broadly, the facility serves as a tangible blueprint for what future-focused healthcare investment can achieve in injury and disability management by integrating wound care, rehabilitation and custodial care with vocational reskilling infrastructure, all under one roof.
Inclusive innovation
Innovation, too, must be inclusive. RMA’s willingness to integrate independent joint-venture partners in key clinical areas, such as orthotics and prosthetics, demonstrates how ethical investment can fuel niche specialisations that were previously inaccessible in under-resourced regions. As private and public sectors increasingly intersect, providers who prioritise equitable collaboration will shape the standards for occupational health, post-acute care and sustainable rehabilitation pathways.
The Welkom upgrade also delivered tangible socioeconomic benefits. Construction created temporary jobs for local labourers, artisans and suppliers. As the hospital transitions to full operation, it will sustain roles in clinical services, administration, facilities management and auxiliary support – all drawing from the surrounding community.
Building equitable, resilient healthcare
Crucially, the project demonstrates that ethical healthcare investments need not be confined to metropolitan hubs. In a world where access to healthcare and especially rehabilitation services is driven primarily by affordability more than by need, RMA raises the banner of corporate citizenship by investing in the community where the health-insured population resides, and that mainstream healthcare providers might otherwise overlook, so as to promote health equity goals. By situating a cutting-edge sub-acute hospital in Welkom, Free State, RMA created a ripple effect, attracting specialised talent, strengthening referral networks and inspiring similar initiatives in other underserved areas. This industry influence signals a turning point where sub-acute care is no longer an afterthought but a strategic pillar of resilient health systems.
Looking ahead, RMA remains committed to scaling these principles, thus advocating for policy frameworks that foster public-private collaboration, driving research into cutting-edge rehabilitation modalities and championing community-centred care models. In doing so, it positions itself as a social insurer that is invested in shaping a more equitable, resilient future for South Africa and beyond.
Media enquiries: Gopolang Peme, Group Communications Manager, Rand Mutual Assurance
Author: Dr Tryphine Zulu, Head Healthcare, Rand Mutual Assurance
Most medical devices are used in healthcare settings but some like bandages, thermometers, condoms, and blood pressure monitors are used at home. Photo by Mockup Graphics on Unsplash
By Catherine Tomlinson
Unlike with medicines, and with a few exceptions, South Africa’s regulator does not assess whether diagnostic tests and other medical devices on the market are safe and work as they are supposed to. The regulator has however started down a road that should eventually lead to the regulation of all medical devices in the country.
From scalpels to surgical robots, finger-prick diagnostic tests to MRIs, thermometers to wearable AI-powered health monitoring devices, bandages to prosthetics: the range of products classified as medical devices is vast.
Some medical devices are used briefly and then disposed of after a single use, while others are designed to stay in our bodies for long periods of time, such as implants to prevent pregnancy and pacemakers to help the heart beat regularly.
While most medical devices are used in medical settings, some, like bandages, thermometers, condoms, and blood pressure monitoring devices, are used at home.
The World Health Organization estimates that there are more than two million different types of medical devices used around the world. Given the enormous diversity of medical devices, it can be tricky to see what links all these products together.
One answer, and essentially the one used in South African law, is that it is the intended use of the device. A medical device is thus simply any device that is intended to be used to prevent, diagnose, monitor, or treat a disease, injury, or other medical condition.
Because medical devices are sold for medical purposes, they require regulatory oversight to ensure that they are safe to use and work as intended. But in South Africa, this regulatory oversight is not yet fully in place, and you can’t always trust that devices do what they claim to do, or that tests are accurate.
‘Inaccurate readings’
On a recent webinar hosted by FIND, an international non-profit engaged in the development of diagnostics for low resource settings, the chairperson of NGO SA Diabetes Advocacy, Kirsten de Klerk, told participants that “a lot of people assume that if a medical device is available for purchase, it has been correctly tested and approved for use” but “unfortunately, that’s not the case”.
De Klerk added: “I have unfortunately had community members sharing stories of life-threatening situations because of inaccurate readings” from continuous glucose monitors (CGMs). These are medical devices used by people with diabetes to monitor their blood sugar level.
To address the challenge of poor-quality CGMs on the market, South African diabetes advocates and FIND launched a tool to assist people with diabetes and healthcare providers to identify and use monitors that have been properly assessed for safety and functioning.
