A treatment for stroke patients was no more effective than an inactive drug
Source: CC0
The first international trial of an unproven stroke treatment available in the US has concluded that, while harmless, perispinal etanercept is no more effective than an inactive dummy drug, or placebo.
Survivors of stroke have travelled at considerable expense to private clinics in the US to be treated with the arthritis drug etanercept.
In the clinics, the drug is injected into the cervical spinal area, and the patient is then tilted head-down in the belief that this allows the drug to enter the brain.
Stroke is a leading cause of disability throughout the world, affecting more than 7 million people a year. Despite advances, treatments for impairment after stroke remain limited. Some patients call perispinal etanercept a “miracle cure”.
Florey leading stroke researcher, neurologist Professor Vincent Thijs led the Perispinal Etanercept to improve STroke Outcomes – or “PESTO” – trial to investigate this further, supported by funding from the Australian Government.
“We understand why people living with the long-term effects of stroke seek hope and new options,” Professor Thijs said. “With support from the Stroke Foundation and the Medical Research Future Fund, we put this treatment to the test using the gold standard of clinical research – a double-blind randomised trial.”
Half of the PESTO participants were treated with the drug, and half were treated with an inactive dummy drug, with patients and doctors “blind” to who was getting which.
This type of trial eliminates biases because neither doctors nor patients knew who was getting etanercept and who was getting the placebo. Because the results for the 2 patient groups were so similar, we concluded that while the drug did not cause harm, we found no evidence that it led to improved quality of life compared to placebo.
Professor Thijs, who leads the Young Stroke Service at The Florey, said improvements could be due to the placebo effect, a well-established medical phenomenon where some patients in a trial may notice an improvement, despite only receiving a dummy treatment.
126 people from Australia and New Zealand participated in PESTO.
63 received the treatment, 63 the placebo.
Their stroke symptoms were measured before the trial and 28 days after.
There were no adverse side effects.
Among participants who received perispinal etanercept, 52 per cent (33 out of 63) felt better.
Among participants who received the placebo, 57 per cent (36 out of 63) felt better.
The difference in results between the 2 groups is deemed statistically insignificant.
“It’s important for doctors and the stroke survivor community in Australia and around the world to know that we found no evidence that perispinal etanercept improved quality of life,” Professor Thijs said.
Kelvin Hill, Executive Director of Stroke Programs, Research and Innovation at Stroke Foundation said: “Every Australian stroke patient should have access to the best, evidence-based treatment. Findings of the PESTO study underscore the critical importance of robust research and clinical trials in discovering if treatments work or not.
“Australians experience around 46 000 stroke events every year (one every 11 minutes), and there are now over 440 000 survivors of stroke living in Australia. Stroke Foundation will continue to advocate for more research funding to unlock new effective treatments for stroke; and ensure that advice provided in the Living Clinical Guidelines for Stroke Management enables clinicians to provide the best stroke care possible,” Mr Hill added.
Overall, there was a 14% reduction in skin cancer risk. When nicotinamide was taken after a first skin cancer, the risk reduction rose to 54%.
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
The dietary supplement nicotinamide has been recommended by dermatologists for people with a history of skin cancer since 2015, when a clinical study with 386 participants showed that those who took the vitamin B3 derivative developed fewer new occurrences.
But data to validate those findings in a larger study group has been lacking because nicotinamide can be purchased over the counter without being entered into patients’ medical records.
In a new study published in JAMA Dermatology, researchers found a way to get that data by analysing records from the Veterans Affairs Corporate Data Warehouse. Nicotinamide is on the VA’s official formulary, so the researchers checked the outcomes of 33 833 patients for their next skin cancer diagnosis following baseline treatment with 500 milligrams of nicotinamide twice daily for longer than 30 days. They looked for occurrences of basal cell carcinoma and cutaneous squamous cell carcinoma.
The researchers compared 12 287 patients who received the treatment with 21 479 who did not. Overall, there was a 14% reduction in skin cancer risk. When nicotinamide was taken after a first skin cancer, the risk reduction rose to 54%, but the benefit declined with treatment initiation following subsequent skin cancers. The risk reduction was much larger for squamous cell carcinoma.
