A new study from the University of Minnesota Medical School demonstrated that faecal microbiota transplantation (FMT) can rapidly reverse systemic inflammation and improve survival in patients with fulminant Clostridioides difficile (C. difficile) infection – a life-threatening condition characterised by a sepsis-like state. The findings were published in Clinical Gastroenterology and Hepatology.
C. difficile infection is the most common cause of healthcare-acquired diarrhoeal illnesses. Most of the mortality, estimated at 15 000 people annually in the United States alone, is associated with the severe and fulminant forms of the disease. C. difficile is listed as one of the most urgent infectious disease threats by the Centers for Disease Control and Prevention. The infection occurs in people with disrupted microbial communities in the gut, most commonly by antibiotic medications.
In this study, investigators implemented a standardised FMT protocol developed at the University of Minnesota specifically for critically ill patients who were deteriorating despite intensive antibiotic therapies and were often too unstable for surgery. Among 18 patients treated, FMT was associated with rapid declines in inflammatory markers and achieved a 78% 30-day survival.
“There is an important caveat to our findings – the window for the FMT intervention is very narrow because these patients are generally extremely sick,” said Alexander Khoruts, MD, professor at the University of Minnesota Medical School, director of the UMN Microbiota Therapeutics Program and a gastroenterologist with M Health Fairview. “Therefore, the FMT formulation needs to be easily accessible. We are in a unique position at the University because we have a facility in our institution where our FMT products are manufactured in accordance with pharmaceutical standards, and treatment units are always on hand in our cryobank.”
The University of Minnesota Microbiota Therapeutics program is the leading program in the world in developing microbiome-targeted therapies with live microbial communities. As a result of the team’s work, M Health Fairview recently implemented a dedicated system that alerts providers to hospitalized patients at risk of developing severe C. difficile infection so that they can get access to the optimal treatments earlier.
Importantly, the findings also suggest an entirely novel mechanism by which FMT can modulate systemic inflammation in severe C. difficile infection. This is a topic of ongoing research. The team is also currently working to make this FMT treatment option more widely available to patients across the United States.
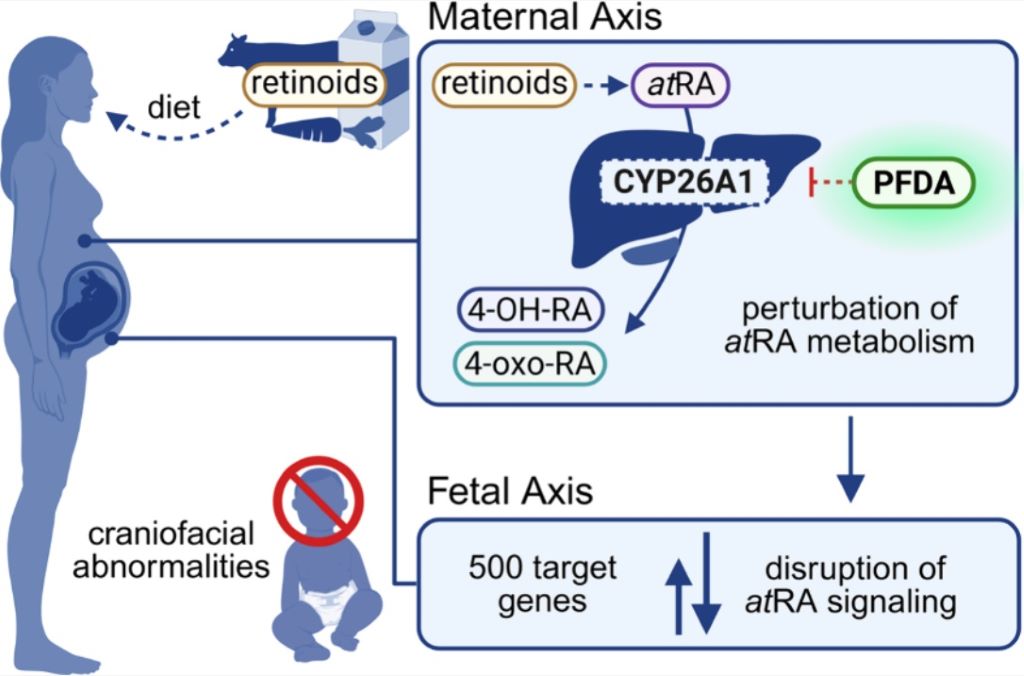
Researchers discovered perfluorodecanoic acid is the most toxic during foetal craniofacial development
Credit: Chemical Research in Toxicology (2026). doi:10.1021/acs.chemrestox.5c00468
Researchers have long associated per- and polyfluoroalkyl substances (PFAS), commonly known as “forever chemicals,” to certain severe birth defects but exactly how these pollutants harm a developing foetus has remained mostly a mystery. New research now provides the first clear molecular explanation, showing how one PFAS, called perfluorodecanoic acid (PFDA), can trigger craniofacial abnormalities before birth.
“Most people are exposed to small amounts of PFAS in everyday life but higher exposure can occur through contaminated water, living near manufacturing sites or certain jobs like firefighting and ski waxing, which is why it’s so important to understand the chemicals better,” said the paper’s senior author Jed Lampe, PhD, associate professor at University of Colorado Anschutz Skaggs School of Pharmacy and Pharmaceutical Sciences. “We wanted to understand which PFAS compounds are truly harmful during foetus development, especially for people with higher exposure, and how they cause damage.”