But what role does the South African Health Products Regulatory Authority (SAHPRA) play in ensuring the safety and effectiveness of medical devices used in the country, and what steps is it taking to better protect the public?
A mandate to regulate
Though medical devices aren’t yet registered, SAHPRA does have a legal mandate to regulate medical devices. The relevant legal requirements were introduced in the 2015 Medicines and Related Substances Amendment Act 14. Before the 2015 Amendment Act came into force in 2017, only electromagnetic or radiation-emitting medical devices were regulated in South Africa.
The 2015 amendments provided for the establishment of SAHPRA to replace the Medicines Control Council as the country’s health products regulator and expanded SAHPRA’s regulatory scope to cover all medical devices.
SAHPRA’s first big move towards regulating the medical device industry was to introduce requirements for medical device companies to be licensed as medical device establishments. Medical device companies were informed that they would need a medical device establishment license to operate in the country in a government gazette notice issued in 2017. (Manufacturers of the lowest risk products – Class A medical devices that don’t have a measuring function and/or are not required to be sterile – are currently exempt from the licensing requirements.)
Today, over 2 500 companies hold active medical devices establishment licenses from SAHPRA. In their applications for these licenses, companies must list the medical devices that they will manufacture, import, or wholesale in South Africa and the establishment licenses that they are granted are specific to the class of products that they are manufacturing or handling.
Medical devices are classed in four groups from lowest to highest risk products, based on the risk posed by the product to patients and the broader public health. Bandages for example are classed as low risk, while heart valves are classed as high risk. Using a risk-based approach allows SAHPRA to harmonise how medical devices are regulated in South Africa with international norms and will allow the regulator to prioritise review of high-risk products as it phases in requirements for registration of medical devices used in the country.
In addition to listing the devices that they manufacture, distribute, or wholesale, companies seeking medical device establishment licenses from SAHPRA are also required to provide a declaration regarding the quality management systems that they have in place.
Critically, however, the devices themselves are not yet being assessed by SAHPRA.
Dr Dimakatso Mathibe, senior manager of SAHPRA’s medical device unit, told Spotlight that more than 200 000 different medical devices are used in South Africa. While over two thousand companies hold active medical device establishment licenses, she explained that a single company may be importing over a hundred products. She noted that as SAHPRA has increased the regulatory requirements for operating in South Africa, some medical device companies have voluntarily withdrawn from the market.
ISO 13485 certification
SAHPRA’s second big move, which is now being rolled out, is the introduction of requirements for medical device companies to gain ISO 13485 certification verifying that they meet international quality management standards.
Medical device companies operating in South Africa can receive certification that they meet ISO 13485 standards from an international or local conformity assessment body that has been accredited to provide this certification.
When SAHPRA first introduced medical device establishment licenses, it did not require companies to have ISO 13485 certification, as it was concerned that enforcing this too quickly could disrupt access to medical devices in the country. This was in part due to the lack of local conformity assessment bodies accredited by the South African National Accreditation System (SANAS) to grant this certification at the time.
John Ndalamo, accreditation manager for SANAS’ certification programme, told Spotlight that six local conformity assessment bodies have now been accredited to provide ISO 13485 certification.
SAHPRA now requires that companies renewing their five-year medical device establishment licenses provide either proof of ISO 13485 certification or evidence that the company has begun the process of seeking this certification.
What about regulation of the actual devices?
While important strides have been made by SAHPRA toward regulating the medical device industry, medical devices themselves still remain mostly unregulated in South Africa.
What this means is that, as pointed out by SA Diabetes Advocacy, medical devices may currently be marketed in the country without an independent regulator confirming that they are safe to use and perform as advertised.
The registration of the over 200 000 medical devices in use in the country is a mammoth job. Mathibe said that when SAHPRA introduces requirements for the registration of medical devices, it will do so in a phased and transitional manner. She explained that the call-up of medical devices for registration will likely be phased by product risk classes and conditions. Presumably, SAHPRA will start with the highest risk products and work down from there.
Assessing feasibility
SAHPRA is conducting a feasibility study of its intended approach to register medical devices. Companies holding medical device establishment licenses have been asked to voluntarily participate in the study.
In documentation published for the feasibility study, SAHPRA indicated it plans to include 32 medical devices used for HIV and TB in the study. These will cover in vitro diagnostic tests, condoms, and X-ray devices used for TB screening.
