A groundbreaking study by researchers at Rutgers Health has uncovered a way to precisely identify and target trauma sites in the body within minutes of injury. The findings, published in the journal Med (Cell Press), could revolutionise emergency care by enabling real-time diagnostics and site-specific treatments delivered within minutes of injury.
A team of scientists, led by Renata Pasqualini and Wadih Arap at the Rutgers Cancer Institute discovered something new about how the body reacts to injury. When cells are damaged, like in a major bone break, calcium levels shift, which causes certain proteins to change shape. These changed proteins, called the “traumome,” are only found in injured tissues and show up right after an injury happens. This discovery opens up a new way to treat injuries directly, without affecting healthy parts of the body.
“The moment trauma occurs, specific proteins undergo structural changes, creating a molecular footprint of injury,” said Arap. “This opens the door to delivering diagnostics or therapies directly to the site – without affecting healthy tissues.”
This discovery has relevance in emergency treatment because many medicines can affect healthy organs when they’re given too soon. With this new approach, doctors could deliver treatments like imaging agents, clotting factors or antibiotics directly to the injured area, which would help the body heal faster with fewer side effects.
“Our long-term vision is a simple injection that autonomously finds and treats injury sites,” said Pasqualini. “This could be transformative for battlefield medicine and emergency trauma care, where every second matters.”
The team used advanced testing on a pig model with major injuries to find tiny protein pieces called peptides. These peptides are like guides that can find and stick to the specific proteins altered by injury. One of these peptides stands out because it can attach to a protein that changes shape when calcium levels rise after an injury. This makes it possible to use special scans, like PET or MRI, to see exactly where the injury is in the body.
The trauma-targeting peptide worked the same way in rats, which shows that this injury “signature” is similar in all mammals, including humans.
The work was supported by the Defense Advanced Research Projects Agency (DARPA), an agency of the U.S. Department of Defense, underscoring its strategic value in both civilian and military medical applications. “Non-compressible bleeding remains a leading cause of death among soldiers before they reach a hospital, and localised treatment could dramatically improve survival rates, which was the original impetus of this research,” said Jon Mogford, a study co-author and former DARPA official.
The next phase of research will involve linking therapeutic agents to the trauma site-homing peptides and testing them in animal models before moving to early human clinical trials. The team envisions translational applications ranging from battlefield medicine to civilian trauma response and possibly even sports injuries or surgical recovery.
“We are actively developing peptide-linked drugs and imaging agents based on this discovery,” said Arap. “The traumome concept may also have applications beyond trauma, including in surgery, inflammation and tissue regeneration.”
In South Africa, men are four to five times more likely to die by suicide than women. The silence around men’s mental health has become a national crisis. Momentum Health is confronting the uncomfortable truth: traditional ideas of masculinity are costing South African men their lives. The need for a more inclusive and proactive approach to men’s health is urgent.
With men accounting for a staggering 37.6 suicides per 100 000 people2 and depression affecting over 27% of South Africans3, the economic and human cost of ignoring men’s overall wellbeing has reached a breaking point. Mental health-related absenteeism alone costs the economy billions every year, a price tag that extends far beyond financial metrics into affected families and communities.
“We’ve long lived in a society that praises men for physical strength but punishes them for emotional vulnerability. While this is slowly changing, it’s not happening fast enough to make real impact,” says Damian McHugh, Chief Marketing Officer at Momentum Health. “This is why we’re challenging South Africa to redefine what strength really means. True strength is not silently suffering; it’s having the courage to reach out before crisis hits.”
A New Narrative for Men’s Health
In many communities across South Africa, men delay seeking medical help until conditions become critical and avoid mental health services despite growing internal struggles.
“When we tell boys to ‘man up’ we’re essentially telling them to disconnect from their emotional and mental wellbeing,” McHugh explains. “At Momentum Health, we believe real strength lies in connection to yourself, to professional support and to your community. That is why our approach integrates physical, mental, emotional and financial wellbeing, rather than treating them as separate issues.”
This holistic approach sets Momentum Health apart from conventional healthcare models that focus only on symptoms instead of the whole person.
The New Frontline for Men’s Mental Health
According to the 2025 Digital Report for South Africa5, 78.9% of the population are now online, with mobile connectivity exceeding 193% due to multiple device ownership. Recognising that many men would rather engage privately through an app than visit a therapist’s office, Momentum Health has deployed technology to meet men where they are.
