A healthy lifestyle has important benefits, but weight alone might not give an adequate picture of someone’s health, say experts
Source: Pixabay CC0
Focusing solely on achieving weight loss for people with a high body mass index (BMI) may do more harm than good, argue experts in The BMJ.
Dr Juan Franco and colleagues say, on average, people with high weight will not be able to sustain a clinically relevant weight loss with lifestyle interventions, while the potential harms of weight loss interventions, including the reinforcement of weight stigma, are still unclear.
They stress that a healthy lifestyle has important benefits, but that weight alone might not give an adequate picture of someone’s health, and say doctors should provide high quality, evidence based care reflecting individual preferences and needs, regardless of weight.
Lifestyle interventions that focus on restricting an individual’s energy intake and increasing their physical activity levels have for many decades been the mainstay recommendation to reduce weight in people with obesity, explain the authors.
However, rigorous evidence has indicated that these lifestyle interventions are largely ineffective in providing sustained long term weight loss and reducing cardiovascular events (eg, heart attacks and strokes) or death.
Even though a healthy lifestyle provides important benefits, acknowledging that weight alone might not give an adequate picture of someone’s health, and recognising the limitations of lifestyle interventions for weight loss, could pave the way for more effective and patient centred care, they say.
Focusing on weight loss might also contribute to societal weight bias – negative attitudes, assumptions, and judgments about people based on their weight – which may not only have adverse effects on mental health but may also be associated with disordered eating, the adoption of unhealthy habits, and weight gain, they add.
They point out that recent clinical guidelines reflect the growing recognition that weight is an inadequate measure of health, and alternative approaches, such as Health at Every Size (HAES), acknowledge that good health can be achieved regardless of weight loss and have shown promising results in improving eating behaviours.
While these approaches should be evaluated in large clinical trials, doctors can learn from them to provide better and more compassionate care for patients with larger bodies, they suggest.
“Doctors should be prepared to inform individuals seeking weight loss about the potential benefits and harms of interventions and minimise the risk of developing eating disorders and long term impacts on metabolism,” they write. “Such a patient centred approach is likely to provide better care by aligning with patient preferences and circumstances while also reducing weight bias.”
They conclude: “Doctors’ advice about healthy eating and physical activity is still relevant as it may result in better health. The main goal is to offer good care irrespective of weight, which means not caring less but rather discussing benefits, harms, and what is important to the patient.”
Women diagnosed with premenstrual symptoms have a slightly increased risk of developing cardiovascular disease later in life. This is shown by a new study from Karolinska Institutet published in Nature Cardiovascular Research.
Premenstrual symptoms include premenstrual syndrome (PMS) and the more severe form, premenstrual dysphoric disorder (PMDD). The symptoms, which appear a few days before menstruation and then subside, can be both psychological and physical.
The study included more than 99 000 women with premenstrual symptoms who were followed for up to 22 years. The researchers compared their health with women without these symptoms – both in the general population and by comparing them with their own sisters to take into account hereditary factors and upbringing.
The results show that women with premenstrual symptoms had about a ten per cent higher risk of developing cardiovascular disease. When the researchers also looked at different types of cardiovascular disease, they found that the link was particularly strong for heart rhythm disorders (arrhythmias), where the risk was 31 per cent higher, and for stroke caused by a blood clot, where the risk was 27 per cent higher. Even after the researchers took into account other factors such as smoking, BMI and mental health, the link between premenstrual symptoms and increased disease risk remained.
”The increased risk was particularly clear in women who were diagnosed before the age of 25 and in those who had also experienced postnatal depression, a condition that can also be caused by hormonal fluctuations,” says first author Yihui Yang, PhD student at the Institute of Environmental Medicine.
Research has not yet identified the cause of this link, but the researchers behind the study suggest three possible explanations. One is that women with premenstrual symptoms may have a disrupted regulation of the renin-angiotensin-aldosterone system (RAAS), which controls blood pressure and fluid balance in the body, among other things. The second is that these women have increased levels of inflammation in the body, which is a known risk factor for atherosclerosis and other heart problems. Finally, it may be because women with premenstrual symptoms may have metabolic abnormalities, which are linked to an increased risk of both stroke and heart attack.
”We hope that our findings will contribute to greater awareness that premenstrual disorders not only affect daily life but can also have consequences for long-term health,” says last author Donghao Lu, associate professor at the same department.
New UCLA research finds that small group professional coaching can reduce physician burnout rates by up to 30%, suggesting that it is more effective than the traditional, and more expensive, one-on-one coaching method.