SAHPRA also aims for half of the products included in the study to be manufactured locally and the other half to be imported. In doing so, SAHPRA can use the study to test its approach for registering products that are evaluated locally, as well as products assessed in other countries with which it has a regulatory reliance mechanism in place (meaning it can rely on regulatory evaluations performed in these countries).
How will safety and performance be assessed in the feasibility study?
Mathibe said that SAHPRA will not directly assess the safety and performance of medical devices in the feasibility study. Instead, this will be done by accredited conformity assessment bodies, which is the same approach used by regulators in Europe. The assessment made by the conformity assessment bodies will then be used by SAHPRA in determining whether a product should be approved for use in the country.
For medical devices already registered in jurisdictions with which SAHPRA has a reliance mechanism in place, like the European Union, Australia, and Japan, companies can submit evidence of such conformity assessments and marketing approval. SAHPRA can then use this information to help make its own registration decisions.
Devices that are not approved by a regulatory authority recognised by SAHPRA, must undergo a safety and performance assessment by a locally accredited conformity assessment body.
Mathibile said insights from the study will be shared with stakeholders next year, and the lessons will help inform how SAHPRA introduces medical device registration in South Africa.
Emergency authorisation of COVID-19 and Mpox medical devices
While SAHPRA has not yet registered medical devices, it introduced rules in 2020 for emergency authorisation listings for certain medical devices used for COVID-19 in South Africa, and it announced in 2024 that diagnostic tests for Mpox required approval from SAHPRA before they could be used in the country.
SAHPRA has thus “listed” multiple COVID-19 tests and two Mpox diagnostic tests as approved for use in South Africa. Khanyisile Nkuku of SAHPRA’s medical devices unit told Spotlight that the diagnostic products for COVID-19 and Mpox received interim Section 21 authorisation.
Section 21 authorisation allows for the use of unregistered products under certain conditions, including public health emergencies. This mechanism has been used by SAHPRA both to respond to the public health needs posed by COVID-19 and Mpox and to prevent the use of substandard products, which was a challenge faced in the early days of COVID-19.
Nkuku added while South Africa has had a relatively low number of Mpox cases, South Africa is a leading supplier of in vitro diagnostics to the rest of the continent, including countries facing large Mpox crises, and so SAHPRA shares the responsibility of ensuring that Mpox diagnostics used on the continent work properly and is working with the African Medicines Regulatory Harmonisation programme to review Mpox diagnostics.
A new project led by Oxford University aims to develop a novel breathing test that could detect asthma and COPD earlier, more accurately, and closer to home – reducing pressure on the NHS and improving outcomes for patients.
This work is included in a portfolio of research funded by the Engineering and Physical Sciences Research Council (EPSRC), part of UK Research and Innovation, to make diagnostic testing more accessible by designing simple, affordable tools that can be used in everyday settings. The project, called ACCESS (A Community-based diagnostiC for early airwayS disease), focuses on airway diseases, and will receive £1.3 million over three years.
Chronic respiratory diseases such as asthma and chronic obstructive pulmonary disease (COPD) affect more than half a billion people worldwide and cause over four million deaths every year. In the UK, these conditions hit disadvantaged communities hardest, with people in areas of socioeconomic deprivation facing particular challenges in accessing hospital-based diagnostic care.
A volunteer undertaking a computed cardiopulmonography based breath test. (The volunteer is Dr Nick Smith, a member of the research team developing the CCP technology). Credit: Department of Chemistry, University of Oxford.
Currently, asthma and COPD diagnosis relies on a test called spirometry. This measures how much air a person can forcefully breathe out, but it is difficult for many patients to perform and often fails to detect disease in its earliest stages. By the time spirometry picks up abnormalities, damage to the lungs is usually irreversible, resulting in late diagnoses, missed chances for early treatment, and poorer outcomes.
The project is enabled by the strong ethos for collaborative and innovative research in this University and will be delivered by a multi-disciplinary team, working across university departments and the NHS.
To address these issues, Oxford researchers have developed a new test, known as computed cardiopulmonography (CCP), that could transform the way lung diseases are diagnosed. CCP is performed while a patient breathes normally for 12 minutes through a mouthpiece linked to a highly accurate gas analyser. Using cutting-edge laser technology and advanced mathematical modelling, the test captures a detailed picture of how evenly air flows through the lungs. This “fingerprint” of lung function changes early in the course of disease, making CCP a powerful tool for spotting subtle problems that spirometry can miss.