“Technology is a powerful equaliser,” says McHugh. “It breaks down barriers of stigma, geography, and access. By meeting men in the digital spaces, they already inhabit, we’re not just offering support, we are changing the way mental health care is delivered.”
The Hello Doctor platform lets men chat privately with health experts right on their phones. It gives them a safe, non-judgmental space to talk about their mental health without feeling embarrassed. This service isn’t just offering help; it’s changing the way mental health care works in South Africa.
Health and Wealth: Two Sides of the Same Coin
The link between health and financial wellbeing is clear. Poor health can derail financial goals, while financial stress can strain mental and emotional resilience. Momentum Health’s integration of financial and health services addresses a critical reality: mental health struggles and financial problems can create a devastating downward spiral.
“You cannot separate these aspects of wellbeing and expect sustainable outcomes. When we say, ‘your health is your wealth,’ we are talking about a fundamental truth: without mental and physical resilience, financial success becomes meaningless,” says McHugh.
Creating a Culture of Support
South African men must take a proactive stance, not just for themselves, but for their families, their communities and future generations.
“This is not about perfection. It is about progress,” says McHugh. “And this is not just about saving lives, though that alone would be enough, it is about transforming what it means to be a man in today’s society.”
Findings support use of P2Y12 therapy instead of aspirin for long term prevention
Source: Wikimedia CC0
Giving a P2Y12 inhibitor anti-clotting drug to patients with coronary artery disease is associated with lower rates of cardiovascular death, heart attack and stroke compared with traditional aspirin, with no increased risk of major bleeding, finds a study published by The BMJ.
P2Y12 inhibitors are often given to patients alongside aspirin (“dual therapy”) after percutaneous coronary intervention (PCI) – a procedure to widen or unblock a coronary artery – to help prevent cardiovascular events including heart attack and stroke.
After several months, patients are usually switched from dual therapy to lifelong aspirin, but some trials have suggested that a P2Y12 inhibitor may be more effective for long term prevention than aspirin.
To explore this further, researchers analysed individual patient data from five randomised clinical trials involving 16 117 patients (average age 65; 24% women) who were assigned to a P2Y12 inhibitor (clopidogrel or ticagrelor) or aspirin after completing dual therapy following PCI.
After an average follow-up period of around 4 years, P2Y12 inhibitor therapy was associated with a 23% lower risk of an outcome that combined cardiovascular death, heart attack, or stroke, compared with aspirin, with no significant difference in major bleeding. This means that for every 46 patients taking a P2Y12 inhibitor instead of aspirin after dual therapy, one cardiovascular death, heart attack, or stroke would be prevented.
When considering outcomes individually, P2Y12 inhibitor therapy reduced heart attacks and stroke compared with aspirin. However, all-cause death, cardiovascular death, and stent thrombosis were similar between the treatments.
The researchers acknowledge that some changes in the original design of some trials were needed to create uniform data, and that certain characteristics of individual trial populations may reduce the generalisability of the findings.
But they say no significant difference in major bleeding between groups was seen, and results were consistent after further analyses accounting for factors such as age, sex, geographical region, smoking, previous heart attack or stroke, underlying conditions and medication history, suggesting they are robust.
“Overall, this study supports preferential P2Y12 inhibitor monotherapy prescription over aspirin due to reductions in major adverse cardiac and cerebrovascular events (MACCE) without increasing major bleeding in the medium term,” say researchers in a linked editorial.
However, they note that “medium term efficacy does not necessarily extend lifelong, which is the duration we advise patients to continue these medications.”
As such, they suggest that “a large-scale globally representative trial directly comparing different monotherapy strategies (including discontinuation) with extended follow-up would benefit our understanding of the long-term impact of P2Y12 inhibitor monotherapy across the treatment class for secondary prevention following PCI.”
In a new study, investigators from McLean Hospital (a member of Mass General Brigham), Harvard Medical School, and the National Institute on Drug Abuse Intramural Research Program (NIDA-IRP) discovered that the tendency of people’s arousal to wane over the course of brain scans has been distorting the brain connection maps produced by functional magnetic resonance imaging (fMRI).