Nearly half of physicians in the US suffer from burnout, which is marked by emotional exhaustion, depersonalisation and decreased personal accomplishment. These can lead to medical errors and other harmful consequences to the healthcare system and patient outcomes, said lead author Dr Joshua Khalili, director of physician wellness in the UCLA Department of Medicine and assistant clinical professor of medicine at the David Geffen School of Medicine at UCLA.
“Most current evidence related to professional coaching is related to individual coaching and its impact on reducing burnout,” Khalili said. “But individual coaching can be quite costly, which is a barrier to broad implementation.”
Physician burnout is estimated to cost the US healthcare system about $4.6 billion annually, mostly due to costs associated with physician turnover and fewer clinical hours.
The researchers conducted a randomised, wait-list controlled trial with 79 UCLA attending internal medicine physicians for just over a year starting in March 2023. The intervention consisted of six one-hour coaching sessions, with one-third of the group receiving one-on-one coaching via Zoom while another third were coached in small groups consisting of three physicians and one coach. The final third acted as control group, receiving no coaching during the first few months of the trial, and subsequently received six, one-on-one coaching sessions.
The primary outcome the researchers measured was overall burnout. They also examined areas of work life such as workload, control rewards, community, fairness, and values; work engagement such as vigour, dedication, and absorption; self-efficacy, and social support. They measured each of these outcomes before and after the intervention and again six months afterwards.
They found that small group intervention participants experienced a nearly 30% reduction in burnout rate. The burnout rate for the one-on-one coaching fell by 13.5%. By contrast, the control group experienced an 11% increase in burnout rates. Burnout remained stable among the small group participants and continued to fall in the one-on-one group six months after the initial intervention.
Coaching for the one-on-one sessions cost $1000 per participant, compared with $400 for the small group coaching sessions.
“This new, small-group model of professional coaching can make a significant impact in physician burnout and costs much less than the one-on-one model,” Khalili said.
Study limitations include potential selection bias among participants who would most likely benefit from the intervention. The baseline overall burnout rate was higher in the small group coaching arm (70.4%) compared to the one-on-one group (40.0%); however, relative reductions in burnout were similar: 42% in the small group intervention compared to 34% the one-on-one group. In addition, the study was conducted at a large academic centre whose physicians may not be comparable to those in other healthcare institutions.
The researchers are now providing coaching to physicians in the UCLA Department of Medicine and hope that this research encourages other health care institutions and organisations to implement professional coaching, Khalili said.
“By improving physicians’ well-being, engagement, and sense of support, interventions like coaching can enhance the quality of care patients receive, making this a public health priority, not just a workplace issue,” he said.
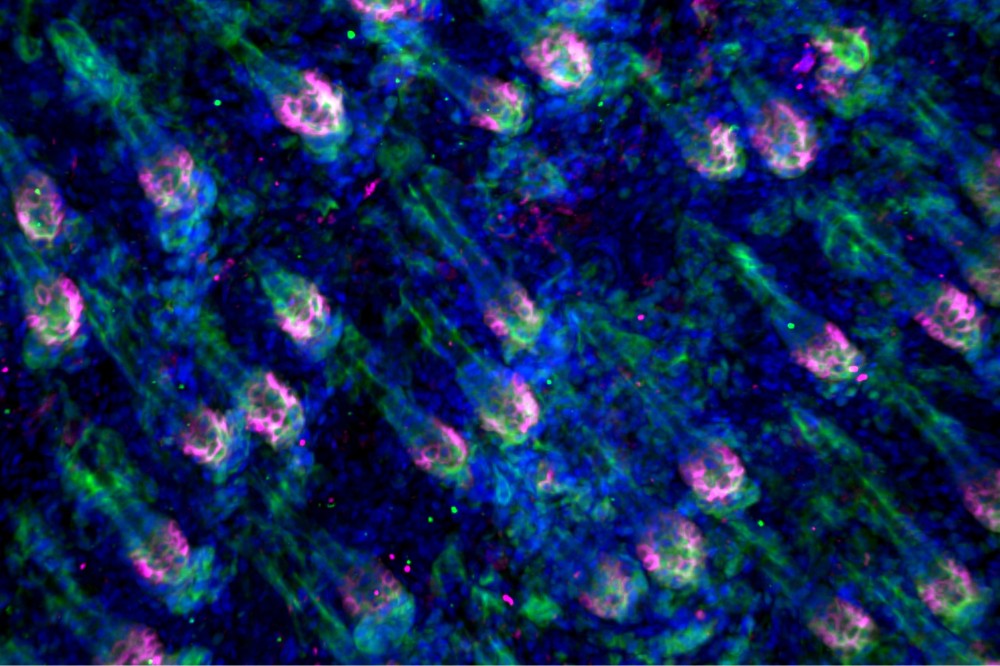
Immunofluorescent microscopy shows hair follicles in the early stages of hair regrowth. (Fuchs Lab)
The skin has two types of adult stem cells: epidermal and hair follicle. Their jobs seem pretty well-defined: maintain the skin, or maintain hair growth. But as research from Rockefeller University has shown, hair follicle stem cells (HFSCs) can switch teams, pitching in to heal the skin when it receives an injury. How do these cells know it’s time to pivot?
