Credit: Darryl Leja National Human Genome Research Institute National Institutes Of Health
Because treatment of the whole prostate can lead to long-term side effects in patients with prostate cancer, interest in minimally invasive, focal treatment options has been growing for certain patients. A clinical trial published in BJU International generated promising results for a type of focal therapy, which directly targets the cancer and spares the remainder of the unaffected prostate gland.
The ProFocal Laser Therapy for Prostate Tissue Ablation (PFLT-PC) trial is the first pivotal trial of ProFocal®, a novel, cooled laser focal therapy device for prostate cancer treatment.
In the 100-participant trial, 84% of patients had no clinically significant prostate cancer on their 3-month post-treatment biopsy. The treatment provided similar cancer-related outcomes to those that have been reported for other focal therapy devices, but with an improved safety profile and low rates of incontinence.
“This new technology is very promising with excellent cancer control while preserving patients’ quality of life,” said corresponding author Jonathan Kam, MD, of Nepean Hospital, in Australia. “Traditional radical prostatectomy and radiotherapy for prostate cancer results in very high rates of incontinence and erectile dysfunction. With this new technology, patients can have their prostate cancer treated with very low risk of suffering the side effects associated with traditional prostate cancer treatments.”
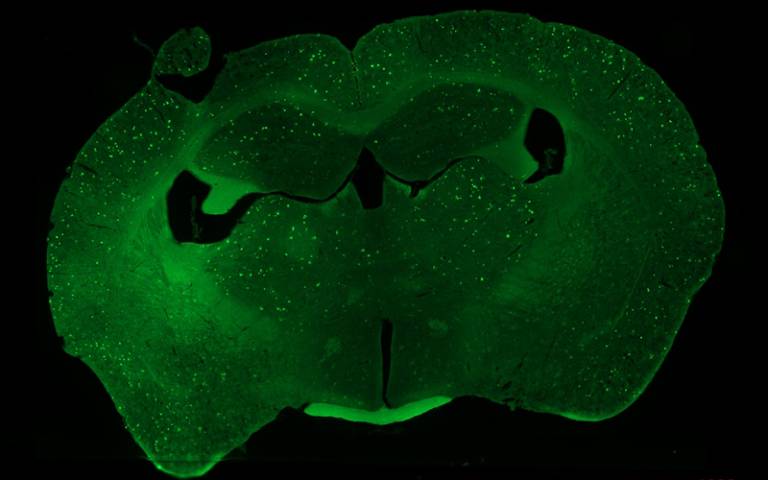
Mouse brain section highlights amyloid plaques, seen as bright green flecks (due to staining). Credit: Shipley et al.
Memory dysfunction in Alzheimer’s disease may be linked to impairment in how the brain replays our recent experiences while we are resting, according to a new study in mice by UCL scientists. The researchers say their findings, published in Current Biology, could help scientists develop drug treatments targeting this impaired brain function, or help design new tests for early diagnosis.
Co-lead author Dr Sarah Shipley (UCL Cell & Developmental Biology) said: “Alzheimer’s disease is caused by the build-up of harmful proteins and plaques in the brain, leading to symptoms such as memory loss and impaired navigation – but it’s not well understood exactly how these plaques disrupt normal brain processes.
“We wanted to understand how the function of brain cells changes as the disease develops, to identify what’s driving these symptoms.
“When we rest, our brains normally replay recent experiences – this is thought to be key to how memories are formed and maintained. We found this replay process is disrupted in mice engineered to develop the amyloid plaques characteristic of Alzheimer’s, and this disruption is associated with how badly animals perform on memory tasks.”
The replay process, which occurs in the brain’s hippocampus, involves place cells firing in rapid sequences during rest. Place cells – discovered by Nobel prize-winning UCL neuroscientist Professor John O’Keefe – are neurons (brain cells) that represent specific locations. When we visit somewhere, particular place cells fire, and as we move the cells fire in a sequence. Later, when we rest, these cells reactivate in the same sequence, helping memories become ingrained.
For the study, the researchers were testing how well mice performed in a simple maze task, while monitoring their brain activity with sets of electrodes that could simultaneously track roughly 100 individual place cells.