The team found that as people’s arousal levels dwindle during an fMRI, such as if they become more relaxed and sleepy, changes in breathing and heart rates alter blood oxygen levels in the brain—which are then falsely detected on the scan as neuronal activity.
“You’re laying down in a snug scanner for quite some time, often with only a low-engagement button press task to attend to or nothing to do at all, as the scanner monotonously hums and vibrates around you,” said first author Cole Korponay, PhD, MPA, a research fellow at the McLean Hospital Imaging Center. “These arousal-dampening conditions create the illusion that people’s brain connection strengths continuously inflate throughout the scan.”
fMRI scans are commonly used to non-invasively map brain connectivity, but the technique relies on changes in brain blood oxygen to indirectly measure neuronal activity. It is therefore vulnerable to “noise” from other processes that can affect blood oxygen – such as changes in breathing and heart rates.
And because breathing and heart rate patterns are closely tied to arousal levels, changes in arousal can introduce significant noise into fMRI data. Problematically, the conditions of an fMRI scan tend to progressively lull people into lower arousal states.
In the present study, the research team identified a specific blood flow signal that seemed to track both the decline in subject arousal levels and the illusory inflation of functional brain connection strengths.
This non-neuronal, physiological noise signal, termed the “systemic low frequency oscillation” (sLFO) signal, grew over time during scanning, in a spatial and temporal pattern that closely followed the pattern of the connection strength increases.
The researchers then demonstrated that a method called RIPTiDe, developed by co-senior author Blaise Frederick, PhD, an associate biophysicist at the McLean Imaging Center, to remove the sLFO signal from fMRI data, was able to eliminate the illusory connection strength increases.
“By adopting this sLFO denoising procedure, future studies can mitigate the distortive effects of arousal changes during brain scans and enhance the validity and reliability of fMRI findings,” said Korponay.
This research was supported by the National Institute on Drug Abuse, the National Institute of Mental Health, and the National Institute on Aging, all part of the National Institutes of Health.
Pretoria, 15 July 2025 – The South African Health Products Regulatory Authority (SAHPRA) was notified of the Lancet Global Health 2025; 13: e1250, an investigational study and its findings on substandard anti-cancer medications in Sub-Saharan African countries, including Ethiopia, Kenya, Malawi, and Cameroon. This study did not include South Africa. The seven (7) medicines/dosage forms mentioned in the study are cisplatin, oxaliplatin, methotrexate, doxorubicin, cyclophosphamide, ifosfamide, and leucovorin. The specific brands mentioned/shown in the article are neither registered nor marketed in South Africa.
SAHPRA, in terms of the Medicines and Related Substances Act 101 of 1965, as amended, and its General Regulations, requires medicines marketed in the country to meet prescribed requirements and adhere to set standards. Every batch of medicine produced must undergo testing to ensure that the integrity of the product is consistent with approved specifications before the release for sale, and imported medicines must additionally comply with the Guideline for Post-Importation Testing.
SAHPRA commenced internal processes to verify whether any of the South African-registered cancer medicines with the mentioned Active Pharmaceutical Ingredients (API) might have been affected or implicated. The cancer products registered and marketed in South Africa were not implicated/affected by the investigational study and its findings on substandard anti-cancer medicines. SAHPRA conducts risk-based post-market surveillance (PMS), sampling, and testing on high-risk medical products.
SAHPRA is satisfied that the marketed and registered cancer medicines meet the appropriate specifications; therefore, no substandard cancer medicines were detected.
“SAHPRA is committed to the three pillars of quality, safety, and efficacy. I am satisfied that our rigorous regulatory processes have borne fruit and that all patients, especially cancer patients, can rest assured that their health and well-being are not compromised,” indicated SAHPRA CEO, Dr Boitumelo Semete-Makokotlela.
A new weekly injectable drug could transform the lives of more than eight million people living with Parkinson’s disease, potentially replacing the need for multiple daily tablets.
UniSA PhD candidate Deepa Nakmode and Professor Sanjay Garg in the lab. Credit: UniSA
Scientists from the University of South Australia (UniSA) have developed a long-acting injectable formulation that delivers a steady dose of levodopa and carbidopa – two key medications for Parkinson’s – over an entire week.
The biodegradable formulation is delivered in a subcutaneous or intramuscular injection, where it gradually releases the medication over seven days.