Early studies in people with asthma, COPD, and even in otherwise healthy smokers suggest CCP is a highly sensitive marker of small airways damage. But while the results are promising, the test currently takes too long and requires specialist gas supplies, restricting its use to hospitals and research labs.
The goal of the ACCESS project is to adapt CCP for community use, for instance in GP surgeries, pharmacies, and community diagnostic hubs. Specifically, the research team will work to reduce the time duration and volume of gas needed for each test, and speed up the data analysis so that results can be shared with the patient during the same appointment. Towards the end of the project, CCP will be trialled in a community diagnostic centre to gather feedback from patients and healthcare professionals.
The long-term goal is to support earlier diagnosis and treatment, helping reduce hospital visits and tackle health inequalities. By enabling earlier intervention and delivering care closer to home, CCP has the potential to improve outcomes for millions of people living with lung disease.
The country that performed the first successful heart transplant has very low organ donation rates. Now a student-run medical non-profit is hoping to make a difference. (Photo: Nasief Manie/Spotlight)
By Elri Voigt
Thousands of people in South Africa are waiting for a life-saving organ transplant, but our very low organ donation rates mean that many won’t get a transplant in time. Spotlight asks the experts why our donation rates are so low and what can be done about it.
Back in 2002, Rentia le Roux received a horrifying diagnosis that her kidneys were failing. “My kids still need me, they are still small, what are we going to do?” Le Roux recalls telling her doctor. After a long journey trying to manage her kidney failure, she would eventually get a kidney from her sister in 2011.
Le Roux, now the chairperson of the Western Cape Transplant Sports Association, is one of the lucky ones. She spoke to Spotlight ahead of a trip to Germany to take part in the 2025 World Transplant Games.
“There are so many people that are on the list waiting for an organ and the waiting period, it can take many years,” she says.
Incomplete data
While there isn’t a coordinated, centralised database of everyone in South Africa who needs a lifesaving organ transplant, various groups do collect data. This is according to Professor David Thomson, an abdominal transplant surgeon and a critical care sub-specialist. Thomson is also the head of the Transplant Centre of Excellence Project at Groote Schuur Hospital in Cape Town.
“Various entities do collect levels of data, but it’s not very centralised and coordinated, and it could be better…we do have the renal registry that’s trying to track the number of people on dialysis, that’s a good source of information,” Thomson says. The Renal registry is a not-for-profit database that collects and publishes data on dialysis and transplant patients in the country. The database itself is an initiative of the South African Nephrology Society, an NPO that aims to further the field of nephrology and improve patient care.
The society estimates that in 2022, just over 9000 people across the public and private healthcare system were receiving “kidney replacement therapy” – which were either medications to help kidney function, dialysis or a kidney transplant.
A report by the South African Transplant society, an NPO that seeks to advance tissue and organ donation and transplantation, estimated that in 2021, across South Africa’s private and public hospitals, 2 586 people were on a waitlist for a lifesaving organ. Of those, 2382 people were waiting for a kidney, 52 needed a liver, 108 needed a heart transplant, and 44 were waiting for a lung.
But in the same year, the report recorded only 229 transplants done across the country.
South Africa does not have a good organ donation culture, says Professor Mignon McCulloch, the head of paediatric nephrology and solid organ transplant at the Red Cross War Memorial Children’s Hospital. In fact, according to McCulloch, and other experts we spoke to, South Africa has some of the lowest transplantation rates in the world.
While we couldn’t find any straightforward ranking system of organ donation rates, reports by the Global Observatory on Donation and Transplantation (GODT) do provide some insight into how some countries compare to one other. In 2017, according to data from the GODT cited in this 2020 study published in the South African Medical Journal, South Africa had 91 deceased donors, which is a rate of 1.6 per million. By contrast, Spain, which is regarded as having one of the highest rates of organ donation in the world, had 2183 deceased donors, a rate of 47.05 per million.
How it works
Organ donation is broadly classified into living donation and deceased donation.
There are two scenarios where someone can become an organ donor. The first, Thomson explains, is when a healthy person donates an organ without which they can live a normal life, like one of their kidneys. The second is when someone has been declared brain dead and is on a mechanical ventilator or when someone has experienced circulatory death -meaning their heart has stopped beating and “futile non-beneficial treatments have been stopped”. The latter is less common in South Africa.
