Four Cyclists Take on the 2025 KAP sani2c to Inspire South Africans with a Message of Hope
L-R_Steph Bester CEO of AllLife with Billy McLeod
From 8 to 10 May 2025, four cyclists will take on one of South Africa’s most iconic and challenging mountain bike stage races – the KAP sani2c. Covering 265 kilometres over three days from the Southern Drakensberg to Scottburgh on the KwaZulu-Natal South Coast, the event is known for its tough terrain, stunning scenery, and relentless pace. But this year, one team will be racing with more than just medals in mind.
Team Change of Heart is made up of two heart transplant recipients – Billy Macleod (56) and Pedro Basson (20) – and their two experienced cycling partners: Steph Bester, CEO of AllLife, and long-time cycling companion Guy Dudley. Together, they’re not just riding to finish – they’re riding to inspire.
Billy, once an accomplished cyclist and triathlete, was sidelined for six years by heart disease and given just two weeks to live before receiving his transplant.
He made a remarkable comeback in 2024 when he became the first South African heart transplant recipient to complete the KAP sani2c. This year, Billy returns with a renewed purpose – not just to ride, but to support 20-year-old Pedro through his very first stage race. For Billy, this ride is about passing the baton of hope and helping another transplant recipient believe in the impossible.
Pedro, the youngest team member at just 20 years old, will be attempting his first-ever mountain bike stage race. Having received his transplant as a teenager, Pedro’s journey to recovery has been nothing short of remarkable. Taking on sani2c is a bold and symbolic step, one he hopes will encourage other young people with chronic health conditions to dream big and push boundaries.
“This is more than a race – it’s a celebration of life and second chances,” says Steph Bester, who was set to ride alongside Billy last year but had to withdraw at the last minute due to a sudden illness. “Missing out in 2024 was heartbreaking for me, especially because this cause and this team are so close to my heart. I can’t wait to finally be on the bike with them this year. Billy and Pedro are living proof that your story doesn’t end with a diagnosis. At AllLife, we believe in the power of resilience, and this team embodies that belief. It’s an honour to support them – not only on the bike but in sharing their powerful message with the country.”
The team will be riding on e-bikes, enabling them to manage pace, terrain, and energy levels more effectively while still tackling the full challenge of the race. For Pedro, who has never raced before, the support of his three teammates – all experienced sani2c finishers – is crucial.
“Knowing I have a team behind me who understands the journey and is there to support every climb and descent makes all the difference,” Pedro shared. “It’s not just about the bike – it’s about proving to myself that anything is possible.”
AllLife is once again using this race to raise awareness for Hero777, a non-profit foundation focused on increasing organ and tissue donor registrations in South Africa. The foundation is deeply personal to the AllLife family as they deal with so many people in need of transplants daily.
It takes a community that truly understands both the unique challenges individuals face and the deep love for cycling to make something like this possible. The team is incredibly grateful for the support from AllLife, the wider cycling community, and especially race founder Glen Haw (Farmer Glen). Pedro will ride an e-bike generously sponsored by Cannondale, allowing him to tackle this life-affirming challenge alongside his team.
Whether it’s climbing steep hills or sharing laughs around the campfire, Team Change of Heart is ready to show that with support, courage, and a whole lot of heart – anything is possible.
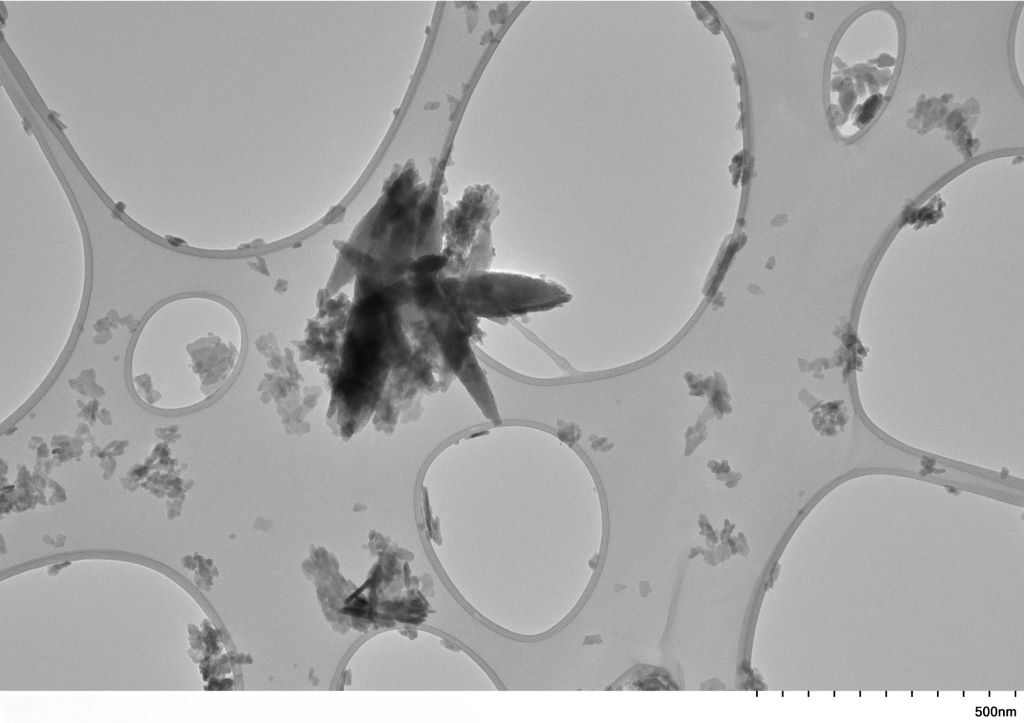
Transmission Electron Microscopy (TEM) picture of nanoplastic particles derived from carotid plaque. Copyright University of New Mexico
People with plaque in the blood vessels of their neck have a higher amount of tiny plastic particles in those vessels compared to people with healthy arteries. This increase was significantly higher in people who had experienced a stroke, mini-stroke or temporary loss of vision due to clogged blood vessels, according to preliminary research presented at the American Heart Association’s Vascular Discovery 2025 Scientific Sessions: From Genes to Medicine.