Parkinson’s disease is the second most common neurological disorder, affecting more than 8.5 million people worldwide. Currently there is no cure and the symptoms – tremors, rigidity and slow movement – are managed with oral medications that must be taken several times a day.
The frequent dosing is a burden, especially for elderly patients or those with swallowing difficulties, leading to inconsistent medication levels, more side effects, and reduced effectiveness.
Lead researcher Professor Sanjay Garg, from UniSA’s Centre for Pharmaceutical Innovation, says the newly developed injectable could significantly improve treatment outcomes and patient adherence.
“Our goal was to create a formulation that simplifies treatment, improves patient compliance, and maintains consistent therapeutic levels of medication. This weekly injection could be a game-changer for Parkinson’s care,” Prof Garg says.
“Levodopa is the gold-standard therapy for Parkinson’s, but its short life span means it must be taken several times a day.”
UniSA PhD student Deepa Nakmode says the in-situ implant is designed to release both levodopa and carbidopa steadily over one week, maintaining consistent plasma levels and reducing the risks associated with fluctuating drug concentrations.
“After years of focused research, it’s incredibly rewarding to see our innovation in long-acting injectables for Parkinson’s disease reach this stage. Our invention has now been filed for an Australian patent,” Nakmode says.
The injectable gel combines an FDA-approved biodegradable polymer PLGA with Eudragit L-100, a pH-sensitive polymer, to achieve a controlled and sustained drug release.
Extensive lab tests confirmed the system’s effectiveness and safety:
More than 90% of the levodopa dose and more than 81% of the carbidopa dose was released over seven days.
The implant degraded by over 80% within a week and showed no significant toxicity in cell viability tests.
The formulation can be easily administered through a fine 22-gauge needle, minimising discomfort and eliminating the need for surgical implant.
“The implications of this research are profound,” Prof Garg says. “By reducing the frequency of dosing from multiple times a day to a weekly injection is a major step forward in Parkinson’s therapy. We’re not just improving how the drug is delivered; we’re improving patients’ lives.”
Prof Garg says the technology could also be adapted for other chronic conditions such as cancer, diabetes, neurodegenerative disorders, pain management, and chronic infections that require long-term drug delivery.in
The system can be tuned to release drugs over a period ranging from a few days to several weeks depending on therapeutic needs.
UniSA scientists hope to start clinical trials in the near future and are exploring commercialisation opportunities.
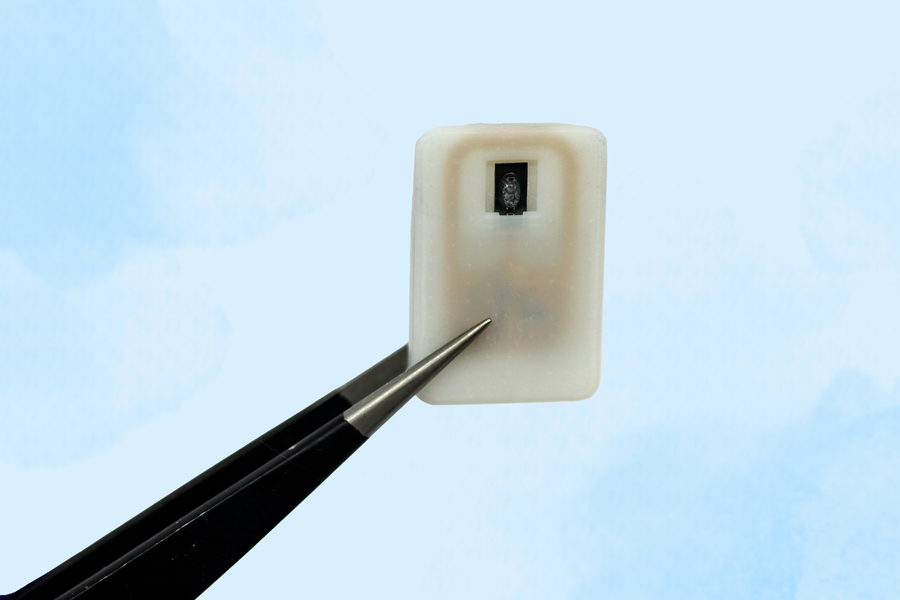
The new implant carries a reservoir of glucagon that can be stored under the skin and deployed during an emergency — with no injections needed.
