
Drug Combo Cuts Risk of Death in Advanced Prostate Cancer by 40%
Cedars-Sinai Led Clinical trial showed combo treatment reduced deaths in patients with an aggressive form of the disease

Men whose prostate cancer returns after surgery or radiation therapy may now benefit from a new drug combination shown in clinical trials to cut the risk of death by more than 40%.
The combination therapy, which adds the drug enzalutamide to commonly prescribed hormone therapy, reduced deaths in patients with recurrent prostate cancer after surgery or radiation for whom other treatments are no longer an option. The trial results were published in The New England Journal of Medicine (NEJM) with simultaneous presentation during the European Society for Medical Oncology Congress (ESMO) Oct. 19 in Berlin.
“After initial treatment, some patients see their prostate cancer come back in an aggressive way and are at risk for their disease to spread quickly,” said Stephen Freedland, MD, director of the Center for Integrated Research in Cancer and Lifestyle at Cedars-Sinai Cancer and co-principal investigator of the study. “Hormone therapy, which is what we’ve been offering patients for 30 years, has not improved survival and neither has anything else. That makes these findings a real game changer.”
The trial included more than 1000 patients from 244 sites in 17 countries. All the patients were diagnosed with what is known as high-risk biochemically recurrent prostate cancer. Following the patients’ surgery or radiation therapy, the levels of prostate specific antigen, or PSA, in their blood had risen rapidly. PSA is a protein used to detect prostate cancer, and a rapid rise in PSA levels after treatment indicates a patient’s cancer is likely to return and metastasise, often to the bones or spine.
“We know these patients are at high risk of developing metastatic disease and dying of their cancer unless we offer a meaningful treatment option,” said Freedland, professor of Urology and the Warschaw, Robertson, Law Families Chair in Prostate Cancer.
Patients were randomly selected to receive standard hormone therapy alone, enzalutamide alone, or a combination of the two. After eight years, the risk of death was 40.3% lower in the combination group than in the other two groups, Freedland said.
“This clinical trial, one of many that Cedars-Sinai Cancer has offered to its patients, is an example of the translational work being done by our physician-scientists,” said Robert Figlin, MD, interim director of Cedars-Sinai Cancer. “The result will be improved treatment and better outcomes for patients everywhere.”
Freedland noted that, based on previous results published by the team, enzalutamide is approved by the Food and Drug Administration and listed in National Comprehensive Cancer Network treatment guidelines. These latest results, he said, are likely to strengthen the network’s recommendation and solidify this drug combination as the standard of care for patients with high-risk biochemically recurrent prostate cancer.
“These important findings identify a treatment that prolongs survival in men with aggressive prostate cancer,” said Hyung Kim, MD, a urologic oncologist and chair of the Department of Urology at Cedars-Sinai. “The latest analysis complements previous studies that found enzalutamide significantly improved survival in other prostate cancer settings, and will change how we take care of our patients.”
Source: Cedars-Sinai Medical Center

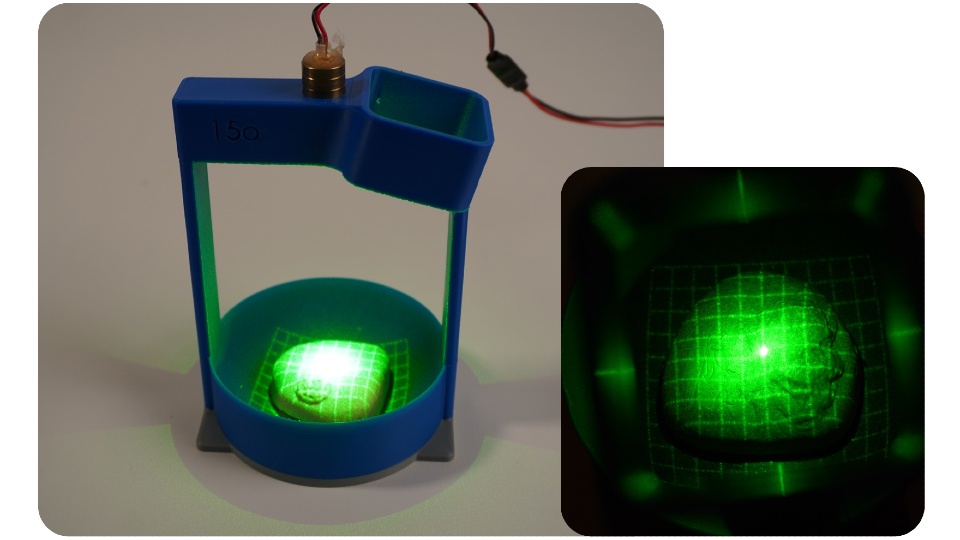 PRO check prototype one demonstrated how laser gridlines and a camera can be used to image the surface of the prostate.
PRO check prototype one demonstrated how laser gridlines and a camera can be used to image the surface of the prostate.