There are approximately 15 000 PFAS used in consumer and industrial products but scientists are increasingly finding that only some pose serious health risks. In this study, Lampe worked with the paper’s first author Michaela Hvizdak and co-author Sylvie Kandel to test 13 commonly found PFAS and discovered PFDA as the most toxic during foetal craniofacial development.
They demonstrated a possible link between PFDA and the extensive facial changes observed in humans and laboratory animals, with some estimates indicating a 10% increased risk at extremely low exposure levels.
“This finding moves us beyond association by providing a clear explanation for how PFDA can interfere with foetal development. It’s a critical step toward understanding a vast and complex class of environmental chemicals,” said Lampe.
The cause of underdeveloped eyes and an abnormal jaw
They found that PFAS disrupts retinoic acid, a molecule essential for shaping the face and head during early pregnancy. Retinoic acid regulates hundreds of genes and its levels must be controlled. Because a foetus cannot produce or safely eliminate excess retinoic acid, it relies entirely on the mother to maintain the homeostatic balance of the hormone.
The researchers discovered PFDA blocks CYP26A1, a key enzyme responsible for breaking down excess retinoic acid. When this enzyme is inhibited, retinoic acid levels can rise too high, disrupting normal facial development. PFDA also suppresses the genes that produce this enzyme through a separate biological pathway, delivering a “double hit” to the system that regulates early development.
“As a result, severe craniofacial abnormalities can develop, including underdeveloped eyes and abnormal jaw formation, which were the most common effects of PFDA exposure during foetal development,” said Lampe.
The researchers hope by providing a molecular explanation for this abnormality that the research and scientific community can work to develop targeted laboratory assays and computer‑based screening tools to quickly rank PFAS by risk. They say this could help regulators and manufacturers distinguish more dangerous compounds from safer alternatives and guide the design of less toxic chemicals in the future.
They also hope the research can open the door to practical interventions for people with higher exposure, such as firefighters and ski wax technicians. This could include looking into how to reduce exposure levels and whether strategies can be developed to lower PFDA during pregnancy to protect foetal development.
In a study of US adults, walking was, by far, the most popular leisure-time physical activity, while rural residents also enjoyed gardening, hunting and fishing, and urban residents more commonly reported running, weightlifting and dance. Urban residents were more likely than rural residents to meet physical activity guidelines. Christiaan Abildso of West Virginia University, US, and colleagues present these findings in the open-access journal PLOS One on April 1, 2026.
The US Department of Health and Human Services publishes guidelines on recommended amounts of aerobic and muscle-strengthening physical activity for adults. While the overall proportion of U.S. adults meeting these guidelines has increased in recent decades, certain populations are less likely to meet them, including adults living in rural areas. Understanding differences in preferred recreational physical activities could help inform efforts to reduce such disparities.
However, few studies have examined urban versus rural preferences for leisure-time physical activities, and how they relate to meeting guidelines. To address that gap, Abildso and colleagues analysed telephone survey data collected from a national sample of 396 261 U.S. adults in 2019.
Out of 75 survey options for leisure-time physical activities, walking was the most popular among both urban and rural adults, with 44.1% reporting walking as the activity they spent the most time doing. This finding echoes a similar study of U.S. data collected in 2011, which also found walking to be the top activity. However, further analysis of the 2019 data showed that even among walkers, only 25% met combined guidelines for aerobic and muscle-strengthening physical activity, and about 22% did not meet either guideline.
The popularity of other activities varied. For instance, rural residents reported higher rates of gardening, hunting, fishing, and farm work, while urban residents had higher participation in running, weightlifting, bicycling, and dance. However, in general, rural adults were more likely to be inactive and less likely to meet guidelines for aerobic or muscle-strengthening physical activity.
These findings could help inform efforts to boost physical activity by tailoring solutions to be more culturally and demographically appropriate. The researchers also call for a similar analysis of more recently collected data, as habits may have shifted during the COVID-19 pandemic.
Christiaan Abildso adds: “We expected to see that walking would continue to be the most common physical activity. However, it was surprising to see that nearly 1 in 4 adults who walk as their main activity did not meet either of the physical activity guidelines. That is, they reported less than the recommended 150 minutes per week of moderate-intensity aerobic activity and less than the recommended 2 days per week of muscle strengthening activity, such as yoga or exercises with resistance bands.”
“What we might be seeing in these rural-urban differences in preferences may just reflect what people have access to or what is culturally supported. In our work, we see a need to continue to support our partners in small towns and rural places by creating physical, social, and cultural conditions that support physical activity. This could mean creating a wide shoulder on a country road for running and cycling, helping a senior centre with their chair exercise programming, creating or improving park spaces, expanding the national network of rail-trails, renovating abandoned and dilapidated structures (Brownfields) into viable activity centres, keeping school facilities open to the public, and many other strategies. Everyone needs to ask, ‘how does what we’re doing affect physical activity,’ in order to help get people more active, more often, in more places.”
Analysis of nearly 7 billion Taco Bell transactions finds sugary drink taxes not linked to lower beverage calorie purchases
Photo by Breakingpic on Pexels
Taxes on sugary drinks had no effect on beverage calorie purchases from fast-food chain restaurants in the U.S., according to a new study by Brian Elbel and Pasquale Rummo from NYU Grossman School of Medicine and colleagues publishing April 2nd in the open-access journal PLOS Medicine.