The lab behind those original findings has now identified a key signal telling HFSCs when to drop the hair cycle and pick up the skin repair: an integrated stress response (ISR) that directs stem cells to conserve energy for essential tasks.
In the skin, nutrient deficits are sensed by a non-essential amino acid known as serine that’s found in common foods such as meat, grains, and milk. As they demonstrate in a recent study in Cell Metabolism, when serine levels drop, the ISR is activated, causing HFSCs to slow hair production. If the skin is injured on top of nutrient deficits, the ISR is elevated even more, halting hair production and funnelling efforts towards skin repair. This reprioritisation accelerates the healing process.
“Serine deprivation triggers a highly sensitive cellular ‘dial’ that fine tunes the cell’s fate – towards skin and away from hair,” says first author Jesse Novak, former PhD student at Rockefeller’s Robin Chemers Neustein Laboratory of Mammalian Cell Biology and Development, led by Elaine Fuchs. “Our findings suggest that we might be able to speed up the healing of skin wounds by manipulating serine levels through diet or medications.”
Hair stem cells’ second job
Adult tissues harbour stem cell pools that tightly balance cell proliferation, differentiation, and turnover to maintain homeostasis, or normal functioning, and repair wounds. But their metabolic needs remain poorly understood. For the current study, Novak aimed to identify the metabolic factors that keep stem cells humming along during everyday operations – then, track what changes when an injury forces HFSCs to moonlight in wound recovery.
“Most skin wounds that we get are from abrasions, which destroy the upper part of the skin. That area is home to a pool of stem cells that normally takes charge in wound repair. But when these cells are destroyed, it forces hair follicle stem cells to take the lead in repair,” Novak says. “Knowing that, we thought that tracking these skin cells through wound healing presented a very good model for testing if and how metabolites are regulating this process overall.”
Previous findings from the Fuchs lab indicated that pre-cancerous skin stem cells become addicted to serine circulating in the body, and that these cells can be prevented from turning fully cancerous by restricting serine in the diet. These findings demonstrated that the metabolite is a key regulator of tumour formation and inspired trials to implement serine-free diets as cancer treatments. But no one understood how dietary serine deprivation would affect normal tissue functioning. So Novak focused on this amino acid for his studies.
Findings
The team subjected the hair follicle stem cells to a series of metabolic stress tests by either depriving them of serine in their diet or using genetic tricks in mice to selectively prevent hair follicle stem cells from making serine. They found that serine is in direct and constant communication with the ISR, a trigger activated when tissue conditions go off balance. When the serine tank is low, HFSCs tune down hair growth, which requires substantial energy.
Turning to another stress challenge, the team then focused on wound repair. They discovered that the ISR also activates in HFSCs after injury. Moreover, when mice experience both serine deficiency and injury, the pendulum swings even further, suppressing hair regeneration and favoring wound repair. In this way, the ISR measures overall tissue stress levels and prioritizes regenerative tasks accordingly.
“No one likes to lose hair, but when it comes down to survival in stressful times, repairing the epidermis takes precedence,” says Fuchs. “A missing patch of hair isn’t a threat to an animal, but an unhealed wound is.”
Serine’s effect does not go both ways
It was clear that low levels of serine had a significant impact on stem cell fate and behaviour. But what about the opposite? Could a large dose of serine supercharge hair growth, for example?
Unfortunately for anyone who suffers from hair loss, it turns out that the body tightly regulates the amount of serine in circulation. When Novak fed mice six times the amount of serine than normal, their serine levels only rose 50%.
“However, we did see that if we prevented a stem cell from making its own serine and replenished its losses through a high-serine diet, we were able to partially rescue hair regeneration,” Novak adds.
Next on the horizon is exploring the potential to speed up wound healing through reducing dietary serine or via medications that affect serine levels or ISR activity. The team also wants to test other amino acids to find out whether serine is unique in its influence. “Overall, the ability of stem cells to make cell fate decisions based upon the levels of stress they experience is likely to have broad implications for how tissues optimise their regenerative capacities in times where resources are scarce,” says Fuchs.