“There are no guidelines for when to start treatment with nicotinamide for skin cancer prevention in the general population. These results would really shift our practice from starting it once patients have developed numerous skin cancers to starting it earlier. We still need to do a better job of identifying who will actually benefit, as roughly only half of patients will develop multiple skin cancers,” said the study’s corresponding author, Lee Wheless, MD, PhD, assistant professor of Dermatology and Medicine at Vanderbilt University Medical Center and a staff physician at VA Tennessee Valley Healthcare System.
The researchers were also able to ascertain the outcomes of 1,334 patients who were immunocompromised due to having received solid organ transplants. Among solid organ transplant recipients, no overall significant risk reduction was observed, although early nicotinamide use was associated with reduced occurrences of cutaneous squamous cell carcinoma.
The findings from the current study suggest that magnesium also increases the gut synthesis of vitamin D, which does not go to the blood and takes effect locally.
Photo by Danilo Alvesd on Unsplash
Researchers from Vanderbilt University Medical Center have demonstrated in a precision-based clinical trial that a magnesium supplement increases gut bacteria in humans that have been shown to synthesise vitamin D and inhibit colorectal cancer carcinogenesis.
However, the effect was observed primarily in females – an outcome that the researchers surmised may be attributable to the role that oestrogen plays in shifting magnesium from circulation into cellular uptake.
Intestinal microbiome data and colonoscopy results were analysed from participants who were randomised by whether they had the TRPM7 genotype, which plays a crucial role in regulating magnesium and calcium uptake.
Previously, the investigators showed in the same randomised trial that magnesium enhances the synthesis of vitamin D and increases the blood levels of vitamin D. The findings from the current study suggest that magnesium also increases the gut synthesis of vitamin D, which does not go to the blood and takes effect locally.
“Our previous study showed magnesium supplementation increased blood levels of vitamin D when vitamin D levels were low,” said Qi Dai, MD, PhD, professor of Medicine. “The current study reveals that magnesium supplementation also increases the gut microbes which have been shown to synthesise vitamin D in the gut without sunlight and locally inhibit colorectal cancer development.”
The participants were divided into two arms, one that received the magnesium supplement and another that received a placebo. Their gut microbiome was analysed from stools, rectal swabs and rectal tissues. Among participants with adequate TRPM7 function, the magnesium supplement increased Carnobacterium maltaromaticum and Faecalibacterium prausnitzii, which were previously found to work synergistically to increase vitamin D and decrease colorectal carcinogenesis. Among those with inadequate TRPM7 function, the magnesium supplement reduced the abundance of F. prausnitzii in rectal mucosa.
Among 236 participants who all had a history of colorectal polyps, 124 underwent colonoscopies after completing the trial with a 3.5-year median follow-up time. A higher abundance of F. prausnitzii in rectal mucosa was associated with an almost threefold increase in developing additional polyps.
Study of nearly 4 million children and adolescents finds that 10% of paediatric blood and bone marrow cancers may have stemmed from radiation exposure.
Credit: Pixabay CC0
A study led by UC San Francisco and UC Davis has concluded that radiation from medical imaging is associated with a higher risk of blood cancers in children.
For the study, which appears in NEJM, the researchers examined data from nearly 4 million children and estimated that 1 in 10 blood cancers – some 3000 cancers in all – may be attributable to radiation exposure from medical imaging. The risk increased proportionally based on the cumulative amount of radiation the children received.
The investigation is the first comprehensive assessment using data from children and adolescents in North America that quantifies the association between radiation exposure from medical imaging and blood and bone marrow cancers, such as leukaemia and lymphoma, which are the most common forms of cancer in children and adolescents.
Medical imaging saves lives by enabling timely diagnosis and effective treatment, but it also exposes patients to ionizing radiation, a known carcinogen, particularly through computed tomography (CT).
The authors caution that doctors and parents should avoid excessive radiation doses and minimize exposure when clinically feasible.
“Children are particularly vulnerable to radiation-induced cancer due to their heightened radiosensitivity and longer life expectancy,” said Rebecca Smith-Bindman, MD, a radiologist and professor of Epidemiology and Biostatistics, as well as Obstetrics, Gynecology and Reproductive Sciences at UCSF and the first author of the paper.
