Cardiologists have long known that up to half of all heart attacks and strokes occur among apparently healthy individuals who do not smoke and do not have high blood pressure, high cholesterol, or diabetes, the “standard modifiable risk factors” which doctors often call “SMuRFs.” How to identify risk among the “SMuRF-Less” has been an elusive goal in preventive cardiology, particularly in women who are often under-diagnosed and under-treated.
A new study by Mass General Brigham researchers that leverages data from the Women’s Health Study has found hsCRP, a marker of inflammation, can help identify women who are at risk but are missed by current screening algorithms. Results are presented at a late-breaking clinical science session at the European Society of Cardiology Congress (ESC) and simultaneously published in The European Heart Journal.
“Women who suffer from heart attacks and strokes yet have no standard modifiable risk factors are not identified by the risk equations doctors use in daily practice,” said Paul Ridker, MD, MPH, a preventive cardiologist at Mass General Brigham’s Heart and Vascular Institute. “Yet our data clearly show that apparently healthy women who are inflamed are at substantial lifetime risk. We should be identifying these women in their 40s, at a time when they can initiate preventive care, not wait for the disease to establish itself in their 70s when it is often too late to make a real difference.”
As part of the federally funded study, researchers studied 12 530 initially healthy women with no standard modifiable risk factors who had the inflammatory biomarker hsCRP measured at study entry and who were then followed over 30 years. Despite the lack of traditional risks, women who were inflamed as defined by hsCRP levels > 3 mg/L had a 77% increased lifetime risk of coronary heart disease, a 39% increased lifetime risk of stroke, and a 52% increased lifetime risk of any major cardiovascular event.
Additionally, researchers released a new analysis of randomised trial data showing that “SMuRF-Less but Inflamed” patients can reduce their risk of heart attack and stroke by 38% using statin therapy.
“While those with inflammation should aggressively initiate lifestyle and behavioural preventive efforts, statin therapy could also play an important role in helping reduce risk among these individuals,” said Ridker.
Every 34 seconds, someone in the United States dies from heart disease. As nearly half of the country suffers from some form of cardiovascular disease (CVD), another 1 in 4 adults experience a mental health disorder in their lifetime, signalling an inevitable overlap.
Now, a new report from Emory University shows that certain mental health conditions escalate the risk of developing heart disease by 50–100% – and adverse outcomes from existing heart conditions by 60–170%.
The report, published in The Lancet Regional Health-Europe, summarises cardiovascular health disparities among those diagnosed with depression, anxiety, schizophrenia, bipolar and post-traumatic stress disorders (PTSD). The article is part of a series aiming to raise awareness around disparities in CVD health in four populations: women, the elderly, racial minorities and those with mental health conditions.
Emory University professor Viola Vaccarino, MD, PhD, led this metareview linking mental health conditions to CVD, along with co-authors Amit Shah, MD, and Douglas Bremner, MD, also Emory professors.
The report associated the following conditions and their corresponding risks of developing CVD:
Major depression, 72%
PTSD, 57%
Bipolar disorder, 61%
Panic disorder, 50%
Phobic anxiety, 70%
Schizophrenia, nearly 100%
The research also shows that these conditions are associated with a poorer prognosis, greater risk for readmission and higher mortality from existing heart conditions. For example, major depression more than doubles the mortality rate in those with existing CVD.
Additionally, the report emphasises a bidirectional relationship. “More than 40 percent of those with cardiovascular disease also have a mental health condition,” adds Vaccarino.
The physiology of stress
According to the report, a well-documented relationship exists among depression, schizophrenia, PTSD, and abnormal stress responses in the autonomic nervous system (ANS) and hypothalamic-pituitary adrenal axis (HPA).
The former allows the brain to manage involuntary responses, such as functions of the liver, heart, sweat glands, and eye muscles. ANS also manages both acceleration and deceleration of these functions, regulating inflammatory responses. Since most major organs have ANS nerve endings, this system impacts most bodily functions.
The hypothalamic-pituitary adrenal axis (HPA) also influences immune response and metabolism, which can impact cardiovascular function.
According to the report, dysregulation of these systems creates “adverse downstream effects that can affect cardiovascular risk chronically, including increased inflammation, metabolic abnormalities, high blood pressure, enhanced systemic vascular resistance and autonomic inflexibility.” Inflammation has also been implicated in both the development of heart disease and mental health conditions.
Social determinants and quality of care
The role of social determinants of health in CVD disparities is critical. Those with mental health conditions may face disruptions and barriers in the continuum of care, such as affordability and accessibility. Compromised health literacy or communication can also impede access to health screenings and treatment.
Clinicians could also be challenged to care for patients with certain mental conditions, which can be compounded by stigma and existing models that fragment mental and physical health care. Stigmas are also present in the field of clinical research, where having a mental health condition is often an exclusionary criterion in randomised trials.
Moreover, according to the report, current prediction models don’t account for mental health disorders when forecasting the risk of developing heart disease.
Next steps toward a healthier future
To address the disparities of CVD among people with mental health disorders, the authors recommend an integrated approach with interdisciplinary care encompassing behavioural, mental and cardiovascular health.