Approximately 40% of the European population are allergic to pollen, and their symptoms cause an estimated loss of 100 million school- and workdays every year. The prevalence of hay fever has been surging for decades and this is likely to continue – a change so fast that genetic and health changes can’t be solely responsible. Improved hygiene, the widespread use of antibiotics and antiseptics, lifestyle changes, diet, pollution, and the climate crisis are also thought to play a major role in this increase.
But now there is new hope for sufferers. As proof-of-principle, researchers have engineered an antibody from mice, which when applied to the inside of the nose stops mice from developing hay fever and asthma symptoms in response to mugwort pollen. Mugwort is the most common cause of pollen allergies in central Asia and parts of Europe, where between 10% and 15% of people with hay fever are allergic to it. The article was published in Frontiers in Immunology.
“This is the first time a monoclonal antibody designed to block a specific pollen allergen has been delivered directly into the nose, and been shown to protect against allergy symptoms in the upper and lower airways,” said Prof Kaissar Tabynov, the director of the International Center for Vaccinology at the Kazakh National Agrarian Research University (KazNARU) in Almaty, and the study’s senior author.
“In the future, similar antibodies could be developed for other major pollen allergens, such as ragweed or grass. This opens the door to a new generation of precision allergy treatments that are fast-acting, needle-free, and tailored to individual allergen sensitivities.”
‘Molecular shield’
Traditional treatment is allergen-specific immunotherapy: patients are exposed to gradually increasing doses of the allergen, until they become desensitised. However, this doesn’t work for all patients, and in recent decades, so-called ‘allergen-specific monoclonal antibody therapy’ has increasingly come to the fore as an alternative.
In allergen-specific monoclonal antibody therapy, researchers engineer antibodies of the IgG class, which either specifically recognise the allergen itself and block it, or bind to IgE antibodies in general. In either case, this prevents the allergen from triggering an allergic reaction. A disadvantage is that typically, these antibodies needed to be injected into the bloodstream – until now.
“Our method acts immediately and locally at the lining of the nose, by neutralising the allergen on contact. This ‘molecular shield’ not only prevents IgE antibodies from being activated, but may also reduce inflammation through other mechanisms, such as calming immune cell responses and promoting regulatory pathways,” explained Tabynov.
The researchers injected mice with a dose of mugwort pollen, stimulating them to produce antibodies against it. The mice were then humanely euthanised and their spleens harvested to isolate white blood cells. The use of mice was approved by the local Institutional Animal Care and Use Committee, under the Ministry of Health of the Republic of Kazakhstan.
The white blood cells were then fused with laboratory-grown cancer cells from mice with multiple myeloma. This yielded five immortal ‘hybridoma’ cell lines which each secreted a single type (hence ‘monoclonal’) of antibody against mugwort pollen. A suite of diagnostic tests showed that the most powerful was produced by hybridoma cell line XA19, which was selected for further development.
Reduction in allergy symptoms
To test their efficacy, purified antibodies from XA19 were administered to the interior of the nose of five mice, which had been stimulated to become allergic to mugwort pollen through injections of pollen extract. Five additional mice served as positive control: they had been similarly sensitized but received a placebo. A further five mice were the negative control, neither sensitized to the pollen nor given monoclonal antibodies. Three weeks later, all mice were exposed three times under anaesthesia to an aerosol of mugwort pollen, as well as to pollen extract delivered directly inside the nose.
The results showed that the sensitized mice given the XA19 antibody displayed a major reduction in allergy symptoms compared to controls: for example, they showed a weaker ear swelling response to the pollen (a common allergic reaction in rodents); they rubbed their nose less frequently, indicating less irritation of the upper airways; their full lung capacity was preserved upon exposure to the pollen; and they showed less inflammation inside the nostrils. Inside the lungs, levels of two inflammation-promoting molecules called cytokines were likewise reduced.
The researchers concluded that the monoclonal antibody from XA19 is effective in blocking allergic reactions against mugwort pollen triggered by IgE, at least in mice.
“Before this treatment can be tested in people, we need to adapt the antibody to make it suitable for humans – a process called ‘humanisation’ – and conduct additional preclinical safety and efficacy studies,” said Tabynov.
“If these are successful and provided we have adequate support, we could begin clinical trials in two to three years, though bringing it to market would likely take five to seven years. We are already planning for this transition and working on scaling up production.”
