
Research Supports Continued Use of Nasogastric Tube After Oesophageal Cancer Surgery
In the largest Nordic study to date concerning oesophageal cancer surgery, the researchers found clear evidence that decompression with a nasogastric tube is associated with less serious complications. Their results challenge a trend of declining use of the nasogastric tube after major surgical procedures. The study was led from Uppsala University and has now been published in Lancet Regional Health Europe.
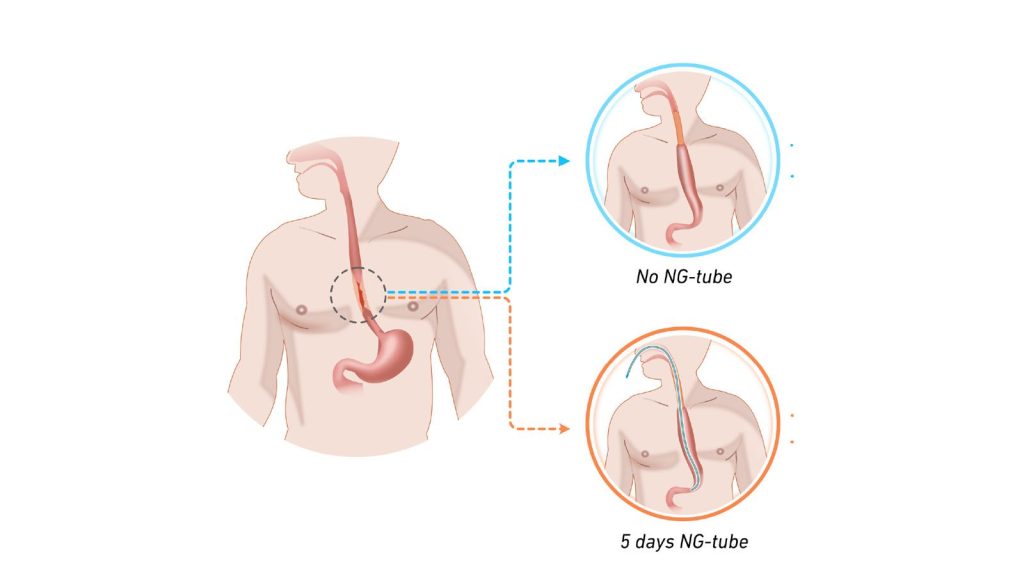
A number of small studies had previously suggested that it is safe to abandon the tradition of leaving in a decompressing – but for many patients unpleasant – nasogastric tube after surgery to remove oesophageal cancer (gullet cancer). The tube is plastic and runs from the nose down to the stomach, and its use in this particular context is to relieve and reduce pressure in this newly operated area. When the question was discussed in a Nordic research collaboration, it was concluded that these smaller studies lacked sufficient statistical power to justify a change in care. Subsequently, a randomised trial was carried out at 12 university hospitals across Sweden, Norway, Denmark and Finland, where patients were randomised to have or not have a decompressing nasogastric tube in their oesophagus following this type of surgery.
Patients without the tube experienced leakage
To the researchers’ surprise, it was not without risk to omit the tube after this surgery, as more patients without the tube experienced leakage in the anastomosis created during the operation. Leakage must be treated immediately, often with interventions under general anaesthesia, resulting in suffering for the patient and a longer length of hospital stay.
Although no differences in survival rates or other complications were found, this new knowledge may help to reduce suffering for patients in the future.
“Oesophageal cancer is an uncommon form of cancer, with only about 200 operations of this type being performed per year in Sweden. National and international cooperation is therefore absolutely necessary in order to conduct sufficiently large trials to answer the research questions we have. The fact that in just over two years, almost 450 patients have been recruited for the trial surpassed our expectations and represents a great success for this network,” says Jakob Hedberg, surgical oncologist, associate professor at Uppsala University and consultant surgeon at Uppsala University Hospital who is also principal investigator for the study.
“Strong interest has been shown at international conferences where our preliminary results have been presented, and the principle of building surgical care on solid evidence has allowed us to provide the best care to our patients. Another important effect of this successful collaboration is that we can build more clinical trials within the Nordic network which has now been consolidated. In fact, the next clinical trial is already under development,” says Jakob Hedberg.
Source: Uppsala University