Micronanoplastics are tiny pieces of plastic created in industrial processes or from larger plastic objects as they degrade in the ocean or the soil. Micronanoplastics are not uniform in size and are a mixture of micro and nano plastic sizes. While microplastics are sometimes visible at less than 5 millimetres in size, nanoplastics are microscopic (invisible to the naked eye), less than 1000 nanometres across. This makes them more easily dispersed and able to penetrate cells and tissues in living organisms. Researchers suggest that terminology should gradually transition to nanoplastics because that is more precisely what is being studied.
“These types of plastics are commonly found in the environment, especially in ocean garbage patches. Over many years, these plastics break down, mix into the soil and water, and can build up in the food chain,” said lead study author Ross Clark, MD, MBA, RPVI, a vascular surgeon-scientist at the University of New Mexico in Albuquerque. “Many people think that micro and nanoplastics mainly come from using plastic utensils, cutting boards, packaging, water bottles and other plastic items. However, the main source is the food and water we eat and drink.”
In 2024, researchers in Italy reported finding micronanoplastics in plaque from some people without symptoms who underwent surgery to remove carotid artery plaque. Symptoms caused by carotid plaque buildup may include stroke, mini-stroke or temporary blindness. Followed for almost three years after surgery, people with micronanoplastics in their carotid plaque were significantly more likely to die or to have a non-fatal heart attack or stroke.
The current study, which included fewer than 50 participants, was built on the previous research conducted in Italy. Researchers compared the levels of micronanoplastics found in the carotid arteries of three groups: people with healthy arteries; those with plaque but no symptoms; and those experiencing symptoms due to plaque buildup. Researchers also compared plaques with low and high plastic levels to assess the effects of micronanoplastics on markers of inflammation, the gene activity of immune cells called macrophages and stem cells that help stabilise plaque.
The analysis found that the concentration of micronanoplastics in carotid arteries was:
16 times higher (895 micrograms/gram vs. 57 micrograms/gram) in plaque among people without symptoms compared to the levels found in artery walls of deceased tissue donors of similar age with no plaque; and
51 times higher (2888 micrograms/gram vs. 57 micrograms/gram) in plaque from people who had experienced stroke, mini-stroke or temporary loss of vision due to blockage of blood flow to the retina, in comparison to samples from age-matched, deceased tissue donors.
Comparing high-plastic and low-plastic plaque levels, the analysis found:
no link between the amount of micronanoplastics and signs of sudden inflammation; and
differences in gene activity in plaque-stabilizing cells and less activity in anti-inflammatory genes of plaque macrophage immune cells.
“These findings indicate that the biological effects of micronanoplastics on fatty deposits are more complex and nuanced than simply causing sudden inflammation,” Clark said. In their next phase of work, they will focus on better understanding the immunological effects of micronanoplastics in clogged arteries.
“It’s very important to study what these materials do to our bodies. However, we should be cautious about the early results of this study. We won’t fully understand the biological effects for many years to come,” Clark said.
The study has several limitations. It cannot prove that micronanoplastics in plaque were the cause of symptoms of carotid artery disease; micronanoplastics might be a sign of another health issue that caused these symptoms. Researchers did not have access to data detailing the sex or race/ethnicity of the tissue donors. Additionally, pyrolysis gas chromatography-mass spectrometry, used to measure plastic in biological samples may have limitations. This technique allows measurements to include nanoplastics and larger microplastic particles and uses high temperatures to break down plastics into smaller organic molecules. However, parts of the biological samples may also break down into similar molecules. For instance, fatty acids found in artery-clogging plaque could break down into compounds appearing similar to polyethylene.
“We are constantly improving our method to reduce the amounts of lipids in the samples to lessen their impact on the results. Lipids have a very similar spectral signature on gas chromatography as some plastic polymers (in particular polyethylene). It can be challenging to distinguish between the lipids and the polyethylene in the results. That’s why removing the lipids is so important. We believe our methods are currently the best way to address this specific criticism. However, new discoveries might change how we understand this data in the future,” Clark said.
“This is a very interesting and troubling study. To date, we have not considered exposure to plastic micronanoparticles a modifiable risk factor for stroke. Although it is important to understand the mechanism at play in the pathophysiology of symptomatic carotid atherosclerosis, this association presents a novel potential target for stroke prevention,” said Karen L. Furie, MD, MPH, FAHA, volunteer vice chair of the American Heart Association Stroke Brain Health Science Subcommittee and professor and chair of neurology at the Warren Alpert Medical School of Brown University in Providence, Rhode Island. Furie was not involved in this study.