In mice with amyloid pathology, the replay process was fundamentally altered. Surprisingly, replay events occurred just as frequently as in healthy mice, but their structure was disorganised. The normal, coordinated patterns of place cell activity that should reinforce memories were scrambled. The researchers also found that place cells in affected mice became less stable over time, with individual neurons no longer reliably coding the same locations, particularly after rest periods – precisely when replay should be strengthening these representations.
This disruption had consequences on memory tasks: affected mice performed worse in the maze, appearing to forget where they had already been and revisiting corridors that led nowhere.
Co-lead author Professor Caswell Barry (UCL Cell & Developmental Biology) said: “We’ve uncovered a breakdown in how the brain consolidates memories, visible at the level of individual neurons. What’s striking is that replay events still occur – but they’ve lost their normal structure. It’s not that the brain stops trying to consolidate memories; the process itself has gone wrong.
“We hope our findings could help develop tests to detect Alzheimer’s early, before extensive damage has occurred, or lead to new treatments targeting this replay process. We’re now investigating whether we can manipulate replay through the neurotransmitter acetylcholine, which is already targeted by drugs used to treat Alzheimer’s symptoms. By understanding the mechanism better, we hope to make such treatments more effective.”
Following a Mediterranean diet is associated with a lower risk of all types of stroke among women, according to a study published on February 4, 2026, in Neurology® Open Access, an official journal of the American Academy of Neurology. The study does not prove that the Mediterranean diet is the cause of the lower risk of stroke; it only shows an association.
The diet was associated with a lower risk of stroke overall, as well as ischaemic stroke and haemorrhagic stroke. The Mediterranean diet includes a high intake of vegetables, legumes, fruits, fish and healthy fats such as olive oil, and a low intake of dairy products, meats and saturated fatty acids.
“Our findings support the mounting evidence that a healthy diet is critical to stroke prevention,” said study author Sophia S. Wang, PhD, of City of Hope Comprehensive Cancer Center in Duarte, California. “We were especially interested to see that this finding applies to haemorrhagic stroke, as few large studies have looked at this type of stroke.”
The study involved 105 614 women with an average age of 53 at the start of the study who had no history of stroke. The participants filled out a questionnaire at the start of the study about their diet. Participants were given a score of zero to nine based on how closely they followed the Mediterranean diet. People received one point if they consumed above the overall average in the population in these categories: whole grain cereals, fruits, vegetables, legumes, olive oil and fish, plus drinking a moderate amount of alcohol.
They also received one point if they consumed a below-average amount of red meat and dairy products. A total of 30% of participants had scores of six to nine – the highest group. And 13% had scores of zero to two, the lowest group.
The participants were followed for an average of 21 years. During that time, 4083 strokes occurred, with 3358 ischaemic strokes and 725 haemorrhagic strokes. For ischaemic strokes, there were 1058 among the 31 638 people in the highest group compared to 395 cases among the 13 204 people in the lowest group.
For haemorrhagic stroke, there were 211 strokes among those in the highest group, compared to 91 among the lowest group. When researchers adjusted for other factors that could affect stroke risk, such as smoking, physical activity and high blood pressure, they found that those in the highest group were 18% less likely to have a stroke than those in the lowest group. They were 16% less likely to have an ischaemic stroke and 25% less likely to have a haemorrhagic stroke.
“Stroke is a leading cause of death and disability, so it’s exciting to think that improving our diets could lessen our risk for this devastating disease,” said Wang. “Further studies are needed to confirm these findings and to help us understand the mechanisms behind them so we could identify new ways to prevent stroke.”
A limitation of the study is that people reported their own diet information, so they may not have remembered correctly.
Under South African law, no one may practise medicine unless they have the proper training and are officially registered. Photo by Usman Yousaf on Unsplash
By Elna Schütz
Bogus medical practitioners threaten the health of patients and undermine trust in doctors. The problem might be growing, but so is the fight against it.
“If you’re in the hands of an unqualified person, you’re as well as dead, and we think it is not fair for the country,” Dr Magome Masike tells Spotlight.
He is the Registrar of the Health Professions Council of South Africa (HPCSA), which is responsible for the registration of medical doctors and other health professionals in South Africa.
The controversy over bogus doctors gained widespread attention in late 2023 when it was discovered that ‘TikTok doctor’ Matthew Lani lied about being a medical doctor. In his videos, Lani was often seen in scrubs and wearing a stethoscope, impersonating a medical doctor. Although he was arrested at Helen Joseph Hospital in Johannesburg, the National Prosecuting Authority eventually decided not to prosecute.