Caption:A new implantable device carries a reservoir of glucagon that can be stored under the skin and could save diabetes patients from dangerously low blood sugar.
Image: Courtesy of the researchers
For people with Type 1 diabetes, developing hypoglycaemia, or low blood sugar, is an ever-present threat. When glucose levels become extremely low, it creates a life-threatening situation for which the standard treatment of care is injecting a hormone called glucagon.
As an emergency backup, for cases where patients may not realise that their blood sugar is dropping to dangerous levels, MIT engineers have designed an implantable reservoir that can remain under the skin and be triggered to release glucagon when blood sugar levels get too low.
This approach could also help in cases where hypoglycaemia occurs during sleep, or for diabetic children who are unable to administer injections on their own.
“This is a small, emergency-event device that can be placed under the skin, where it is ready to act if the patient’s blood sugar drops too low,” says Daniel Anderson, a professor in MIT’s Department of Chemical Engineering, a member of MIT’s Koch Institute for Integrative Cancer Research and Institute for Medical Engineering and Science (IMES), and the senior author of the study. “Our goal was to build a device that is always ready to protect patients from low blood sugar. We think this can also help relieve the fear of hypoglycaemia that many patients, and their parents, suffer from.”
The researchers showed that this device could also be used to deliver emergency doses of epinephrine, a drug that is used to treat heart attacks and can also prevent severe allergic reactions, including anaphylactic shock.
Siddharth Krishnan, a former MIT research scientist who is now an assistant professor of electrical engineering at Stanford University, is the lead author of the study, which appears today in Nature Biomedical Engineering.
Emergency response
Most patients with type 1 diabetes use daily insulin injections to help their body absorb sugar and prevent their blood sugar levels from getting too high. However, if their blood sugar levels get too low, they develop hypoglycaemia, which can lead to confusion and seizures, and may be fatal if it goes untreated.
To combat hypoglycaemia, some patients carry preloaded syringes of glucagon, a hormone that stimulates the liver to release glucose into the bloodstream. However, it isn’t always easy for people, especially children, to know when they are becoming hypoglycaemic.
“Some patients can sense when they’re getting low blood sugar, and go eat something or give themselves glucagon,” Anderson says. “But some are unaware that they’re hypoglycaemic, and they can just slip into confusion and coma. This is also a problem when patients sleep, as they are reliant on glucose sensor alarms to wake them when sugar drops dangerously low.”
To make it easier to counteract hypoglycaemia, the MIT team set out to design an emergency device that could be triggered either by the person using it, or automatically by a sensor.
The device, which is about the size of a quarter, contains a small drug reservoir made of a 3D-printed polymer. The reservoir is sealed with a special material known as a shape-memory alloy, which can be programmed to change its shape when heated. In this case, the researcher used a nickel-titanium alloy that is programmed to curl from a flat slab into a U-shape when heated to 40 degrees Celsius.
Like many other protein or peptide drugs, glucagon tends to break down quickly, so the liquid form can’t be stored long-term in the body. Instead, the MIT team created a powdered version of the drug, which remains stable for much longer and stays in the reservoir until released.
Each device can carry either one or four doses of glucagon, and it also includes an antenna tuned to respond to a specific frequency in the radiofrequency range. That allows it to be remotely triggered to turn on a small electrical current, which is used to heat the shape-memory alloy. When the temperature reaches the 40-degree threshold, the slab bends into a U shape, releasing the contents of the reservoir.
Because the device can receive wireless signals, it could also be designed so that drug release is triggered by a glucose monitor when the wearer’s blood sugar drops below a certain level.
“One of the key features of this type of digital drug delivery system is that you can have it talk to sensors,” Krishnan says. “In this case, the continuous glucose-monitoring technology that a lot of patients use is something that would be easy for these types of devices to interface with.”
Reversing hypoglycaemia
After implanting the device in diabetic mice, the researchers used it to trigger glucagon release as the animals’ blood sugar levels were dropping. Within less than 10 minutes of activating the drug release, blood sugar levels began to level off, allowing them to remain within the normal range and avert hypoglycaemia.
The researchers also tested the device with a powdered version of epinephrine. They found that within 10 minutes of drug release, epinephrine levels in the bloodstream became elevated and heart rate increased.