Study details, background and design:
Researchers tested 48 samples of carotid arteries from 48 different adults collected in 2023-2024 at the University of New Mexico and the Office of the Medical Investigator (a state agency and part of the Department of Pathology at the University of New Mexico).
About one-third of the samples were from people aged 60 to 90 who had surgery to remove plaque from their carotid arteries. These people had symptoms including stroke, mini-stroke or temporary blindness (called amaurosis fugax).
About one-third of the samples came from people of similar age with no symptoms. They were having surgery to remove plaque buildup in their carotid arteries because a blockage was found during screening or a physical exam.
The last one-third of the samples came from tissue donors. These age-matched donors had died of any cause and did not have carotid artery blockage.
The researchers also compared plaques with low vs high amounts of micronanoplastics on inflammation-related measures. All samples were analysed to measure inflammation by looking at levels of inflammatory molecules TNF-α and IL-6. The levels were compared to the amount of plastics to find any connections. For the RNA sequencing studies, researchers examined samples with the highest and lowest concentrations of plastics.
By Raynold Tlhavani, Partner & Micaela Pather, Senior Associate from Webber Wentzel
The recent judgment in Moss v Road Accident Fund,1 handed down by the Western Cape High Court, has reignited debate regarding the Road Accident Fund’s (RAF’s) liability to compensate accident victims for past medical expenses already covered by their medical aid.
If this sounds familiar, that’s because it is. Recently, the same court in Rahldeyah Esack v the Road Accident Fund1 dealt with the same legal question raised in Moss: can a claimant’s right to compensation under the RAF Act 56 of 1996 be diminished by third-party payments? The court in Moss followed the earlier ruling in Esack, which held that the RAF is liable for a claimant’s past hospital and medical expenses, even if these were covered by a medical scheme.
The facts in Moss were that, in September 2017, the 77-year-old plaintiff sustained bodily injuries when he was struck by a vehicle while cycling. He claimed ZAR 34 286.59 in past medical expenses, of which ZAR 4 173.80 had been paid out of pocket, while the balance had been settled by his medical aid. The RAF opposed the claim, relying on its internal directives from 2022 and 2023, which instructed staff to reject past medical expense claims where the expenses had already been paid by a medical scheme. These directives were not formally introduced before the court. The defence was described as ill-conceived and procedurally inappropriate. Although the court declined to rule substantively on the legal issues raised by the RAF’s directives, it noted that the directive touches on complex areas of law, including common and statutory law, champerty, subrogation, and medical scheme law, which it would not address in context of this judgment.
The court also remarked on the RAF’s litigation practices, observing that the fund had drastically reduced its reliance on external counsel and instead “overburdened” a handful of attorneys at the State Attorney’s office.
It noted with concern that counsel from previously disadvantaged backgrounds, who had historically relied on RAF work, were no longer being briefed, undermining transformation imperatives. It further highlighted the impact on practitioners who, through no fault of their own, were forced to juggle multiple RAF matters in a single day.
Ultimately, the court’s decision in Moss mirrored that in Esack, granting the plaintiff a full award for past medical expenses, regardless of third-party payments. It remains to be seen whether this approach in the Western Cape Division, at odds with a Full Bench decision of the Gauteng Division, will gain traction in other divisions.
Finding a path forward for South Africa’s healthcare workers
Donald McMillan
By Donald McMillan, Managing Director at Allmed Healthcare Professionals
06 May 2025
South Africa’s healthcare system is under serious pressure. The sudden suspension of critical US funding has resulted in the loss of around 15 000 healthcare jobs – many of them linked to HIV/AIDS programmes that served as lifelines for vulnerable communities. Combined with broader public sector budget cuts and a national hiring freeze, the situation threatens to undo decades of progress in healthcare delivery. As public hospitals struggle with fewer staff and shrinking resources, the country is at risk of losing not only jobs, but skills, infrastructure, and hope. But in the face of these challenges, there are still ways to keep services running and people employed. One of them is through Temporary Employment Services (TES), which provides a flexible staffing approach that can help stabilise the system while longer-term solutions are explored.
A healthcare system under pressure
The US aid cut has had an immediate and devastating impact. Programmes focused on HIV, tuberculosis, and reproductive health, many of which were propped up by international donor funding, have been forced to scale back or shut down entirely. Thousands of community healthcare workers, nurses, counsellors, and administrators have found themselves jobless, while patients are left facing longer wait times and reduced access to care.
At the same time, cost-cutting across the public sector has put a freeze on new hires, even in essential departments like health and the impact is already being felt. With public hospitals and clinics stretched thin, they’re unable to take on newly trained doctors and nurses. And while the private sector plays a role, it simply cannot absorb the overflow. This isn’t just a staffing issue, it’s a setback for the entire healthcare system, affecting everything from medical training to frontline care.
Young professionals left in limbo
Every year, South Africa produces thousands of highly trained doctors and healthcare workers, many of whom move into the public health system after completing their compulsory community service. These roles used to be a given but with hiring freezes and shrinking budgets, many young professionals are now finishing their training with nowhere to go. Despite their skills and frontline experience, these workers are left in limbo. This is a double blow as South Africa loses out on the return from its investment in their education, while the risk of a growing skills drain looms large. With countries like the UK, Australia, and Canada actively recruiting healthcare workers, there’s a real chance they may leave and not come back.