The term bogus doctor has become a shorthand for any medical practitioner who is working without being properly qualified or registered by the HPCSA. In practice, being “bogus” can also apply to physiotherapists, interns, or anyone else practising medicine.
The misrepresentation may include using fraudulent certificates, using another practitioner’s registration, or being suspended or erased from the register. It can involve someone who studied but did not fully qualify, or has not kept up to date with their registration. Masike gives the example of the child of a registered practitioner who decides to take on their parent’s practice after their death without themselves being registered.
It is an ongoing problem. In the beginning of February, the HPCSA says it facilitated the arrest of a woman working at a medical facility in Midrand, north of Johannesburg, allegedly without being correctly registered to practice medicine.
Bogus qualifications are part of the larger problem of healthcare fraud. According to research in a report by risk management services firm D-Finitive, it is estimated that this fraud overall costs African countries more than USD50 billion in 2012. In the South African private sector, that comes to about R22-28 billion a year. The report explains that beyond bogus practitioners, there is a problem with similar fraud, like doctors billing more clients than is realistic, manipulating diagnostic and procedural codes, or deceased doctors billing the government for decades after their death. At times, this type of fraud is reportedly executed by syndicates.
“While the majority of practitioners are honest and committed to patient care, it takes only a small number of bad actors, whether unregistered impostors or credentialed professionals abusing the system, to inflict widespread damage,” says Dr Katlego Mothudi, Managing Director of the Board of Healthcare Funders (BHF).
A substantial problem
Masike says that from March 2024 to February 2025, 49 bogus practitioners were caught and arrested. From April to December 2025, that number was at 17. Even though these numbers do not suggest a year-on-year increase, Masike says that overall, the numbers are increasing.
The HPCSA’s annual report for 2024/2025 shows that 589 investigations into unregistered persons were concluded in the year in question. Over the past five years, 3 708 complaints were received.
The majority of bogus practitioners who have been caught were operating in economic hubs of the Western Cape, Gauteng, and KwaZulu-Natal, Masike says. “Bogus people want money, so they go where there’s money,” he explains. However, while the trend tends urban, he says rural communities also fall prey to scammers.
“A notable pattern is that many of these individuals use or forge the details of legitimately registered practitioners,” Masike says.
It is, of course, unclear how many unlicensed practitioners are not yet caught. “We can tell you the problem is bigger than we think,” Masike says. The problem, he says, is sector-wide and stretches across different health professions, with most of these illegal practices occurring in the private sector. Masike adds that bogus doctors often work with a network of others, for example, those who supply unregistered or fake medicines.
Mothudi also says that the problem is growing. “Medical schemes are seeing a rise in suspicious provider activity picked up through claims analysis and credential verification processes,” he says. This may include practitioners misrepresenting their registration status, practising outside their approved scope, or using the registration details of legitimate practitioners to submit claims.
Risk to patients
Catching and prosecuting bogus practitioners is crucial because they can pose a direct danger to unsuspecting patients. “Unregistered medical doctors, like other health professionals, pose severe risks to patients, including serious physical harm, injury, and misdiagnosis which may lead to death, due to their lack of necessary training, ethical standards and relevant qualifications,” warns Foster Mohale, the spokesperson for the National Department of Health.
Dr Zanele Bikitsha, National Vice Chairperson of the South African Medical Association, cautions that if bogus doctors are performing procedures, it will likely be in settings that are not appropriate or sterile.
“They’re not going to go to a registered facility, because they know they’ll be caught, so this puts patients in danger as well.”
While some operate on a cash basis, Mothudi says that submitting claims to medical schemes is attractive because it allows for much larger and repeatable payouts. “In some cases, bogus practitioners submit claims using stolen, borrowed or fraudulently obtained practice numbers belonging to legitimately registered healthcare professionals,” he says. “In other instances, they collude with registered providers who allow their credentials to be misused in exchange for payment.”
Knowing the signs
While the HPCSA undertakes compliance inspections, there are some clear signs that might help the public spot a bogus practitioner. Firstly, it is a legal requirement to have registration information easily visible in a practitioner’s practice and on the letterhead of documents or prescription notes.
Members of the public can also look up a doctor’s credentials. All registered practitioners should be listed in the HPCSA’s digital register online, which is publicly searchable. With as little as the practitioner’s surname, the system lets users search for registered practitioners.