“While medical imaging can be lifesaving, our findings underscore the critical need to carefully evaluate and minimise radiation exposure during paediatric imaging to safeguard children’s long-term health,” said Smith-Bindman, who is also a member of the Philip R. Lee Institute for Health Policy Studies. “This involves ensuring that imaging is performed only when it provides essential information for the child’s care and, in cases such as CT scans, using the lowest possible radiation doses.”
Documenting risks in children
The study uses a retrospective cohort design, looking back at the complete imaging histories of 3.7 million children who were born between 1996 and 2016. The children were treated at six health care systems in the U.S. and Ontario, Canada. Investigators found a significant relationship between cumulative radiation dose and the risk of a hematologic malignancy, which includes tumours affecting the blood, bone marrow, lymph, and lymphatic system.
The risk of developing cancer varied significantly by imaging modality. CT, which is used to detect many abnormalities such as tumours, heart disease, and injuries of the spinal cord and brain, entails significant radiation exposure. But radiographs, which are used to diagnose both broken bones and pneumonia, expose children to much lower doses.
Among all the forms of medical imaging, the study found that chest radiography was the most common imaging exam that doctors performed. The most common form of CT was of the head and brain.
For children who underwent a head CT, the researchers attributed about a quarter of the children’s subsequent hematologic malignancies to radiation exposure. For those who had radiographs, by contrast, they estimated that only a small fraction of the children’s subsequent cancers were associated with radiation exposure.
Getting one or two head CTs was associated with a 1.8-fold increased risk of a cancer diagnosis, and this rose to 3.5 times for children who received more scans and were therefore exposed to more radiation.
Altogether, 2961 haematologic malignancies were diagnosed during the study period. Lymphoid malignancies accounted for 79.3%, while myeloid malignancies and acute leukaemia together accounted for 15.5%. About 58% of cancers occurred in males, and about half were diagnosed in children under 5.
The authors said that up to 10% of haematologic malignancies in children and adolescents could be prevented by reducing unnecessary imaging and optimising radiation doses. In many cases, the authors said, substituting non-ionising imaging modalities like ultrasound or MRI may be feasible without compromising diagnostic accuracy.
Benefits vs risks
The authors emphasised that while medical imaging remains an invaluable tool in paediatric care, their findings highlight the need to carefully balance its diagnostic benefits with potential long-term risks.
“This study provides robust, directly observed evidence of a clear dose–response relationship between radiation from medical imaging and hematologic malignancy risk in children and adolescents,” said Diana Miglioretti, PhD, UC Davis Health professor and chief of the Division of Biostatistics.
“Our findings align with international research highlighting that children are especially radiosensitive,” Miglioretti added. “It’s crucial for clinicians to weigh the immediate benefits of imaging against potential long-term health risks and to optimise imaging protocols to minimize radiation exposure.”
For women who’ve overcome cervical cancer, new research from MUSC Hollings Cancer Center points to another health risk that may not be on their radar: anal cancer.
While cervical cancer is one of the most preventable cancers, with a survival rate of over 90% when found early, clinical guidelines have not addressed what comes next for these patients, who may be at high risk for a related type of cancer.
“We’ve known for a long time that both cervical and anal cancers are caused by HPV, the human papillomavirus,” Deshmukh said. “But what hasn’t been well-understood is how that shared risk might connect the two diseases over a woman’s lifetime.”
Currently, anal cancer screening is recommended for certain high-risk groups, such as people living with HIV, organ transplant recipients and women with a history of vulvar cancer. But there are no clear screening guidelines for women with cervical cancer.
One problem has been a lack of long-term data on their risk and how that risk changes with age and over time. This study helps to fill that gap using high-quality, population-based data.
The researchers turned to the National Cancer Institute’s SEER (Surveillance, Epidemiology and End Results) program – a comprehensive set of registries that tracks cancer diagnoses across the US. They analysed data from more than 85 000 women diagnosed with cervical cancer, tracking them over two decades to see how many went on to develop anal cancer and when those diagnoses occurred.
What they found was striking. Compared with the general population, women with a history of cervical cancer had nearly twice the risk of developing anal cancer.
Anal cancer rates increased with age and over time, with the most diagnoses found in women ages 65 to 74 who were more than 15 years out from their original diagnosis. For women in this age group, the rate of anal cancer diagnoses surpassed a widely accepted threshold for recommending routine screening.
“Our study shows that the risk doesn’t go away – it actually increases with age and over time,” Damgacioglu said.