In this study, the researchers kept the devices implanted for up to four weeks, but they now plan to see if they can extend that time up to at least a year.
“The idea is you would have enough doses that can provide this therapeutic rescue event over a significant period of time. We don’t know exactly what that is — maybe a year, maybe a few years, and we’re currently working on establishing what the optimal lifetime is. But then after that, it would need to be replaced,” Krishnan says.
Typically, when a medical device is implanted in the body, scar tissue develops around the device, which can interfere with its function. However, in this study, the researchers showed that even after fibrotic tissue formed around the implant, they were able to successfully trigger the drug release.
The researchers are now planning for additional animal studies and hope to begin testing the device in clinical trials within the next three years.
“It’s really exciting to see our team accomplish this, which I hope will someday help diabetic patients and could more broadly provide a new paradigm for delivering any emergency medicine,” says Robert Langer, the David H. Koch Institute Professor at MIT and an author of the paper.
Other authors of the paper include Laura O’Keeffe, Arnab Rudra, Derin Gumustop, Nima Khatib, Claudia Liu, Jiawei Yang, Athena Wang, Matthew Bochenek, Yen-Chun Lu, Suman Bose, and Kaelan Reed.
The research was funded by the Leona M. and Harry B. Helmsley Charitable Trust, the National Institutes of Health, a JDRF postdoctoral fellowship, and the National Institute of Biomedical Imaging and Bioengineering.
A healthy lifestyle has important benefits, but weight alone might not give an adequate picture of someone’s health, say experts
Source: Pixabay CC0
Focusing solely on achieving weight loss for people with a high body mass index (BMI) may do more harm than good, argue experts in The BMJ.
Dr Juan Franco and colleagues say, on average, people with high weight will not be able to sustain a clinically relevant weight loss with lifestyle interventions, while the potential harms of weight loss interventions, including the reinforcement of weight stigma, are still unclear.
They stress that a healthy lifestyle has important benefits, but that weight alone might not give an adequate picture of someone’s health, and say doctors should provide high quality, evidence based care reflecting individual preferences and needs, regardless of weight.
Lifestyle interventions that focus on restricting an individual’s energy intake and increasing their physical activity levels have for many decades been the mainstay recommendation to reduce weight in people with obesity, explain the authors.
However, rigorous evidence has indicated that these lifestyle interventions are largely ineffective in providing sustained long term weight loss and reducing cardiovascular events (eg, heart attacks and strokes) or death.
Even though a healthy lifestyle provides important benefits, acknowledging that weight alone might not give an adequate picture of someone’s health, and recognising the limitations of lifestyle interventions for weight loss, could pave the way for more effective and patient centred care, they say.
Focusing on weight loss might also contribute to societal weight bias – negative attitudes, assumptions, and judgments about people based on their weight – which may not only have adverse effects on mental health but may also be associated with disordered eating, the adoption of unhealthy habits, and weight gain, they add.
They point out that recent clinical guidelines reflect the growing recognition that weight is an inadequate measure of health, and alternative approaches, such as Health at Every Size (HAES), acknowledge that good health can be achieved regardless of weight loss and have shown promising results in improving eating behaviours.
While these approaches should be evaluated in large clinical trials, doctors can learn from them to provide better and more compassionate care for patients with larger bodies, they suggest.
“Doctors should be prepared to inform individuals seeking weight loss about the potential benefits and harms of interventions and minimise the risk of developing eating disorders and long term impacts on metabolism,” they write. “Such a patient centred approach is likely to provide better care by aligning with patient preferences and circumstances while also reducing weight bias.”
They conclude: “Doctors’ advice about healthy eating and physical activity is still relevant as it may result in better health. The main goal is to offer good care irrespective of weight, which means not caring less but rather discussing benefits, harms, and what is important to the patient.”
Women diagnosed with premenstrual symptoms have a slightly increased risk of developing cardiovascular disease later in life. This is shown by a new study from Karolinska Institutet published in Nature Cardiovascular Research.
Premenstrual symptoms include premenstrual syndrome (PMS) and the more severe form, premenstrual dysphoric disorder (PMDD). The symptoms, which appear a few days before menstruation and then subside, can be both psychological and physical.