“The tight connection between cardiovascular and psychological health warrants changes in the health care system that are more amenable to patients with comorbidities,” says Vaccarino. “A clinical team would be ideal for the care of these patients – a team of specialists, social workers, and nursing staff who work in collaboration to provide multidisciplinary care and resources.”
The report concludes that closing the health disparity gap upholds the rights of those living with a mental health condition to achieve the highest level of health and fully participate in society.
Researchers at the University of Arizona College of Medicine – Tucson found evidence that a drug that improves the ability to walk in people with multiple sclerosis can also make bone fractures heal faster.
The findings help further the understanding of specific factors involved in the bone healing process, and potentially open avenues for new therapeutic approaches.
“Broken bones are typically slow to heal in many people, and they can impact lives for months and in different ways. People lose time at work and daily activities at home with family and friends are impacted,” said senior author John Elfar, MD, professor, surgeon and chair of the Department of Orthopaedic Surgery at the U of A College of Medicine – Tucson. “This drug has the potential to change that.”
Elfar partnered with Prem Kumar Govindappa, PhD, DVM, an assistant professor in the department, on the preclinical study that showed treatment with the drug 4-aminopyridine, or 4-AP, resulted in leg fractures healing faster and stronger than without the drug. The paper was published in The Journal of Bone and Joint Surgery.
“Mice with bone fractures healed quicker and were stronger after they healed after treatment with 4-AP,” said Elfar said, who is a member of the university’s BIO5 Institute. “We saw more bone mass and less intermediate cartilage, meaning there was accelerated bone healing.”
The drug is approved for use in chronic neurological conditions, where it helps with walking by improving how signals from the brain and spinal cord reach limbs.
The team also saw improvements in bone mass and the ability to bear weight after treatment with 4-AP. Collagen deposition and bone mineralization, both of which are necessary for bone healing, also received a boost. Collagen forms the structural foundation of bones. In bone mineralization, minerals like calcium and phosphate join the newly forming bone matrix, strengthening and hardening the bone.
“We found that every fine-tuned measure of the strength of bone was better after administering 4-AP to mice,” Elfar said. “We also found more BMP2 protein in bone-forming cells at the fracture site, which again told us we found something that could accelerate the process.”
Examining human bone cells exposed to 4-AP in a dish, the scientists saw increased production of bone morphogenetic protein, or BMP2, a bone-building substance used clinically to help with some kinds of bone repair. BMP2 prompted the production of stem cells that become cells called osteoblasts, which are essential to form new bone.
The research team also measured 4-AP’s effects on human bone narrow mesenchymal stem cells and human osteoblast cells in the lab. 4-AP increased the conversion of the stem cells into osteoblasts and the latter’s ability to migrate and grow, which are essential to the healing process.
Elfar said that 4-AP’s role in driving BMP2 gene and protein activity is key to its bone healing effects, and using 4-AP to prompt BMP2 production in the body could be especially important.
“BMP2 is a hormone the body makes to accelerate bone healing,” Elfar said.
BMP2 is known to modulate bone healing and is approved for use in certain medical procedures, including spinal fusion and sinus reconstruction surgery. An artificial version that has orthopedic medicine uses can have side effects, though, including bone resorption and cervical spine swelling. Finding a way to channel naturally produced BMP2 could improve bone healing while avoiding such problems.
The scientists previously showed that 4-AP could prevent bone and muscle loss in a mouse model of nerve damage. Similarly, they saw indications of 4-AP’s healing effects for wound, nerve and limb injuries.
The researchers plan to eventually test 4-AP’s potential use in healing bones in a clinical trial. They also want to better understand the drug’s effects on BMP2 production, and more broadly, on the biology of healing bone.
New research from the University of South Australia shows that the trusted staples of paracetamol and ibuprofen are quietly fuelling one of the world’s biggest health threats: antibiotic resistance.
In the first study of its kind, researchers found that ibuprofen and paracetamol are not only driving antibiotic resistance when used individually but amplifying it when used together.
Assessing the interaction of non-antibiotic medications, the broad-spectrum antibiotic ciprofloxacin, and Escherichia coli, researchers found that ibuprofen and paracetamol significantly increased bacterial mutations, making E. coli highly resistant to the antibiotic.
It’s an important finding that has serious health implications, particularly for people in aged care homes, where multiple medications are regularly administered.
Lead researcher UniSA’s Associate Professor Rietie Venter says the findings raise important questions about the risks of polypharmacy in aged care.
“Antibiotics have long been vital in treating infectious diseases, but their widespread overuse and misuse have driven a global rise in antibiotic-resistant bacteria,” Assoc Prof Venter says.
“This is especially prevalent in residential aged care facilities, where older people are more likely to be prescribed multiple medications – not just antibiotics, but also drugs for pain, sleep, or blood pressure – making it an ideal breeding ground for gut bacteria to become resistant to antibiotics.
“In this study we looked at the effect of non-antibiotic medicines and ciprofloxacin, an antibiotic which is used to treat common skin, gut or urinary tract infections.