The age of menarche can offer valuable clues about a woman’s long-term risk for conditions like obesity, diabetes, heart disease and reproductive health issues, according to a study being presented Sunday at ENDO 2025, the Endocrine Society’s annual meeting in San Francisco.
The Brazilian study found that both early and late menarche – the age when women first get their period– are linked to different health risks. Women who had their first period before age 10 were more likely to develop obesity, hypertension, diabetes, heart problems and reproductive issues like pre-eclampsia later in life. Women who started their period after age 15 were less likely to be obese but had a higher risk of menstrual irregularities and certain heart conditions.
“We now have evidence from a large Brazilian population that confirms how both early and late puberty can have different long-term health impacts,” said study author Flávia Rezende Tinano of the University of Sao Paulo in Sao Paulo, Brazil. “While early menarche increases the risk for multiple metabolic and heart problems, late menarche may protect against obesity but increase certain heart and menstrual issues. Most women can remember when they had their first period, but they might not realise that it could signal future health risks. Understanding these links can help women and their doctors be more proactive about preventing conditions like diabetes, high blood pressure and heart disease.”
Tinano said the study is one of the largest of its kind in a developing country, providing valuable data on a topic that has mostly been studied in wealthier countries. “It highlights how early and late puberty can affect a woman’s long-term health, especially in underrepresented populations like those in Latin America,” she said.
The study was part of the Brazilian Longitudinal Study of Adult Health (ELSA-Brazil) and evaluated data from 7623 women ages 35 to 74. The age of their first period was categorised as early (less than 10 years old), typical (ages 10 to 15) or late (older than 15). They assessed the women’s health through interviews, physical measurements, lab tests and ultrasound imaging.
“Our findings suggest that knowing a woman’s age at her first period can help doctors identify those at higher risk for certain diseases,” Tinano said. “This information could guide more personalised screening and prevention efforts. It also emphasises the importance of early health education for young girls and women, especially in developing countries.”
Investigators have developed an artificial intelligence-assisted diagnostic system that can estimate bone mineral density in both the lumbar spine and the femur of the upper leg, based on X-ray images. The advance is described in a study published in the Journal of Orthopaedic Research.
A total of 1454 X-ray images were analysed using the scientists’ system. Performance rates for the lumbar and femur of patients with bone density loss, or osteopenia, were 86.4% and 84.1%, respectively, in terms of sensitivity. The respective specificities were 80.4% and 76.3%. (Sensitivity reflected the ability of the test to correctly identify people with osteopenia, whereas specificity reflected its ability to correctly identify those without osteopenia). The test also had high sensitivity and specificity for categorising patients with and without osteoporosis.
“Bone mineral density measurement is essential for screening and diagnosing osteoporosis, but limited access to diagnostic equipment means that millions of people worldwide may remain undiagnosed,” said corresponding author Toru Moro, MD, PhD, of the University of Tokyo. “This AI system has the potential to transform routine clinical X-rays into a powerful tool for opportunistic screening, enabling earlier, broader, and more efficient detection of osteoporosis.”
Dementia poses a major health challenge with no safe, affordable treatments to slow its progression. Researchers at Lawson Research Institute (Lawson), the research arm of St. Joseph’s Health Care London, are investigating whether Ambroxol – a cough medicine used safely for decades in Europe – can slow dementia in people with Parkinson’s disease.
Published in JAMA Neurology, this 12-month clinical trial involving 55 participants with Parkinson’s disease dementia (PDD) monitored memory, psychiatric symptoms and GFAP, a blood marker linked to brain damage.
Parkinson’s disease dementia causes memory loss, confusion, hallucinations and mood changes. About half of those diagnosed with Parkinson’s develop dementia within 10 years, profoundly affecting patients, families and the health care system.
Led by Cognitive Neurologist Dr Stephen Pasternak, the study gave one group daily Ambroxol while the other group received a placebo.
“Our goal was to change the course of Parkinson’s dementia,” says Pasternak. “This early trial offers hope and provides a strong foundation for larger studies.”
Key findings from the clinical trial include:
Ambroxol was safe, well-tolerated and reached therapeutic levels in the brain.
Psychiatric symptoms worsened in the placebo group but remained stable in those taking Ambroxol.
Participants with high-risk GBA1 gene variants showed improved cognitive performance on Ambroxol.
A marker of brain cell damage (GFAP) increased in the placebo group but stayed stable with Ambroxol, suggesting potential brain protection.
Although Ambroxol is approved in Europe for treating respiratory conditions and has a long-standing safety record – including use at high doses and during pregnancy – it is not approved for any use in Canada or the U.S.
