Glycopeptide probes detect tumour-associated antibodies in blood samples
Pancreatic cancer. Credit: Scientific Animations CC BY-SA 4.0
Pancreatic cancer is one of the most lethal forms of cancer, primarily because it is usually diagnosed very late. Current markers are too insensitive and unspecific for early detection screenings. In the journal Angewandte Chemie, a research team has now introduced a new method that could lead to a significantly more precise and reliable diagnosis. It is based on the selective detection of specific antibodies in blood samples.
Tumours produce certain proteins (tumour-associated antigens) that draw the attention of our constantly “patrolling” immune system and trigger an immune response. As a consequence, antibodies directed against the tumours (tumour-associated autoantibodies) are formed, circulating in the blood at very early stages of the disease – which makes them useful for early detection. An international team led by Roberto Fiammengo and Giovanni Malerba at the University of Verona (Italy) as well as Alfredo Martínez at the Center for Biomedical Research of La Rioja (Logroño, Spain) and Francisco Corzana at the Universidad de La Rioja, has now developed an approach to diagnostic testing for pancreatic cancer that is based on the detection of such special tumour-associated autoantibodies.
They chose to use autoantibodies directed against the tumour-associated form of mucin-1 (TA-MUC1). Mucin-1 is a heavily glycosylated protein (a protein with sugar components) that occurs, for example, in glandular tissue. In many types of tumours, including pancreatic cancer, it is found in significantly elevated concentrations. In addition, the pattern of glycosylation is different from the normal form. The team’s goal was to detect autoantibodies that are directed specifically against TA-MUC1 and are a clear indicator of pancreatic cancer.
Based on structural analyses and computer simulations of known antibodies against TA-MUC1 (SM3 and 5E5), the team designed a collection of synthetic glycopeptides that mimic different segments (epitopes) of TA-MUC1. They also made unnatural modifications to increase the chances of identifying autoantibody subgroups indicative of the disease. The team immobilised these model antigens on gold nanoparticles achieving probes suitable for a serological assay (dot-blot assay). The diagnostic assay was validated with real samples from patients with pancreatic cancer and a healthy control group. Some of the nanoparticle probes could differentiate very well between samples from diseased and healthy individuals demonstrating they detected tumour associated autoantibodies. Notably, these specific autoantibodies displayed significantly better correct positive/false positive ratios than current clinical biomarkers for pancreatic cancer.
Probes with smaller glycopeptide antigens that correspond to only a single epitope, gave better results than larger probes that mimic multiple epitopes – an advantage for easier synthetic production. A short glycopeptide with an unnatural modification to its sugar component was found to be particularly effective for the detection of discriminating autoantibodies. This new structure-based approach could help in the selection of autoantibody subgroups with higher tumour specificity.
Risk of cancer by specific site based on blood test abnormalities in symptomatic patients can help guide referral strategies
Photo by National Cancer Institute on Unsplash
Incorporating information from common blood tests can enhance cancer risk assessment in patients with abdominal symptoms, according to a study publishing July 30th in the open-access journal PLOS Medicineby Meena Rafiq from University College London, UK, and colleagues.
Early cancer detection is key to successful treatment. However, many undiagnosed cancer patients present to their primary care provider with non-specific symptoms that can be a result of several other benign causes, making it difficult to determine who warrants additional diagnostic testing or referral. Most guidelines focus on “alarm” symptoms specific to a given type of cancer to guide referrals. There is limited guidance on non-specific symptoms to guide cancer assessment and referral decisions across different cancer types.
In this study, researchers used data from the UK Clinical Practice Research Datalink to identify more than 470 000 patients aged 30 years or older who had visited a general practitioner due to abdominal pain or bloating. Within a year of that visit, approximately 9000 patients with abdominal pain and 1000 patients with bloating were diagnosed with cancer. The researchers looked at 19 abnormal blood test results collected during the initial primary care visit to see if they could predict who was more likely to be diagnosed with cancer.
Several blood abnormalities were predictive of cancer risk across sex and age groups. For example, in patients aged 30–59 years with abdominal symptoms, anaemia, low albumin, raised platelets, abnormal ferritin, and increased inflammatory markers strongly predicted a risk of undiagnosed cancer. Among older patients (aged 60 years and above), the presence of abdominal pain or bloating alone was enough to warrant a cancer referral.