“When bacteria were exposed to ciprofloxacin alongside ibuprofen and paracetamol, they developed more genetic mutations than with the antibiotic alone, helping them grow faster and become highly resistant. Worryingly, the bacteria were not only resistant to the antibiotic ciprofloxacin, but increased resistance was also observed to multiple other antibiotics from different classes.
“We also uncovered the genetic mechanisms behind this resistance, with ibuprofen and paracetamol both activating the bacteria’s defences to expel antibiotics and render them less effective.”
Assoc Prof Venter says the study shows how antibiotic resistance is a more complex challenge than previously understood, with common non-antibiotic medications also playing a role.
“Antibiotic resistance isn’t just about antibiotics anymore,” Assoc Prof Venter says.
“This study is a clear reminder that we need to carefully consider the risks of using multiple medications – particularly in aged care where residents are often prescribed a mix of long-term treatments.
“This doesn’t mean we should stop using these medications, but we do need to be more mindful about how they interact with antibiotics – and that includes looking beyond just two-drug combinations.”
The researchers are calling for further studies into drug interactions among anyone on long-term medication treatment regimes so we can gain a greater awareness of how common medications may impact antibiotic effectiveness.
As of September 2025, Aspen Pharmacare will undertake the distribution of selected Boehringer Ingelheim prescription medicines across South Africa. This partnership represents a significant step towards ensuring that more patients gain timely access to the treatments they need, helping improve health outcomes today and for generations to come.
“Our priority is always patients. Partnering with Aspen means we can bring our innovative medicines to people faster, addressing urgent needs in cardio-renal-metabolic and lung diseases as well as stroke. As a company, we focus on developing innovative therapies that can improve and extend lives in areas of high unmet medical need. Together, we are not only improving access today but also transforming the lives of future generations across South Africa,” says Dr Anthony Lauw, General Manager and Head of Human Pharma, Boehringer Ingelheim Southern Africa.
Commenting on the partnership, Heinz Schütte, Aspen Regional CEO South Africa Commercial said: “For us, this collaboration is about putting patients first. By leveraging our reach and expertise in South Africa, we can ensure that Boehringer Ingelheim’s innovative therapies are accessible to more people, when and where they need them. This is an important milestone in our ongoing mission to improve health outcomes across the country.”
Boehringer Ingelheim, an independent and family-owned company, takes a long-term view of healthcare, investing heavily in research and development to deliver innovative therapies that address unmet medical needs.
This agreement was approved by the South African Competition Tribunal on 15 July 2025, following a recommendation from the Competition Commission.
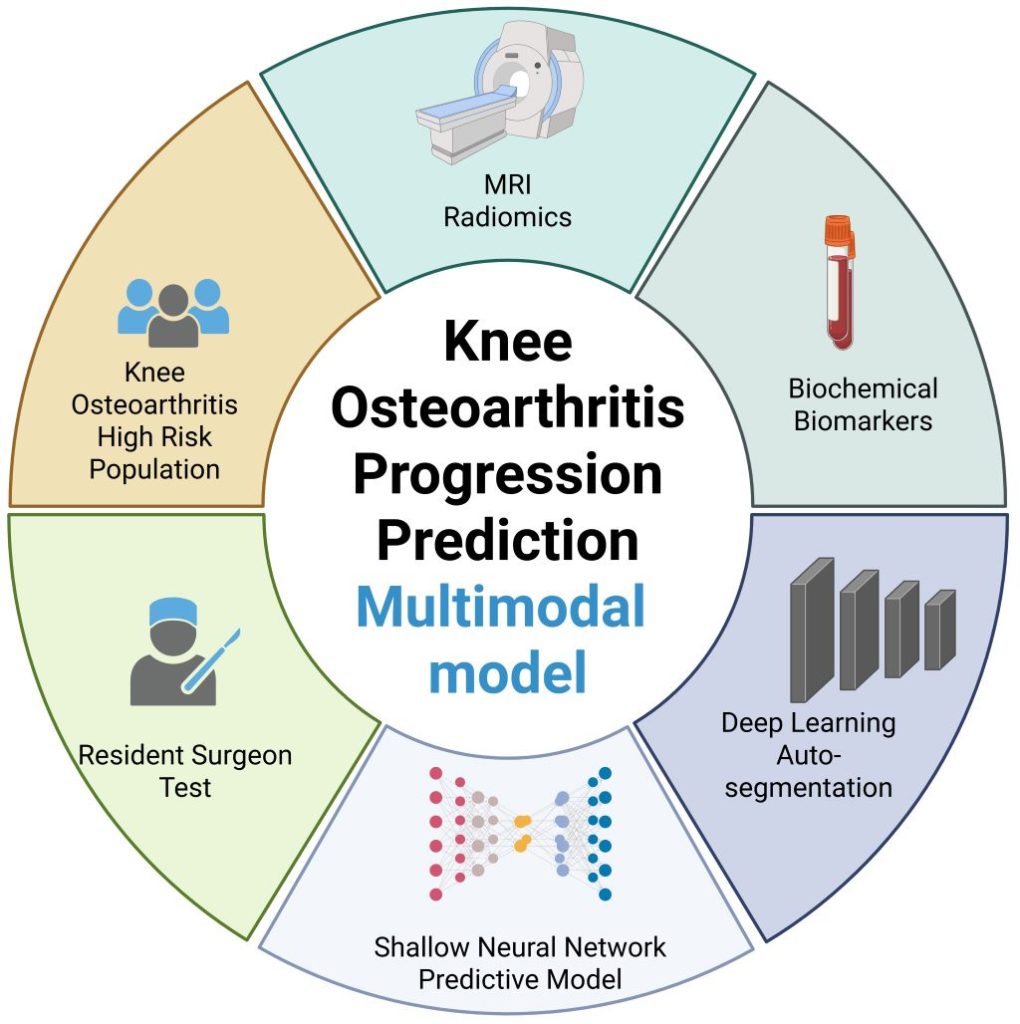
New model that combines MRI, biochemical, and clinical information shows potential to enhance care
Illustration highlighting the integration of MRI radiomics and biochemical biomarkers for knee osteoarthritis progression prediction. Created with Biorender.