For deceased donation from a brain-dead patient to take place, the potential donor needs to be in an ICU facility on a mechanical ventilator and referred by their clinical team to a transplant coordinator, says Thomson. If that person is eligible, then the transplant team has to get permission from the next of kin who ultimately have the final say even if the potential donor is registered as an organ donor.
“Organ donation can only happen if someone is on a mechanical ventilator in the end-of-life care pathway, so that is always a complicated and emotional discussion,” he says. “Tissue donations such as corneas, bones, skin, that can happen at the mortuary afterwards and there’s a slightly longer period for when these can be successfully recovered but all donation still requires you to have conversations with and get permission from grieving families.”
Juggling resources
McCulloch describes organ donation as being a bit like “a silent Cinderella”, until someone needs a lifesaving transplant, “and then people suddenly start asking questions about why, why don’t we have more transplantation?”
One reason for this is the allocation of resources and competing priorities within the healthcare system.
Thomson says that organ transplants are a “health intensive resource”, and it’s important to acknowledge that it exists in the context of an already overburdened healthcare system. There is a Deputy Director of dialysis and transplantation within the National Department of Health, Thomson explains, but there isn’t an “overarching central coordinating authority supporting deceased donation”. Instead, he says it is driven by hospital groups and within the provincial healthcare departments by healthcare workers
Adding to this, McCulloch says that doctors are always having to “juggle resources” and if there is only one bed available in an ICU, weighing up whether to give it to someone who will potentially become an organ donor or someone with pneumonia and will likely have a good outcome, is difficult.
Another challenge is the limited number of surgeons, physicians, and hospitals with the skill and equipment to perform an organ transplant. This strategy roadmap document by the South African Transplant Society list 21 transplants centres across the whole country – 14 of them offer kidney transplants, six offer heart transplants, four offer lung transplants, four offer liver transplants, and only one offers pancreas transplants.
Graphic of transplant centres in South Africa. (Source: Organ and Tissue Donation in South Africa – Creating a National Strategy Roadmap)
One can save seven
Earlier this year, an unused room in Tygerberg Hospital got a face-lift and a new purpose from a student-run medical non-profit. The initiative called Save7 was kickstarted by a conversation on kidney donation on Stellenbosch University’s Medical Campus. Its initial goal was to raise awareness, particularly among students, that one donor can save up to seven lives. And if tissue like corneas, heart valves, bone and skin are donated, one person can improve the lives of around 50 people.
Jonty Wright, who cofounded Save7, tells Spotlight that the organisation’s founding group of four has now grown to over 200 across multiple universities countrywide. Among others, the group created a Lifepod to solve a transplant-related problem at Tygerberg Hospital. Doctors and staff involved in transplantation at the hospital were citing competing resources as the reason behind low referral rates of potential organ donors by healthcare providers.
The solution posed by Save7, professors on the campus and some of the doctors involved with transplantation was to create a designated bed space for patients who are brain dead and are potential organ donors. The hope was that referrals for potential organ donations would be increased.
The room, Wright says, was an old minor operating theatre and storeroom that belonged to the orthopaedic surgery department and was situated in an ideal spot – in a corridor between the emergency medicine and trauma admissions.
Three of the Save7 co-founders, from left to right Jonty Wright, Suhayl Khalfey and Sachen Naidu. (Photo: Nasief Manie/Spotlight)
About three months ago, after fundraising efforts and backing by the Health Foundation and other partners, the Lifepod opened. The room currently holds a hospital bed, a ventilator on lease from the surgical department, vitals monitor, cardiac monitor, infusion pumps, emergency trolley, fridge, and crash cart. All the things needed to keep someone who is brain dead’s body comfortable and allow the doctors to counsel their loved ones about potentially donating their organs.
So far, according to Wright, referrals of potential candidates for organ donation at Tygerberg have gone up by 500%, but at the time of the interview none of the next of kin have consented to donating their loved one’s organs. (Data on this has not yet been published).
This ties onto another layer of complexity around organ donation, the reasons why next of kin don’t always give permission.
Need for better education
Samantha Nichols, the executive director of operations for the Organ Donor Foundation, an NGO advocating for organ donations, tells Spotlight that the problem isn’t so much a lack of awareness of organ donation, as a lack of good education around it. She says this affects everyone, including healthcare workers.
Nichols says that “it’s almost like the stars have to align” for a deceased donor to donate their organs, because of how many steps and doctors are involved in the process.