Why the delay? HPV-related cancers often take years, sometimes decades, to develop. In some cases, the virus may linger undetected or have spread from another part of the body.
“It’s a slow process,” Deshmukh said, “and that’s part of why it’s been so hard to detect. By the time symptoms show up, the cancer is often advanced.”
While anal cancer screening is not as routine as screening for other cancers, reliable methods do exist, including anal cytology (a kind of Pap screen) and anoscopy. Unfortunately, access to specialised screening remains limited. In South Carolina, for example, there is currently only one provider trained to perform high-resolution anoscopy.
That is why it is so important to identify and prioritise the highest-risk groups.
“These results tell us that women who had cervical cancer years ago should be considered for routine anal cancer screening,” Damgacioglu said. “Right now, that’s not happening.”
Deshmukh and his team are now working on a project to determine when and how often screening should happen.
The courts have spoken. The health ombud has issued devastating reports. The Auditor-General has again put damning evidence on the table. Civil society has protested. Yet, the devastating crisis in Gauteng’s health system shows no sign of improvement.
The rot in Gauteng appears to be deepening. Nowhere is this more evident than in the province’s health department, which remains trapped in a cycle of institutional decay and administrative failure.
The consequences are catastrophic, with real and devastating impacts on lives and the delivery of essential health services.
A case in point is the department’s failure to provide life-saving treatment to cancer patients. In a stunning rebuke, a high court found this failure unlawful and unconstitutional. Rather than comply with its constitutional obligations, Health MEC Nomantu Nkomo-Ralehoko and the health department chose to appeal the judgment to the Supreme Court of Appeal.
Making matters worse, a second high court ruling ordered the department to implement the original judgment. And yet again the department is appealing.
Jack Bloom, a DA MP in Gauteng, suggests that the MEC and the department is fighting so hard because they may eventually be held accountable in a case he says evokes the horrors of the Life Esidimeni tragedy. Bloom may have a point.
The background is dismaying.
Prior to the recent court rulings on cancer care, sustained pressure from activists had helped the department secure a R784 million budget for outsourcing radiation oncology services. But the department returned the first tranche of R250 million to Treasury unspent.
At last count in 2022, more than 3 000 patients were on a waiting list for treatment. Many of them would by now have lost their lives. Others may still be alive, but the optimal time for them to get radiation therapy may have passed and their chances of survival are thus substantially diminished.
That R250 million meant to help these desperate people and families simply went unspent boggles the mind.
It is no doubt too late for many, but there are at least some limited signs of progress. While the department has not been answering Spotlight’s questions, Nkomo-Ralehoko has indicated in the Gauteng legislature that a significant number of cancer patients are being treated with the help of private sector facilities. That the MEC and the department is nevertheless challenging the high court ruling, much of which is a demand for greater transparency, suggests that they know they have at best taken several more steps back than they have taken forward.
Add it all up and it is clear the rot runs very deep.
The reason for this is no mystery. The Gauteng health department has an annual budget of around R67 billion. This is more than 20% of the South African government’s entire spending on health. For the corrupt, the Gauteng health department is an obvious target.
And that it has been systematically targeted is not in doubt. Human rights activist Mark Heywood and Wits University Professor Alex van den Heever reckon that close to R20 billion has been stolen from the Gauteng health department over the past decade. “The scale of this theft makes former President Jacob Zuma look like a clumsy shoplifter,” Heywood writes in the Daily Maverick.
Perhaps the clearest dissection of how deep the rot goes is to be found in investigative journalist Jeff Wicks’ excellent book The Shadow State: Why Babita Deokaran Had to Die. In it, he unpacks the industrial-scale corruption at Tembisa Hospital where R830 million was siphoned off in just four months by a network of ruthless, well-connected looters. Allegedly, one of the key beneficiaries was Vusimusi “Cat” Matlala, a businessman with a criminal record and close ties not only to ANC bigwigs but also to senior police officials.
Meanwhile, the department is also failing to pay its creditors on time. Recently, City Press reported that Gauteng’s health department was the only provincial department flagged for noncompliance across all audit areas — despite having received a clean audit opinion. Accruals now exceed R8 billion, consuming 12% of the department’s R67 billion budget. “The problems are huge,” admitted Lebogang Maile, Gauteng’s MEC for Treasury and Economic Development.