A flexible solution in Temporary Employment Services
In response to this crisis, temporary employment solutions have become a practical and effective solution. TES providers offer qualified healthcare professionals short- to medium-term flexible contracts, enabling them to continue working in their field while delivering essential support to overburdened healthcare facilities.
This approach offers a lifeline not just for displaced workers, but for clinics and hospitals struggling with limited resources. TES employees can be rapidly deployed where they are needed most, whether to cover staff shortages, serve remote communities, or support seasonal fluctuations in demand. Unlike permanent hires, they don’t carry long-term costs such as medical aid or pension contributions, making them a more budget-conscious option in uncertain times.
The benefits of the TES model have already been proven. During the COVID-19 pandemic, temporary staff played a key role in scaling up testing, vaccination, and treatment efforts across the sector. That same adaptability is needed now to respond to the healthcare funding crisis.
Rethinking the future of healthcare work
While temporary employment solutions cannot not solve the problem alone, it can provide an important stopgap and potentially a new way of thinking about workforce planning in the healthcare sector. Rather than relying solely on permanent positions, South Africa may need to adopt a more fluid, demand-based deployment model that allows professionals to move between roles, regions, and areas of urgent need.
Shifting to this model calls for a change in mindset. Permanent posts have traditionally been seen as the gold standard in healthcare, valued for their stability and benefits. But in a time of uncertainty, contract and locum roles – especially when managed by trusted TES providers – can offer a practical alternative, combining income, ongoing experience, and flexibility.
Retaining talent, restoring hope
Avoiding long-term damage to South Africa’s healthcare system will require urgent, coordinated action. Government departments must urgently reprioritise spending toward essential services like health and education. At the same time, private healthcare providers and staffing agencies must step up and work together to ensure that skilled professionals are not lost to the system or the country.
Despite the current turbulence, South Africa’s healthcare workers remain among the best trained and most resilient in the world and with the right support structures, including flexible employment options like TES, we can preserve our healthcare capacity and continue to serve those who need it most.
Researchers have found a possible new explanation for muscle memory by investigating thousands of muscle proteins. This study by the Faculty of Sport and Health Sciences at the University of Jyväskylä showed for the first time that muscles “remember” training at the protein level. The memory trace of previous resistance training persists in muscle proteins for over two months.
It is often thought that the effects of exercise are short-lived, and a break from the gym for just a few weeks can cause stress over muscle loss for some people. However, the research from the University of Jyväskylä has shown that this stress is partly unnecessary, as the effects of resistance training persist in muscles for up to two months and the gains are fast when training is started again after the break. But what mechanisms and changes at the cellular and molecular levels explain muscle memory? This is what the researchers investigated by studying the quantities of thousands of muscle proteins from muscle.
In the study, ten weeks of resistance training was followed by a break of the same length and then followed by another ten weeks of resistance training. Using the proteomics method, it was possible to simultaneously study the quantities of over 3,000 muscle proteins using advanced mass spectrometry equipment.
Training gets encoded into muscle proteins
The study found two types of change profiles in muscle proteins.
Some proteins changed as a result of training, returned to their pre-training state during the break, and changed again during the new training period similarly to the first training period. These included proteins related to aerobic metabolism.
Another group of proteins changed as a result of training and remained changed during the break and after the new training period. Among these proteins were several calcium-binding proteins, such as calpain-2, whose gene has recently been identified to retain a memory trace even after a training break.
“At the level of the number of muscle nuclei and the memory traces of genes, that is, epigenetics, long-term responses that persist even after a break and possibly explain ‘muscle memory’ have previously been observed,” says the lead researcher, Professor Juha Hulmi from the Faculty of Sport and Health Sciences.
“Now, for the first time, we have shown that muscles ‘remember’ previous resistance training at the protein level for at least two and a half months.”
“So, even though muscles eventually shrink back to their original size during a long training break, a memory trace of previous training remains in the muscles. This can make it easier to start training again”, explains Hulmi.
The data collection was carried out at the Faculty of Sport and Health Sciences, University of Jyväskylä. The participants were young adult and middle-aged Finnish men and women who were physically quite active but had no previous experience of systematic resistance training. Proteomic analyses were conducted on 116 muscle samples at the University of Helsinki in the laboratory of research director Markku Varjosalo.
Both high and low-middle income countries have stepped up their efforts to reduce antibiotic resistance
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
National-level policies can reduce the impact of antibiotic resistance across diverse countries, according to a study published April 30, 2025 in the open-access journal PLOS Global Public Health by Peter Søgaard Jørgensen from Stockholm University and the Royal Swedish Academy of Sciences, Sweden, and colleagues.
Antibiotic resistance is a major public health concern, contributing to 1.27 million deaths per year. In 2016, countries around the world committed to developing and implementing national action plans to combat antibiotic resistance. These plans have been criticised for not being fully operationalised. Assessing their impact is challenging – change doesn’t happen overnight, not all countries report their data systematically, and the COVID-19 pandemic disrupted monitoring.