Image credit: Wang T, et al., 2025, PLOS Medicine, CC-BY 4.0
An artificial intelligence (AI)-assisted model that combines a patient’s MRI, biochemical, and clinical information shows preliminary promise in improving predictions of whether their knee osteoarthritis may soon worsen. Ting Wang of Chongqing Medical University, China, and colleagues present this model August 21st in the open-access journal PLOS Medicine.
In knee osteoarthritis, cartilage in the knee joint gradually wears away, causing pain and stiffness. It affects an estimated 303.1 million people worldwide and can lead to the need for total knee replacement. Being able to better predict how a person’s knee osteoarthritis may worsen in the near future could help inform more timely treatment. Prior research suggests that computational models combining multiple types of data – including a patient’s MRI results, clinical assessments, and blood and urine biochemical tests – could enhance such predictions.
The integration of all three types of information in a single predictive model has not been widely reported. To address that gap, Wang and colleagues utilized data from the Foundation of the National Institutes of Health Osteoarthritis Biomarkers Consortium on 594 people with knee osteoarthritis, including their biochemical test results, clinical data, and a total of 1,753 knee MRIs captured over a 2-year timespan.
With the help of AI tools, the researchers used half of the data to develop a predictive model combining all three data types. Then, they used the other half of the data to test the model, which they named the Load-Bearing Tissue Radiomic plus Biochemical biomarker and Clinical variable Model (LBTRBC-M).
In the tests, the LBTRBC-M showed good accuracy in using a patient’s MRI, biochemical and clinical data to predict whether, within the next two years, they would experience worsening pain alone, worsening pain alongside joint space narrowing in the knee (an indicator of structural worsening), joint space narrowing alone, or no worsening at all.
The researchers also had seven resident physicians use the model to assist their own predictions of worsening knee osteoarthritis, finding that it improved their accuracy from 46.9 to 65.4 percent.
These findings suggest that a model like LBTRBC-M could help enhance knee osteoarthritis care. However, further model refinement and validation in additional groups of patients is needed.
The authors add, “Our study shows that combining deep learning with longitudinal MRI radiomics and biochemical biomarkers significantly improves the prediction of knee osteoarthritis progression—potentially enabling earlier, more personalized intervention.”
The authors state, “This work is the result of years of collaboration across multiple disciplines, and we were especially excited to see how non-invasive imaging biomarkers could be leveraged to support individualized patient care.”
Co-author Prof. Changhai Ding notes, “This study marks a step forward in using artificial intelligence to extract meaningful clinical signals from complex datasets in musculoskeletal health.”