Whichever way you slice it, the harsh truth is that even in 2025, the devastating crisis in Gauteng’s health system shows no sign of improvement. Corruption still plagues the department just as severely as it did a decade ago, if not more so. In the end, it is the province’s many committed healthcare workers and the people who depend on the public healthcare system who pay the price – whether a cancer patient or someone with a stoma and in need of a reliable supply of colostomy bags.
Where to from here?
Ultimately, the person responsible for fixing all this is Gauteng Premier Panyaza Lesufi. As Premier, he appoints both the province’s MEC for health and the head of its health department. It is because of Lesufi that Nkomo-Ralehoko and head of department Lesiba Malotana are still in place, despite the havoc around them.
From one perspective, it is hard to fathom why an ambitious politician like Lesufi would stand for such gross incompetence. His party, the ANC, has after all already been severely punished at the polls – in 2024 they got just under 35% of the votes in the province. Letting the province’s already eroded health services decay further can only lead to further electoral decline.
It is of course also possible that Lesufi and those around him are being misled, or intentionally not paying much attention, to just how bad things really are. Zuma too insisted that “we have a good story to tell” even as the state capture looters were in full stride. Maybe reality will similarly catch up with Lesufi if he continues faffing about while Rome burns.
After all, the courts have spoken. The health ombud has issued devastating reports. The Auditor-General has again put damning evidence on the table. Civil society has protested time and time again and spoken out in the media. Doctors and nurses have tried to raise issues through the correct channels and have been ignored. Expert help has been offered and declined. Most damningly, whistleblowers have paid with their lives.
Disclosure: SECTION27 is involved in the cancer court case proceedings as well as ongoing efforts seeking justice for the Life Esidimeni tragedy. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
University students have limited spending money and their schedules are packed. Many are adapting to new lifestyles on campus. Eating a healthy diet is crucial: a poor diet leads to reduced concentration, lower grades and increased stress.
Campus cafés, especially at universities that are some distance from supermarkets, often sell mainly fast food such as white bread sandwiches, hot chips and doughnuts. It’s easy to eat on the go, but places nutritious choices out of reach.
I’m an urban geographer who researches the relationship between food, health and place. My work examines how urban agriculture, informal food systems and everyday urban infrastructures shape well-being, sustainability and spatial justice in African cities.
Research has already found that through pricing, menu design and information provision, campus cafés play a decisive role in shaping dietary behaviours among young adults. I wanted to find out how students at the University of the Western Cape in South Africa choose what to eat when they’re on campus, what they see as healthy food and what stands in the way of them buying nutritious meals.
The university is one that was underfunded during apartheid. Until 1994 it primarily taught students who were Black and people of Colour. Today, it serves about 23 000 students, many of whom are drawn from low-income backgrounds, and has few supermarkets within walking distance. The campus cafés are a key food supply area for students.
My research found that at the University of the Western Cape, only 32% of the food offered at the student café was healthy. It also cost more than the fast food. The students I surveyed knew healthy food was important. But only a small minority consistently chose nutritious meals. Nearly 40% of the group reported that the healthy options were too expensive.
When students face the twin challenges of financial hardship and inadequate access to affordable, nutritious food, this deepens inequality. It also undermines their efforts to succeed. Even worse, it can cause students to develop long term, unhealthy eating habits that damage their health.
Unless affordability, availability and awareness of healthy food choices are addressed together, students will struggle to eat well and to perform at their best.
Universities must implement targeted food subsidies, introduce clearer nutritional labelling, and expand healthy menu options to make nutritious eating more accessible and appealing to students.
Students speak out about their food choices
I conducted a survey that sampled 112 students in five campus cafés at the university. These cafés are mainly used by students in the 18-24 age group.
My survey revealed that 75.9% of students considered healthy offerings at least “somewhat important” when choosing where to eat. Yet only 6.3% always selected nutritious options; 28.6% rarely or never did so. Meanwhile, 38.4% of students described nutritious meals as “expensive” and another 8% found the healthy options “very expensive”.
My research also found that University of the Western Cape students ate very little fruit and vegetables. Just 41% of the students I surveyed ate two or more servings a day and 9.8% admitted they ate none.