The study also showed which types of cancer were most common based on age, sex, and blood test abnormality. For example, among women aged 50–59 years with anaemia and abdominal bloating, the most common types of cancer were bowel and ovarian cancer. This level of granularity can help guide providers on which diagnostic strategies to prioritise.
The study shows that common, routine blood test results can provide additional context in patients with non-specific abdominal symptoms to improve cancer risk assessment and identify patients who warrant additional testing and/or referral to a specialist.
The authors add, “Using existing blood tests can be an effective and affordable way to improve early diagnosis of cancer in people who see their GP with vague symptoms. Our study identified several commonly used GP blood tests where abnormal results increase a patient’s risk of having cancer and these can be used to diagnose cancer earlier.”
The Stockholm3 blood test, developed by researchers at Karolinska Institutet, is equally effective at detecting prostate cancer in different ethnic groups, according to a new paper published in The Journal of Clinical Oncology. The test produces significantly better results than the current PSA standard.
Stockholm3, a prostate cancer test developed in Sweden, runs a combination of protein and genetic markers from a blood sample through an algorithm to find the probability of a patient having clinically significant cancer.
Studies in more than 90 000 men have shown that Stockholm3 produces significantly better results than the current PSA standard. The test improves prostate cancer diagnosis by reducing unnecessary MRI and biopsies and by identifying significant cancers in men with low or normal PSA values.
Ethnically diverse group
However, previous studies have been conducted primarily in Scandinavia on a mainly White population with uncertain generalisability to the rest of the world. A Swedish-American research group has now examined how well it works in an ethnically mixed group of men in the USA and Canada.
The study included over 2000 men at 17 different clinics, 16% of whom were Asian, 24% African-American, 14% Latin American and 46% White American. All participants had a referral for a prostate biopsy on the basis of an elevated PSA score, abnormal rectal examination, MRI scan or other suspicious clinical finding.
Before the biopsy was performed, a blood test was taken along with clinical data pertinent to the Stockholm3 test, which was conducted blinded to the biopsy results.
Halving the number of unnecessary biopsies
The analysis shows that clinically relevant prostate cancer cases were found in a total of 29% of the men, somewhat more in African Americans and slightly fewer in Asians.
It also shows that the Stockholm3 test could almost halve the number of unnecessary biopsies (45 per cent fewer: 673 as opposed to 1226) while being no less effective at detecting all clinically relevant cases. The results were similar across the different ethnic groups.
“The study demonstrates that the Stockholm3 test is just as effective on an ethnically mixed group as it is on a White, Swedish population,” says the study’s lead author Hari T. Vigneswaran, doctor and PhD student at the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet.
According to him, the research answers several important questions and will lead to a more widespread use of the method:
“Colleagues in other countries are very interested in these data, which show that Stockholm3 works for a non-Swedish population and among minorities.”
Dr Ali Bashashati observes an endometrial cancer sample on a microscope slide. Credit: University of British Columbia
A discovery by researchers at the University of British Columbia promises to improve care for patients with endometrial cancer, the most common gynaecologic malignancy. Using artificial intelligence (AI) to spot patterns across thousands of cancer cell images, the researchers have pinpointed a distinct subset of more stubborn endometrial cancer that would otherwise go unrecognised by traditional pathology and molecular diagnostics.
The findings, published in Nature Communications, will help doctors identify patients with high-risk disease who could benefit from more comprehensive treatment.
“Endometrial cancer is a diverse disease, with some patients much more likely to see their cancer return than others,” said Dr Jessica McAlpine, professor at UBC. “It’s so important that patients with high-risk disease are identified so we can intervene and hopefully prevent recurrence. This AI-based approach will help ensure no patient misses an opportunity for potentially lifesaving interventions.”
AI-powered precision medicine
The discovery builds on work by Dr McAlpine and colleagues in the Gynaecologic Cancer Initiative, who in 2013 helped show that endometrial cancer can be classified into four subtypes based on the molecular characteristics of cancerous cells, with each posing a different level of risk to patients.
Dr McAlpine and team then went on to develop an innovative molecular diagnostic tool, called ProMiSE, that can accurately discern between the subtypes. The tool is now used across parts of Canada and internationally to guide treatment decisions.
Yet, challenges remain. The most prevalent molecular subtype, encompassing approximately 50% of all cases, is largely a catch-all category for endometrial cancers lacking discernible molecular features.