Sugary drink taxes have been adopted in several U.S. jurisdictions as a public health strategy to curb sugar consumption and improve dietary behaviors. Research on the impact of these taxes on grocery stores purchases attribute sugary drink taxes to an estimated 15% decrease in sales. However, whether this translates to an impact in restaurant sales has not been well studied.
Researchers analyzed six years of sales data (2015–2020) from more than 7,300 Taco Bell locations nationwide, focusing on drive‑through purchases. The study compared beverage calories per transaction at 60 restaurants across five jurisdictions with sugary drink taxes—Albany, California; Cook County, Illinois; Oakland, California; Philadelphia, Pennsylvania; and Seattle, Washington—with a matched group of similar restaurants in areas without such taxes.
Overall, the analysis found no significant association between sugary drink taxes and beverage calories per transaction, suggesting that sugary drink taxes of this size or alone may not substantially reduce beverage calorie consumption in fast food restaurant settings.
The authors note that consumer behaviour in restaurants—such as choosing combo meals or prioritising convenience—may limit the effectiveness of these policies.
Elbel adds, “Using millions of transactions from six years of sales data, we found that sugary beverage taxes did not influence beverage calories when implemented in five cities in the U.S.”
Rummo notes, “These results suggest that sugary drink taxes may not be effective in reducing beverage calorie consumption in fast food restaurants, as compared to supermarkets. This could be because the sizes of sugary drink taxes in the U.S. are too small for consumers or that they just aren’t responsive to price changes in these settings, among other reasons.”
Houston Methodist researchers find antibiotics aid recovery from traumatic brain injury
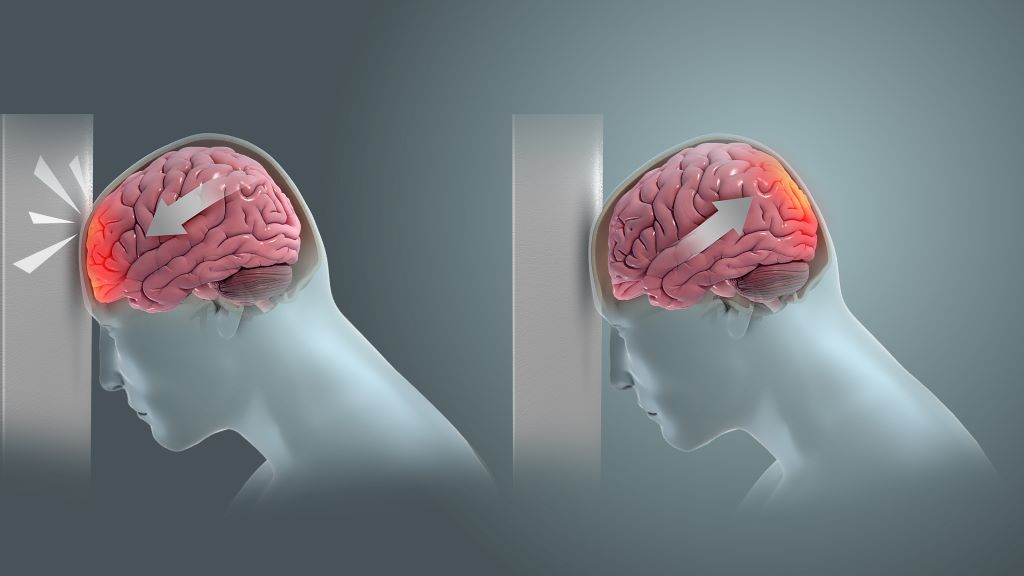
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
In a new study published in Nature Communications Biology, Houston Methodist researchers led by Sonia Villapol, PhD, found that short-term antibiotic treatment significantly reduced neuroinflammation and neurodegeneration following traumatic brain injury (TBI) by altering the gut microbiome in animal models.
“We found that antibiotic treatment following TBI can reduce harmful gut bacteria, decrease lesion size and limit cell death,” said Villapol, an associate professor in the Department of Neurosurgery at Houston Methodist. “Our results support a gut–brain mechanism in which microbiome changes influence peripheral immunity and, in turn, neuroinflammation after TBI.”
Administering antibiotics cleans the gut of harmful bacteria, allowing beneficial bacteria to flourish. The study found that two helpful bacteria, Parasutterella excrementihominis and Lactobacillus johnsonii, are key to driving cell repair. According to Villapol, they could also be major regulators for peripheral inflammation in the body.
Notably, 70% of immune system regulation is generated by the gut microbiome. During gut imbalance, the bidirectional nature of the brain-gut axis can wreak havoc throughout the entire body.
“Our brains are constantly sending signals to the rest of our bodies. Following a traumatic brain event, those signals can get scrambled and disrupt other organs, including our digestive system,” Villapol said. “If the gut stays out of balance, the brain may have a harder time healing.”
There are an estimated 4 million traumatic brain injuries a year in the U.S. Recent studies indicate that TBI-induced gut microbiome imbalance may even contribute to the development of neurodegenerative diseases like Parkinson’s, Alzheimer’s and dementia.
Villapol’s lab is focused on investigating and developing new neuroprotective treatments to fight inflammation linked with neurodegenerative disease. “If we can break neuroinflammation in the acute or chronic stage, we can reduce the risk of developing Alzheimer’s or dementia,” said Villapol.
The next phase of the research will focus on bioengineering Parasutterella excrementihominis and Lactobacillus johnsonii to further develop precision therapies to reduce neuroinflammation.