“[W]hen a person is sent to an ICU or trauma unit, the team of doctors that work on that person to save their life is a totally different team to the transplant team,” she says. A transplant team is only ever called in if a potential donor has been declared brain dead by two different doctors who aren’t part of or affiliated with a transplant team.
“[O]nly then can they start the process of talking to the family, and then they still need to get consent from the family before the organs are removed,” she says.
The Opt-in versus Opt-out debate
When it comes to consent for organ donation, South Africa has what is referred to as an opt-in system. An opt-in system means that someone must provide explicit consent of their desire to donate an organ. While an opt-out system means all adults are automatically considered organ donors after death, unless they explicitly withdraw consent beforehand.
There has been some debate about whether switching to opt-out systems would improve organ donation rates. One recent study, in which researchers analysed deceased donor rates in five countries that had switched from an opt-in to an opt-out system, did not find an increase in organ donation rates.
“Unless flanked by investments in healthcare, public awareness campaigns, and efforts to address the concerns of the deceased’s relatives, a shift to an opt-out default is unlikely to increase organ donations,” the researchers concluded.
A 2024 editorial in the Lancet medical journal made a similar point, saying “a simplistic switch to the ‘opt-out’ model is alone not sufficient to boost donation”. Instead, it lists the three components that makes Spain’s transplant programme so successful. “A solid legislative framework, strong clinical leadership, and a highly organised logistics network overseen by the National Transplant Organization.” An opt-out system is also unlikely to work well in South Africa from a legislative perspective, since it might be seen by some to impinge upon an “individual’s rights to personal autonomy and bodily and psychological integrity”, as argued in this article in the Conversation.
The experts Spotlight spoke to instead point to several other changes that could be made to improve donation rates.
‘Everyone can do a bit better’
The responsibility around improving organ transplantation rests on us as society and as a coordinated healthcare system, according to Thomson.
“[E]veryone can do a bit better…and I don’t think you want to make it one person’s responsibility for the performance. It’s actually a collective and how we work together,” Thomson says. “…a lot of things like supporting donation actually links into good palliative care services, and that should be something we’re offering to everyone.”
Thomson advocates for upskilling healthcare workers to be able to better counsel families during end-of-life care, not necessarily just around organ donation but around “engaging humanely with “families and end of life and navigating that complexity with them as the healthcare team”.
He recommends making counselling of grieving families and palliative care discussion a hospital system issue, instead of an individual responsibility by adding it to institutional operating standards. “And then you actually need to audit it, measure it, reflect on it and monitor the outcomes,” he says.
Suhayl Khalfey, a Save7 cofounder, says now that the Lifepod is ready to use, their focus is shifting to educate people about the importance of organ donation. As part of its education efforts, Khalfey says Save7 is putting together a database of different religious leaders to help counsel families uncertain about their faith’s stance on organ donation.
Nichols stresses that transplant teams will honour different religious beliefs and funeral practises and that a donor’s body will not appear disfigured in any way after they’ve donated their organs.
Start by having the conversation
Anyone can register as an organ donor with the Organ Donor Foundation, says Nichols. The process is free and will take less than a minute (see their website here). If a situation arises where you are brain dead and you are a candidate for organ donation your family will still need to give permission.
This is why it is so important to have the conversation with your loved ones about what your wishes are, says Khalfey.
Sachen Naidu, another cofounder of Save7, adds to this saying that often with the students they’ve spoken to, organ donation is viewed as something to think about in the distant future. He encourages young people to reconsider this mindset.
Even children can learn about organ donation.
The non-profit organisation Transplant Education for Living Legacies (TELL) recently launched an educational campaign in South Africa aimed at children in the 5 to 11 age group. The initiative, called the Orgamites Mighty Education Programme, is an international child health education programme originating from Canada. At its heart, the programme is a conversation starter, says Thomson who spoke on a TELL webinar.
“All we want is for people to be having educated conversations about it [organ donations],” he says. “Children need transplants too.”
For McCulloch, organ donation goes beyond impacting just the recipients. She uses the example of families who have lost a child in a tragic accident.
“You had a completely well child five minutes ago and then something terrible happened, and now you’ve got a child who’s died and you’re going to go home with a gap in your heart. Whereas at least when you donate [the] organs to another child, something good can come of out of a really hopeless, tragic situation,” she says.