“There are patients in this very large category who have extremely good outcomes, and others whose cancer outcomes are highly unfavourable. But until now, we have lacked the tools to identify those at-risk so that we can offer them appropriate treatment,” said Dr McAlpine.
Dr McAlpine turned to long-time collaborator and machine learning expert Dr.Ali Bashashati, an assistant professor of biomedical engineering and pathology and laboratory medicine at UBC, to try and further segment the category using advanced AI methods.
Dr Bashashati and his team developed a deep learning AI model that analyses images of tissue samples collected from patients. The AI was trained to differentiate between different subtypes, and after analysing over 2300 cancer tissue images, pinpointed the new subgroup that exhibited markedly inferior survival rates.
“The power of AI is that it can objectively look at large sets of images and identify patterns that elude human pathologists,” said Dr Bashashati. “It’s finding the needle in the haystack. It tells us this group of cancers with these characteristics are the worst offenders and represent a higher risk for patients.”
Bringing the discovery to patients
The team is now exploring how the AI tool could be integrated into clinical practice alongside traditional molecular and pathology diagnostics.
“The two work hand-in-hand, with AI providing an additional layer on top of the testing we’re already doing,” said Dr McAlpine.
One benefit of the AI-based approach is that it’s cost-efficient and easy to deploy across geographies. The AI analyses images that are routinely gathered by pathologists and healthcare providers, even at smaller hospital sites in rural and remote communities, and shared when seeking second opinions on a diagnosis.
The combined use of molecular and AI-based analysis could allow many patients to remain in their home communities for less intensive surgery, while ensuring those who need treatment at a larger cancer centre can do so.
“What is really compelling to us is the opportunity for greater equity and access,” said Dr Bashashati. “The AI doesn’t care if you’re in a large urban centre or rural community, it would just be available, so our hope is that this could really transform how we diagnose and treat endometrial cancer for patients everywhere.”
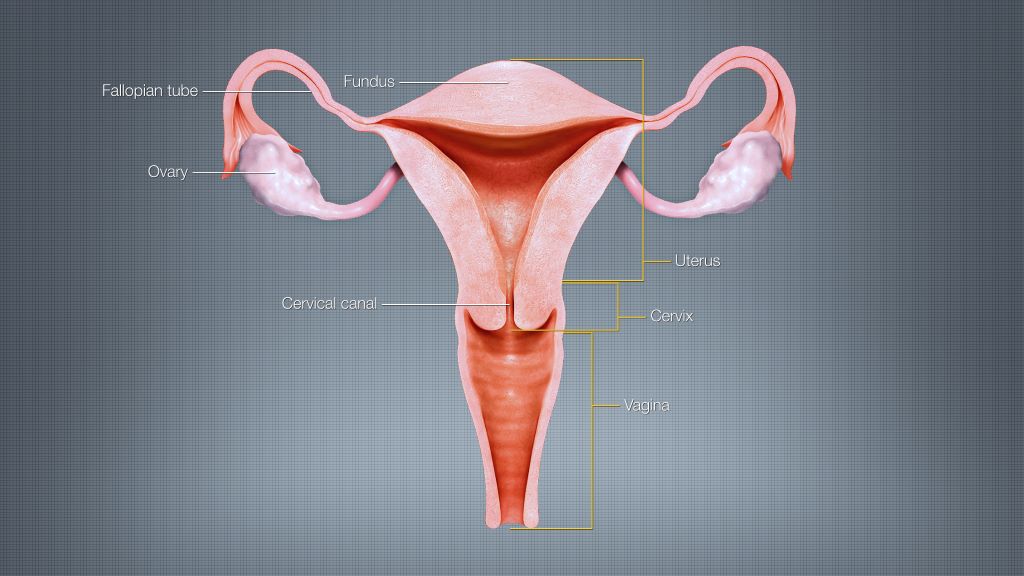
Researchers have developed a simpler and more effective screening method for cervical cancer than the method used today. A comprehensive study published in Nature Medicine shows that the test detects significantly more cancers and precancerous stages.
Most countries have a very extensive cervical cancer screening program that starts with testing for different variants of the human papillomavirus (HPV) that causes cervical cancer. In the case of an HPV-positive test, this is followed by cytological analysis, the examination of gynaecological cell samples by microscopy, which is dependent on human interpretation.
The new molecular test WID-qCIN, which could replace the cytological analysis, can automatically analyse epigenetic changes in cells. These changes, where genes are switched on or off, are influenced by factors such as environment, lifestyle, and aging, and can increase the risk of cancer and other diseases.