I also did a detailed menu audit at one café to see what was on the menu. I found that only 32.6% of 46 distinct items met basic “healthy” criteria (they were low in saturated fats and made up of whole-grains or vegetables).
The majority of students (55.4%) had not noticed any campus healthy-eating campaigns, but agreed (57.1%) that balanced meals boosted academic performance and overall well-being:
I feel much more focused and energetic when I eat well, which helps me do better in my studies and feel healthier overall.
Only a small handful of the students said they could afford healthy campus café meals:
I choose cafés based on food quality. If the food is fresh and tasty, I’ll pay more, but it needs to be worth it.
What needs to happen next
High prices for nutritious items, narrow menu selections and barely visible information about nutrition are preventing students from eating healthy foods on campus.
Campus café offerings tend to mirror the broader inequities of national and global food systems. Food environments of big institutions like universities can prop up food inequality, even if these universities are committed to social justice.
Universities should adopt these steps to make healthy food available to students:
Subsidised meal plans and discounts: Introducing a tiered subsidy for students from low-income backgrounds would directly reduce costs. For example, meal vouchers could make salads, whole-grain sandwiches and fruit bowls as affordable as a pastry or soft drink.
A wider range of food on the menu and smaller portions: Partnerships between university caterers and local cooperatives or farmers could expand the range of fresh produce. Smaller portions or “light” meal options could be sold at lower prices to suit tighter budgets. Regularly rotating healthy specials and clearly labelling ingredients and calories would help students become accustomed to choosing healthy meals.
Visible nutrition campaigns: Digital and printed standout posters about healthy foods could be placed around campus. Universities could hold social-media challenges and pop-up tasting events. Integrating simple tips into lecture slides or student newsletters would also help by repeatedly exposing students to healthy food tips.
Peer-led workshops and cooking classes: These should be arranged to empower students to take ownership of their diets and learn about budgeting, meal planning and quick, nutritious cooking skills. Peer facilitators can demystify healthy eating and create a supportive healthy eating community.
Seeking feedback: To see if their healthy food campaigns are working, universities should survey students, and analyse sales data from the cafés to see what’s being eaten. They should get feedback from students through focus groups that identify emerging needs and ensure that campaigns and projects reflect the realities of students’ lives.
My research suggests that by tackling cost, choice and communication together, universities can transform their cafés from sites of compromise into engines of student well-being. Such interventions would unlock academic potential and set young people on healthier life paths. This is an outcome as enriching as any degree.
A new study suggests that physical frailty may contribute to the development of dementia. The study was published on September 17, 2025, in Neurology®, the medical journal of the American Academy of Neurology.
Physical frailty is defined as having three or more of these five symptoms: often feeling tired; little or no physical activity; slow walking speed; low grip strength; and unintentional weight loss.
“We’ve known that frailty is associated with a higher risk of dementia, but our study provides evidence that frailty may be an actual cause of dementia,” said study author Yacong Bo, PhD, of Zhengzhou University in China. “On the other hand, despite this new evidence, we can’t rule out the possibility that frailty is instead a marker of the early changes in the disease process.”
The study involved 489 573 people with an average age of 57 who were followed for an average of 14 years. A total of 4.6% of the participants met the definition for frailty, with three or more of the symptoms. Another 43.9% who had one or two symptoms were categorised as pre-frailty and 51.5% had no symptoms and were categorised as not frail.
During the study, 8900 people developed dementia. A total of 4.6% of those with frailty developed dementia, compared to 2.2% of those with pre-frailty and 1.3% of those without frailty. After researchers adjusted for other factors that could affect the risk of dementia, such as age, education level and physical activity, they found that the people who met the definition for frailty were nearly three times more likely to develop dementia than those who had no symptoms of frailty.
Those categorised as pre-frailty were 50% more likely to develop dementia. People with frailty who also had genes linked to dementia were nearly four times more likely to develop dementia than those without frailty or the genetic risk. The researchers also analysed the data and found evidence suggesting that frailty may potentially be a factor in causing dementia.
“These findings reinforce the importance of identifying and managing frailty as a strategy for preventing dementia,” Bo said.
Looking at the data from the other direction, the researchers found that dementia is unlikely to increase the risk of frailty. The researchers also looked at brain imaging and biological biomarkers and found that people with frailty were more likely to have changes in their brain structure related to dementia.