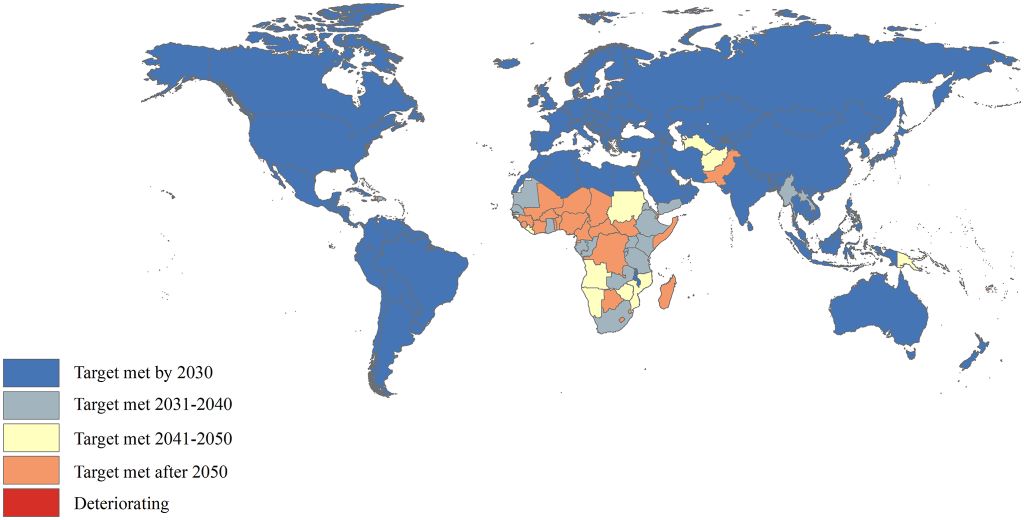
Despite a 63% drop in under-five deaths since 1990, more than a quarter of countries won’t reach the UN’s 2030 child mortality target on time, with sub-Saharan Africa lagging the most
Years in which the U5MR reduction target is expected to be achieved. U5MR: under-5 mortality rate. Image credit: Cao et al., 2026, PLOS One, CC-BY 4.0
A new study tracking global progress on child mortality finds that the world will miss a key United Nations (UN) health target by at least five years at current rates, with the burden falling heavily on Sub-Saharan Africa. The findings are published on April 1, 2026, in the open-access journal PLOS One by Min Liu of Peking University, Beijing, China, and colleagues.
The UN’s Sustainable Development Goal 3.2 calls for all countries to reduce the mortality rate for children under five to fewer than 25 deaths per 1000 live births by 2030. As that deadline approaches, there has been no comprehensive assessment of where countries stand.
In the new study, researchers used data from the UN to analyse annual under-five death counts and mortality rates from 1990 to 2023 across 200 countries and territories. They calculated the rate of change in mortality over time and used those trends to project when those countries still above the target threshold would be expected to reach it.
The researchers found that globally, under-five deaths fell by 63% over the study period – from nearly 13 million in 1990 to 4.78 million in 2023 – and the mortality rate dropped by an average of 3.18% per year. However, the global rate still stands at 36.72 deaths per 1000 live births, well above the SDG target, and is not projected to reach the target until 2035. 133 countries have already met the target and nine more are on track to do so by 2030. However, 58 countries will miss the deadline, including 25 that are not projected to reach the target until after 2050, and Dominica, where under-five deaths have risen. More than four-fifths of all under-five deaths worldwide are concentrated in just two regions: Sub-Saharan Africa, where the mortality rate remains at 68.82 deaths per 1000 live births and is not projected to meet the SDG target until 2055, and Central and Southern Asia.
The study is limited by the assumption that trends over the last two decades will continue unchanged. Data quality was also poor in some conflict-affected regions and low-income countries, the very places where child mortality is highest.
The authors conclude that to meet UN targets, policymakers must focus on scaling up proven interventions – including skilled birth attendance, postnatal care, vaccination, improved nutrition, and treatment for common childhood illnesses – in every community, and especially in Sub-Saharan Africa.
The public health sector serves roughly 84% of South Africans, yet per-person spending in private healthcare is around five times higher. The National Health Insurance (NHI) is designed to change that equation. As President Ramaphosa stated, the right to healthcare “cannot depend on where you were born, how much you earn or where you live.”
For patients with blood cancer and blood disorders, that promise could not be more urgent. On World Health Day 2026, Palesa Mokomele, Head of Community Engagement and Communication at DKMS Africa, says this is an opportunity to ask whether the NHI is being designed to reach them. “Blood cancer and blood disorder patients depend on highly specialised treatment pathways – exactly the kind the NHI has an opportunity to strengthen. They cannot be an afterthought in the benefit package conversation.”
The NHI Act was signed into law in May 2024 but has not yet commenced, with key constitutional challenges set to be heard in May 2026. Despite legal uncertainty, the government has been clear that foundational work will continue.
The Reality on the Ground
Stem cell transplantation is one of the most effective treatments for blood cancers and blood disorders, and among the most resource-intensive, requiring specialist physicians, trained nurses, dedicated infrastructure, and in 70% of cases, a matched unrelated donor (MUD).
The capacity to deliver these treatments is already under severe strain. Just 25% of South Africa’s oncologists serve more than 75% of the population. Long treatment delays, limited resources, high patient volumes, and advanced disease at presentation make for a deeply challenging environment.