In this study, researchers used the Global Database for Tracking Antimicrobial Resistance Country Self- Assessment Survey (TrACSS) and data on antibiotic use and antibiotic resistance to evaluate the impact of national action over time in 73 countries, representing six continents across high and low-middle income countries. They looked at national trends in indicators related to antibiotic resistance, including antibiotic use, rates of antibiotic resistance, and impact of resistant infections.
By assigning each country an action index, they found that national action was consistently associated with improved indicators of antibiotic resistance. These associations persisted after controlling for factors like socioeconomic conditions, population density, and climate.
Since 2016, both high and low-middle income countries have become more ambitious with their national action plans; only one-third have decreased their efforts to reduce antibiotic resistance.
The authors noted some bias in their sample size in that high-income countries are more likely to have established monitoring systems but stressed the importance of studies like this to establishing the impact of national policies on tackling antibiotic resistance.
The authors add: “Our research shows the importance of all countries taking additional action to address antibiotic resistance. Very ambitious action will be needed to achieve reductions in resistance, but even incremental improvements will help reduce the projected increases…We were not sure that it would be possible to reduce levels of antibiotic resistance while also keeping using antibiotics to the extent that is required by modern health systems, but our research indicates that it is indeed possible.”
Hyperbaric oxygen treatment provides long-term relief for patients suffering from late radiation-induced injuries after treatment of cancer in the lower abdominal area. Five years after hyperbaric oxygen therapy, the positive effects remain. This has been shown in a study conducted at the University of Gothenburg, published in eClinicalMedicine.
Radiation therapy is a component of many cancer treatments in organs such as the prostate, colon, ovaries and cervix. While tumour cells are destroyed, 5-10% of patients experience severe side effects due to healthy tissue being affected by the radiation therapy.
Symptoms may include urinary incontinence, bleeding and severe pain from the lower abdomen that becomes both physically and socially disabling. These problems can occur several years after radiation therapy and cause chronic and increasing discomfort.
Researchers have previously shown that patients experience significantly less discomfort after hyperbaric oxygen treatment. The question in the current study was whether the relief would last over several years. The time aspect is important for future decisions on broader use of the method.
From severe problems to a normal life
Initially, all participants had severe symptoms. The group that was randomly assigned to hyperbaric oxygen treatment fared significantly better than the control group in terms of incontinence, bleeding and pain. The positive effects were sustained over the five year follow-up period.
Nicklas Oscarsson, senior consultant in anaesthesiology and intensive care, and researcher at the University of Gothenburg and Sahlgrenska University Hospital was the principle investigator of the study:
“Patients who respond to treatment go from being very distressed by their symptoms and restricted by their need to have quick access to a toilet, to being able to live a fully normal life. Now we know that this pronounced improvement last for at least five years. The treatment can therefore lead to the healing of an otherwise chronic injury,” he states.
The effects achieved are due to cells sensing and adapting to high oxygen levels. The increased levels of oxygen provided in a hyperbaric chamber increases vascular growth and stops chronic inflammation, reducing severe side effects.
For the oxygen treatments, participants spent 90 minutes a day in a hyperbaric chamber on 30-40 occasions, at a pressure of 1.4 atmospheres (equivalent to 14m underwater). The control group received the usual treatment, which normally includes medication and physiotherapy, for example.
The capacity already exists today
“We have reason to believe that there are many patients with severe symptoms who are never referred to hyperbaric oxygen therapy. Today we already have the capacity to treat more patients, but we need to be better at sharing our knowledge with our colleagues and with patient associations,” says Nicklas Oscarsson.
Severe side effects after radiation therapy are one of the main limitations on the dose of radiation that can be given in cancer treatment. The availability of a treatment that can reduce the number of people affected by these side effects opens the door to increased radiation doses and thus more curable tumours. One area for further investigation, according to the researchers, is whether early treatment with hyperbaric oxygen can prevent the occurrence of severe side effects.
The results are based on surveys and analyses of the participants who have been involved all the way, 70 adults. The treatments were conducted at five university hospitals in the Nordic countries: Rigshospitalet in Denmark, Turku in Finland, Haukeland in Norway, and Karolinska and Sahlgrenska in Sweden.
A review published in The Laryngoscope indicates that climate change’s effects on pollen seasons and concentrations are contributing to increasing rates of allergic rhinitis.
When investigators assessed research published between 2000 and 2023, they identified 30 studies that reported on the current epidemiological state of allergic rhinitis, described factors related to climate change, and observed how global warming is affecting pollen seasons and allergy symptoms.
Sixteen studies reported longer pollen seasons and/or higher pollen concentrations related to climate change. As an example, total pollen emissions in the U.S. are projected to increase by 16–40% by the end of the century and pollen season length to increase by 19 days. Four studies reported an increase in allergic rhinitis–related health care usage, particularly among low-income residents. Two studies reported that health care professionals want more education on climate change.
“Physicians are uniquely positioned to witness the impact of allergic rhinitis on patient outcomes and can adapt their practice as climate change intensifies,” said corresponding author Alisha R. Pershad, BS, a third-year medical student at the George Washington University School of Medicine and Health Sciences. “As trusted voices in the community, they should leverage their frontline experience to advocate for meaningful change in addressing the climate crisis.”