Fewer invasive procedures
The current study by researchers at Karolinska Institutet and the University of Innsbruck included more than 28 000 women over the age of 30 who underwent screening in Stockholm between January and March 2017. The researchers analysed a total of 2377 HPV-positive samples with the WID-qCIN test combined with a test for two high-risk HPV types (HPV 16 and 18). In this way, they were able to detect 100% of all invasive cervical cancer and 93% of all serious precancerous lesions that occurred within a year of sampling.
In addition, the new test, in combination with the HPV 16/18 test, was able to predict 69% of all cancers and precancerous lesions up to six years after the sample was taken. This can be compared with only 18% with today’s screening method.
“By integrating the WID-qCIN test into our screening programs, we would be able to identify more cancer cases while reducing the need for invasive procedures,” says Joakim Dillner, Professor of Infectious Disease Epidemiology at Karolinska Institutet and co-author of the study.
A significant improvement
When cell changes are detected in today’s screening program, the woman undergoes a vaginal examination, a so-called colposcopy, where the gynaecologist looks at the cervix with the help of a microscope and, if necessary, takes a biopsy. The biopsy involves a surgical procedure that, among other things, can lead to negative pregnancy outcomes like premature delivery. The results of the current study suggest that implementation of the WID-qCIN test could reduce the number of colposcopy examinations by 40%.
“This would mean a significant improvement compared to today’s screening methods, which were introduced in the 1960s,” says the study’s last author Martin Widschwendter, Professor at the University of Innsbruck (Austria) and visiting Professor at Karolinska Institutet. “With its simplicity and objective assessment, the WID-qCIN test can improve the effectiveness of these programs and support the global strategy to eliminate cervical cancer.”
A breakthrough study published in The American Journal of Pathology describes a new machine-learning model that may improve accuracy in early diagnosis of hepatocellular carcinoma and monitoring the impact of treatment.
Early diagnosis of hepatocellular carcinoma (HCC) – one of the most fatal malignancies – is crucial to improve patient survival. In this breakthrough study, investigators report on the development of a serum fusion-gene machine-learning model. This important screening tool may increase the five-year survival rate of patients with HCC from 20% to 90% because of its improved accuracy in early diagnosis of HCC and monitoring the impact of treatment.
HCC is the most common form of liver cancer and accounts for around 90% of cases. Currently, the most common screening test for the HCC biomarker, serum alpha-foetal protein, is not always accurate, and up to 60% of liver cancers are only diagnosed in advanced stages, resulting in a survival rate of only around 20%.
Lead investigator Jian-Hua Luo, MD, PhD, Department of Pathology, High Throughput Genome Center, and Pittsburgh Liver Research Center, University of Pittsburgh School of Medicine, explained: “Early diagnosis of liver cancer helps save lives. However, most liver cancers occur insidiously and without many symptoms. This makes early diagnosis challenging. What we need is a cost-effective, accurate, and convenient test to screen early-stage liver cancer in human populations. We wanted to explore if a machine-learning approach could be used to increase the accuracy of screening for HCC based on the status of the fusion genes.”
In the search for a more effective and efficient diagnostic tool to predict non-HCC and HCC cases, investigators analysed a panel of nine fusion transcripts in serum samples from 61 patients with HCC and 75 patients with non-HCC conditions using real-time quantitative reverse transcription PCR (RT-PCR). Seven of the nine fusions were frequently detected in HCC patients. The researchers generated machine-learning models based on serum fusion-gene levels to predict HCC in the training cohort, using the leave-one-out cross-validation approach.
A four fusion gene logistic regression model produced an accuracy of 83% to 91% in predicting the occurrence of HCC. When combined with serum alpha-foetal protein, the two-fusion gene plus alpha-foetal protein logistic regression model produced 95% accuracy for all the cohorts. Furthermore, quantification of fusion gene transcripts in the serum samples accurately assessed the impact of the treatment and was able to monitor for the recurrence of the cancer.
Dr. Luo commented, “The fusion gene machine-learning model significantly improves the early detection rate of HCC over the serum alpha-fetal protein alone. It may serve as an important tool in screening for HCC and in monitoring the impact of HCC treatment. This test will find patients who are likely to have HCC.”