Thomson adds to this saying: “And that’s a memory that lives with that family for a long time afterwards …not just that time point. That’s what they’re going to remember as part of that event, and it really does offer them a degree of solace for a tragedy.”
And the difference to those receiving organs can obviously be life changing. Receiving a kidney gave Le Roux the chance to see her children grow up. “So, every [milestone] when they wrote matric, when they got their degrees, everything. It’s like a step forward, something I can tick off, I’m still here. I’m able, I’m healthy,” she says.
Chest pain ranks as the second most common reason for emergency department (ED) visits, making it a key concern for patients and doctors. However, 80% of these cases are considered low-risk and not related to heart disease, and for these patients, anxiety and panic disorders are frequent diagnoses.
A new study led by the Indiana University School of Medicine and Regenstrief Institute shows that many patients who visit the emergency department (ED) with low-risk chest pain might benefit more from treatment for underlying psychological conditions than from extensive cardiac testing. The study appears in Academic Emergency Medicine.
Anxiety is not only common among low-risk chest pain patients, but is often accompanied by other treatable comorbidities, including depression, somatisation – the experience of psychological distress through physical symptoms – and post-traumatic stress disorder. By identifying and addressing these conditions, more targeted follow-up strategies can be developed to reduce repeat ED visits and unnecessary evaluations, improving patient outcomes and allowing health systems to focus resources where they matter most.
“Anxiety is a common fellow traveller with low-risk chest pain,” said corresponding author, IU School of Medicine and Regenstrief Research Scientist Kurt Kroenke, MD. “It is a frequent issue in the emergency department. While many patients worry about their heart, in many cases the chest pain is not cardiac, which raises the important question of whether there is something else that can be treated.”
The research, part of the Patient-Centered Treatment of Anxiety after Low-Risk Chest Pain in the Emergency Room (PACER) trial, showed that more than 42% of patients had severe anxiety, defined by a score of 15 or higher on the Generalized Anxiety Disorder (GAD-7) scale, a standardised tool developed by Dr Kroenke to assess the severity of anxiety symptoms. In addition, three-quarters of ED patients screened positive for panic disorder.
Evidence-based treatments for anxiety and comorbidities
Researchers identified two effective approaches to reduce anxiety in patients with low-risk chest pain: Cognitive Behavioural Therapy (CBT) and prescription medications. These treatments can be used on their own or combined to create a more comprehensive care plan, helping to better manage symptoms and prevent unnecessary return visits to the ED.
Psychotropic medications such as antidepressants and anti-anxiety medicines remain important tools for managing anxiety disorders. When used appropriately, these medications can lessen both the intensity and frequency of symptoms and are often most effective when paired with psychological therapy.
“There are classes of medicines that are effective for anxiety, particularly when it’s chronic,” said Dr Kroenke. “It’s no different than taking a medicine for high blood pressure – if someone has high blood pressure, we have medicines that lower it. Similarly, if someone has high anxiety, we have medicines that can effectively reduce it.”
The other effective approach is CBT, which helps individuals recognize and reframe thought patterns, manage panic symptoms and reduce fear associated with chest discomfort. Research shows that even brief courses of this behavioral therapy can significantly improve anxiety and quality of life. The PACER trial is comparing standard therapist-administered CBT to peer-supported internet-based CBT in patients with LRCP and anxiety.
“Emergency physicians often reassure patients that their chest pain isn’t caused by the heart, but reassurance alone is not enough. Connecting patients with proven therapies like cognitive-behavioural therapy and medications can change the trajectory of their care and improve long-term outcomes,” said IU School of Medicine and Regenstrief Researcher Paul Musey, MD, MS.
A new study from Karolinska Institutet, published in The BMJ, shows how a simple blood analysis can predict the risk of developing severe liver disease. The method may already start to be applied in primary care to enable the earlier detection of cirrhosis and cancer of the liver.
“These are diseases that are growing increasingly common and that have a poor prognosis if detected late,” says Rickard Strandberg, affiliated researcher at Karolinska Institutet’s Department of Medicine, Huddinge, who has developed the test with his departmental colleague Hannes Hagström. “Our method can predict the risk of severe liver disease within 10 years and is based on three simple routine blood tests.”
For the study, the researchers at Karolinska Institutet and their colleagues in Finland evaluated how well the method can estimate the risk of severe liver disease. The model, which is called CORE, was produced with advanced statistical methods and is based on five factors: age, sex and levels of three common liver enzymes (AST, ALT and GGT), which are commonly measured during regular health checks.