“These biomarkers may be a mechanism underlying the pathway from frailty to dementia,” said Bo. A limitation of the study was that four of the five symptoms of frailty were reported by the participants, so they may not have provided accurate information.
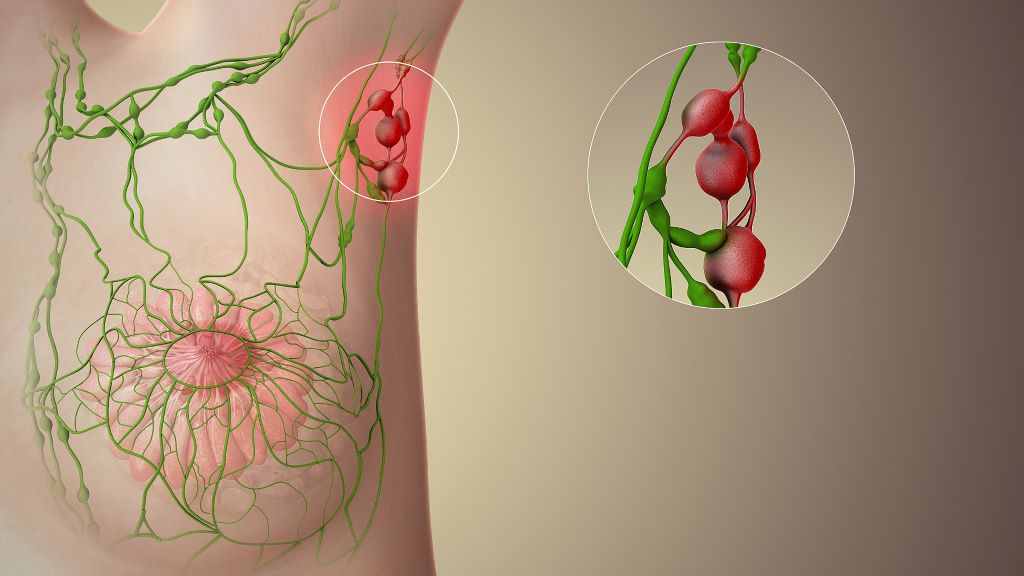
New research has shown why preserving lymph nodes, often removed near tumours to prevent cancer spread, could improve patient outcomes and make immunotherapies more effective.
A team of researchers, led by the Peter Doherty Institute for Infection and Immunity (Doherty Institute), explored the cellular and molecular interactions revealing how lymph nodes play a crucial role in the fight against chronic infection and cancer.
The research, published across two papers in Nature Immunology (references and links below), showed that lymph nodes provide the right environment for stem-like T cells, an important type of immune cell, to survive, multiply and produce killer cells that can fight cancer or viruses. In other immune organs, such as the spleen, these cells don’t develop or proliferate as effectively, making lymph nodes essential for a strong immune response and successful immunotherapy.
The University of Melbourne’s Professor Axel Kallies, Laboratory Head at the Doherty Institute and senior author of both papers, said the findings have important implications for cancer therapy.
“Lymph nodes aren’t just passive waiting rooms for immune cells, they actively train and educate T cells, and send them off to do their job,” said Professor Kallies.
“Our research suggests that removing lymph nodes during cancer surgery, a common practice to prevent tumour spread, may inadvertently reduce the effectiveness of treatments, such as checkpoint blockade and CAR T cell therapies. Preserving lymph nodes could strengthen immune responses and increase the effectiveness of immunotherapy.”
This work may also help explain why some patients respond better to immunotherapy than others. The state and function of lymph nodes influence how well the immune system can produce cancer-fighting T cells, directly impacting the success of immunotherapy.
The University of Melbourne’s Dr Carlson Tsui, Postdoctoral Researcher at the Doherty Institute and first author of one of the papers, said the findings could help to develop new strategies to make immunotherapy more effective.
“Our research identifies molecular signals that are involved in the regulation of stem-like cells and in their capacity to produce effective killer cells. These findings could guide the development and refinement of immune-based treatments for cancer and chronic infection,” said Dr Tsui.
“Furthermore, our research shows that rather than only focusing on the tumour itself, therapies should also be designed to preserve and enhance lymph node function. By targeting these critical immune hubs, we could boost the body’s natural ability to fight cancer, increase the effectiveness of existing immunotherapies and help more patients respond to treatment.”