Dr. Luo concluded, “Early treatment of liver cancer has a 90% five-year survival rate, while late treatment has only 20%. The alternative to this test is to subject every individual with some risk of liver cancer to imaging analysis every six months, which is very costly and ineffective. In addition, when imaging results are ambiguous, this test will help to differentiate malignant versus benign lesions.”
Melanoma is often detected later in people with darker skin complexions – and the consequences can be devastating, according to the results of a Mayo Clinic study published in the Journal of Surgical Oncology.
While melanoma may be found less frequently in people with darker complexions than fair ones, this aggressive form of skin cancer, accounting for 75% of all skin-cancer-related deaths, can strike anyone. The study, which consisted of 492 597 patients with melanoma, suggests that added vigilance in early screening is particularly needed for Black men, whose cancers are often found at later stages, leading to worse outcomes compared to white patients or Black women.
“We compared non-Hispanic Black patients to white patients and saw striking differences in how patients presented with the disease,” says surgical oncologist Tina Hieken, MD, senior author of the study and a researcher at Mayo Clinic Comprehensive Cancer Center. “We saw more extremity melanoma, and more later-stage disease.”
Extremity melanoma refers to skin cancer that can develop on the arms, legs, hands and feet. Various factors, including social risk factors and biological components, could be at play, but further research is needed to help determine why these differences exist.
Revealing differences in sex-based immune response
The research found that Black female patients with melanoma fared better than Black male patients. Men tended to be older at diagnosis and more likely to have cancer that had spread to their lymph nodes compared to women. This translated to worse survival rates: the five-year survival for Black men with stage 3 melanoma was only 42% chance, compared to 71% for Black women.
Most research on melanoma hasn’t focused on how race and sex affect outcomes and hasn’t looked at the influence of race and ethnicity across all groups. Dr Hieken says the study highlights the need to understand these differences better, noting that this is the first large study to confirm that sex-based differences in melanoma outcomes exist within the non-Hispanic Black population.
“When we talk about later-stage melanoma patients who are female versus male in that non-Hispanic Black patient cohort who ended up doing worse, some biological things may be going on here that are interesting,” says Dr Hieken.
One theory centres on variations in immune response.
“Several immune signals suggest that women may respond better to some immunotherapies than males,” says Dr Hieken.
Researchers note that more studies focused on melanoma in a broader range of people, including more Black participants in clinical trials, is key to bridging this knowledge gap and potentially identifying more effective treatments.
Healthcare professionals should screen carefully
Dr Hieken notes that this study is a wake-up call for everyone battling to diagnose and cure melanoma, regardless of the patient’s sex or skin tone.
She emphasises that healthcare professionals should carefully examine areas like palms, soles and under fingernails, where melanoma might be more challenging to spot on darker skin.
“We can incorporate screening for skin lesions or lesions under the nails into the visit for patients as part of their regular checkups,” says Dr Hieken. “What we want to do is elevate care for our patients.”
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
A mobile app that uses artificial intelligence, AI, to analyse images of suspected skin lesions can diagnose melanoma with very high precision. This is shown in a study led from Linköping University in Sweden where the app has been tested in primary care. The results have been published in the British Journal of Dermatology.
“Our study is the first in the world to test an AI-based mobile app for melanoma in primary care in this way. A great many studies have been done on previously collected images of skin lesions and those studies relatively agree that AI is good at distinguishing dangerous from harmless ones. We were quite surprised by the fact that no one had done a study on primary care patients,” says Magnus Falk, senior associate professor at the Department of Health, Medicine and Caring Sciences at Linköping University, specialist in general practice at Region Östergötland, who led the current study.
Melanoma can be difficult to differentiate from other skin changes, even for experienced physicians. However, it is important to detect melanoma as early as possible, as it is a serious type of skin cancer.
There is currently no established AI-based support for assessing skin lesions in Swedish healthcare.
“Primary care physicians encounter many skin lesions every day and with limited resources need to make decisions about treatment in cases of suspected skin melanoma. This often results in an abundance of referrals to specialists or the removal of skin lesions, which in the majority of cases turn out to be harmless. We wanted to see if the AI support tool in the app could perform better than primary care physicians when it comes to identifying pigmented skin lesions as dangerous or not, in comparison with the final diagnosis,” says Panos Papachristou, researcher affiliated with Karolinska Institutet and specialist in general practice, main author of the study and co-founder of the company that developed the app.
And the results are promising.