Masike points out that a trained doctor tends to take an extensive medical history and make a systemic or wide-reaching inquiry. He recommends that patients look out for how doctors speak and whether they use and are able to explain medical terminology.
Complaints can be filed with the HPCSA’s Inspectorate, including anonymously. Their call centre is at 0123389300/1 and they can be e-mailed at office@hpcsa.co.za. Suspicious practitioners may also be reported to hospitals, the Department of Health, SAMA or other medical organisations.
Processing the problem
Complaints typically lead to an investigation by the HPCSA Inspectorate, which works together with other entities, such as the South African Health Products Regulatory Authority (SAHPRA), the Office of Health Standards Compliance, the Special Investigating Unit (SIU), and the South African Police Service.
Masike explains that the investigation tends to lead to a clandestine operation and involves the police arresting the suspects. He adds that police recently assigned specific staff members to focus on these cases. He says that once the case goes to court, there is a conviction rate of around 77%, although this may have changed. “Many of the cases from 2023 to 2025 remain before the courts, and therefore updated conviction statistics are not yet available.”
Practising medicine without proper training and registration is in contravention of Section 17(1) of the Health Professions Act, 56 of 1974. Typical sentences for such fraud include fines, such as R12 000, or around two years imprisonment. In one 2017 case, a man who had treated almost a thousand patients over six years was sentenced to 20 years’ imprisonment by the Mahikeng High Court in the North West.
Bikitsha says there are other systemic changes that could help catch the problem earlier on. “If you are still paper-based, you are at risk,” she says, referring to the way that hospitals and institutes tend to verify the qualifications of most interns, locums and medical practitioners. She argues that upgrading to biometrics and digital systems would decrease the risk of fraud.
Another step forward is simply to increase public awareness and education, so that patients know the risks.
Masike concurs. “We need society to stand up to this,” he says. “We need a participating community to get rid of this malaise, otherwise it will continue forever.”
The largest genetic study of anxiety disorders to date has identified 58 genetic variants associated with anxiety, most of which have not been identified before now.
Photo by Joice Kelly on Unsplash
In the largest genetic study of anxiety disorders to date, new research from the Institute of Psychiatry, Psychology & Neuroscience (IoPPN) at King’s College London, in partnership with Texas A&M and the Institute of Psychiatric Phenomics and Genomics (IPPG) at LMU Munich, has identified 58 genetic variants associated with anxiety, most of which have not been identified before now.
The research, published in Nature Genetics, confirmed that, rather than being driven by a single “anxiety gene”, anxiety disorders are influenced by numerous genetic variants from across the genome, with each contributing a small effect.
The researchers compared the genetic data of 120 000 people diagnosed with an anxiety disorder to almost 730 000 people without.
Their analysis of the data notably highlighted the role of several genes involved in GABAergic signalling; a key system that regulates brain activity.
“Anxiety disorders arise from the interplay of genetic vulnerability and life experience. At a time when rates of anxiety are rising rapidly in our young people, by identifying robust genetic signals offering novel insight into the biological foundations of these debilitating disorders, this research helps move the field toward more precise and effective approaches to prevention and care.”
Professor Thalia Eley, Professor of Developmental Behavioural Genetics at King’s IoPPN and one of the study’s senior authors
While the research provides a biological basis for anxiety, the researchers do not advocate for the use of genetic testing to diagnose anxiety.
Professor John Hettema, from the Department of Psychiatry at Texas A&M University Naresh K. Vashisht College of Medicine, another of the study’s senior authors said, “Anxiety disorders and their underlying sources of genetic risk have been understudied compared to other psychiatric conditions, so this study substantially advances this critical knowledge.”
Prof Jürgen Deckert, Julius Maximilians University, Würzburg, Germany wrote “The results of the study provide evidence for a role of several previously unknown molecular pathways in the etiology of anxiety, beyond the previously identified GABAergic system. They will provide the basis for future studies in cell culture, animal models and humans which will contribute to a better understanding of the neurobiology of anxiety and as a consequence to innovative and individualized therapies.”
Genome-wide association study of major anxiety disorders in 122,341 European ancestry cases identifies 58 loci and highlights GABAergic signaling (DOI 10.1038/s41588-025-02485-8) (Eley, Mattheisen, Hettema et al) was published in Nature Genetics.