Phthalates are commonly used in plastic medical equipment
Photo by Marcelo Leal on Unsplash
Daily exposure to certain chemicals used to make plastic household items could be linked to the more than 356 000 global deaths from cardiovascular disease that occurred in 2018 alone, a new analysis of population surveys shows.
Although the chemicals, called phthalates, are in widespread use globally, the Middle East, South Asia, East Asia, and the Pacific bore a much larger share of the death toll than others – about three-fourths of the total.
For decades, experts have connected health problems to exposure to certain phthalates found in cosmetics, detergents, solvents, plastic pipes, bug repellents, and other products. These chemicals break down into microscopic particles and are ingested, and studies have linked such exposure to an increased risk of conditions ranging from obesity and diabetes to fertility issues and cancer.
Led by researchers at NYU Langone Health and published in eBioMedicine, the current study focused on a kind of phthalate called di-2-ethylhexyl phthalate (DEHP). This chemical is used to increase the flexibility and softness of food containers, medical equipment, and other plastic items. Exposure has been shown in other studies to prompt inflammation in the heart’s arteries, which over time is associated with increased risk of heart attack or stroke. In their new analysis, the authors estimated that DEHP exposure contributed to 356 238 deaths, or more than 13% of all global mortality from heart disease in 2018 among men and women ages 55 through 64.
“By highlighting the connection between phthalates and a leading cause of death across the world, our findings add to the vast body of evidence that these chemicals present a tremendous danger to human health,” said study lead author Sara Hyman, BS, an associate research scientist at NYU Grossman School of Medicine.
In a past study from 2021, the research team tied phthalates to more than 50 000 premature deaths each year, mostly from heart disease, among older Americans. Their latest investigation is believed to be the first global estimate to date of cardiovascular mortality, or indeed any health outcome, resulting from exposure to the chemicals, said Hyman, who is also a graduate student at NYU School of Global Public Health.
For the research, the team used health and environmental data from dozens of population surveys to estimate DEHP exposure across 200 countries and territories. The information included urine samples containing chemical breakdown products left by the plastic additive. Mortality data was obtained from the Institute for Health Metrics and Evaluation, a research group in the United States that collects medical information worldwide to identify trends in public health.
Among the key findings, the study showed that losses in the combined region of East Asia and the Middle East and the combined region of East Asia and the Pacific accounted, respectively, for about 42% and 32% of the mortality from ardiovascular disease linked to DEHP. Specifically, India had the highest death count, at 103 587 deaths, followed by China and Indonesia. The larger heart death risks in these populations held true even after the researchers adjusted their statistical analysis to take into account population size within the studied age group.
A possible explanation, the authors say, is that these countries face higher rates of exposure to the chemicals, possibly because they are undergoing a boom in plastic production but with fewer manufacturing restrictions than other regions.
“There is a clear disparity in which parts of the world bear the brunt of heightened heart risks from phthalates,” said study senior author Leonardo Trasande, MD, MPP. “Our results underscore the urgent need for global regulations to reduce exposure to these toxins, especially in areas most affected by rapid industrialisation and plastic consumption,” added Dr Trasande, Professor of Pediatrics at NYU Grossman School of Medicine.
Dr Trasande, who is also a professor in the Department of Population Health, cautions that the analysis was not designed to establish that DEHP directly or alone caused heart disease and that higher death risks did not take into account other types of phthalates. Nor did it include mortality among those in other age groups. As a result, the overall death toll from heart disease connected to these chemicals is likely much higher, he says.
Dr Trasande says that the researchers next plan to track how reductions in phthalate exposure may, over time, affect global mortality rates, as well as to expand the study to other health concerns posed by the chemicals, such as preterm birth.
Experts say bacterial infections are responsible for more infant deaths than is generally recognised, and things may get worse as more of the bugs become resistant to commonly used antibiotics. We asked local experts about this growing threat to newborns.
A two-week-old baby is referred to the Red Cross War Memorial Children’s Hospital (RCWMCH) in Cape Town. The infant, who was born prematurely at six months, has come from a nearby neonatal hospital.
She’s developed complications, including a feed intolerance and constant vomiting. On investigation, she is found to have a bowel perforation and a condition called necrotising enterocolitis. Surgeons conclude she needs an operation to repair the perforation. A sample of pus from inside her abdomen is sent to a laboratory to identify any infections. While the tests are being done, the infant is started on second-line antibiotics. The doctors suspect she picked up an infection due to pathogens that may be resistant to first-line antibiotics while in the neonatal hospital.
“But 48 hours later, when the results are available, they may show that the antibiotics we’ve been treating the baby with are not treating the bacteria that have now been detected in the lab,” says Associate Professor James Nuttall, a paediatric infectious diseases sub-specialist at RCWMCH and the University of Cape Town.
“In response to those results, we’d change to a different set of antibiotics to try and target the bacteria that have been detected. In the meantime, the child has deteriorated and requires a second operation. Throughout all the subsequent treatments, we are testing samples for infections she might – and frequently will – acquire along the way.”
From then on, he says it’s a case of trying to keep up with the sequence of infections that the baby might develop. Some of these infections may have originated at the neonatal hospital, while others could have been acquired during her treatment in the Intensive Care Unit (ICU) at RCWMCH, possibly from the operating theatre, intravenous lines, or healthcare workers’ hands.