“First of all, the app missed no melanoma. This disease is so dangerous that it’s essential not to miss it. But it’s almost equally important that the AI decision support tool could acquit many suspected skin lesions and determine that they were harmless,” says Magnus Falk.
In the study, primary care physicians followed the usual procedure for diagnosing suspected skin tumours. If the physicians suspected melanoma, they either referred the patient to a dermatologist for diagnosis, or the skin lesion was cut away for tissue analysis and diagnosis.
Only after the physician decided how to handle the suspected melanoma did they use the AI-based app. This involves the physician taking a picture of the skin lesion with a mobile phone equipped with an enlargement lens called a dermatoscope. The app analyses the image and provides guidance on whether or not the skin lesion appears to be melanoma.
To find out how well the AI-based app worked as a decision support tool, the researchers compared the app’s response to the diagnoses made by the regular diagnostic procedure.
Of the more than 250 skin lesions examined, physicians found 11 melanomas and 10 precursors of cancer, known as in situ melanoma. The app found all the melanomas, and missed only one precursor. In cases where the app responded that a suspected lesion was not a melanoma, including in situ melanoma, there was a 99.5% probability that this was correct.
“It seems that this method could be useful. But in this study, physicians weren’t allowed to let their decision be influenced by the app’s response, so we don’t know what happens in practice if you use an AI-based decision support tool. So even if this is a very positive result, there is uncertainty and we need to continue to evaluate the usefulness of this tool with scientific studies,” says Magnus Falk.
The researchers now plan to proceed with a large follow-up primary care study in several countries, where use of the app as an active decision support tool will be compared to not using it at all.
Deaths from breast cancer dropped 58% between 1975 and 2019 due to a combination of screening mammography and improvements in treatment, according to a new study led by Stanford Medicine clinicians and biomedical data scientists.
Nearly one-third of the decrease (29%) is due to advances in treating metastatic breast cancer, also known as stage 4 breast cancer or recurrent cancer. Although these advanced cancers are not considered curable, women with metastatic disease are living longer than ever.
The analysis helps cancer researchers assess where to focus future efforts and resources.
“We’ve known that deaths from breast cancer have been decreasing over the past several decades, but it’s been difficult or impossible to quantify which of our interventions have been most successful, and to what extent,” said Jennifer Caswell-Jin, MD, assistant professor of medicine. “This type of study allows us to see which of our efforts are having the most impact and where we still need to improve.”
Caswell-Jin and Liyang Sun are co-first authors of the study, which was published in the Journal of the American Medical Association. Sylvia Plevritis, PhD, professor and chair of biomedical data science, and Allison Kurian, MD, MSc, professor of medicine and of epidemiology and population health, are co-senior authors.
The study was a collaborative effort by a national consortium of researchers called CISNET, or the Cancer Intervention and Surveillance Modeling Network. CISNET was established in 2000 by the National Cancer Institute to understand the impact of cancer surveillance, screening and treatment on incidence and mortality. Doing so requires sophisticated computer algorithms capable of modelling the natural course of the disease and the typical treatment paths of individual patients, then translating that information to population-level data collected by the national Surveillance, Epidemiology, and End Results Program, or SEER registry, from 1975 to 2019.
The study is the third in a trio of papers from CISNET published since 2005 that assess the relative contributions of regular screening and treatment advances on breast cancer deaths. The previous two papers informed national guidelines and helped cancer researchers focus their efforts on the most intractable problems.
“Twenty years ago, there was a question whether routine screening mammography actually decreased the number of deaths from breast cancer,” Plevritis said. But in 2005, she and other CISNET researchers published a paper in the New England Journal of Medicine that conclusively demonstrated that screening was responsible for anywhere from 28% to 65% (different models came up with varying degrees of impact) of the reduction in mortality by 2000 between 1975 and 2000.
The second paper, published in 2018 in the Journal of the American Medical Association, highlighted the differences in treatment responsiveness and survival outcomes among women with differing breast cancer subtypes from 2000 to 2012, pinpointing subgroups with poorer survival.
“We found that, while screening still had an important impact, most of the decline in annual deaths was due to improvements in treating early-stage breast cancer based on each cancer’s molecular profile,” Plevritis said.
The current study is the first to explicitly include patients with metastatic breast cancer in its models. The finding that 29% of the decrease in mortality is due to advances in treating metastatic breast cancer both surprised and gratified the researchers.