“What we see is a system doing its best under enormous pressure,” says Mokomele. “The NHI has a real opportunity to address those structural gaps, but it requires deliberate investment where the need is greatest.”
What Universal Coverage Must Include
The NHI benefit packages for the treatment of blood cancer and disorders have yet to be finalised. With South Africa projected to see a 78% increase in cancer incidence by 2030, whether those packages cover the full cost of finding, matching, and transplanting an unrelated donor will be a test of whether universal health coverage means what it says.
“We are not here to debate the merits of the NHI,” shares Mokomele. “We are here to make sure that when it is implemented, it works for every patient. The full treatment pathway must be funded, and the clinical infrastructure to deliver it must be in place.”
President Ramaphosa has called for genuine partnerships between the public and private health sectors, academic institutions, NGOs, and communities. “That vision of cross-sector collaboration reflects exactly how we believe this challenge must be met,” notes Mokomele.
A Blueprint for Access
DKMS Africa’s Access to Transplant programme offers a practical example of barrier-free access in the public sector. Working across six provinces, it aims to invest in infrastructure upgrades at public hospitals, training for specialist nurses and mobilises its global network to collaborate with physicians, and patient support services addressing practical barriers, such as transport and housing, that often cause patients to abandon treatment.
“When you remove barriers systematically, outcomes improve,” points out Mokomele. “Each barrier removed is a patient who makes it to transplant. That is the model the NHI needs to learn from and scale.”
The organisation is also preparing for a more centralised system, ensuring its programmes can integrate into national frameworks while maintaining global standards – through early diagnosis education, donor registry diversification, stronger referral pathways, and local research capacity.
Your Health System, Your Voice
The decisions being made about the NHI benefit package today will shape healthcare for decades. Young South Africans will inherit both the growing burden of disease and the system designed to address it.
“World Health Day is a reminder that universal means everyone,” concludes Mokomele. “We are asking young South Africans to support us in uniting towards a healthcare system that works for everyone.”
Real-world trial finds long-lasting benefit for TENS with physical therapy in reducing movement pain, fatigue
Credit: University of Iowa
Adding TENS (transcutaneous electrical nerve stimulation) to outpatient physical therapy reduced movement-based pain and fatigue in patients with fibromyalgia, and the effects lasted for at least six months, according to a new study led by researchers at University of Iowa Health Care.
“It is one of the few treatments that specifically targets movement-evoked pain and fatigue, which are major barriers to participation in daily activities,” says Sluka, UI professor of physical therapy and rehabilitation science.
TENS uses a small device with adhesive electrodes to send mild electrical pulses through the skin to block or reduce pain. The study found that the effect of TENS for reducing pain was similar, if not better, than current FDA-approved medications for fibromyalgia.
“We were excited to see that patients also had less fatigue,” Sluka added. “Right now, there are no good treatments for fatigue. So, the fact that we had anything that touched the fatigue was pretty powerful.”
Fibromyalgia: complicated, misunderstood, and hard to treat
Fibromyalgia affects about 4% to 7% of the population. It significantly impacts a person’s physical function, cognitive abilities, and sleep. In addition to chronic pain, a key feature of the condition is whole-body fatigue, which interferes with day-to-day life and contributes to patients’ inability to concentrate and perform functional activities.
Exercise is often the first line of treatment recommended to people with fibromyalgia, and research has shown that it can be beneficial. However, fibromyalgia causes fatigue and pain, which is a key reason why the research team focused on alleviating pain with movement.
“Pain with movement hinders a person’s ability to participate in an effective exercise program and do their day-to-day activities.” Sluka says.
Science translated to real-world benefit
Sluka and her colleagues have spent decades studying the biological mechanisms affected by TENS, developing the ideal parameters of TENS stimulation and testing the efficacy of TENS for treating chronic pain and fatigue in human trials.
They have previously shown that under the ideal conditions of a randomized, controlled clinical trial, TENS in conjunction with physical therapy can significantly decrease movement pain.
The new Fibromyalgia TENS in Physical Therapy (FM-TIPS) study was designed to test the effect of TENS under real-world conditions. The study was conducted in 28 outpatient physical therapy clinics across six health care systems in the Midwest, and included 384 people of different ages, education levels, and socioeconomic backgrounds. Almost 50% of the participants were from rural areas.
“It was a challenge to recruit participants for this study, but the clinics and the physical therapists we worked with were great. This would never have happened without them,” Sluka says.
The clinics were randomised to provide either physical therapy (PT) with TENS or physical therapy alone. In the PT-TENS group, participants were asked to use TENS for two hours a day for six months. That time could be split into short periods or done all at once. The TENS electrodes were placed on the upper and lower back and delivered a mixed frequency signal at an intensity as strong as the participant could tolerate.
After 60 days, movement-evoked pain during TENS treatment was significantly improved in the PT-TENS group. Adding TENS also significantly reduced resting pain and resting and movement-fatigue. In contrast, participants who received only physical therapy had no change in their movement-evoked pain.
When we gave the PT-only patients the TENS unit and they started using it, we also saw the same improvements as the PT with TENS patients, which is powerful. – Kathleen Sluka, PT, PhD
The response also was dose-dependent, with people who used TENS daily for 60 days having the best outcomes.
Unlike many pain-relieving drugs that can become less effective over time as the body develops a tolerance for the medication, the study shows that over time, TENS maintained its ability to improve pain and fatigue at a significant level.