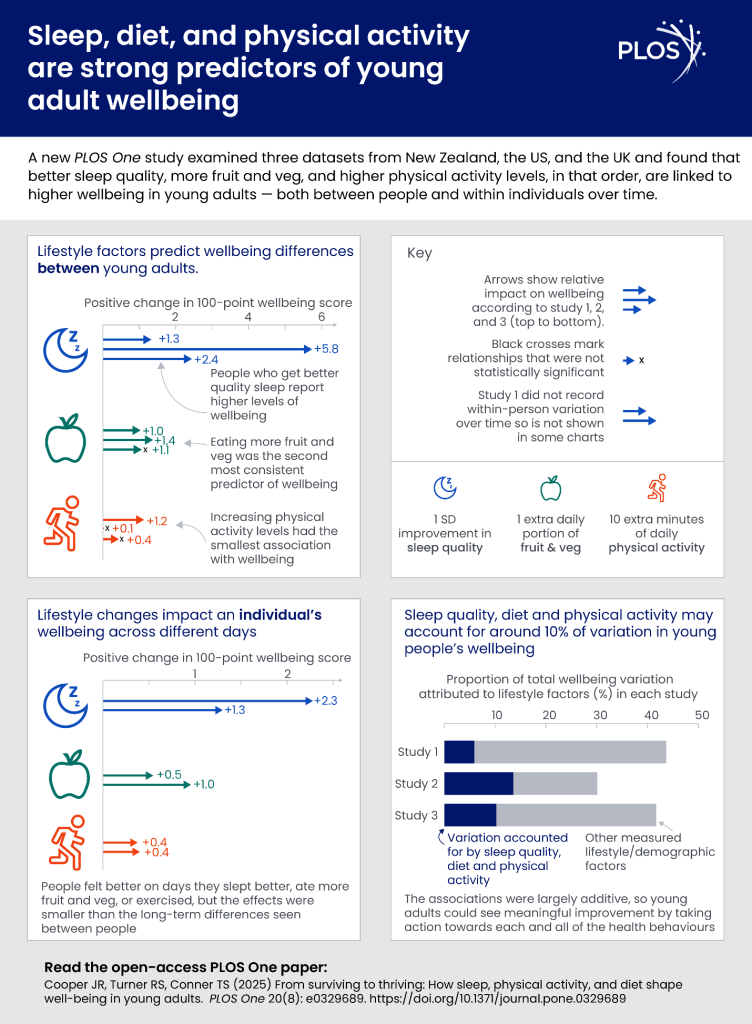
Study also suggests eating fruit and vegetables and exercising are linked with strong benefits – and fruit and vegetable consumption might compensate for poor sleep
A new study of young adults has strongly linked better sleep quality with better mental wellbeing, with fruit and vegetable consumption and physical activity also strongly associated with psychological wellbeing. Perhaps surprisingly, the findings also suggest that boosting fruit and vegetable intake could potentially help mitigate the effects on wellbeing of a poor night’s sleep. Dr Jack Cooper, previously from the University of Otago, New Zealand, and colleagues present these findings in the open-access journal PLOS One on August 27, 2025.
Prior research has linked better health behaviours—actions that people can adjust in their lives—to better physical health. Evidence also suggests that health behaviours may be linked to mental wellbeing. However, research on this topic has been limited. For example, studies have typically focused only on mental illness, a separate measure from positive psychological wellbeing, and they typically neglect to consider how different health behaviours might interact to affect wellbeing.
To address these and other gaps, Cooper and colleagues analysed relationships between three health behaviours – sleep quality, eating fruits and vegetables, and physical activity – and psychological wellbeing in adults aged 17 to 25. They used data from three studies: a survey study of 1032 adults in New Zealand, the UK, and the US; a 13-day study of 818 New Zealand adults who were asked to keep a daily diary; and an 8-day diary study of 236 New Zealand adults who also wore Fitbits tracking physical activity.
Across all three studies, better sleep quality was most strongly associated with better mental wellbeing, with fruit and vegetable consumption coming in second. Both behaviours showed benefits even when comparing between different days for the same person – so eating more fruit and vegetables one day was associated with a real-time wellbeing boost. Physical activity – whether measured by FitBits or diaries, which aligned – was also linked to better wellbeing, but mostly when comparing between days for an individual rather than when comparing across individuals.
Links between each of the three behaviors and wellbeing appeared to be independent and additive – which might mean that the more of them you do, the bigger the wellbeing benefit. The only exception: above-average intake of fruits and vegetables appeared to mitigate the effects of a poor night’s sleep, and a good night’s sleep appeared to protect against lower fruit and vegetable intake.
This study used samples of young adults from three countries—the U.K., U.S., and New Zealand—and samples sizes were relatively homogeneous. Future research could address some of these limitations by including participants from additional countries and increasing the sample size to improve generalizability. Although this study could not prove a causative link between these behaviors and mental wellbeing, the authors hope that their findings could inform efforts to improve psychological wellbeing of young adults.
Lead author Dr. Jack Cooper adds: “Young adults don’t have to reach some objective benchmark of healthiness to see wellbeing improvement. Sleeping a little better, eating a little healthier, or exercising even for 10 minutes longer than you normally do was associated with improvements to how you feel that day.”
Senior author Professor Tamlin Conner, of the University of Otago Psychology Department, adds: “Understanding what lifestyle factors support wellbeing can help young adults not just ‘get by’ but thrive during this critical life stage.”
“Of these healthy habits, sleep quality stood out as the strongest and most consistent predictor of next-day wellbeing, but eating fruit and vegetables and being active also helped boost wellbeing”.
“This age group faces unique pressures – such as leaving home, financial stress, educational pressures and social stressors – that can lower happiness. Understanding what lifestyle factors support wellbeing can help young adults not just ‘get by’ but thrive during this critical life stage.
Time to work together to close vaccine gap putting children and communities at risk
Photo by Mufid Majnun on Unsplash
South Africa is facing a growing public health concern, as large numbers of children1 miss out on life-saving vaccinations.
According to Dr Zeina Elian, Vaccines Medical Head for Sanofi Africa, the country is seeing a resurgence in ‘zero dose’ communities. These are areas where children have not received a single routine vaccine. In low dose communities, under-immunisation is similarly leaving many children at risk for preventable diseases.