“This is the kind of scenario we are faced with all the time,” says Nuttall. “The fact is, an infant might come into hospital with one infection and, unfortunately, pick up a bunch of other infections while in the hospital from transmission of pathogens that may be resistant to one or more of the commonly used first- or second-line antibiotics.”
Sitting in a boardroom at the Red Cross Hospital, close to the paediatric wards and clinics in which he treats sick children referred from other hospitals in Cape Town and beyond, Nuttall says there are two possible outcomes for this baby.
“She might turn the corner and respond to the new antibiotics, together with interventions from the surgical doctors and expert management in an ICU. Or she might not respond to the treatment, and die two days later, because of ongoing infection that doesn’t respond to treatment.”
Nuttall is discussing the ongoing issue of rising antibiotic resistance, particularly among neonates, the group most vulnerable to this. He’s responding to Spotlight’s main question: Will the antibiotics used to treat bacterial infections, such as Klebsiella pneumoniae – which have seen hundreds of babies die in hospitals in recent years – keep working? And, how big is the risk of antibiotic resistance to infants?
“The short answer to whether the antibiotics we currently use to treat bacterial infections will keep working is no,” he says.
‘Almost endemic’
In some South African healthcare facilities, especially in the public sector, antibiotic-resistant bacteria have become “almost endemic”, says Professor Shabir Madhi, director of the Wits Vaccines and Infectious Diseases Analytics Unit at University of Witwatersrand (WITS VIDA).
“There are a large number of deaths occurring on an ongoing basis. We still have clusters of outbreaks, but those are underpinned by a really widespread dissemination of these antibiotic-resistant bacteria, and persistently high rates of hospital-acquired infections, especially in the first month of life,” he says. “Despite the best of efforts, we haven’t been able to get on top of this.”
Madhi headed up a study at the Chris Hani Baragwanath Academic Hospital in Soweto in which they used molecular testing to look at evidence of infections in 153 babies who had passed away. The researchers found that infections were the immediate or underlying cause of death in 58% of all the neonatal deaths, including the immediate cause in 70% of neonates with complications of prematurity as the underlying cause.
Overall, 74.4% of 90 infection-related deaths were hospital-acquired, mainly due to multidrug-resistant Acinetobacter baumannii (52.2%), Klebsiella pneumoniae (22.4%), and Staphylococcus aureus (20.9%).
Also asked whether the antibiotics used to treat Klebsiella and other bacterial infections will keep working, Madhi says: “The short answer is that we’ve already run out of antibiotics in the public sector that can treat all of these different bacteria.”
He says that there are two bacteria that are of particular concern in South Africa.
“The one is Klebsiella pneumoniae, which that has become resistant to almost all of the antibiotic classes that are available for use, except perhaps for colistin, (a reserve antibiotic which is seen as a last-resort treatment for multidrug-resistant Gram-negative infections), but even antibiotic resistance to colistin in bacteria is emerging.
“The other big one is Acinetobacter baumannii, which is also a common cause of hospital-acquired infections. Here the bacteria have become resistant to all classes of antibiotics including colistin.”
Madhi says compared to other African countries, South Africa is better equipped to provide high-level care, including intensive care, to prematurely-born babies.
“Consequently, we end up spending a mini fortune to get these very premature children to survive the first few days of life, only for them then to succumb to hospital-acquired infections. Whereas in other settings many of these babies will die in the first few hours of life.”
He adds: “The single leading cause of neonatal mortality in South Africa is antibiotic resistant bacterial infections, but that is underpinned by other conditions which increases the susceptibility of babies to eventually succumb to these hospital-acquired infections.”
In the public sector, Madhi says hospital-acquired infections are a major reason why children are dying. In the private sector, there is more attention on identifying these infections, along with better resources, which helps reduce the problem.
Meanwhile, physicians like Nuttall are put in impossible situations at Red Cross.
“When doing blood tests on an infant to check for infection, you can’t wait for those results. You have to start treatment with what you think is the appropriate treatment. That’s the empirical treatment,” explains Nuttall.
“Then, when you isolate a bacterium and know its resistance profile (or antibiotic susceptibility profile), you must redirect your treatment to what’s known as ‘directed’ or definitive treatment. But there’s now been a time gap of 24 to 72 hours where the infant is on treatment, and you don’t know if it’s the right treatment. That’s a critical issue, because the baby might deteriorate in that time because they’re not on the right treatment,” he says.
He says the choice of empiric antibiotics is becoming more difficult, “as what we previously used as empiric antibiotic treatment is less and less reliable to treat serious infections, particularly in patients who acquire resistant infections in hospital”.
In a position paper, Nuttall and his colleagues write that growing antibiotic resistance is linked to the increased use of “reserve” and “watch” antibiotics. The WHO classifies antibiotics into three groups. Access antibiotics are the common ones used to treat everyday infections in the community. Watch antibiotics are broad-spectrum antibiotics that carry a higher risk of causing resistance, so their use must be carefully monitored and limited. Reserve antibiotics are last-resort treatments for infections caused by multi-drug-resistant bacteria and should only be used when all other options have failed.
‘Totally underestimated’
Following the research described earlier, Madhi says they convened an expert panel, to deliberate on what the causes of death was in children.