After the primary endpoint at day 60, the PT-only group was also given TENS, and all the participants continued in the study for another four months.
“When we gave the PT-only patients the TENS unit and they started using it, we also saw the same improvements as the PT with TENS patients, which is powerful,” Sluka says.
Overall, the study showed that 80% of patients found TENS helpful. At six months, 80% were still using TENS once a week, and over 70% reported they felt better after using TENS.
TENS adds benefit
Dana Dailey, PT, PhD, UI assistant research scientist and the first author of the study, notes that it’s important for people to realize that the benefit of TENS comes from using it as a part of a total treatment plan that includes physical therapy.
“Using TENS on its own will not give the same benefits,” Dailey says. “However, the study shows that TENS provides an added benefit on top of any relief from other treatments. All the study participants were also using pain medications and receiving physical therapy, yet TENS still provided additional relief.”
Fibromyalgia often needs multiple interventions to help patients feel less pain and fatigue and improve their overall function. The new findings suggest that TENS could be particularly helpful as a part of a multipronged approach because it can be safely and easily used as a self-management tool that uniquely targets movement-associated pain and fatigue.
“Often, when you move a randomised, controlled clinical trial into a real-world setting, it doesn’t work because there are too many confounding factors. But this intervention still works,” Sluka says. “Not only did the treatment reduce movement pain and fatigue during the testing period, but patients continued to use it at six months.”
Autism has a significant and enduring sex bias, with roughly four boys diagnosed for every girl. For many years, experts have believed this disparity arises primarily from diagnostic inequities because much of autism research – and the screening tools that grew out of it – has historically focused on boys, effectively setting a male standard for what autism “looks like.” As a result, girls and women are more likely to be overlooked, misdiagnosed, or diagnosed much later in life.
This disparity has also shaped the science around autism. When fewer females with the condition are identified, fewer are included in research studies, creating a feedback loop where scientific understanding of autism in females remains limited. Because of this underrepresentation of females, it has been difficult for scientists to disentangle how much of the sex bias in autism reflects social inequities versus underlying biological differences between the sexes.
While the search for biological explanations has largely lagged behind, one leading theory, known as the “female protective effect,” proposes that females may be biologically buffered against developing autism in a way males aren’t.
The idea can be traced back to studies showing that females diagnosed with autism tend to carry a higher number of genetic mutations or “hits” than males with the condition, meaning that they require a higher load of the same genetic mutations for autism to manifest. But, until now, there’s been little clarity on the exact biological mechanism behind this apparent resilience.
Now, a perspective from the lab of Whitehead Institute Member David Page, published March 30 in Nature Genetics, proposes a genetic explanation for the female protective effect and suggests that biological differences between males and females contribute to autism’s strong sex bias.
The work is one of many projects from the Page lab uncovering the biological underpinnings of sex bias in everything from heart health and autoimmune disease to certain cancers.
“The fact that we see sex biases in disease all across the body gives credence to the notion that the sex bias in autism isn’t simply emerging from diagnostic inequities and gendered expectations of what the conditions looks like,” says Page, who is also a professor of biology at Massachusetts Institute of Technology and an investigator at the Howard Hughes Medical Institute (HHMI).
The researchers propose that this protective effect extends beyond autism, and could help explain why 17 other congenital and developmental disorders predominately affect males. By characterizing the biological factors that make one sex more or less likely to develop certain health conditions, scientists see an opportunity to improve how these conditions are diagnosed and how people receive care.
“The fact that we see sex biases in disease all across the body gives credence to the notion that the sex bias in autism isn’t simply emerging from diagnostic inequities and gendered expectations of what the conditions looks like,” says Page.
Page and Harvard-MIT MD-PhD student Maya Talukdar trace the female protective effect to the X chromosome. Talukdar is a graduate student in Page’s lab and the lead author of the perspective.
Most females have two X chromosomes (XX) while most males have one X and one Y chromosome (XY). Sex chromosomes can dial up and down the expression of thousands of genes on the other 22 pairs of chromosomes in a cell, impacting cell function across the entire body.
Historically, scientists believed that the second X chromosome in females is largely inactive. But, in recent years, research out of the Page lab has shown that the so-called “inactive X,” also called Xi, plays a crucial role in regulating gene expression on the active X chromosome, and the rest of the chromosomes.
In this perspective, the researchers point to a subset of genes that are expressed from both the active and inactive X chromosome — often known as genes that “escape” X chromosome inactivation. Many of these genes are dosage-sensitive regulators of key cellular processes. These processes influence thousands of other genes across the genome, including many linked to autism.
Because females have an extra copy of these regulatory genes expressed from Xi, Page and Talukdar propose that they may be better able to buffer the effects of autism-associated mutations than males.
The female protective effect beyond autism
This mechanism, the researchers say, extends beyond autism to a range of congenital and developmental diseases with a male bias.
“Many of the other congenital or developmental conditions we’re pointing to aren’t subject to diagnostic inequities in the way autism is,” says Talukdar. “This strengthens the idea that the female protective effect is emerging from genetic differences in males and females.”
One example is pyloric stenosis, which like autism, affects four boys for every girl. Infants with the condition experience severe vomiting due to thickening of the pyloric sphincter, the passage between the stomach and small intestine. As with autism, girls with pyloric stenosis appear to require more genetic “hits” in order to develop the condition.