“We are seeing entire groups of children falling through the cracks,” says Dr Elian. “If these children remain unvaccinated, diseases we thought were under control can, and will, return.”
What is a ‘zero dose’ child?
A ‘zero dose’ child is one who has not received any of the vaccines scheduled under South Africa’s national Expanded Programme on Immunisation (EPI). “In these communities, children miss out on all opportunities for protection, leaving them vulnerable to highly contagious and often dangerous diseases like diphtheria, pertussis (whooping cough) and measles,” says Dr Elian.
Recent data shows South Africa had 220 000 zero-dose children1 in 2023, ranking it among the top 20 countries globally with the highest number of unvaccinated children. “We’ve seen outbreaks of whooping cough in the past year and are currently experiencing a rise in diphtheria cases. These diseases are preventable. Their return points directly to gaps in coverage,” says Dr Elian.
Role of the health care provider
Health care providers play a crucial role in catch-up vaccination. They identify patients who are behind on their vaccines, explain the importance of protection, and address concerns with clear, trusted information. With the right training and guidelines, they create safe and supportive environments where patients feel comfortable catching up on missed doses. By confidently recommending and administering vaccines, providers help close immunity gaps and protect both individuals and the wider community.
Vaccine hesitancy and misinformation put lives at risk
“Vaccine hesitancy and the spread of misinformation are undermining immunisation efforts. False information spreads faster than facts. Rebuilding trust in vaccines is crucial, not just to protect individuals, but to protect entire communities through herd immunity,” says Dr Elian.
Herd immunity means that when most people in a community are vaccinated, it becomes much harder for diseases to spread. This protects everyone, especially babies, the elderly, and people with health conditions who can’t get vaccinated themselves.
Dr Elian also stresses that we need to take flu more seriously. “We don’t talk enough about flu. People think it’s just a seasonal thing or a mild illness, but flu can be serious, especially for pregnant women, the elderly and people with chronic conditions. Every year, we have people ending up in hospital with flu complications. It’s vaccine-preventable, and yet uptake remains low.”
Immunisation is important at every stage of life
Vaccination is a lifelong health strategy, not just a childhood milestone. Dr Elian says that life-course immunisation means starting with vaccines during pregnancy and continuing through all stages of life. The aim is to protect people at the times they are most vulnerable, a need that changes as we age.
Key examples include:
Pregnant women: flu and whooping cough vaccines
Adolescents: HPV, tetanus, diphtheria and pertussis boosters
Young adults: meningococcal vaccines for students and military recruits
Adults: pertussis boosters every 5 to 10 years, especially for those with asthma or COPD
Older adults: annual flu vaccines and pneumococcal vaccines to prevent serious complications
According to the latest National Institute for Communicable Diseases (NICD) alert, in the current diphtheria outbreak2, 70% of cases occurred in adults, and the case-fatality rate was 21%. “These are not just childhood diseases,” says Dr Elian. “Adults are clearly vulnerable too. Lifelong immunisation must become standard in South Africa.”
Dr Elian adds that public and professional attitudes need to change.
“Every health appointment is a chance to check vaccine status. Not just for kids, but for parents, grandparents, students and workers. It’s a shift in culture, where we all become more proactive about protecting our health.”
Falling vaccination rates carry a heavy economic cost
While routine vaccines are free in the public system, indirect barriers such as time off work and transport costs persist. But the economic cost of illness is often much higher.
“Missing a day of work to vaccinate a child may feel like a loss, but missing five days to care for a sick child is far worse,” says Dr Elian. “For adults, illness can mean lost income, expensive treatment and even hospitalisation. At a national level, low vaccination coverage fuels more frequent and severe outbreaks, forcing costly catch-up campaigns, increasing the need for surveillance, and placing added strain on already stretched health systems. The economic toll includes reduced productivity and higher healthcare expenditure, making prevention through vaccination the far more cost-effective option.”
Act now to keep yourself, your family and community safe
Take a more active role in your health by speaking to healthcare professionals. “Every visit to the clinic or doctor is an opportunity to ask, ‘What vaccines do I need?’ ‘What about my children?’, ‘What’s recommended for my age or condition?’, ‘Am I up to date on my vaccines?’ That one question could prevent serious illness or even death,” says Dr Elian.
Dr Elian also advises parents and caregivers to check their children’s Road to Health booklets to ensure vaccines are up to date, especially before school entry.
“Vaccines save lives. They prevent suffering and they protect the people around us. But only if we use them.”
Quick facts
Since 1974, the Expanded Programme on Immunisation has saved more than 50 million lives3 across Africa.
Vaccines protect against serious diseases like diphtheria, pertussis (whooping cough), measles, flu, and more.
Childhood vaccines are free at public clinics.
South Africa is currently experiencing preventable disease outbreaks due to low vaccination rates.
Everyone has a role to play in preventing illness – parents, students, healthcare workers, and older adults.
Ask your healthcare provider if you’re due for a vaccine or booster.
In the latest chapter of a long-running legal battle over the Gauteng Department of Health’s obligation to provide people in the province with radiation oncology services, the department has suffered another loss in the courts. Spotlight assesses the legal situation and asks what it means for people still waiting for the life-saving treatment.