Together, the two peer-reviewed papers provide a deeper understanding of how lymph nodes shape immune responses. While they are based on work with animal models, they will guide future treatment strategies for chronic infection and cancer treatment.
Professor Shahneen Sandhu, Research Lead for the Melanoma Medical Oncology Service at the Peter MacCallum Cancer Centre, commented on the clinical implications of this work.
“While this research was done in the laboratory with pre-clinical models, we’re excited to study these findings in clinical samples from patients receiving immune checkpoint inhibitors, as part of an ongoing Melanoma Research Victoria collaboration with Professor Kallies,” Professor Sandhu said.
“Combining clinical and preclinical studies will help us translate these discoveries from bench to bedside and back, ultimately improving outcomes for cancer patients.”
Tsui C, Heyden L, et al. Lymph nodes fuel KLF2-dependent effector CD8+ T cell differentiation during chronic infection and checkpoint blockade. Nature Immunology (2025). DOI: https://doi.org/10.1038/s41590-025-02276-7
Wijesinghe SKM, Rausch L, et al. Lymph-node-derived stem-like but not tumor-tissue-resident CD8+ T cells fuel anticancer immunity. Nature Immunology (2025). DOI: https://doi.org/10.1038/s41590-025-02219-2
Sepsis is the No.1 cause of death in the intensive care unit of hospitals worldwide and a major concern for health scientists and medical professionals alike.
Dr Scott Widenmaier (PhD), an associate professor in the Department of Anatomy, Physiology and Pharmacology in USask’s College of Medicine, has zeroed in on a specific protein that might be key to helping the body fight back against the potentially life-threatening condition.
By manipulating this protein, researchers believe there is a new avenue to protect patients against sepsis. Widenmaier and his team have had their research recently published in Cellular and Molecular Gastroenterology and Hepatology.
“Sepsis is the largest cause of death in the intensive care unit globally,” Widenmaier said. “Sepsis can cause damage to organs like the heart, kidney, and lungs. It can also cause liver dysfunction, and when this occurs, the liver is not able to properly perform its functions that are useful in helping the body deal with an infection.”
Sepsis is caused by the body’s immune system response to infection causing damage to the body itself. As Widenmaier puts it, many people believe that bacteria or a virus they acquire are what causes people to get sick. However, it’s the body’s response to the infection that results in severe sickness and can escalate to sepsis – what Widenmaier identified as “a dysregulated immune response that leads to life-threatening complications.”
“The immune system releases cytokines and various factors that are trying to kill the bacteria or the virus, but the process of doing it actually dramatically changes our physiology and leads to us being really sick,” Widenmaier said.
While conventional methods for treating sepsis have been targeted at mitigating the infections that might lead to sepsis, Widenmaier said more recent studies have recognised that the body itself has built-in disease tolerance mechanism that could be harnessed to protect itself from the potential damage. In other words, when disease tolerance is working well, the process of killing the infection won’t cause the person to get nearly as sick and preserve healthy organ function.
Widenmaier and his team identified a “transcription factor” protein in the liver called NRF1, which acts as a “molecular switch” to help control the body’s own disease tolerance response. In experimental models infected with E. coli, over-expressing the NRF1 protein led to better overall responses to infection and protection against sepsis.
When over-expressed, the protein enables the liver to secrete more very low-density lipoprotein (VLDL) particles, which better protects organs against damage caused by sepsis. It’s this connection between the NRF1 “switch” and the liver’s production of VLDL that Widenmaier says may be a promising approach to improve the outcomes of patients with sepsis.
“Our lab is very interested in finding ways to either pharmacologically or genetically manipulate NRF1 to promote health,” he said.
Widenmaier credited his team – including colleagues, students and trainees – for their work in identifying this potential target for sepsis treatments and for the resulting research paper.
The next step for this research would be to see how feasible this pathway might be for treatment and whether it is still active in conditions when sepsis is very common – and while they aren’t at the stage of human trials yet, Widenmaier said he wants to delve deeply into this new area in the search for better sepsis care.
“We want to explore this quite intensively,” he said. “There’s a lot of clinical investigators across the country … I’m interested in continuing those connections and trying to strengthen them, and hopefully we can find a place where clinicians and our lab can benefit from the science.”