The researchers’ new framework of looking at Xi to understand sex differences in disease could impact treatment and care not just for conditions that predominately affect males, but also for those that are more common in women, such as autoimmune diseases.
“Our biology isn’t one-size-fits-all,” Talukdar says “Sex differences clearly play a huge role in health, and it’s so important that we understand them.”
Many regions in the Northern Hemisphere experienced a slightly earlier start to their flu season, driven in some part by a novel variant of influenza A(H3N2). As our flu season also kicks off slightly earlier than usual, Spotlight reports on the detection of this variant in South Africa and what we might expect from this year’s flu season.
As the mercury slowly starts dropping across the country, so does the risk of picking up flu. For many, this might only mean a few days of illness and discomfort, but for some, especially the elderly, it can be life-threatening.
Despite temperatures throughout most of the country remaining moderate so far, this year’s flu season has started, somewhat ahead of schedule. This is according to the National Institute for Communicable Diseases (NICD) in a press release issued on Wednesday.
What we refer to as flu, is commonly caused by one of two types of influenza viruses, influenza A and influenza B. These two are further typed into different lineages, the most common for influenza A is A(H1N1) and A(H3N2) and for influenza B, the B-Victoria and B-Yamagata.
The Yamagata lineage has not been detected since 2020 and is thought to have gone extinct, said Dr Sibongile Walaza. She is a medical epidemiologist and head of epidemiology at the Centre for Respiratory Disease and Meningitis at the NICD.
A key reason why influenza viruses continue to circulate year after year is how fast they mutate and learn to dodge our immune defenses. These mutations eventually result in different subtypes of lineages that are called clades, within which there can be further sub-clades.
It was a sub-clade of the A(H3N2) virus, known as sub-clade K, that led to the flu season starting earlier than usual in some parts of the Northern Hemisphere. The World Health Organization (WHO) reported that the variant was identified in 2025 and spread fast.
“This [sub-clade] contributed to an earlier start to the influenza season in many countries, with several reporting higher‑than‑usual levels of activity. ‘Subclade K’ accounted for the majority of influenza viruses reported across regions,” the WHO stated in a press release.
Sub-clade K was also responsible for an unusual spike in flu cases in South Africa in October and November 2025. Walaza told Spotlight there weren’t enough flu cases detected to cross the seasonal threshold for an additional flu wave, but the increase so late in the year, outside of the typical flu season, was unusual.
Early start
Usually, South Africa’s flu season starts sometime in April or May and spans the winter months, said Walaza, but it is difficult to predict exactly what will happen in any particular year.
This year’s flu season officially started in the second week of March, according to the NICD’s latest report, albeit at a low transmission level for now. 134 samples were tested between 16 and 22 March. Of those, 12 (9%) tested positive for influenza, 12 (9%) were cases of RSV and 3 (2.2%) tested positive for SARS-CoV-2.
In a rather unusual occurrence, the NICD reported that the start of this year’s RSV season coincided with that of the flu season. RSV refers to respiratory illness caused by the Respiratory syncytial virus. The RSV season usually starts before the flu season, but infections can occur all year round.
“The fact that both the flu and RSV seasons are starting at the same time means clinicians could potentially see a high burden of patients with respiratory illness in medical facilities in the coming weeks,” the NICD said in the press release.
Two potential scenarios
Professor Tulio de Oliveira, the director of the Center for Epidemic Response Innovation at Stellenbosch University, said the reality is that we do not know what to expect for this year’s flu season.
“[At]t the moment, we are working with potentially two different scenarios,” he told Spotlight.
The one scenario is that we may be in for a more extreme flu season, he explained, since last year was an unusually mild season and population immunity against the viruses that cause flu may currently be lower. The other scenario, depending on which flu virus circulates, is that South Africa may have some herd immunity because of the unusual spike in flu cases near the end of last year.
In other words, it all comes down to which flu viruses, and their subtypes end up circulating.
“I think this year we’ll have the three influenza lineages [A(H3N2), A(H1N1)pdm09 and influenza B-Victoria] circulating, but in terms of which one is going to be dominant in the season, it’s difficult to tell in advance,” Walaza said.
What we know about sub-clade K
Based on what we’ve seen so far, it does seem that sub-clade K is more transmissible, but it doesn’t appear to cause more severe disease, according to Walaza. De Oliveira added that sub-clade K has between seven and 10 mutations on the surface protein that allow it to bind to a cell’s receptor and enter the body, making it more infectious.
Whether or not it will be the driver of our flu season this year remains to be seen, but Walaza said that within the sporadic cases of flu detected and sequenced so far this year, most of the cases have been sub-clade K. In an NICD report from March, of the 24 influenza samples that were sequenced between 29 December 2025 and 22 March 2026, 11 were confirmed as being sub-clade K.
Experts will be keeping a close eye on circulating flu viruses with real-time genomic surveillance.
“South Africa is considered to be one of the top virus genomic surveillance places in the world,” De Oliveira said. “[A]t the moment, we don’t see a big reason for concern [about the flu season],” he said. “We do genomic surveillance every week, both with public and private laboratories – and if we see anything unusual, that’s going to be highlighted very promptly.”
Trends seen in previous flu seasons
Overall, in the last ten years, influenza A seems to be the driver of the majority of flu cases in South Africa, said De Oliveira, usually causing a big wave of flu cases at the start of the season. This is usually followed by a smaller wave of influenza B cases. In this time period, the influenza A subtype that dominates during the flu season appears to alternate between A(H1N1) one year and A(H3N2) the following year, but it also doesn’t always follow this pattern.