A web-based calculator
Their aim has been to produce a tool that is easy to use in primary care, where most patients first seek medical attention. A web-based calculator is already available for doctors and nurses at www.core-model.com.
“This is an important step towards being able to offer early screening for liver disease in primary care,” says principal investigator Hannes Hagström, adjunct professor at the Department of Medicine, Huddinge, and senior consultant at Karolinska University Hospital. “Drug treatment is now available, soon hopefully also in Sweden, for treating people at a high risk of developing liver diseases such as cirrhosis or liver cancer.”
The study is based on data from over 480 000 people in Stockholm who underwent health checks between 1985 and 1996. On following the participants for up to 30 years, the researchers could see that some 1.5% developed severe liver disease, such as liver cirrhosis and liver cancer, or required a liver transplant.
Highly accurate risk prediction
The CORE model proved highly accurate and was able to differentiate between people who either did or did not develop the disease in 88 per cent of cases, which is an improvement on the currently recommended FIB-4 method.
“Primary care hasn’t had the tools to detect the risk of severe liver disease in time,” says Professor Hagström. “FIB-4 is not suited for the general population and is less effective at predicting the future risk of severe liver disease.”
The model was also tested on two other population groups in Finland and the UK, where it again demonstrated a high accuracy in predicting this risk. The researchers make the point, however, that it needs to be further tested on groups at especially high risk, such as people with type 2 diabetes or obesity. They also recognise a need to integrate the model into medical records systems to facilitate its clinical use.
Depression and psychosis are more common in women after childbirth than before, but the risk of suicide attempts decreases. This is shown by two new studies from Karolinska Institutet. The results suggest that national guidelines for screening can help women get help earlier.
Mental ill health in connection with pregnancy and childbirth can have long-term consequences for women’s health. During this period, major biological and psychosocial changes occur that can increase vulnerability to depression, anxiety, and other psychiatric conditions. Despite previous research, knowledge has been limited, especially regarding how different psychiatric diagnoses develop before, during, and after pregnancy.
In a new study, researchers have used data from Swedish registers covering all women who gave birth in Sweden between 2003 and 2019 – a total of nearly 1.8 million pregnancies.
The study, published in the journal Molecular Psychiatry, shows that mental ill health has increased over time during this period, especially before pregnancy. During pregnancy itself, the number of new diagnoses decreases, but after childbirth, the risk increases again, especially for depression and psychosis.
“We can see that the risk of depression is about 20 percent higher during weeks 5 to 15 after childbirth, compared to the year before pregnancy. For psychosis, the risk is up to seven times higher during the first 20 weeks after childbirth,” says the study’s first author Emma Bränn, researcher, Institute of Environmental Medicine, Karolinska Institutet.
When Swedish national guidelines for screening pregnant women for depression were introduced in 2010, it opened up the possibility of detecting mental illness earlier. By comparing women who gave birth before and after 2010, the researchers saw that the peak of depression diagnoses occurred earlier after childbirth in women who gave birth after the guidelines were introduced.
“We don’t see that more people are being diagnosed, but screening could mean that women are identified earlier and don’t have to suffer as long before they can get the support and help they need,” says Emma Bränn.
Lower risk for other psychiatric diagnoses
The study also shows that the risk of other psychiatric diagnoses, such as anxiety, stress-related conditions, and substance abuse, is lower during pregnancy and after childbirth compared to before. The researchers believe that this may be due to biological changes, lifestyle changes, and increased contact with healthcare during pregnancy.
Another study from the same research group has investigated the risk of suicide in connection with pregnancy and childbirth. In the study, published in Nature Human Behaviour, researchers found that mothers were less likely to attempt suicide during and after pregnancy compared to fathers. This is the opposite of what researchers usually observe in the general population, where women tend to have higher rates of suicide attempts than men. For fathers, the risk decreased in the first ten weeks after childbirth, only to increase again.
“Our results suggest that both mothers and fathers are less likely to attempt suicide immediately after having a child, especially mothers,” says first author Yihui Yang, PhD student at the same department. She continues:
“Although suicide attempts during and after pregnancy are rare, they can have devastating consequences and are often preventable. It is therefore important that healthcare providers conduct regular check-ups during and after pregnancy to identify parents who are struggling and offer support to prevent suicide.”