With another court loss suffered this August, the Gauteng Department of Health has once again been ordered to urgently provide treatment for cancer patients who have been left in the lurch.
This ruling, handed down on August 5 by Judge Evette Dippenaar, follows urgent legal action brought by the Cancer Alliance. It was in response to the Gauteng health department’s appeal against a ruling handed down on March 27 by acting Judge Stephen van Nieuwenhuizen. That order compelled the department to clear its years-long backlogs in getting cancer treatment to patients.
In its March ruling, the South Gauteng High Court in Johannesburg found the department’s failure to deliver this critical treatment to be unconstitutional and unlawful. The decision follows the department’s failure to spend a R784 million allocation granted by the provincial Treasury in 2023 to reduce the treatment backlog by outsourcing services to the private sector over a three-year period. Due to severe delays, the department was forced to return the first R250 million tranche.
Van Nieuwenhuizen strongly criticised the department, stating: “The provincial health respondents have done nothing meaningful since the money was allocated in March 2023 to actually provide radiation oncology treatment to the cancer patients. Meanwhile, the health and general well-being of the patients has significantly deteriorated. There is clear, ongoing, and irreparable harm being suffered by those still waiting for treatment.”
He also condemned the department for its lack of accountability and poor management of public resources, finding that it had failed to uphold ethical standards, act transparently, or respond to patients’ needs fairly and effectively.
The court instructed the department to:
Take immediate action, including diversion to private facilities, to provide radiation oncology services to all patients on the backlog list,
Update the backlog list within 45 days,
Submit a detailed progress report on efforts to deliver treatment, and
Present a long-term plan for ongoing cancer treatment services within three months.
But Gauteng health MEC Nomantu Nkomo-Ralehoko and the health department challenged the judgment in May, just as their 45 days to act ran out. They chose instead to take the entire matter on appeal to the Supreme Court of Appeal (SCA).
In response, the Cancer Alliance, represented by SECTION27 (*see disclosure), went back to court for an interim order to make the March 27 ruling immediately enforceable, and not suspended until a ruling is made by the SCA. It is in response to this application that Judge Dippenaar ruled on August 5 that the March ruling is indeed immediately enforceable.
Two courts have now sent a clear message to the Gauteng health department, says attorney Khanyisa Mapipa, who heads health rights at SECTION27. She adds: “The Gauteng Department of Health’s action should be in the interest of the person who is seeking treatment. It should not be to deny, deny, deny and then to fight in the courts and not take any accountability.”
The waiting list
The estimated number of people on a waiting list for cancer treatment in 2022 was around 3 000 people. New data on this has not been made publicly available.
There are some signs of progress, although details are hard to pin down. In a statement released on August 24, which reiterates a July 20 statement, the Gauteng health department said it had introduced a strategic partnership with private service providers. “As the beginning of August 2025, 563 patients were receiving radiation oncology care through private partnerships, while 1 076 patients had completed treatment by end of July 2025,” it stated.
Both statements also noted that work was underway to complete new radiotherapy centres at Chris Hani Baragwanath and Dr George Mukhari Academic Hospitals.
But Mapipa says they still don’t have full details that comply with the court order. “What we’re asking for essentially is what the department should be doing anyway and that is for them to go through their patient files to establish who is still on the backlog list; who has passed away, who has received treatment, when patients were last assessed and what treatment they qualify for; and if it was a public facility or were they diverted to a private facility,” she says.
“As the judge pointed out in March, the department has to do this as a constitutional obligation, whether they fight this to the Constitutional Court or not, their obligation is to provide treatment for people who meet the criteria. Those on the backlog list meets the criteria,” she says.
Part of the March order also compelled the department to file progress reports with the court within three months on the measures taken to provide treatment and its long-term plans to resolve the ongoing cancer treatment crisis in Gauteng. Spotlight’s understanding is that these progress reports have not been submitted.
This is an important measure, Mapipa says, given the department’s poor track record. “The court rulings in both judgments found that because they have failed to be transparent throughout this process, the department is compelled to provide these reports to the courts,” she adds.
It is as yet unclear how the Gauteng health department plans to proceed. The department, in its three-paragraph statement following the August judgment, stated that it would review “the contents and implications” to determine and communicate its next steps. Their deadline to appeal the August 5 ruling was 26 August 2025. The department did not respond to questions from Spotlight.
Calls for accountability
Jack Bloom, Democratic Alliance shadow health MEC in Gauteng, says that without a proper audit and update of the backlog list of patients needing care, the “cancer treatment scandal has probably cost more lives than the 144 mental patients who died in the Life Esidimeni tragedy when they were sent to illegal NGOs”.
Bloom is calling for heads to roll, with Nkomo-Ralehoko and head of department Arnold Lesiba Malotana in his crosshairs.
“The DA condemns the department’s legal stalling tactics that harms patients who urgently require lifesaving treatment…Premier [Panyaza] Lesufi should not allow this cancer disaster to continue,” he says.