“Current therapies for Parkinson’s disease and dementia address symptoms but do not stop the underlying disease,” explains Pasternak. “These findings suggest Ambroxol may protect brain function, especially in those genetically at risk. It offers a promising new treatment avenue where few currently exist.”
An old drug with new possibilities
Ambroxol supports a key enzyme called glucocerebrosidase (GCase), which is produced by the GBA1 gene. In people with Parkinson’s disease, GCase levels are often low. When this enzyme doesn’t work properly, waste builds up in brain cells, leading to damage.
Pasternak learned about Ambroxol during a fellowship at The Hospital for Sick Children (SickKids) in Toronto, where it was identified as a treatment for Gaucher disease – a rare genetic disorder in children caused by a deficiency of GCase. He is now applying that research to explore whether boosting GCase with Ambroxol could help protect the brain in Parkinson’s related diseases.
“This research is vital because Parkinson’s dementia profoundly affects patients and families,” says Pasternak. “If a drug like Ambroxol can help, it could offer real hope and improve lives.”
Funded by the Weston Family Foundation, this study is an important step toward developing new treatments for Parkinson’s disease and other cognitive disorders, including dementia with Lewy bodies. Pasternak and his team plan to start a follow-up clinical trial focused specifically on cognition later this year.
During South Africa’s COVID-19 hard lockdown, Dr Sandile Cele became the first to successfully grow the beta variant of SARS-CoV-2 in the lab. PHOTO: Rosetta Msimango/Spotlight
In a Durban laboratory in 2020, there was dancing and scientists jumping with joy when Dr Sandile Cele realised they had finally successfully “grown” the SARS-CoV-2 Beta variant. It was the holiday season and Cele and a few colleagues had sacrificed their Christmas to continue research at an otherwise deserted laboratory.
The Beta variant (501Y.V2) was first detected in the Eastern Cape in October 2020 and was announced to the public on 18 December that year.
“It was December 2020 and Tulio [Professor Tulio de Oliveira] had just flagged the beta variant and we had been struggling trying to grow it, really struggling for about two weeks,” says Cele. “But then as a scientist, you have to think outside the box and eventually it [the virus] did catch on. I was with Professor Alex Sigal that day in the laboratory. We were so excited. There was a lot of dancing in the lab, jumping up and down…”
The 35-year-old’s work on the Beta and Omicron variants helped propel South Africa to the forefront of COVID-19 research. Cele is the scientist credited with growing both Beta and Omicron in record time as the world reeled under lockdown pressure. Last year, he was awarded a special ministerial Batho Pele excellence award for his contribution to COVID-19 research in South Africa.
The moment of greatest fulfilment
Speaking to Spotlight, Cele says growing the beta variant was the moment of greatest fulfilment in his career so far.
“It was just a crazy, crazy moment. Like, you know when you are with your superior, usually you meet on a basis of respect. I mean, you talk seriously. They ask a question, you answer, and so on. But [at] that moment, all that got thrown out the window. We were celebrating. So yes, it was really special.”
At the time, they were leaping with joy inside PPE (personal protective equipment), including specialised masks, double gloves, plastic sleeves, and boots. Cele points out that due to all the safety measures in place, infection risk was smaller in their lab than at an average mall.
He was working inside a state-of-the-art biosafety level 3 (BSL-3) laboratory at the Africa Health Research Institute (AHRI). The laboratory is on the third floor of the University of KwaZulu-Natal’s medicine building. In the same eight-storey glass and face brick building, on the first floor, de Oliveira had been studying virus samples for genetic clues at KRISP, the KwaZulu-Natal Research and Innovation Sequencing Platform, from where the discovery of Beta and Omicron was first announced.
How he did it – growing the beta variant
Cele explains that viruses are isolated or “outgrown” by infecting cells in the laboratory, using swab samples from infected individuals.
“Growing a virus simply means isolating it from an infected host (humans) and making more of it in the lab for research purposes,” Cele explains. “You cannot study a virus within an infected person, especially a new virus. You need to have it in the lab for identification and clarification. Usually, you get small quantities from an infected person, thus you have to expand or grow – or make more of it – for research.”
Photo by Shvets Production on Pexels
However, the beta variant had not responded like previous SARS-CoV-2 variants. At the time, Cele found a creative solution using both human and monkey cell lines. First, he infected human cell lines with the beta variant, incubating the assay for four days. Then he used the infected human cell lines to infect monkey cell lines, which successfully lead to production of the virus.