The study included more than 99 000 women with premenstrual symptoms who were followed for up to 22 years. The researchers compared their health with women without these symptoms – both in the general population and by comparing them with their own sisters to take into account hereditary factors and upbringing.
The results show that women with premenstrual symptoms had about a ten per cent higher risk of developing cardiovascular disease. When the researchers also looked at different types of cardiovascular disease, they found that the link was particularly strong for heart rhythm disorders (arrhythmias), where the risk was 31 per cent higher, and for stroke caused by a blood clot, where the risk was 27 per cent higher. Even after the researchers took into account other factors such as smoking, BMI and mental health, the link between premenstrual symptoms and increased disease risk remained.
”The increased risk was particularly clear in women who were diagnosed before the age of 25 and in those who had also experienced postnatal depression, a condition that can also be caused by hormonal fluctuations,” says first author Yihui Yang, PhD student at the Institute of Environmental Medicine.
Research has not yet identified the cause of this link, but the researchers behind the study suggest three possible explanations. One is that women with premenstrual symptoms may have a disrupted regulation of the renin-angiotensin-aldosterone system (RAAS), which controls blood pressure and fluid balance in the body, among other things. The second is that these women have increased levels of inflammation in the body, which is a known risk factor for atherosclerosis and other heart problems. Finally, it may be because women with premenstrual symptoms may have metabolic abnormalities, which are linked to an increased risk of both stroke and heart attack.
”We hope that our findings will contribute to greater awareness that premenstrual disorders not only affect daily life but can also have consequences for long-term health,” says last author Donghao Lu, associate professor at the same department.
New UCLA research finds that small group professional coaching can reduce physician burnout rates by up to 30%, suggesting that it is more effective than the traditional, and more expensive, one-on-one coaching method.
Nearly half of physicians in the US suffer from burnout, which is marked by emotional exhaustion, depersonalisation and decreased personal accomplishment. These can lead to medical errors and other harmful consequences to the healthcare system and patient outcomes, said lead author Dr Joshua Khalili, director of physician wellness in the UCLA Department of Medicine and assistant clinical professor of medicine at the David Geffen School of Medicine at UCLA.
“Most current evidence related to professional coaching is related to individual coaching and its impact on reducing burnout,” Khalili said. “But individual coaching can be quite costly, which is a barrier to broad implementation.”
Physician burnout is estimated to cost the US healthcare system about $4.6 billion annually, mostly due to costs associated with physician turnover and fewer clinical hours.
The researchers conducted a randomised, wait-list controlled trial with 79 UCLA attending internal medicine physicians for just over a year starting in March 2023. The intervention consisted of six one-hour coaching sessions, with one-third of the group receiving one-on-one coaching via Zoom while another third were coached in small groups consisting of three physicians and one coach. The final third acted as control group, receiving no coaching during the first few months of the trial, and subsequently received six, one-on-one coaching sessions.
The primary outcome the researchers measured was overall burnout. They also examined areas of work life such as workload, control rewards, community, fairness, and values; work engagement such as vigour, dedication, and absorption; self-efficacy, and social support. They measured each of these outcomes before and after the intervention and again six months afterwards.
They found that small group intervention participants experienced a nearly 30% reduction in burnout rate. The burnout rate for the one-on-one coaching fell by 13.5%. By contrast, the control group experienced an 11% increase in burnout rates. Burnout remained stable among the small group participants and continued to fall in the one-on-one group six months after the initial intervention.
Coaching for the one-on-one sessions cost $1000 per participant, compared with $400 for the small group coaching sessions.
“This new, small-group model of professional coaching can make a significant impact in physician burnout and costs much less than the one-on-one model,” Khalili said.
Study limitations include potential selection bias among participants who would most likely benefit from the intervention. The baseline overall burnout rate was higher in the small group coaching arm (70.4%) compared to the one-on-one group (40.0%); however, relative reductions in burnout were similar: 42% in the small group intervention compared to 34% the one-on-one group. In addition, the study was conducted at a large academic centre whose physicians may not be comparable to those in other healthcare institutions.
The researchers are now providing coaching to physicians in the UCLA Department of Medicine and hope that this research encourages other health care institutions and organisations to implement professional coaching, Khalili said.
“By improving physicians’ well-being, engagement, and sense of support, interventions like coaching can enhance the quality of care patients receive, making this a public health priority, not just a workplace issue,” he said.