“Initially, we assumed that treatment of advanced disease was unlikely to make a significant contribution to the declines in mortality we documented in the previous two papers,” Caswell-Jin said. “But our treatments have improved, and it’s clear that they are having a significant impact on annual mortality.”
The CISNET researchers used four computer models to assess the SEER data from 1975 to 2019 — one developed at Stanford Medicine in the Plevritis Lab, one by researchers at the Dana-Farber Cancer Institute, one at MD Anderson Cancer Center, and another jointly developed by researchers at the University of Wisconsin and Harvard Medical School. The four models came up with remarkably similar estimates for the impact of each intervention: screening mammography, treatment of early-stage (stages 1, 2 or 3) breast cancer and treatment of metastatic breast cancer.
The models reproduced the decline in mortality in breast cancer known from SEER data, from 48 per 100 000 women dying of breast cancer each year in 1975 to 27 per 100,000 in 2019, a decrease of about 44%. The models arrived at a larger estimated reduction in mortality of about 58% because the incidence of breast cancer has risen during the same period and more women would have died had screening and treatments not improved.
The models concluded that about 47% of this reduction in mortality is the result of improved treatments for early-stage breast cancer, and about 25% is attributed to screening mammography. The remainder, or about 29%, is due to improvements in treating metastatic disease.
“Designing the new model, which had to account for individuals with non-metastatic cancer who underwent treatment but later progressed to metastatic cancer, and who may have been treated with multiple drugs over the course of their disease, was extremely complex,” Plevritis said. “It took about four years. But it was really satisfying when we were able to validate the model’s behaviour and see that all four models from different institutions, which used the new model inputs in different ways, delivered consistent findings. The models not only make sense, but also produce meaningful insights.”
The impact of treating metastatic disease is exemplified by the increases in median survival time after metastasis: Patients diagnosed in 2000 with metastatic disease lived an average of 1.9 years versus an average of 3.2 years for those diagnosed in 2019. Survival time varies by subgroup status, however. Patients with what are known as oestrogen receptor-positive and HER2 positive cancers saw an average increase in survival time of 2.5 years. Those with oestrogen receptor-positive and HER2-negative cancers lived an average of 1.6 years longer, but those with cancers that are oestrogen receptor-negative and HER2-negative lived about 0.5 years longer in 2019 than in 2000.
“It was meaningful as a breast oncologist to spend time with this history and see real progress over the past decades,” Caswell-Jin said. “There is much more work to be done; metastatic breast cancer isn’t yet curable. But it is rewarding to see that advances have made a difference in these numbers,” she added. “Our scientific and clinical work is helping our patients live longer, and I believe deaths from breast cancer will continue to steadily decline as innovation continues to grow.”
The exercise stress test, which involves treadmill exercise test with electrocardiogram (ECG), is one of the most familiar tests in medicine. While exercise testing typically is focused on diagnosing coronary artery disease, a recent study from Mayo Clinic finds that exercise test abnormalities, such as low functional aerobic capacity, predicted non-cardiovascular causes of death such as cancer in addition to cardiovascular-related deaths. These new findings are published in Mayo Clinic Proceedings.
The exercise stress test is noninvasive, easily available and provides important diagnostic information. In addition to the ECG itself, the test produces data on functional aerobic capacity, heart rate recovery and chronotropic index, the standardised measure of heart rate during exercise that reflects age, resting heart rate and fitness.
“In our exercise testing cohort, non-cardiovascular deaths were more frequently observed than cardiovascular deaths,” says Thomas Allison, PhD, MPH, director of Mayo Clinic’s Integrated Stress Testing Center and the study’s senior author. “Though this was a cardiac stress test, we found that cancer was the leading cause of death, at 38%, whereas only 19% of deaths were cardiovascular. Exercise test results including low exercise capacity, low peak heart rate, and a slow recovery of the heart rate after exercise test were associated with increased mortality.”
The study looked at 13 382 patients who had no baseline cardiovascular issues or other serious diseases and who had completed exercise tests at Mayo Clinic between 1993 and 2010, then were followed closely for a median period of 12.7 years.
The findings suggest that clinicians should focus not only on ECG results but on data in the exercise test results such as low functional aerobic capacity, low chronotropic index and abnormal heart rate recovery. Patients should be encouraged to increase their physical activity if these results are atypical, even if the ECG results show no significant cardiovascular-related risk, Dr Allison says.