Their moment of triumph arrived when they noticed the monkey cell lines starting to die, meaning that the virus was growing. The isolated virus could then be used in the laboratory to run experiments, like testing vaccine efficacy.
“Looking at the cells under the microscope, you can see them starting to die,” he says. “That they’re not happy. That they have been infected, which then obviously needed to be confirmed.”
While Cele’s Durban mentors – de Oliveira and Sigal – kept the public abreast of research developments, the young scientist kept his head down, pouring over his microscopes. “The world was going crazy, everything was crazy, but I had work to do,” he says.
‘a rising star’
During the interview, Cele readily shares anecdotes and laughs often.
From Ndwedwe, a rural area forty kilometres north of Durban, Cele joined Sigal’s laboratory team at the AHRI in 2014, where he studied HIV drug resistance and later COVID-19. His PhD obtained from UKZN in 2021, focused specifically on understanding the beta variant and its escape from antibodies.
“Actually, Professor Alex Sigal really took a chance on me,” he says. “Because on that post for a laboratory technologist, they stipulated that they wanted someone with three years experience. And I had only been doing my internship [at the Technology Innovation Agency] for eight months.”
But Sigal’s faith paid off, and he subsequently praised Cele in national press interviews on COVID-19. “Sandile is a rising star who spent all his holidays in a laboratory,” Sigal told journalists in January 2021.
Last year, the Bill and Melinda Gates Foundation invited Cele to present his findings at the Grand Challenges Annual Meeting in Brussels. This was his first time abroad. “It was my first time traveling outside South Africa and my first time talking in front of so many people. I presented my go-to talk – based on a paper I did on COVID-infection and HIV – and it went well,” he says.
Earlier this year, Cele was named one of Mail & Guardian’s 200 trailblazing young South Africans in the technology and innovation category. At the time, he could not attend the gala event as he was at the University of Nairobi in Kenya for training relating to a project involving HIV research for the Aurum Institute. Cele started a new job at the Aurum Institute in Johannesburg in March.
Over Zoom, Cele is speaking from his new home in Johannesburg. He is wearing a fluffy blue robe over his clothes, laughing as he says how cold Johannesburg is coming from Durban.
A sudden death
In Ndwedwe, Cele was one of ten boys born to his father, who was away from home often for work. Describing his mother as “a busy lady”, Cele says she was the one who shaped his young everyday life. Growing up in a mud hut without electricity and running water, he recalls how his mother would get up early every morning to prepare vetkoek, which she sold at a local school, and to boil water so her children could have a bath before leaving for school.
In the afternoons, he would look after his father’s goats and play soccer. He says that as a child he preferred herding goats to cows, as goats grazed for only about five hours, whereas cows took all day to eat their fill. From Grade 9 on, he attended school in Durban, at Overport Secondary School.
A childhood memory that inspired him? “Before my mother died, she sat us down and said one day I will be gone and I want you to know there are no shortcuts in life. Work hard and look after one another and you will be okay.”
His mother’s death was sudden, following complications from minor surgery.
“Like, I came back from school on a Friday only to find my father wasn’t around and had left a note… On the Saturday morning, I found out my mother had passed. And I think she went for, I don’t know, an operation or something. But as a kid, I guess they didn’t tell us because they thought it was something minor; that she would get operated [on], then go back home. I’m not really sure what happened. So, yes, it was a sudden death.”
The year after his mother died, Cele’s matric marks suffered. He says his final grade 12 marks had been 48% for maths, 53% for physics, and 66% for biology.
“I wasn’t really studying, I couldn’t really concentrate,” he says. “There was a lot going on when I was doing my matric. My mother passing away… and also the move from a rural school to the city where we were taught in English, everything in English.”
Cele came to study biology quite at random. He applied to study at UKZN only in October of his matric year – with admissions to most of the university’s courses having closed the previous month. He picked one of the last remaining options, which had been biology.
Soon, the young student started excelling. Cele obtained his BSc Biomedical Sciences degree with a Dean’s commendation and his Honours in Medical Microbiology, summa cum laude. He completed his Masters in Biochemistry with an upper-class pass.
To the Mail and Guardian, he shared advice he would give to his younger self: “Do not be afraid, you are a force to be reckoned with.”
Cele’s driving passion is to advance public healthcare, which he will continue to do at the Aurum Institute – an organisation that amongst others does research into Africa’s tuberculosis and HIV response. Cele has a ten-year-old son who lives in Durban.