Zooming in more closely, Walaza said that over the last six years, 2020 and 2021 were outliers, with reduced transmission during 2020 due to the measures taken to curb the spread of the SARS-CoV-2 virus and out of season influenza transmission in 2021. Since 2022, the number of people getting flu every year has returned to roughly similar levels as before 2020.
Last year’s flu season was slightly unusual since it had started in late March, according to Walaza, but wasn’t as intense as some of the previous years as transmission remained at a low threshold level. Flu cases peaked in mid-May and then rose again slightly in October and November.
Data on influenza comes from three sentinel monitoring programmes managed by the NICD, which cover both the public and private healthcare sectors, said Walaza. A sample of healthcare facilities in the public sector and doctors in the private sector are asked to supply swabs taken from people with influenza-like illnesses or respiratory illnesses. Some general practitioners in the private sector are also enrolled in a programme called Viral Watch.
She said that the swabs are sent to the NICD laboratory and tested for the presence of different viruses, including SARS-CoV-2, influenza, RSV, parainfluenza, human metapneumovirus and rhinoviruses. If the samples test positive for flu, the sample is further tested to identify the lineage. This data is included in the weekly reports published on their website.
Members of the public can contribute to flu surveillance through an online web platform called CoughWatch. People are invited to enroll and provide weekly information on whether they have symptoms of flu or other respiratory illnesses. This is aimed at picking up trends among people who aren’t necessarily getting sick enough to go to the doctor or clinic, said Walaza and can hopefully serve as an early warning system for increases in respiratory illnesses, including flu.
CoughWatch has already opened for enrollment this year. (More information can be found here).
Flu vaccination uptake in South Africa remains low
Each year, the WHO releases recommendations on what should be in upcoming flu vaccines for the Northern Hemisphere and then later the Southern Hemisphere, usually announced around six months before the start of the respective flu seasons.
This year’s flu shot’s formulation is a trivalent one, said Walaza meaning it contains inactivated strains of all three influenza strains, including coverage for the A(H3N2) sub-clade K. Because it contains an inactivated virus, the vaccine itself cannot give someone the flu.
The level of protection offered by flu shots vary, but generally it ranges in effectiveness against preventing infection from about 30% to 60%. This means the shot will offer most people protection from severe disease and death, but it won’t necessarily prevent them from getting sick with the flu altogether.
One of the things that makes it difficult to predict effectiveness ahead of time is the possibility that a strain might circulate that is not well covered by the flu shot. De Oliveira said this “mismatch” is what we saw play out in some of the regions in the Northern Hemisphere in their last flu season.
Despite the partial mismatch between the vaccine used in the northern hemisphere and sub-clade K, several surveillancereports from the Northern hemisphere show that the vaccine nevertheless provides some protection against severe flu caused by sub-clade K.
The WHO also recently touched on this, saying that: “While current influenza vaccines help reduce the burden of disease, their effectiveness can vary by season, product, and population group. Protection is limited to one season”. The majority of flu vaccines purchased each year are by upper-middle and high-income countries, the WHO noted.
Usually, South Africa’s National Department of Health procures about 1 million flu shots for the public health sector, said Walaza and sometimes not all these doses are used.
While flu shots are made available each year, the uptake of these shots in the private sector appears to be low. Based on data collected through the NICD’s Viral Watch initiative – last year the uptake of the influenza vaccine in the private sector, among those enrolled in the programme, was only around 3.4%. This is based on data collected from 768 people enrolled, of those, 26 had gotten a flu shot. As far as Spotlight could establish, there currently isn’t any routine publicly available data on uptake in the public sector. One study of around a thousand people aged 65 and older, found that just over 32% of them had gotten the flu jab in 2018.
Spotlight asked the National Department of Health how many flu vaccines were procured for this year’s flu season. A response had not been received by the time of publication.
Low flu vaccine uptake can in part be attributed to South Africa having much milder winters and less severe flu seasons than the Northern Hemisphere, said De Oliveira.
Lack of awareness of the flu vaccine can also play a role, according to Walaza. She encourages more education and efforts by healthcare workers to inform at risk groups of the flu shot and when it will be available.
The flu shot is recommended for people who are at risk of severe disease, including older persons, pregnant women, people who are immunocompromised or with chronic medical conditions, as well as healthcare workers. But anyone aged six months and older can get the shot.
“The influenza vaccine will be available in pharmacies from the first week of April. The early start to the season means that this year, the vaccine is only becoming available as the season is getting started, so members of the public who fall into groups at high risk for severe influenza are urged to get their vaccines as soon as possible,” the NICD press release stated.
The potential of next generation flu vaccines
Earlier this year, the WHO released results from an assessment report on the value of having improved flu vaccines. “If improved, next-generation, or universal influenza vaccines are available and widely used between 2025 and 2050, they could prevent up to [an estimated]18 billion cases of influenza and save up to 6.2 million lives globally,” the report stated.
“This assessment makes clear the potential benefits that improved influenza vaccines could offer across different settings,” said Dr Philipp Lambach, WHO technical lead of the project. “It provides all those working on future influenza vaccine investments, policy development and research priorities a common set of evidence to catalyse vaccine development.”
According to the WHO, as of February 2026, there are 46 next-generation influenza vaccines in clinical development.