Salomé Meyer, spokesperson for Cancer Alliance, says that the legal proceedings are a distraction of the realities on the hospital floor. Charlotte Maxeke Johannesburg Academic Hospital for instance, she says, remains in “crisis”. She maintains there is a scarcity of sufficient and operational radiation oncology machinery, as well as extreme shortages in radiation oncology staff to operate the machines.
Meyer says the situation at Charlotte Maxeke Hospital dates back to 2017 when CEO Gladys Bagoshi was made aware of mounting challenges from a shortage of equipment and staffing.
“In 2021, Bagoshi turned down an equipment allocation, which Charlotte Maxeke Hospital desperately needed, so this allocation went to George Mukhari Hospital and Chris Hani Baragwanath Hospital instead. But the cobalt bunkers required to house the machines at these hospitals had not been built and are only expected to be completed in 2026 – so the machines remain in storage. In 2022, an order was finally placed for additional linacs [used for high energy beam radiation treatments] for the existing cobalt bunkers at Charlotte Maxeke Hospital, but that tender is still not finalised,” says Meyer.
She adds: “This is a failure of planning, governance, and accountability and we have to ask who is being held accountable when the same CEO has remained in place all these years.”
Neither Bagoshi nor the health department responded to questions on these assertions.
Disclosure: SECTION27 was involved in the court proceedings described in this article. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. The Spotlight editors gave special attention to maintaining this editorial firewall in the production of this story.
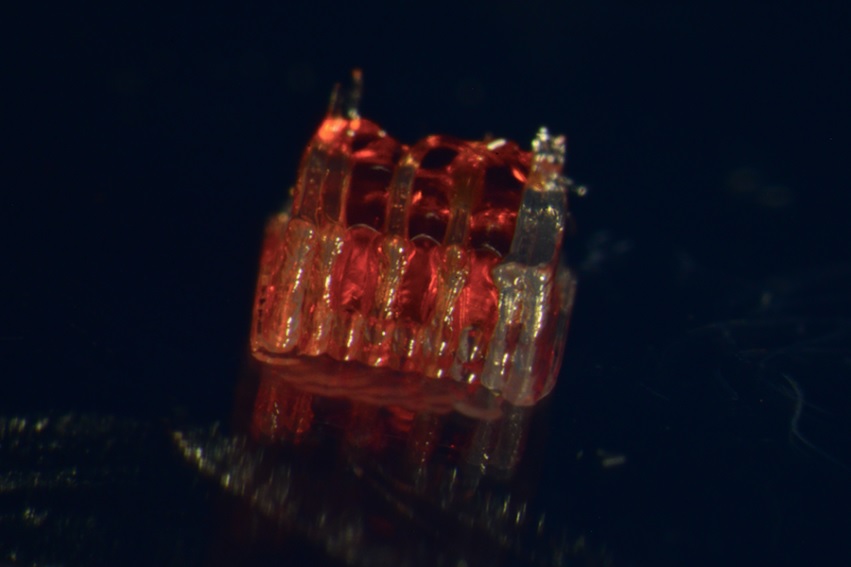
New research combines 3D printing, stem cell biology, and lab-grown tissues for possible treatments of spinal cord injuries. Photo provided by: McAlpine Research Group, University of Minnesota
For the first time, a research team at the University of Minnesota Twin Cities demonstrated a groundbreaking process that combines 3D printing, stem cell biology, and lab-grown tissues for spinal cord injury recovery.
The study was recently published in Advanced Healthcare Materials. Currently, there is no way to completely reverse the damage and paralysis from the injury. A major challenge is the death of nerve cells and the inability of nerve fibres to regrow across the injury site. This new research tackles this problem head-on.
The method involves creating a unique 3D-printed framework for lab-grown organs, called an organoid scaffold, with microscopic channels. These channels are then populated with regionally specific spinal neural progenitor cells (sNPCs), which are cells derived from human adult stem cells that have the capacity to divide and differentiate into specific types of mature cells.
“We use the 3D printed channels of the scaffold to direct the growth of the stem cells, which ensures the new nerve fibres grow in the desired way,” said Guebum Han, a former University of Minnesota mechanical engineering postdoctoral researcher and first author on the paper who currently works at Intel Corporation. “This method creates a relay system that when placed in the spinal cord bypasses the damaged area.”
n their study, the researchers transplanted these scaffolds into rats with spinal cords that were completely severed. The cells successfully differentiated into neurons and extended their nerve fibres in both directions – rostral (toward the head) and caudal (toward the tail) – to form new connections with the host’s existing nerve circuits.
The new nerve cells integrated seamlessly into the host spinal cord tissue over time, leading to significant functional recovery in the rats.
“Regenerative medicine has brought about a new era in spinal cord injury research,” said Ann Parr, professor of neurosurgery at the University of Minnesota. “Our laboratory is excited to explore the future potential of our ‘mini spinal cords’ for clinical translation.”
While the research is in its beginning stages, it offers a new avenue of hope for those with spinal cord injuries. The team hopes to scale up production and continue developing this combination of technologies for future clinical applications.