Note:The Bill and Melinda Gates Foundation is mentioned in this article. Spotlight receives funding from the foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Detail from Small’s reprocessed cryo-EM data zooming in on an unoccupied area of the SARS-CoV-2 NiRAN domain. (Courtesy of Campbell lab)
The COVID pandemic illustrated how urgently we need antiviral medications capable of treating coronavirus infections. To aid this effort, researchers quickly homed in on part of SARS-Cov-2’s molecular structure known as the NiRAN domain – an enzyme region essential to viral replication that’s common to many coronaviruses. A drug targeting the NiRAN domain would likely work broadly to shut down a range of these pathogens, potentially treating known diseases like COVID as well as helping to head off future pandemics caused by related viruses.
In 2022, scientists (Yan et. al.) published a structural model describing exactly how this domain works. It should have been a tremendous boon for drug developers.
But the model was wrong.
“Their work contains critical errors,” says Gabriel Small, a graduate fellow in the laboratories of Seth A. Darst and Elizabeth Campbell at Rockefeller. “The data does not support their conclusions.”
Now, in a new study published in Cell, Small and colleagues demonstrate exactly why scientists still don’t know how the NiRAN domain works. The findings could have sweeping implications for drug developers already working to design antivirals based on flawed assumptions, and underscore the importance of rigorous validation.
“It is absolutely important that structures be accurate for medicinal chemistry, especially when we’re talking about a critical target for antivirals that is the subject of such intense interest in industry,” says Campbell, head of the Laboratory of Molecular Pathogenesis. “We hope that our work will prevent developers from futilely trying to optimise a drug around an incorrect structure.”
A promising lead
By the time the original paper was published in Cell, the Campbell and Darst labs were already quite familiar with the NiRAN domain and its importance as a therapeutic target. Both laboratories study gene expression in pathogens, and their work on SARS-CoV-2 focuses in part on characterizing the molecular interactions that coordinate viral replication.
The NiRAN domain is essential for helping SARS-CoV-2 and other coronaviruses cap their RNA, a step that allows these viruses to replicate and survive. In one version of this process, the NiRAN domain uses a molecule called GDP to attach a protective cap to the beginning of the virus’s RNA. Small previously described that process in detail, and its structure is considered solved. But the NiRAN domain can also use a related molecule, GTP, to form a protective cap. Determined to develop antivirals that comprehensively shut down the NiRAN domain, scientists were keen to discover the particulars of the latter GTP-related mechanism.
In the 2022 paper, researchers described a chain of chemical steps, beginning with a water molecule breaking a bond to release the RNA’s 5′ phosphate end. That end then attaches to the beta-phosphate end of the GTP molecule, which removes another phosphate and, with the help of a magnesium ion, transfers the remaining portion of the GTP molecule to the RNA, forming a protective cap that allows the virus to replicate and thrive.
The team’s evidence? A cryo-electron microscopy image that showed the process caught in action. To freeze this catalytic intermediate, the team used a GTP mimic called GMPPNP.
Small read the paper with interest. “As soon as they published, I went to download their data,” he says. It wasn’t there. This raised a red flag—data is generally available upon release of a structural biology paper. Months later, however, when Small was finally able to access the data, he began to uncover significant flaws. “I tried to make a figure using their data, and realized that there were serious issues,” he says. Small brought his concerns to Campbell and Darst.
They agreed. “Something was clearly wrong,” Campbell says. “But we decided to give the other team the benefit of the doubt, and reprocess all of their data ourselves.”
An uphill battle
It was painstaking work, with Small leading the charge. Working frame by frame, he compared the published atomic model to the actual cryo-EM map and found something striking: the key molecules that Yan and colleagues claimed to have seen, specifically, the GTP mimic GMPPNP and a magnesium ion in the NiRAN domain’s active site, simply were not there.
Not only was there no supporting image data, but the placement of these molecules in the original model also violated basic rules of chemistry, causing severe atomic clashes and unrealistic charge interactions. Small ran additional tests, but even advanced methods designed to pick out rare particles turned up empty. He could find no evidence to support the model previously produced by Yan and colleagues.
Once the Rockefeller researchers validated their results, they submitted their findings to Cell. “It was very important that we publish our corrective manuscript in the same journal that published the original model,” Campbell says, noting that corrections to high-profile papers are often overlooked when published in lower tier journals.
Otherwise, this confusion in the field could cause problems that reach far beyond the lab bench, Campbell adds – a costly reminder that rigorous basic biomedical research is not just academic, but essential to real-world progress. “Companies keep their cards close to their chests, but we know that several industry groups are studying this,” she says. “Efforts based on a flawed structural model could result in years of wasted time and resources.”