Unfortunately, he says, it’s become completely monotonous in that there’s a clear series of events for children born prematurely, who die: They’re admitted to hospital, they usually require ICU, they improve in ICU, and two to three days later, they appear very sick again. “Often you don’t actually identify the bacteria causing the clinical deterioration when you investigate ante-mortem, and you only realise the child actually succumbed to antimicrobial resistant bacterial infections after you’ve done the postmortem sampling”. Postmortem sampling is not done systematically across the country.
“What the post-mortem sampling has unmasked, is that we’ve totally underestimated the contribution of antibiotic-resistant bacteria in relation to causes of neonatal death. If we were to do the same investigations in other facilities, there would be much greater heightened awareness of what is really an unrecognised endemic public health crisis across our healthcare facilities,” says Madhi.
Professor Angela Dramowski, Head of the Clinical Unit: General Paediatrics at Tygerberg Hospital, agrees that outbreaks in low- and middle-income country hospitals, including South Africa are under-reported.
“What we see in the literature and in the headlines of newspapers is the tip of the iceberg. The vast majority of outbreaks in fact are either undetected or unreported. This is almost an invisible problem because a lot of the deaths are currently labelled due to another cause, for example, prematurity.
“This is a crucial public health crisis. We cannot practice modern medicine without effective antibiotics, and, especially for newborns the situation is perilous as we have very few effective treatment options left.”
‘Existential threat’
Though more acute in some areas, the problem is a global one. Marc Mendelson, Professor of Infectious Diseases at the University of Cape Town, describes antibiotic resistance as an existential global health threat.
“If antibiotic resistance is not mitigated, in the next 25 years, 39 million people globally will die of an antibiotic-resistant bacterial infection. That will dwarf HIV, tuberculosis, and malaria,” he says.
“There are bacteria currently causing infections in our hospitals in South Africa that are totally resistant to antibiotics. Those patients would usually die or need extraordinary measures to keep them alive such as amputating a limb to remove the infection in a bone or joint,” Mendelson says.
“People have always assumed if you get sick with a bacterial infection, there will be an antibiotic to treat it. Doctors in and out of hospitals have been too lax in how they prescribe antibiotics. Now we’re paying the price as some bacterial infections are not easily treatable,” he says.
As Dramowski points out, there is a lot of good science confirming the extent of the problem. A systematic review published in The Lancet found that almost 5 million deaths in 2019 were associated with bacterial infections resistant to antibiotics.
“That huge number is more than deaths from HIV and malaria combined,” she says.
Dramowski also points to another review study that found 3 million cases of neonatal sepsis globally each year, with at least 570 000 deaths (likely an underestimate). Over 95% of deaths from neonatal antibiotic resistance occur in low- and middle-income countries (LMICs).
“In a nutshell, in five big studies … they showed that antibiotic resistance to the World Health Organization-recommended antibiotic treatments ranges anywhere between 40 to 70%, so almost half of all babies with severe bacterial infection have resistance to the recommended antibiotic treatment,” she says.
What to do?
To address the major issue of antibiotic resistance in infants, Dramowski stresses the importance of prevention. This includes improving Water, Sanitation, and Hygiene (WASH) as well as Infection Prevention and Control programmes to reduce the spread of antibiotic-resistant bacteria in communities and healthcare facilities. She also stresses the need to prevent pre-term births as much as possible, as hospital admissions carry a high risk of acquiring antibiotic-resistant bacteria and developing infections.
She says increased surveillance of infections in LMICs is also crucial, along with more antibiotic trials to provide better alternatives. Additionally, there is a strong need for responsible antibiotic use (stewardship) to ensure they are only used when necessary, helping to prevent the development of antibiotic resistance.
A challenge in practicing stewardship is the difference in resources between the public and private sectors, says Professor Vindana Chibabhai, Head of the Centre for Healthcare-associated Infections, Antimicrobial Resistance, and Mycology (CHARM) at the National Institute for Communicable Diseases. Expensive antibiotics are more easily accessible in the private sector, while they are often not available in the public sector.
“Antibiotic stewardship is happening all over the country but we need to have a national monitoring system,” she says.
Chibabhai says that private sector clinicians often work independently and are not required to follow stewardship programmes as strictly as those in public sector hospitals. To address antibiotic resistance, she says we need monitoring systems to track the effectiveness of these programmes and provide support to hospitals struggling with them. Even though some hospitals have dedicated pharmacists, microbiologists, and clinicians, Chibabhai says they may need additional help to strengthen their antibiotic stewardship efforts.
‘Lots of lovely paper’
A major issue highlighted by experts is the lack of a clear AMR strategy in South Africa. The last strategy, which covered 2019 to 2024, was not funded, and its impact has not been evaluated.
“We have lots of lovely paper and lots of committed people doing great work but in terms of interventions, none of it is funded,” says Mendelson, who chaired the Ministerial Advisory Committee on Antimicrobial Resistance for the eight years until 2022. “If these interventions were funded, we could save lives.”
Madhi says the consequences of not implementing South Africa’s AMR plan are exactly what we are seeing now. “The problems have become endemic and entrenched in public healthcare facilities and lead to large numbers of unnecessary deaths which could have been prevented if we implemented a proper strategy in place.”
He says the situation now calls for a multi-faceted approach. “It’s not just about the type of antibiotics that should be available but about mitigating the many contributing factors that resulted in these outbreaks. That requires immense investment in terms of resources and expertise.”